Anesthetic Efficacy of Dexmedetomidine versus Midazolam When Combined with Remifentanil for Percutaneous Transluminal Angioplasty in Patients with Peripheral Artery Disease

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
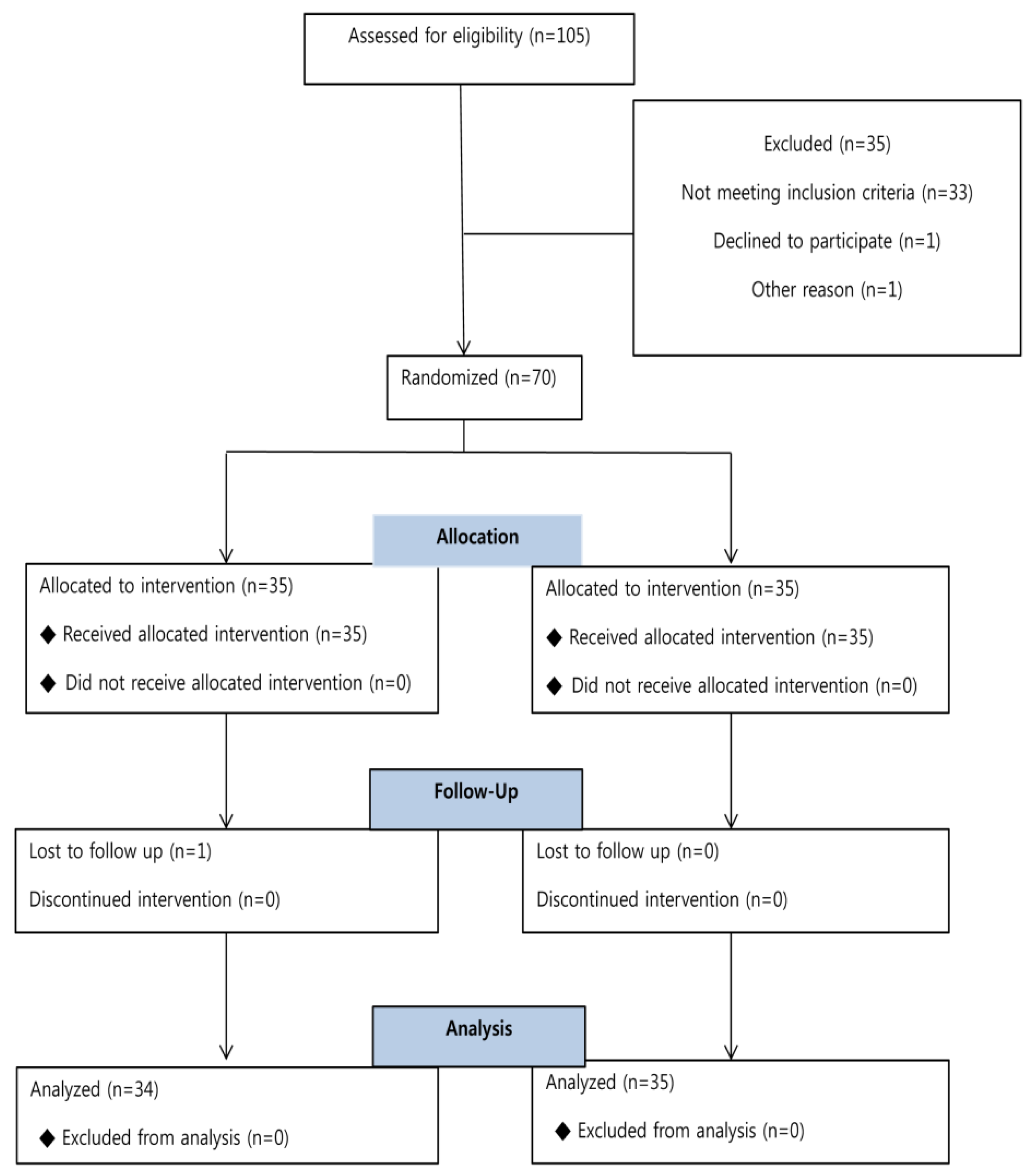
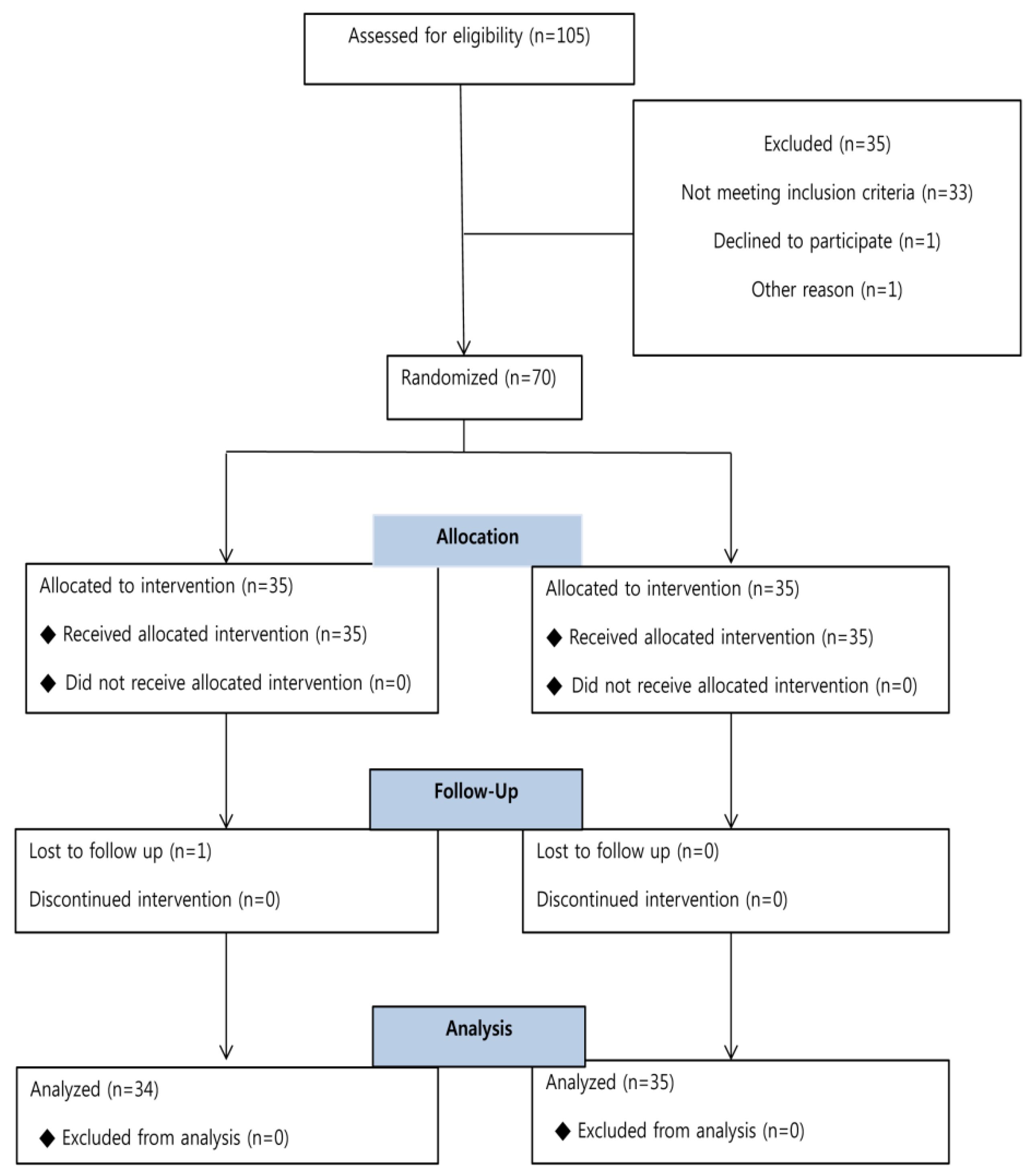
2.1. Study Population
2.2. Anesthetic and Procedural Management
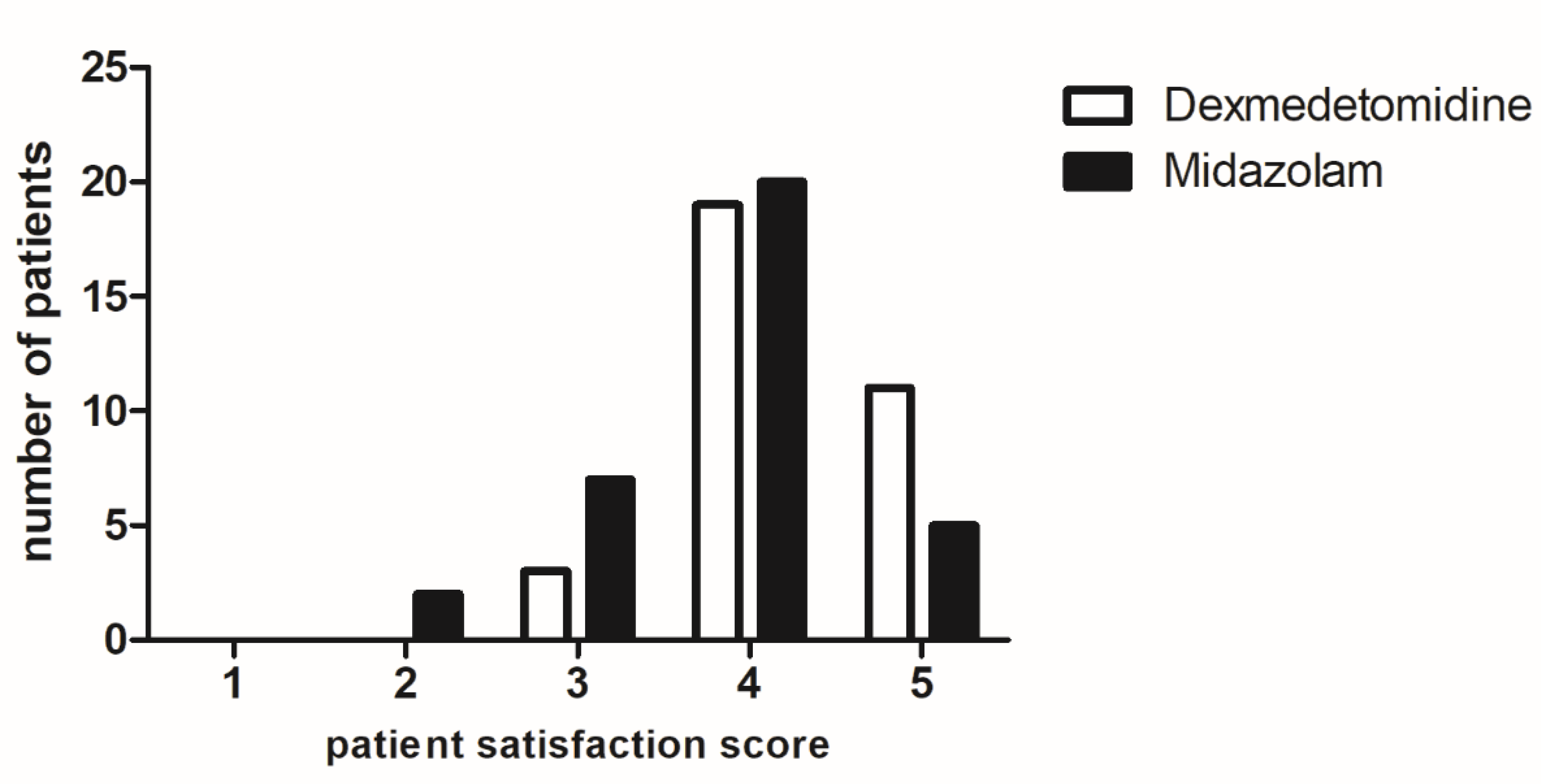
2.3. Primary Endpoint and Assessment
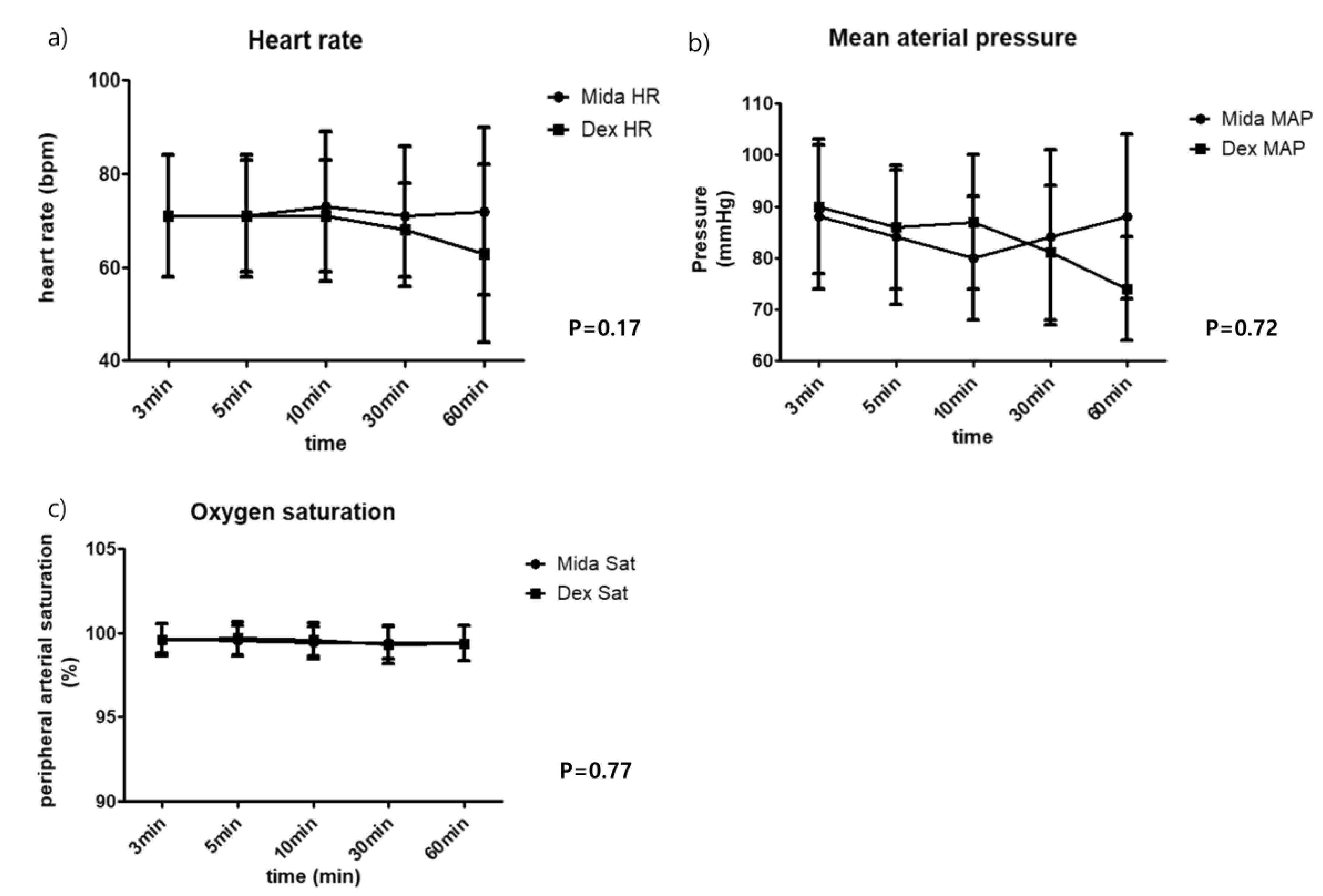
2.4. Secondary Endpoints and Assessments
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Conflicts of Interest
References
- Criqui, M.H.; Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef] [PubMed]
- Marcus, A.J.; Lotzof, K.; Kamath, B.S.; Shanthakumar, R.E.; Munir, N.; Loh, A.; Bird, R.; Howard, A. A new approach: Regional nerve blockade for angioplasty of the lower limb. Cardiovasc. Interv. Radiol. 2006, 29, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.A.; Ackermann, A.M.; Augoustides, J.G.T.; Ender, J.; Gutsche, J.T.; Giri, J.; Vallabhajosyula, P.; Desai, N.D.; Kostibas, M.; Brady, M.B.; et al. Anesthetic evolution in transcatheter aortic valve replacement: Expert perspectives from high-volume academic centers in europe and the united states. J. Cardiothorac. Vasc. Anesth. 2017, 31, 777–790. [Google Scholar] [CrossRef]
