Evaluation of the Association between Menstrual Cycle Irregularity and Dental Pain or Chewing Discomfort in Women before Menopause



Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Anthropometric Measurement and Definition of Variables
2.3. Oral Health Behaviors and Definition of Number of Natural Teeth
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van Anders, S.M.; Watson, N.V. Menstrual cycle irregularities are associated with testosterone levels in healthy premenopausal women. Am. J. Hum. Biol. 2006, 18, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Ko, Y.; Park, Y.G.; Park, J.B. Associations Between the Periodontal Disease in Women Before Menopause and Menstrual Cycle Irregularity: The 2010–2012 Korea National Health and Nutrition Examination Survey. Medicine 2016, 95, e2791. [Google Scholar] [CrossRef] [PubMed]
- Jukic, A.M.; Weinberg, C.R.; Wilcox, A.J.; McConnaughey, D.R.; Hornsby, P.; Baird, D.D. Accuracy of reporting of menstrual cycle length. Am. J. Epidemiol. 2008, 167, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Solomon, C.G.; Hu, F.B.; Dunaif, A.; Rich-Edwards, J.; Willett, W.C.; Hunter, D.J.; Colditz, G.A.; Speizer, F.E.; Manson, J.E. Long or highly irregular menstrual cycles as a marker for risk of type 2 diabetes mellitus. JAMA 2001, 286, 2421–2426. [Google Scholar] [CrossRef] [PubMed]
- Roumain, J.; Charles, M.A.; de Courten, M.P.; Hanson, R.L.; Brodie, T.D.; Pettitt, D.J.; Knowler, W.C. The relationship of menstrual irregularity to type 2 diabetes in Pima Indian women. Diabetes Care 1998, 21, 346–349. [Google Scholar] [CrossRef]
- Rostami Dovom, M.; Ramezani Tehrani, F.; Djalalinia, S.; Cheraghi, L.; Behboudi Gandavani, S.; Azizi, F. Menstrual Cycle Irregularity and Metabolic Disorders: A Population-Based Prospective Study. PLoS ONE 2016, 11, e0168402. [Google Scholar] [CrossRef]
- Machtei, E.E.; Mahler, D.; Sanduri, H.; Peled, M. The effect of menstrual cycle on periodontal health. J. Periodontol. 2004, 75, 408–412. [Google Scholar] [CrossRef]
