Prevalence and Outcome of Secondary Hemophagocytic Lymphohistiocytosis Among SIRS Patients: Results from a Prospective Cohort Study

 ,
,
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design
2.2. Data Collection and Laboratory Analyses
2.3. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Features of Hemophagocytic Syndrome
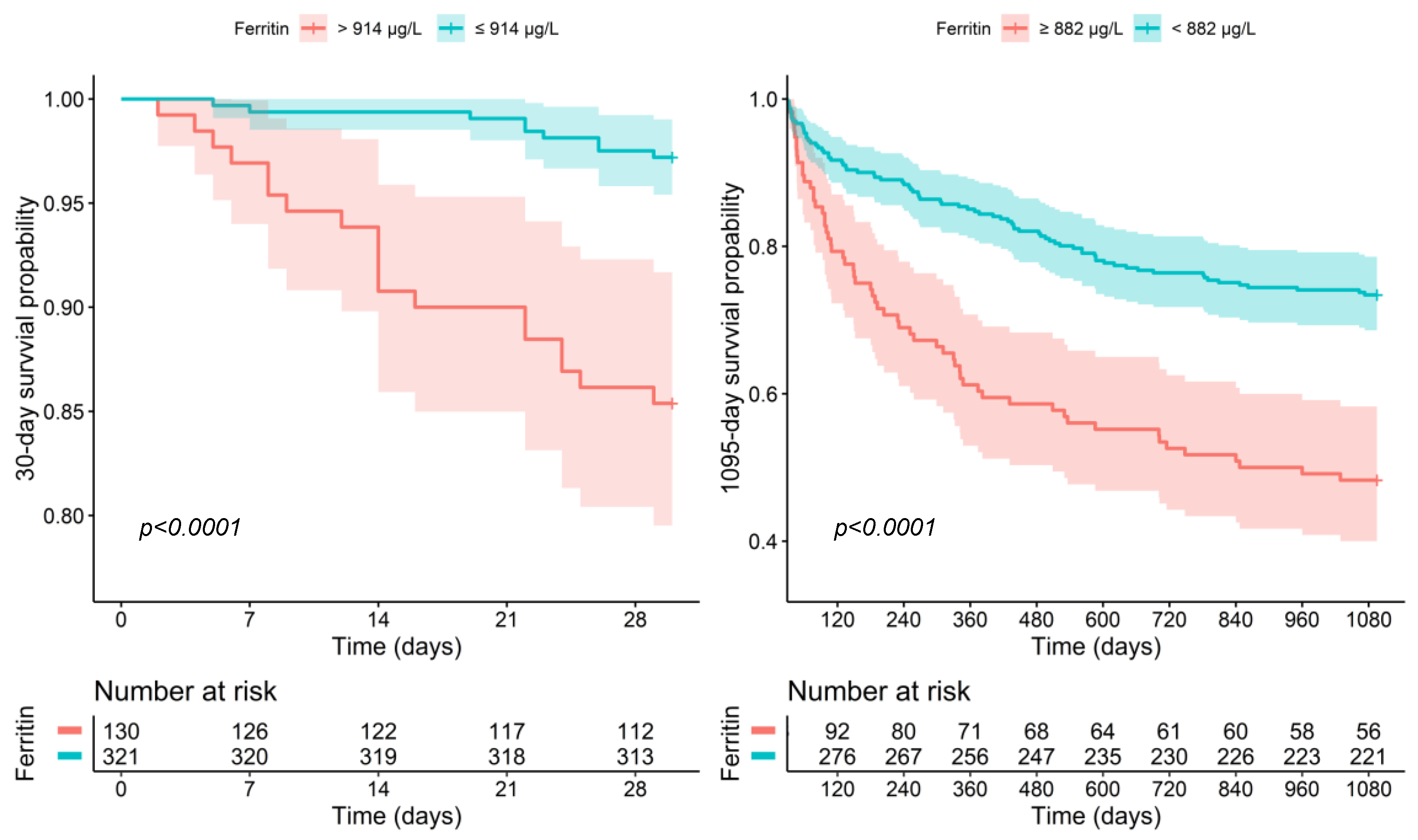
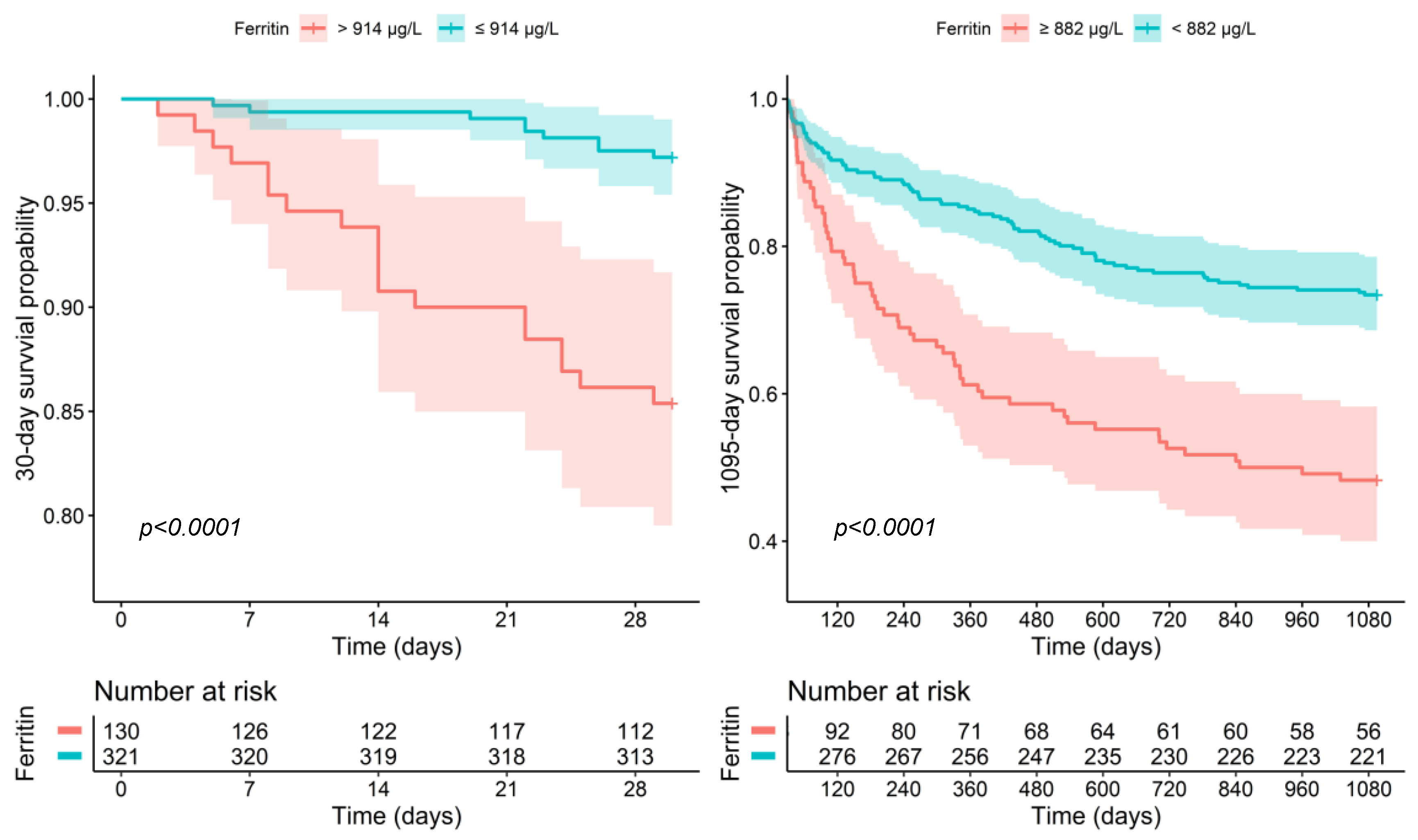
3.3. Survival Data
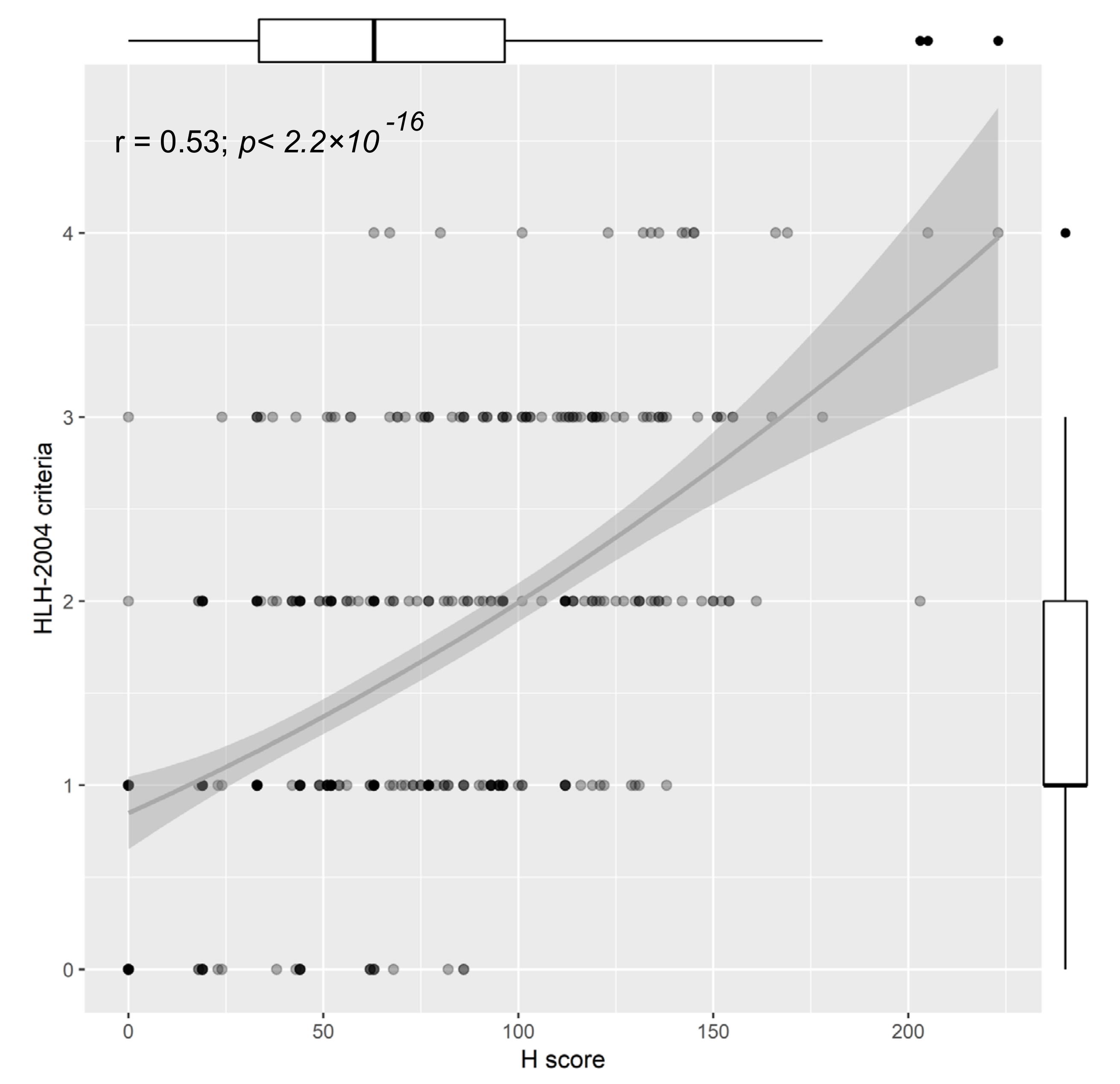
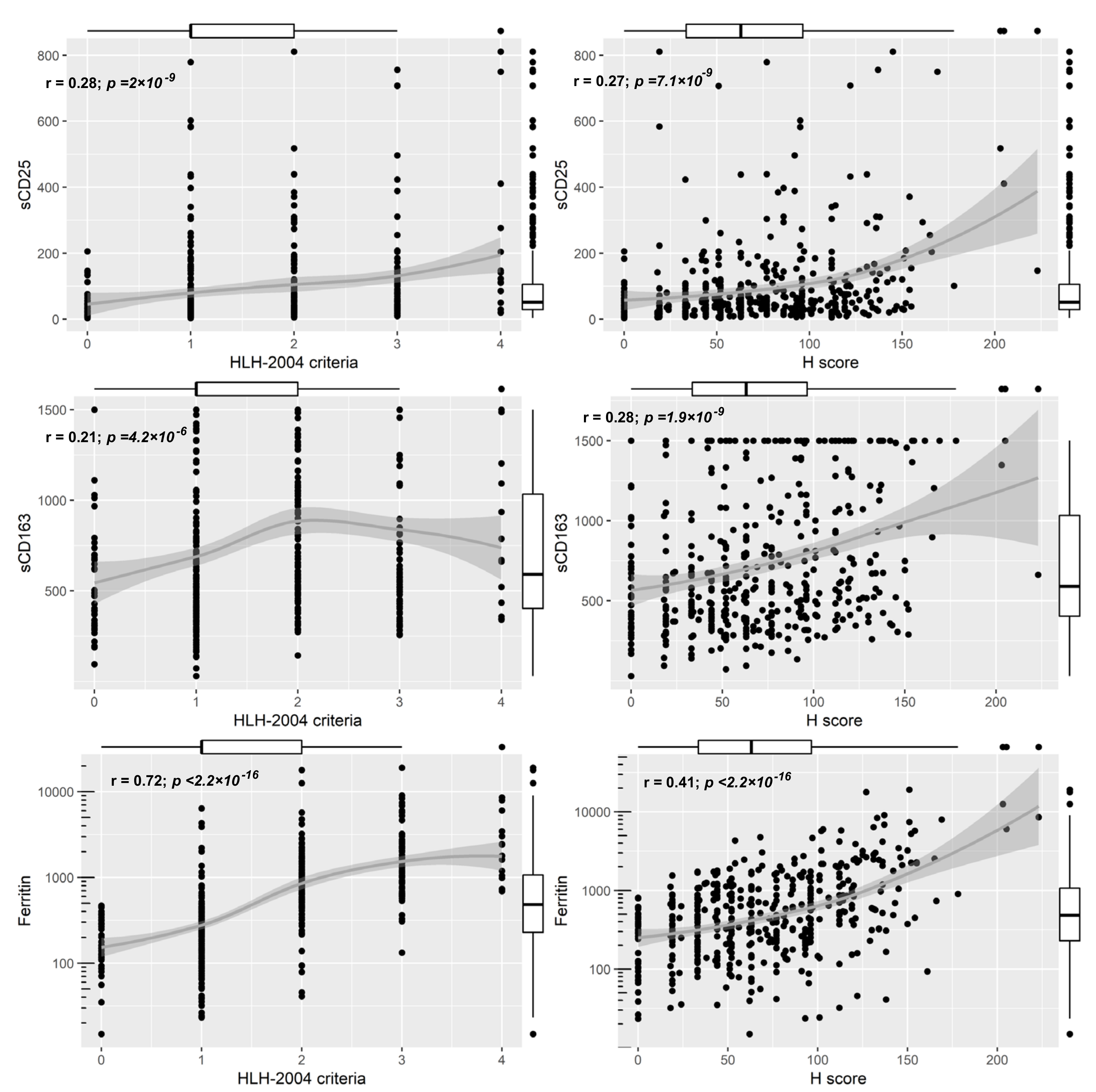
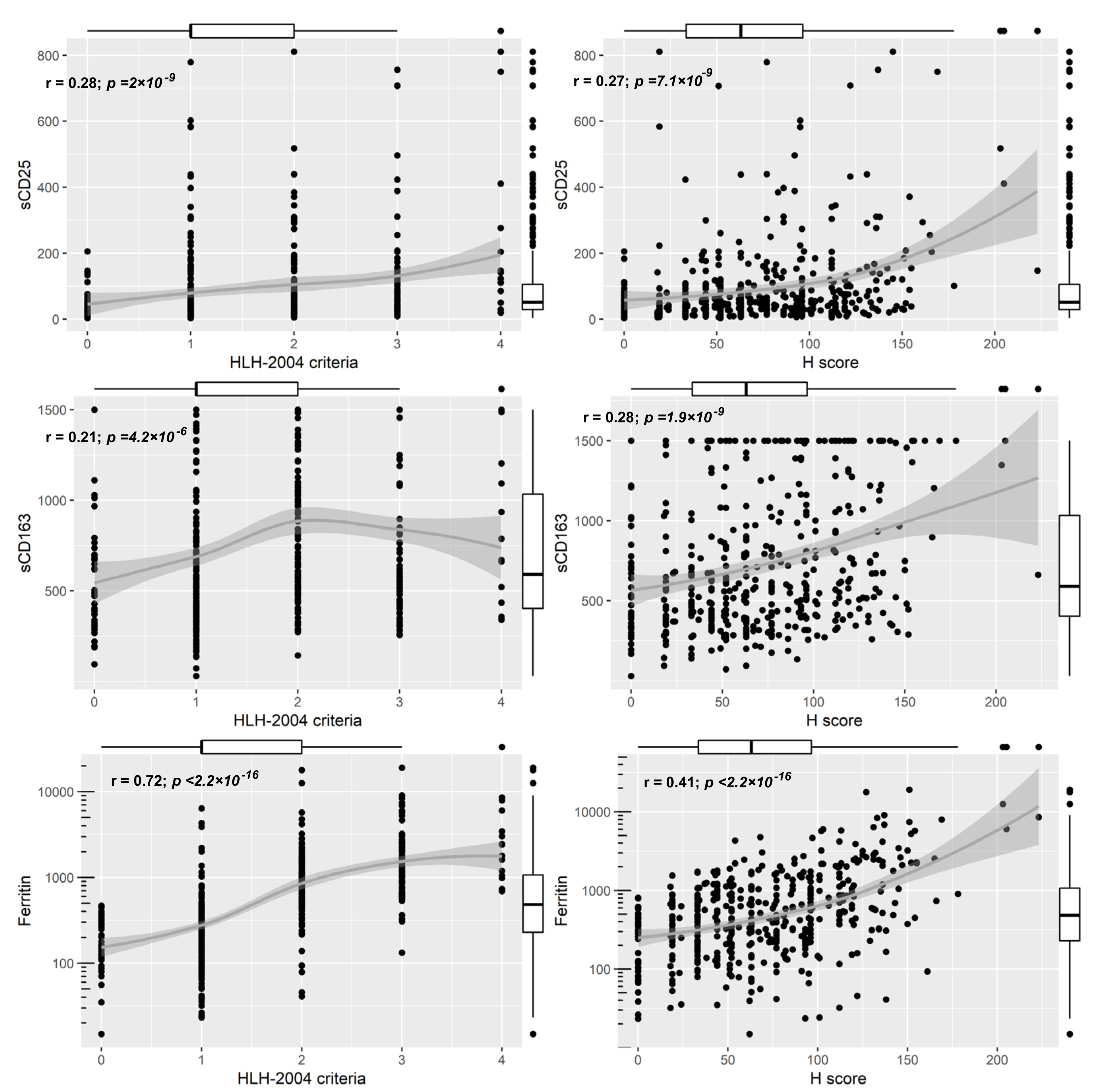
3.4. Prediction of Hemophagocytosis Scores and Utility of Biomarkers
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sepulveda, F.E.; de Saint Basile, G. Hemophagocytic syndrome: Primary forms and predisposing conditions. Curr. Opin. Immunol. 2017, 49, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, R. The histiocytoses. Clin. Lab. Med. 1999, 19, 135–155. [Google Scholar] [CrossRef]
- Janka, G.E.; Lehmberg, K. Hemophagocytic lymphohistiocytosis: Pathogenesis and treatment. Hematol. Am. Soc. Hematol. Educ. Program 2013, 2013, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Kleynberg, R.L.; Schiller, G.J. Secondary hemophagocytic lymphohistiocytosis in adults: An update on diagnosis and therapy. Clin. Adv. Hematol. Oncol. 2012, 10, 726–732. [Google Scholar] [PubMed]
- Morimoto, A.; Nakazawa, Y.; Ishii, E. Hemophagocytic lymphohistiocytosis: Pathogenesis, diagnosis, and management. Pediatr. Int. 2016, 58, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Wohlfarth, P.; Agis, H.; Gualdoni, G.A.; Weber, J.; Staudinger, T.; Schellongowski, P.; Robak, O. Interleukin 1 Receptor Antagonist Anakinra, Intravenous Immunoglobulin, and Corticosteroids in the Management of Critically Ill Adult Patients With Hemophagocytic Lymphohistiocytosis. J. Intensive Care Med. 2017, 0885066617711386. [Google Scholar] [CrossRef]