- Cho, J.S.; Shim, J.K.; Na, S.; Park, I.; Kwak, Y.L. Improved sedation with dexmedetomidine-remifentanil compared with midazolam-remifentanil during catheter ablation of atrial fibrillation: A randomized, controlled trial. Europace 2014, 16, 1000–1006. [Google Scholar] [CrossRef]
- Boom, M.; Niesters, M.; Sarton, E.; Aarts, L.; Smith, T.W.; Dahan, A. Non-analgesic effects of opioids: Opioid-induced respiratory depression. Curr. Pharm. Des. 2012, 18, 5994–6004. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.C.S.; McCarthy, D.; Li, J.; Palczewski, K.; Yuan, S. Designing safer analgesics via μ-opioid receptor pathways. Trends Pharmacol. Sci. 2017, 38, 1016–1037. [Google Scholar] [CrossRef] [PubMed]
- Trentman, T.L.; Fassett, S.L.; Mueller, J.T.; Altemose, G.T. Airway interventions in the cardiac electrophysiology laboratory: A retrospective review. J. Cardiothorac. Vasc. Anesth. 2009, 23, 841–845. [Google Scholar] [CrossRef]
- Fowkes, F.G.; Aboyans, V.; Fowkes, F.J.; McDermott, M.M.; Sampson, U.K.; Criqui, M.H. Peripheral artery disease: Epidemiology and global perspectives. Nat. Rev. Cardiol. 2017, 14, 156–170. [Google Scholar] [CrossRef]