- Koreeda, N.; Iwano, Y.; Kishida, M.; Otsuka, A.; Kawamoto, A.; Sugano, N.; Ito, K. Periodic exacerbation of gingival inflammation during the menstrual cycle. J. Oral Sci. 2005, 47, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Korea Centers for Disease Control & Prevention. Available online: https://knhanes.cdc.go.kr (accessed on 25 March 2016).
- Agarwal, D.P. Cardioprotective effects of light-moderate consumption of alcohol: A review of putative mechanisms. Alcohol Alcohol. 2002, 37, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.Y.; Yang, Y.J.; Kim, B.S.; Kang, J.H. Validity and reliability of Korean version of International Physical Activity Questionnaire (IPAQ) short form. J. Korean Acad. Fam. Med. 2007, 28, 532–541. [Google Scholar]
- Chun, Y.H.; Kim, H.R.; Han, K.; Park, Y.G.; Song, H.J.; Na, K.S. Total cholesterol and lipoprotein composition are associated with dry eye disease in Korean women. Lipids Health Dis. 2013, 12, 84. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, D.H.; Lim, K.S.; Ko, B.J.; Han, B.D.; Nam, G.E.; Park, Y.G.; Han, K.D.; Kim, J.H.; Cho, K.H. Oral health behaviors and metabolic syndrome: The 2008-2010 Korean National Health and Nutrition Examination Survey. Clin. Oral Investig. 2013. [Google Scholar] [CrossRef]
- Chang, P.J.; Chen, P.C.; Hsieh, C.J.; Chiu, L.T. Risk factors on the menstrual cycle of healthy Taiwanese college nursing students. Aust. N. Z. J. Obstet. Gynaecol. 2009, 49, 689–694. [Google Scholar] [CrossRef]
- Kollipaka, R.; Arounassalame, B.; Lakshminarayanan, S. Does psychosocial stress influence menstrual abnormalities in medical students? J. Obstet. Gynaecol. 2013, 33, 489–493. [Google Scholar] [CrossRef]
- Nagma, S.; Kapoor, G.; Bharti, R.; Batra, A.; Batra, A.; Aggarwal, A.; Sablok, A. To evaluate the effect of perceived stress on menstrual function. J. Clin. Diagn. Res. 2015, 9, Qc01. [Google Scholar] [CrossRef] [PubMed]