- Hayden, A.; Park, S.; Giustini, D.; Lee, A.Y.Y.; Chen, L.Y.C. Hemophagocytic syndromes (HPSs) including hemophagocytic lymphohistiocytosis (HLH) in adults: A systematic scoping review. Blood Rev. 2016, 30, 411–420. [Google Scholar] [CrossRef]
- Henter, J.-I.; Horne, A.; Aricó, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Batu, E.D.; Erden, A.; Seyhoğlu, E.; Kilic, L.; Büyükasık, Y.; Karadag, O.; Bilginer, Y.; Bilgen, S.A.; Akdogan, A.; Kiraz, S.; et al. Assessment of the HScore for reactive haemophagocytic syndrome in patients with rheumatic diseases. Scand. J. Rheumatol. 2017, 46, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Fardet, L.; Galicier, L.; Lambotte, O.; Marzac, C.; Aumont, C.; Chahwan, D.; Coppo, P.; Hejblum, G. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. (Hoboken N.J.) 2014, 66, 2613–2620. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Park, S.; Hayden, A.; Giustini, D.; Trinkaus, M.; Pudek, M.; Mattman, A.; Schneider, M.; Chen, L.Y.C. Clinical utility of soluble interleukin-2 receptor in hemophagocytic syndromes: A systematic scoping review. Ann. Hematol. 2017, 96, 1241–1251. [Google Scholar] [CrossRef]
- Grangé, S.; Buchonnet, G.; Besnier, E.; Artaud-Macari, E.; Beduneau, G.; Carpentier, D.; Dehay, J.; Girault, C.; Marchalot, A.; Guerrot, D.; et al. The Use of Ferritin to Identify Critically Ill Patients With Secondary Hemophagocytic Lymphohistiocytosis. Crit. Care Med. 2016, 44, e1045–e1053. [Google Scholar] [CrossRef]
- Wormsbecker, A.J.; Sweet, D.D.; Mann, S.L.; Wang, S.Y.; Pudek, M.R.; Chen, L.Y.C. Conditions associated with extreme hyperferritinaemia (>3000 μg/L) in adults. Intern. Med. J. 2015, 45, 828–833. [Google Scholar] [CrossRef]
- Schaer, D.J.; Schleiffenbaum, B.; Kurrer, M.; Imhof, A.; Bächli, E.; Fehr, J.; Moller, H.J.; Moestrup, S.K.; Schaffner, A. Soluble hemoglobin-haptoglobin scavenger receptor CD163 as a lineage-specific marker in the reactive hemophagocytic syndrome. Eur. J. Haematol. 2005, 74, 6–10. [Google Scholar] [CrossRef]