- Rokyta, R.; Yamamotova, A.; Sulc, R.; Trefil, L.; Racek, J.; Treska, V. Assessment of biochemical markers in patients with pain of vascular origin. Clin. Exp. Med. 2008, 8, 199–206. [Google Scholar] [CrossRef]
- Keating, G.M. Dexmedetomidine: A review of its use for sedation in the intensive care setting. Drugs 2015, 75, 1119–1130. [Google Scholar] [CrossRef]
- Fang, B.; Li, X.Q.; Bi, B.; Tan, W.F.; Liu, G.; Zhang, Y.; Ma, H. Dexmedetomidine attenuates blood-spinal cord barrier disruption induced by spinal cord ischemia reperfusion injury in rats. Cell. Physiol. Biochem. 2015, 36, 373–383. [Google Scholar] [CrossRef]
- Dong, X.; Xing, Q.; Li, Y.; Han, X.; Sun, L. Dexmedetomidine protects against ischemia-reperfusion injury in rat skeletal muscle. J. Surg. Res. 2014, 186, 240–245. [Google Scholar] [CrossRef]
- Consales, G.; Chelazzi, C.; Rinaldi, S.; De Gaudio, A.R. Bispectral index compared to ramsay score for sedation monitoring in intensive care units. Minerva Anestesiol. 2006, 72, 329–336. [Google Scholar]