- Amarasena, N.; Kapellas, K. Psychological distress and self-rated oral health among a convenience sample of Indigenous Australians. J. Public Health Dent. 2015, 75, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Young, E.A.; Midgley, A.R.; Carlson, N.E.; Brown, M.B. Alteration in the hypothalamic-pituitary-ovarian axis in depressed women. Arch. Gen. Psychiatry 2000, 57, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Kyrou, I.; Tsigos, C. Chronic stress, visceral obesity and gonadal dysfunction. Horm. (Athens) 2008, 7, 287–293. [Google Scholar] [CrossRef]
- Ozcaka, O.; Bicakci, N.; Kose, T. Effect of the menstrual cycle on pain experience associated with periodontal therapy: Randomized, pilot study. J. Clin. Periodontol. 2005, 32, 1170–1174. [Google Scholar] [CrossRef]
- Mustaqeem, M.; Sadullah, S.; Waqar, W.; Farooq, M.Z.; Khan, A.; Fraz, T.R. Obesity with irregular menstrual cycle in young girls. Mymensingh Med. J. 2015, 24, 161–167. [Google Scholar]
- Nascimento, G.G.; Leite, F.R. Is there a relationship between obesity and tooth loss and edentulism? A systematic review and meta-analysis. Obes. Rev. 2016. [Google Scholar] [CrossRef]
- Ferraz, E.G.; Silva, L.R.; Sarmento, V.A.; de Jesus Campos, E.; de Oliveira, T.F.; Magalhaes, J.C.; Paraguassu, G.M.; Boa-Sorte, N. Comparison of two visual methods for detecting caries among obese and non-obese children. Acta Odontol. Scand. 2016, 405–410. [Google Scholar] [CrossRef]
- Alswat, K.; Mohamed, W.S.; Wahab, M.A.; Aboelil, A.A. The Association Between Body Mass Index and Dental Caries: Cross-Sectional Study. J. Clin. Med. Res. 2016, 8, 147–152. [Google Scholar] [CrossRef]
- Consolacao Soares, M.E.; Ramos-Jorge, M.L.; de Alencar, B.M.; Marques, L.S.; Pereira, L.J.; Ramos-Jorge, J. Factors associated with masticatory performance among preschool children. Clin. Oral Investig. 2016. [Google Scholar] [CrossRef]