- Bleesing, J.; Prada, A.; Siegel, D.M.; Villanueva, J.; Olson, J.; Ilowite, N.T.; Brunner, H.I.; Griffin, T.; Graham, T.B.; Sherry, D.D.; et al. The diagnostic significance of soluble CD163 and soluble interleukin-2 receptor alpha-chain in macrophage activation syndrome and untreated new-onset systemic juvenile idiopathic arthritis. Arthritis Rheum. 2007, 56, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Machowicz, R.; Janka, G.; Wiktor-Jedrzejczak, W. Similar but not the same: Differential diagnosis of HLH and sepsis. Crit. Rev. Oncol. Hematol. 2017, 114, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Castillo, L.; Carcillo, J. Secondary hemophagocytic lymphohistiocytosis and severe sepsis/systemic inflammatory response syndrome/multiorgan dysfunction syndrome/macrophage activation syndrome share common intermediate phenotypes on a spectrum of inflammation. Pediatr. Crit. Care Med. 2009, 10, 387–392. [Google Scholar] [CrossRef]
- Beutel, G.; Wiesner, O.; Eder, M.; Hafer, C.; Schneider, A.S.; Kielstein, J.T.; Kühn, C.; Heim, A.; Ganzenmüller, T.; Kreipe, H.-H.; et al. Virus-associated hemophagocytic syndrome as a major contributor to death in patients with 2009 influenza A (H1N1) infection. Crit. Care 2011, 15, R80. [Google Scholar] [CrossRef] [PubMed]
- Rivière, S.; Galicier, L.; Coppo, P.; Marzac, C.; Aumont, C.; Lambotte, O.; Fardet, L. Reactive hemophagocytic syndrome in adults: A retrospective analysis of 162 patients. Am. J. Med. 2014, 127, 1118–1125. [Google Scholar] [CrossRef]