- Subherwal, S.; Patel, M.R.; Kober, L.; Peterson, E.D.; Bhatt, D.L.; Gislason, G.H.; Olsen, A.M.; Jones, W.S.; Torp-Pedersen, C.; Fosbol, E.L. Peripheral artery disease is a coronary heart disease risk equivalent among both men and women: Results from a nationwide study. Eur. J. Prev. Cardiol. 2015, 22, 317–325. [Google Scholar] [CrossRef]
- Alberts, M.J.; Bhatt, D.L.; Mas, J.L.; Ohman, E.M.; Hirsch, A.T.; Rother, J.; Salette, G.; Goto, S.; Smith, S.C., Jr.; Liau, C.S.; et al. Three-year follow-up and event rates in the international reduction of atherothrombosis for continued health registry. Eur. Heart J. 2009, 30, 2318–2326. [Google Scholar] [CrossRef]
- Egan, T.D.; Lemmens, H.J.; Fiset, P.; Hermann, D.J.; Muir, K.T.; Stanski, D.R.; Shafer, S.L. The pharmacokinetics of the new short-acting opioid remifentanil (gi87084b) in healthy adult male volunteers. Anesthesiology 1993, 79, 881–892. [Google Scholar] [CrossRef]
- Takechi, K.; Carstens, M.I.; Klein, A.H.; Carstens, E. The antinociceptive and antihyperalgesic effects of topical propofol on dorsal horn neurons in the rat. Anesth. Analg. 2013, 116, 932–938. [Google Scholar] [CrossRef]
- Lang, P.M.; Schober, G.M.; Rolke, R.; Wagner, S.; Hilge, R.; Offenbacher, M.; Treede, R.D.; Hoffmann, U.; Irnich, D. Sensory neuropathy and signs of central sensitization in patients with peripheral arterial disease. Pain 2006, 124, 190–200. [Google Scholar] [CrossRef]