- Labrie, F. DHEA, important source of sex steroids in men and even more in women. Prog. Brain Res. 2010, 182, 97–148. [Google Scholar]
- Labrie, F.; Belanger, A.; Luu-The, V.; Labrie, C.; Simard, J.; Cusan, L.; Gomez, J.L.; Candas, B. DHEA and the intracrine formation of androgens and estrogens in peripheral target tissues: Its role during aging. Steroids 1998, 63, 322–328. [Google Scholar] [CrossRef]
- Glueck, C.J.; McMahon, R.E.; Bouquot, J.E.; Triplett, D. Exogenous estrogen may exacerbate thrombophilia, impair bone healing and contribute to development of chronic facial pain. Cranio 1998, 16, 143–153. [Google Scholar] [CrossRef]
- Kim, Y.S.; Kim, J.H. Body mass index and oral health status in Korean adults: The Fifth Korea National Health and Nutrition Examination Survey. Int. J. Dent. Hyg. 2016. [Google Scholar] [CrossRef]
- Cao, X.; Wang, D.; Zhou, J.; Yuan, H.; Chen, Z. The relationship between dental caries and metabolic syndrome among 13,998 middle-aged urban Chinese. J. Diabetes 2016. [Google Scholar] [CrossRef]
- Cobb, K.L.; Bachrach, L.K.; Greendale, G.; Marcus, R.; Neer, R.M.; Nieves, J.; Sowers, M.F.; Brown, B.W., Jr.; Gopalakrishnan, G.; Luetters, C.; et al. Disordered eating, menstrual irregularity, and bone mineral density in female runners. Med. Sci. Sports Exerc. 2003, 35, 711–719. [Google Scholar] [CrossRef]
- Pedersen, A.B.; Bartholomew, M.J.; Dolence, L.A.; Aljadir, L.P.; Netteburg, K.L.; Lloyd, T. Menstrual differences due to vegetarian and nonvegetarian diets. Am. J. Clin. Nutr. 1991, 53, 879–885. [Google Scholar] [CrossRef]
- Jarvelaid, M. The effect of gynecologic age, body mass index and psychosocial environment on menstrual regularity among teenaged females. Acta Obstet. Gynecol. Scand. 2005, 84, 645–649. [Google Scholar] [CrossRef]
- Wei, S.; Schmidt, M.D.; Dwyer, T.; Norman, R.J.; Venn, A.J. Obesity and menstrual irregularity: Associations with SHBG, testosterone, and insulin. Obesity 2009, 17, 1070–1076. [Google Scholar] [CrossRef]