- Delavigne, K.; Bérard, E.; Bertoli, S.; Corre, J.; Duchayne, E.; Demur, C.; Mansat-De Mas, V.; Borel, C.; Picard, M.; Alvarez, M.; et al. Hemophagocytic syndrome in patients with acute myeloid leukemia undergoing intensive chemotherapy. Haematologica 2014, 99, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Weaver, L.K.; Behrens, E.M. Hyperinflammation, rather than hemophagocytosis, is the common link between macrophage activation syndrome and hemophagocytic lymphohistiocytosis. Curr. Opin. Rheumatol. 2014, 26, 562–569. [Google Scholar] [CrossRef]
- Ratzinger, F.; Schuardt, M.; Eichbichler, K.; Tsirkinidou, I.; Bauer, M.; Haslacher, H.; Mitteregger, D.; Binder, M.; Burgmann, H. Utility of Sepsis Biomarkers and the Infection Probability Score to Discriminate Sepsis and Systemic Inflammatory Response Syndrome in Standard Care Patients. Plos ONE 2013, 8, e82946. [Google Scholar] [CrossRef] [PubMed]
- Ratzinger, F.; Haslacher, H.; Stadlberger, M.; Schmidt, R.L.J.; Obermüller, M.; Schmetterer, K.G.; Perkmann, T.; Makristathis, A.; Marculescu, R.; Burgmann, H. 25(OH)D and 1,25(OH)D vitamin D fails to predict sepsis and mortality in a prospective cohort study. Sci. Rep. 2017, 7, 40646. [Google Scholar] [CrossRef]
- Ratzinger, F.; Haslacher, H.; Perkmann, T.; Pinzan, M.; Anner, P.; Makristathis, A.; Burgmann, H.; Heinze, G.; Dorffner, G. Machine learning for fast identification of bacteraemia in SIRS patients treated on standard care wards: A cohort study. Sci. Rep. 2018, 8, 12233. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [PubMed]
- Haslacher, H.; Gerner, M.; Hofer, P.; Jurkowitsch, A.; Hainfellner, J.; Kain, R.; Wagner, O.F.; Perkmann, T. Usage Data and Scientific Impact of the Prospectively Established Fluid Bioresources at the Hospital-Based MedUni Wien Biobank. Biopreserv. Biobank. 2018, 16, 477–482. [Google Scholar] [CrossRef]
- Lausen, B.; Schumacher, M. Maximally Selected Rank Statistics. Biometrics 1992, 48, 73–85. [Google Scholar] [CrossRef]