- Rabl, H.; Khoschsorur, G.; Colombo, T.; Tatzber, F.; Esterbauer, H. Human plasma lipid peroxide levels show a strong transient increase after successful revascularization operations. Free Radic. Biol. Med. 1992, 13, 281–288. [Google Scholar] [CrossRef]
- Farghaly, H.S.M.; Mahmoud, A.M.; Abdel-Sater, K.A. Effect of dexmedetomidine and cold stress in a rat model of neuropathic pain: Role of interleukin-6 and tumor necrosis factor-α. Eur. J. Pharmacol. 2016, 776, 139–145. [Google Scholar] [CrossRef]
- Huupponen, E.; Maksimow, A.; Lapinlampi, P.; Sarkela, M.; Saastamoinen, A.; Snapir, A.; Scheinin, H.; Scheinin, M.; Merilainen, P.; Himanen, S.L.; et al. Electroencephalogram spindle activity during dexmedetomidine sedation and physiological sleep. Acta Anaesthesiol. Scand. 2008, 52, 289–294. [Google Scholar] [CrossRef]
- Chu, L.F.; Angst, M.S.; Clark, D. Opioid-induced hyperalgesia in humans: Molecular mechanisms and clinical considerations. Clin. J. Pain 2008, 24, 479–496. [Google Scholar] [CrossRef]
- Zheng, Y.; Cui, S.; Liu, Y.; Zhang, J.; Zhang, W.; Zhang, J.; Gu, X.; Ma, Z. Dexmedetomidine prevents remifentanil-induced postoperative hyperalgesia and decreases spinal tyrosine phosphorylation of n-methyl-d-aspartate receptor 2b subunit. Brain Res. Bull. 2012, 87, 427–431. [Google Scholar] [CrossRef]