- Bean, J.A.; Leeper, J.D.; Wallace, R.B.; Sherman, B.M.; Jagger, H. Variations in the reporting of menstrual histories. Am. J. Epidemiol. 1979, 109, 181–185. [Google Scholar] [CrossRef]
- Small, C.M.; Manatunga, A.K.; Marcus, M. Validity of self-reported menstrual cycle length. Ann. Epidemiol. 2007, 17, 163–170. [Google Scholar] [CrossRef]
- Han, K.; Ko, Y.; Park, Y.G.; Park, J.B. Associations between the number of natural teeth in postmenopausal women and duration of lactation: The 2010–2012 Korea National Health and Nutrition Examination Survey. Maturitas 2016, 85, 73–78. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Menstrual Cycle Irregularity | |||
|---|---|---|---|
| No | Yes | P-Value * | |
| Unweighted n | 3940 | 655 | |
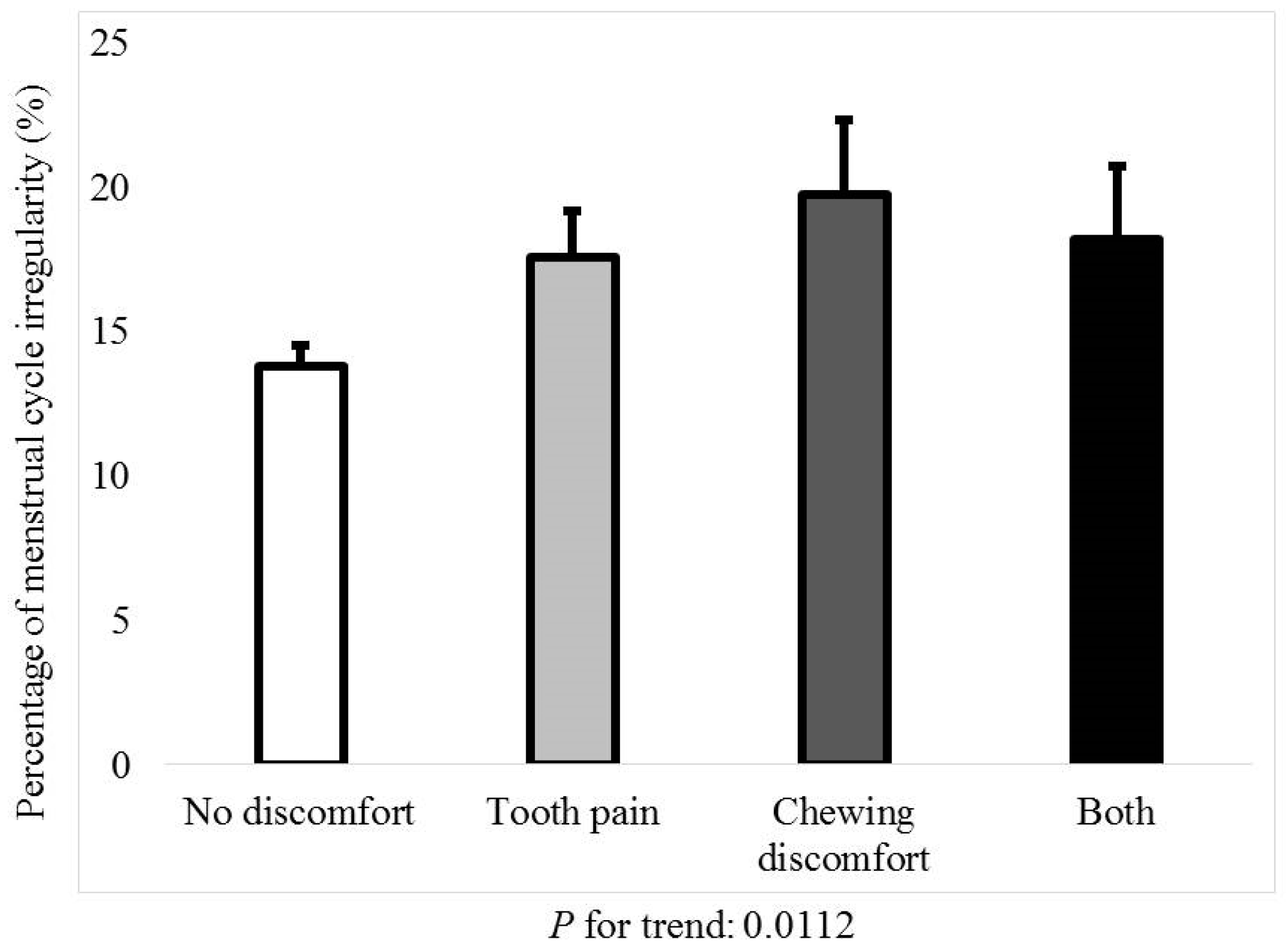
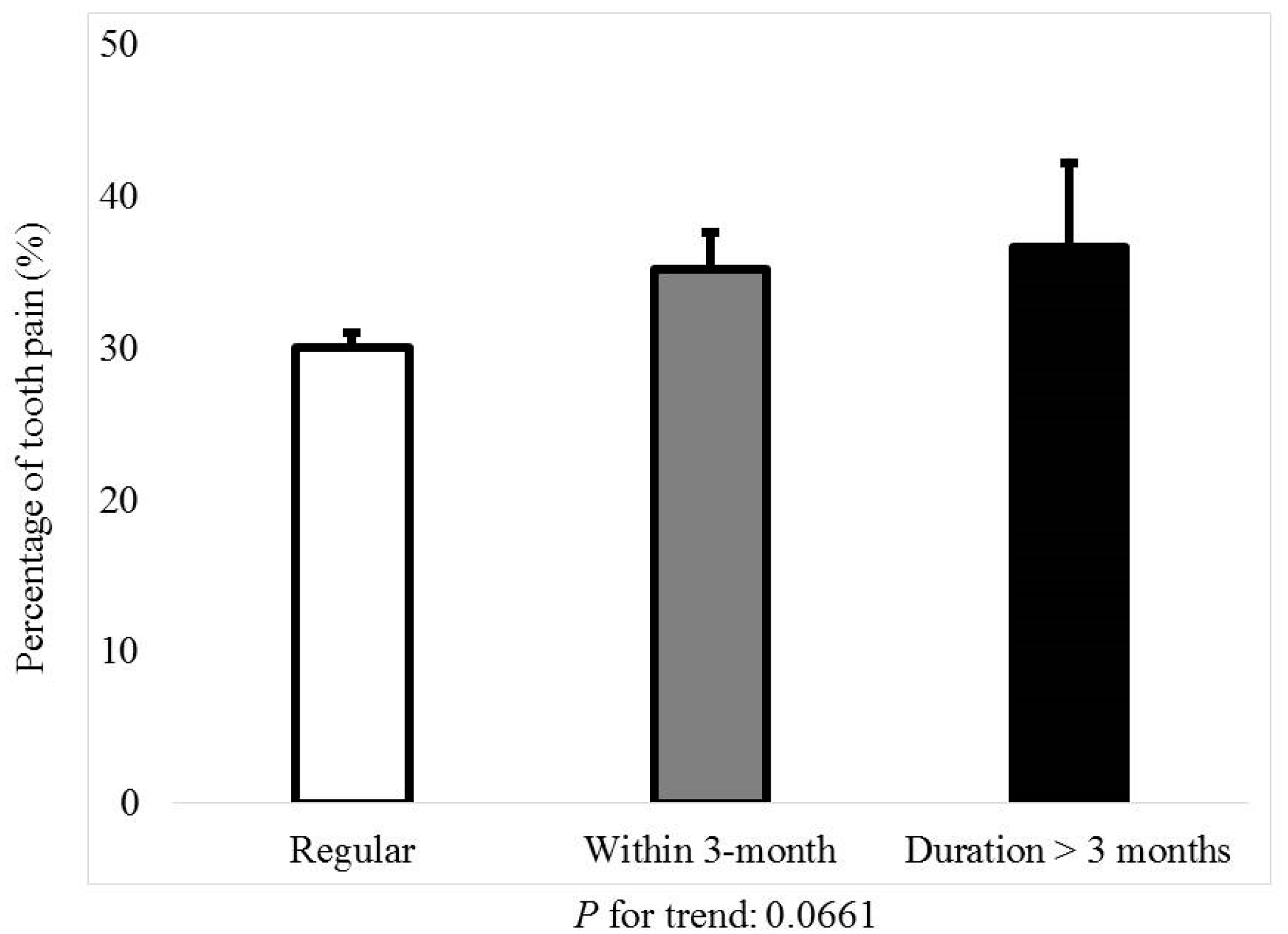
| Tooth pain (yes) | 30.0 (1.0) | 35.4 (2.3) | 0.02 |
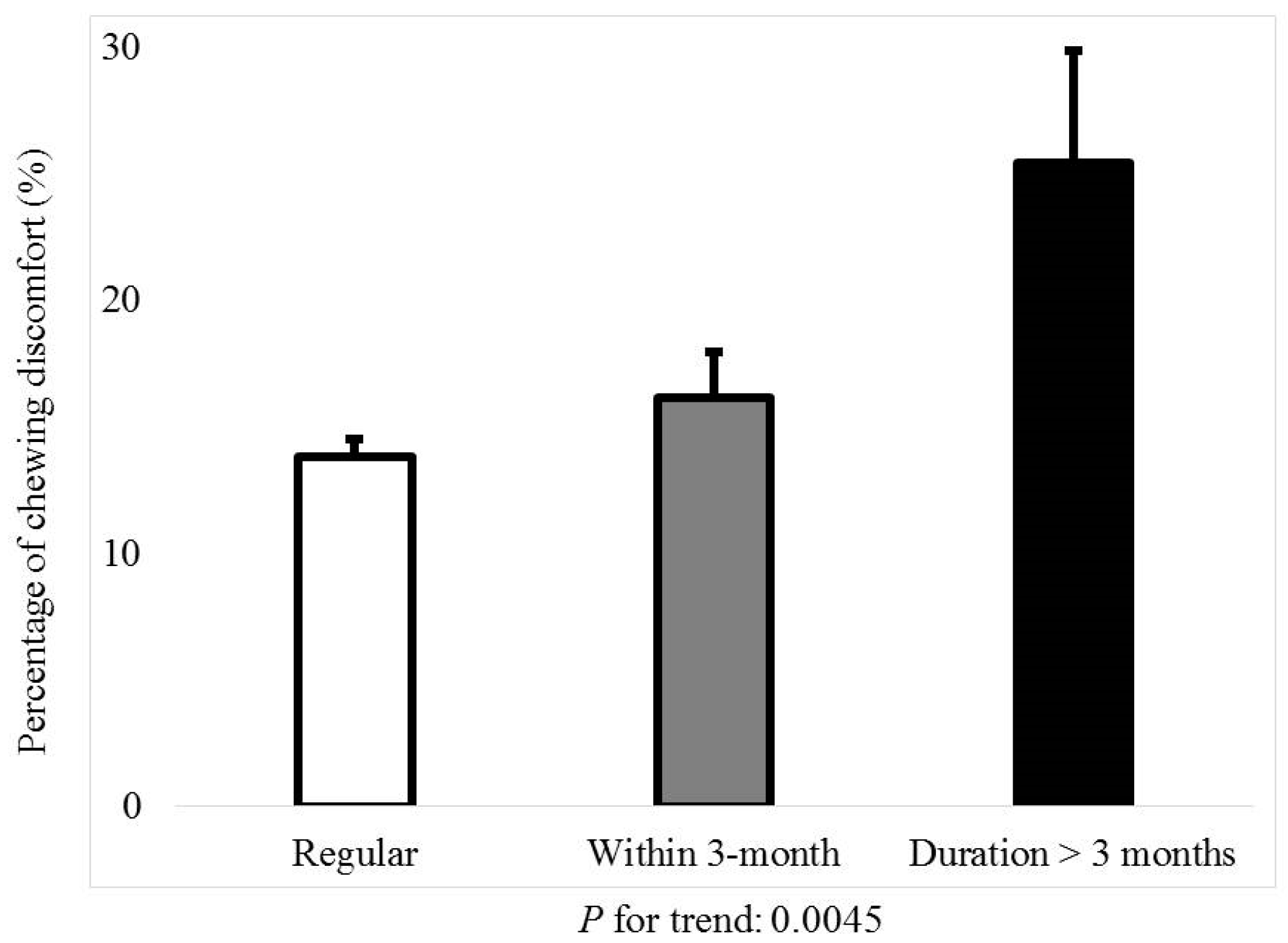
| Chewing (discomfort) | 13.8 (0.7) | 17.37 (1.7) | 0.02 |
| Age (years) | 35.5 ± 0.2 | 34.9 ± 0.5 | 0.27 |
| Body mass index (kg/m2) | 22.4 ± 0.1 | 23.2 ± 0.2 | <0.01 |
| Alcohol within one month | 52.3 (1) | 48.8 (2.5) | 0.18 |
| Smoking (currently) | 5.9 (0.5) | 8.8 (1.4) | 0.02 |
| Exercise (yes) | 16.9 (0.8) | 17.5 (1.8) | 0.77 |
| Income (the lowest quartile) | 8.5 (0.7) | 9.2 (1.5) | 0.63 |
| Education (high school graduate or higher) | 44.9 (1.1) | 31.5 (2.3) | <0.01 |
| White blood cell (×109/L) ** | 74.6 ± 0.2 | 76.4 ± 0.5 | <0.01 |
| Stress (yes) | 32.3(0.9) | 39.8 (2.2) | <0.01 |
| Metabolic syndrome | 10.4 (0.6) | 14.3 (1.6) | 0.01 |
| Number of natural teeth | 27.1 ± 0.03 | 26.92 ± 0.11 | 0.13 |
| Frequency of tooth brushing per day | <0.01 | ||
| ≤1 | 3.8 (0.4) | 5.8 (1.0) | |
| 2 | 37.6 (1.0) | 42.7 (2.3) | |
| ≥3 | 58.5 (1.0) | 51.6 (2.5) | |
| Speech (discomfort) | 2.7 (0.3) | 5.5 (1.1) | <0.01 |
| Dental checkup within 1 year (yes) | 12.7 (0.7) | 9.4 (1.3) | 0.04 |
| Menstrual Cycle Irregularity | |||