- Egües Dubuc, C.; Aldasoro Cáceres, V.; Uriarte Ecenarro, M.; Errazquin Aguirre, N.; Hernando Rubio, I.; Meneses Villalba, C.F.; Uriarte Itzazelaia, E.; Cancio Fanlo, J.J.; Maiz Alonso, O.; Belzunegui Otano, J.M. Secondary macrophage activation syndrome due to autoimmune, hematologic, infectious and oncologic diseases. Thirteen case series and review of the literature. Reum. Clin 2015, 11, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Machaczka, M.; Vaktnäs, J.; Klimkowska, M.; Hägglund, H. Malignancy-associated hemophagocytic lymphohistiocytosis in adults: A retrospective population-based analysis from a single center. Leuk. Lymphoma 2011, 52, 613–619. [Google Scholar] [CrossRef]
- Shakoory, B.; Carcillo, J.A.; Chatham, W.W.; Amdur, R.L.; Zhao, H.; Dinarello, C.A.; Cron, R.Q.; Opal, S.M. Interleukin-1 Receptor Blockade Is Associated With Reduced Mortality in Sepsis Patients With Features of Macrophage Activation Syndrome: Reanalysis of a Prior Phase Iii Trial. Crit. Care Med. 2016, 44, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Kyriazopoulou, E.; Leventogiannis, K.; Norrby-Teglund, A.; Dimopoulos, G.; Pantazi, A.; Orfanos, S.E.; Rovina, N.; Tsangaris, I.; Gkavogianni, T.; Botsa, E.; et al. Macrophage activation-like syndrome: An immunological entity associated with rapid progression to death in sepsis. BMC Med. 2017, 15, 172. [Google Scholar] [CrossRef]
- Rosário, C.; Zandman-Goddard, G.; Meyron-Holtz, E.G.; D’Cruz, D.P.; Shoenfeld, Y. The hyperferritinemic syndrome: Macrophage activation syndrome, Still’s disease, septic shock and catastrophic antiphospholipid syndrome. BMC Med 2013, 11, 185. [Google Scholar] [CrossRef]
- Canna, S.W.; Behrens, E.M. Not all Hemophagocytes are Created Equally: Appreciating the Heterogeneity of the Hemophagocytic Syndromes. Curr. Opin. Rheumatol. 2012, 24, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Rouphael, N.G.; Talati, N.J.; Vaughan, C.; Cunningham, K.; Moreira, R.; Gould, C. Infections associated with haemophagocytic syndrome. Lancet Infect. Dis. 2007, 7, 814–822. [Google Scholar] [CrossRef]