- Bloor, B.C.; Ward, D.S.; Belleville, J.P.; Maze, M. Effects of intravenous dexmedetomidine in humans. Ii. Hemodynamic changes. Anesthesiology 1992, 77, 1134–1142. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Midazolam (n = 35) | Dexmedetomidine (n = 34) | |
|---|---|---|
| Age (years) | 64.7 ± 12.5 | 64.1 ± 11.5 |
| Sex (M/F) | 34/1 | 27/7 |
| Body surface area (m2) | 1.75 ± 0.16 | 1.71 ± 1.9 |
| Hypertension | 25 (71.4) | 20 (58.8) |
| Diabetes mellitus | 19 (54.3) | 16 (47.1) |
| Coronary artery disease | 13 (37.1) | 11 (32.4) |
| End-stage renal disease | 1 (2.9) | 2 (5.9) |
| Cerebrovascular accident | 3 (8.6) | 5 (14.7) |
| Medications | ||
| Aspirin | 30 (85.7) | 23 (67.6) |
| Thienopyridine | 26 (74.3) | 21 (61.8) |
| Cilostazol | 8 (22.9) | 3 (8.8) |
| Warfarin | 3 (8.6) | 1 (2.9) |
| Statin | 20 (57.1) | 19 (55.9) |
| Beta-blocker | 3 (8.6) | 3 (8.8) |
| Rutherford category | ||
| 1 | 1 (2.9) | 1 (2.9) |
| 2 | 4 (11.4) | 5 (14.7) |
| 3 | 18 (51.4) | 17 (50.0) |
| 4 | 5 (14.3) | 8 (23.5) |
| 5 | 4 (11.4) | 1 (2.9) |
| 6 | 3 (8.6) | 2 (5.9) |
| Current smoker, n (%) | 8 (22.9) | 6 (20.0) |