|---|---|---|---|
| No | Yes | P-Value | |
| n | 3940 | 655 | |
| Tooth pain (yes) | 30.0 (1.0) | 35.4 (2.3) | 0.02 |
| Chewing (discomfort) | 13.8 (0.7) | 17.7 (1.7) | 0.02 |
| Frequency of tooth brushing per day | 0.01 | ||
| ≤1 | 3.8 (0.4) | 5.8 (1.0) | |
| 2 | 37.6 (1) | 42.7 (2.3) | |
| ≥3 | 58.5 (1) | 51.6 (2.5) | |
| Speech (discomfort) | 2.7 (0.3) | 5.5 (1.1) | <0.01 |
| Dental checkup within 1 year (yes) | 12.7 (0.7) | 9.4 (1.3) | 0.04 |
| Tooth Pain | Chewing Discomfort | |||
|---|---|---|---|---|
| Odds Ratio (95% Confidence Interval) | P-Value | Odds Ratio (95% Confidence Interval) | P-Value | |
| Model 1 | 1.23 (1.05, 1.60) | 0.02 | 1.35 (1.05, 1.74) | 0.02 |
| Model 2 | 1.28 (1.04, 1.58) | 0.02 | 1.37 (1.06, 1.77) | 0.02 |
| Model 3 | 1.30 (1.05, 1.62) | 0.02 | 1.33 (1.03, 1.72) | 0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, I.-S.; Ki, E.Y.; Han, K.; Ryu, J.-J.; Park, J.-B. Evaluation of the Association between Menstrual Cycle Irregularity and Dental Pain or Chewing Discomfort in Women before Menopause. J. Clin. Med. 2019, 8, 454. https://doi.org/10.3390/jcm8040454
Song I-S, Ki EY, Han K, Ryu J-J, Park J-B. Evaluation of the Association between Menstrual Cycle Irregularity and Dental Pain or Chewing Discomfort in Women before Menopause. Journal of Clinical Medicine. 2019; 8(4):454. https://doi.org/10.3390/jcm8040454
Chicago/Turabian StyleSong, In-Seok, Eun Young Ki, Kyungdo Han, Jae-Jun Ryu, and Jun-Beom Park. 2019. "Evaluation of the Association between Menstrual Cycle Irregularity and Dental Pain or Chewing Discomfort in Women before Menopause" Journal of Clinical Medicine 8, no. 4: 454. https://doi.org/10.3390/jcm8040454
APA StyleSong, I.-S., Ki, E. Y., Han, K., Ryu, J.-J., & Park, J.-B. (2019). Evaluation of the Association between Menstrual Cycle Irregularity and Dental Pain or Chewing Discomfort in Women before Menopause. Journal of Clinical Medicine, 8(4), 454. https://doi.org/10.3390/jcm8040454