- Lerolle, N.; Laanani, M.; Rivière, S.; Galicier, L.; Coppo, P.; Meynard, J.-L.; Molina, J.-M.; Azoulay, E.; Aumont, C.; Marzac, C.; et al. Diversity and combinations of infectious agents in 38 adults with an infection-triggered reactive haemophagocytic syndrome: a multicenter study. Clin. Microbiol. Infect. 2016, 22, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Saeed, H.; Woods, R.R.; Lester, J.; Herzig, R.; Gul, Z.; Monohan, G. Evaluating the optimal serum ferritin level to identify hemophagocytic lymphohistiocytosis in the critical care setting. Int. J. Hematol. 2015, 102, 195–199. [Google Scholar] [CrossRef]
- Emmenegger, U.; Reimers, A.; Frey, U.; Fux, C.; Bihl, F.; Semela, D.; Cottagnoud, P.; Cerny, A.; Spaeth, P.J.; Neftel, K.A. Reactive macrophage activation syndrome: A simple screening strategy and its potential in early treatment initiation. Swiss Med. Wkly. 2002, 132, 230–236. [Google Scholar] [PubMed]
- Emmenegger, U.; Frey, U.; Reimers, A.; Fux, C.; Semela, D.; Cottagnoud, P.; Spaeth, P.J.; Neftel, K.A. Hyperferritinemia as indicator for intravenous immunoglobulin treatment in reactive macrophage activation syndromes. Am. J. Hematol. 2001, 68, 4–10. [Google Scholar] [CrossRef]
- Schram, A.M.; Campigotto, F.; Mullally, A.; Fogerty, A.; Massarotti, E.; Neuberg, D.; Berliner, N. Marked hyperferritinemia does not predict for HLH in the adult population. Blood 2015, 125, 1548–1552. [Google Scholar] [CrossRef]
- Hayden, A.; Lin, M.; Park, S.; Pudek, M.; Schneider, M.; Jordan, M.B.; Mattman, A.; Chen, L.Y.C. Soluble interleukin-2 receptor is a sensitive diagnostic test in adult HLH. Blood Adv. 2017, 1, 2529–2534. [Google Scholar] [CrossRef]
- Goel, S.; Polski, J.M.; Imran, H. Sensitivity and specificity of bone marrow hemophagocytosis in hemophagocytic lymphohistiocytosis. Ann. Clin. Lab. Sci. 2012, 42, 21–25. [Google Scholar] [PubMed]