| Procedure time (min) | 59.7 ± 37.8 | 53.7 ± 31.4 |
| Intraoperative medication | ||
| Remifentanil (µg/kg/h) | 0.72 [0.50, 1.31] | 0.72 [0.49, 1.06] |
| Midazolam (µg/kg/h) | 20.51 [13.79, 44.44] | 0 [0, 0] |
| Dexmedetomidine (µg/kg/h) | 0 [0, 0] | 51.00 [37.87, 74.40] |
| Midazolam (n = 35) | Dexmedetomidine (n = 34) | p-Value | |
|---|---|---|---|
| Primary endpoint | |||
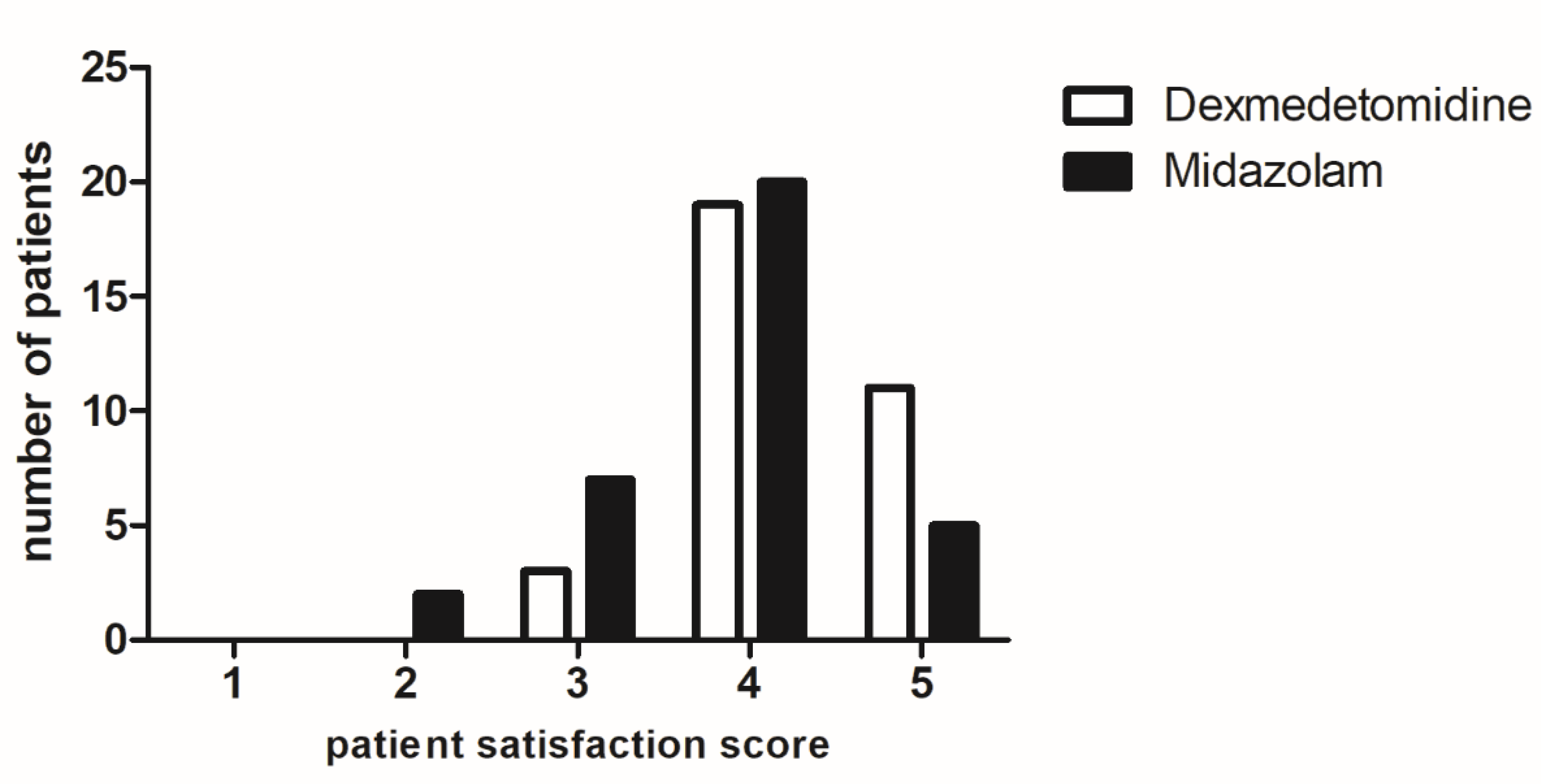
| Patients’ satisfaction | 4.0 [3.0,4.0] | 4.0 [4.0,5.0] | 0.021 * |
| Secondary endpoints | |||
| Interventionists’ satisfaction | 4.0 [4.0,4.5] | 4.0 [3.5,4.0] | 0.860 |
| Pain scores | |||
| Baseline | 2 [1,3] | 2 [2,4] | 0.734 |
| Procedural | 3 [0,4] | 0.5 [0,4] | 0.192 |
| Post-procedural 24 h | 0 [0,3] | 0 [0,1] | 0.213 |
| Pain score ≥3 | 10 (28.6) | 2 (5.9) | 0.013 * |
| Rescue analgesics | 13 (37.1) | 13 (38.2) | 0.925 |
| Rescue morphine dose (mg) | 10.0 [5.5,18.2] | 6.6 [5.0,10.0] | 0.062 |
| Adverse events | |||
| Bradycardia | 0 | 0 | 1.000 |
| Hypotension | 0 | 5 (14.7%) | 0.025 * |
| Hypoxia | 1 (2.9%) | 0 | 1.000 |