- Ho, C.; Yao, X.; Tian, L.; Li, F.-Y.; Podoltsev, N.; Xu, M.L. Marrow assessment for hemophagocytic lymphohistiocytosis demonstrates poor correlation with disease probability. Am. J. Clin. Pathol. 2014, 141, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Park, S.; Jang, J.H.; Kim, K.; Kim, H.-J.; Kim, S.-H.; Kang, C.-I.; Chung, D.R.; Peck, K.R.; Lee, J.; et al. Clinical significance of bone marrow hemophagocytosis in adult patients with malignancy and non-malignancy-induced hemophagocytic lymphohistiocytosis. Ann. Hematol. 2016, 95, 325–335. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Feature | SIRS = 2 (n = 181) | SIRS = 3 (n = 201) | SIRS = 4 (n = 69) | p–Value |
|---|---|---|---|---|
| Age | 57.9 (44.4–69.0) | 58.6 (42.5–69.0) | 56.1 (40.7–69.9) | 0.946 |
| Male:Female | 42%:58% | 45%:55% | 44%:56% | 0.806 |
| Immuno-suppression | 28 (16%) | 27 (13%) | 10 (15%) | 0.857 |
| Neoplasm | 63 (35%) | 84 (42%) | 30 (44%) | 0.275 |
| sCD25 (IU/mL) | 47.5 (26.7–93.3) | 54.7 (28.2–108.9) | 62.2 (36.4–146.1) | 0.091 |
| sCD163 (pg/mL) | 610.9 (381.7–1022.5) | 572.8 (403.3–1046.5) | 631.5 (475.5–1036.3) | 0.404 |
| HLH-2004 criteria | 1.0 (1.0–2.0) | 2.0 (1.0–3.0) | 2.0 (1.0–3.0) | <0.001 * |
| Hscore | 63.0 (33.0–95.0) | 67.0 (33.0–101.0) | 75.0 (44.0–112.0) | 0.212 |
| ID | 38 | 288 | 573 | 726 | 87 | |
|---|---|---|---|---|---|---|
| Hscore | 223 | 205 | 203 | 178 | 169 | |
| HLH Probability* | >96% | >88% | >88% | >70% | ~50% | |
| HLH-2004 Criteria | 4 | 4 | 2 | 3 | 3 | |
| Temp (°C) | 38.5 | 40.2 | 40 | 38.5 | 38.7 | |
| Cytopenia | Hb (g/dL) | 6.8 | 10.4 | 9.1 | 9.2 | 9.8 |
| Platelets (G/L) | 34 | 105 | 166 | 110 | 8 | |
| WBC (G/L) | 0.08 | 13.79 | 6.65 | 2.47 | 15.75 | |
| No of Cytopenia | 3 | 1 | 1 | 1 | 1 | |
| Spleno/Hepatomegaly | HM | SM | HM | n.a. | SM | |
| Immunosuppression | no | no | yes | yes | no | |
| Triglycerides (mg/dL) | 387 | 360 | 252 | 285 | 184 | |
| Fibrinogen (mg/dL) | 705 | 359 | 687 | 227 | 512 | |
| Ferritin (μg/L) | 8577 | 6053 | 12582 | 903 | 7950 | |
| ASAT/GOT (IU/L) | 80 | 190 | 81 | 640 | 127 | |
| Hemophagocytosis | no | n.a. | n.a. | n.a. | n.a. | |
| sCD25 (IU/mL) | 147.4 | 410.8 | 518.0 | 101.1 | 749.9 | |
| sCD163 (pg/mL) | 661.92 | >1500 | 1348.2 | >1500 | >1500 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gualdoni, G.A.; Hofmann, G.A.; Wohlfarth, P.; Winkler, H.-M.; Winkler, S.; Haslacher, H.; Thalhammer, R.; Makristathis, A.; Ratzinger, F.; Burgmann, H. Prevalence and Outcome of Secondary Hemophagocytic Lymphohistiocytosis Among SIRS Patients: Results from a Prospective Cohort Study. J. Clin. Med. 2019, 8, 541. https://doi.org/10.3390/jcm8040541
Gualdoni GA, Hofmann GA, Wohlfarth P, Winkler H-M, Winkler S, Haslacher H, Thalhammer R, Makristathis A, Ratzinger F, Burgmann H. Prevalence and Outcome of Secondary Hemophagocytic Lymphohistiocytosis Among SIRS Patients: Results from a Prospective Cohort Study. Journal of Clinical Medicine. 2019; 8(4):541. https://doi.org/10.3390/jcm8040541
Chicago/Turabian StyleGualdoni, Guido A., Georg A. Hofmann, Philipp Wohlfarth, Heide-Maria Winkler, Stefan Winkler, Helmuth Haslacher, Renate Thalhammer, Athanasios Makristathis, Franz Ratzinger, and Heinz Burgmann. 2019. "Prevalence and Outcome of Secondary Hemophagocytic Lymphohistiocytosis Among SIRS Patients: Results from a Prospective Cohort Study" Journal of Clinical Medicine 8, no. 4: 541. https://doi.org/10.3390/jcm8040541
APA StyleGualdoni, G. A., Hofmann, G. A., Wohlfarth, P., Winkler, H.-M., Winkler, S., Haslacher, H., Thalhammer, R., Makristathis, A., Ratzinger, F., & Burgmann, H. (2019). Prevalence and Outcome of Secondary Hemophagocytic Lymphohistiocytosis Among SIRS Patients: Results from a Prospective Cohort Study. Journal of Clinical Medicine, 8(4), 541. https://doi.org/10.3390/jcm8040541