| Nausea | 0 | 1 (2.9%) | 0.310 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-H.; Soh, S.; Kwak, Y.-L.; Kim, B.; Choi, S.; Shim, J.-K. Anesthetic Efficacy of Dexmedetomidine versus Midazolam When Combined with Remifentanil for Percutaneous Transluminal Angioplasty in Patients with Peripheral Artery Disease. J. Clin. Med. 2019, 8, 472. https://doi.org/10.3390/jcm8040472
Park J-H, Soh S, Kwak Y-L, Kim B, Choi S, Shim J-K. Anesthetic Efficacy of Dexmedetomidine versus Midazolam When Combined with Remifentanil for Percutaneous Transluminal Angioplasty in Patients with Peripheral Artery Disease. Journal of Clinical Medicine. 2019; 8(4):472. https://doi.org/10.3390/jcm8040472
Chicago/Turabian StylePark, Ji-Hyoung, Sarah Soh, Young-Lan Kwak, Bosung Kim, Sohyun Choi, and Jae-Kwang Shim. 2019. "Anesthetic Efficacy of Dexmedetomidine versus Midazolam When Combined with Remifentanil for Percutaneous Transluminal Angioplasty in Patients with Peripheral Artery Disease" Journal of Clinical Medicine 8, no. 4: 472. https://doi.org/10.3390/jcm8040472
APA StylePark, J.-H., Soh, S., Kwak, Y.-L., Kim, B., Choi, S., & Shim, J.-K. (2019). Anesthetic Efficacy of Dexmedetomidine versus Midazolam When Combined with Remifentanil for Percutaneous Transluminal Angioplasty in Patients with Peripheral Artery Disease. Journal of Clinical Medicine, 8(4), 472. https://doi.org/10.3390/jcm8040472