“With Every Step, We Grow Stronger”: The Cardiometabolic Benefits of an Indigenous-Led and Community-Based Healthy Lifestyle Intervention

 ,
,
Abstract
1. Introduction
2. Experimental Section
2.1. Cocreation of an Indigenous-Led Healthy Lifestyle Intervention
2.2. Cultural Safety Protocol
2.3. Eligibility and Exclusion Criteria
2.4. Individualized Exercise Prescriptions
2.5. Motivational Interviewing and Sharing Circles
2.6. Cardiorespiratory Fitness and Anthropometry
2.7. Self-Reported and Accelerometry-Measured Physical Activity
2.8. Statistical Analyses
3. Results
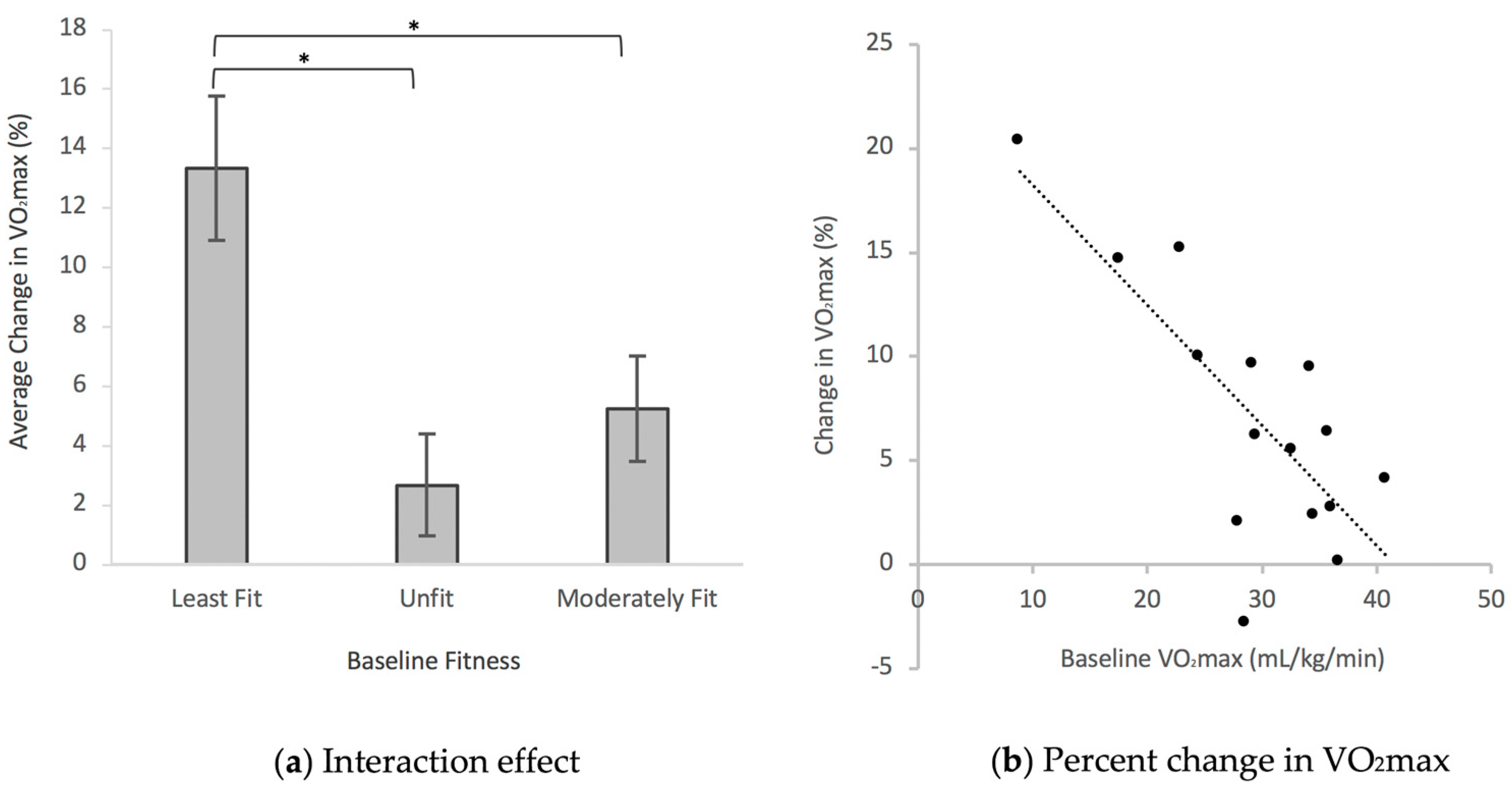
3.1. Cardiorespiratory Fitness and Anthropometric Outcomes
3.2. Exercise Adherence and Adverse Events
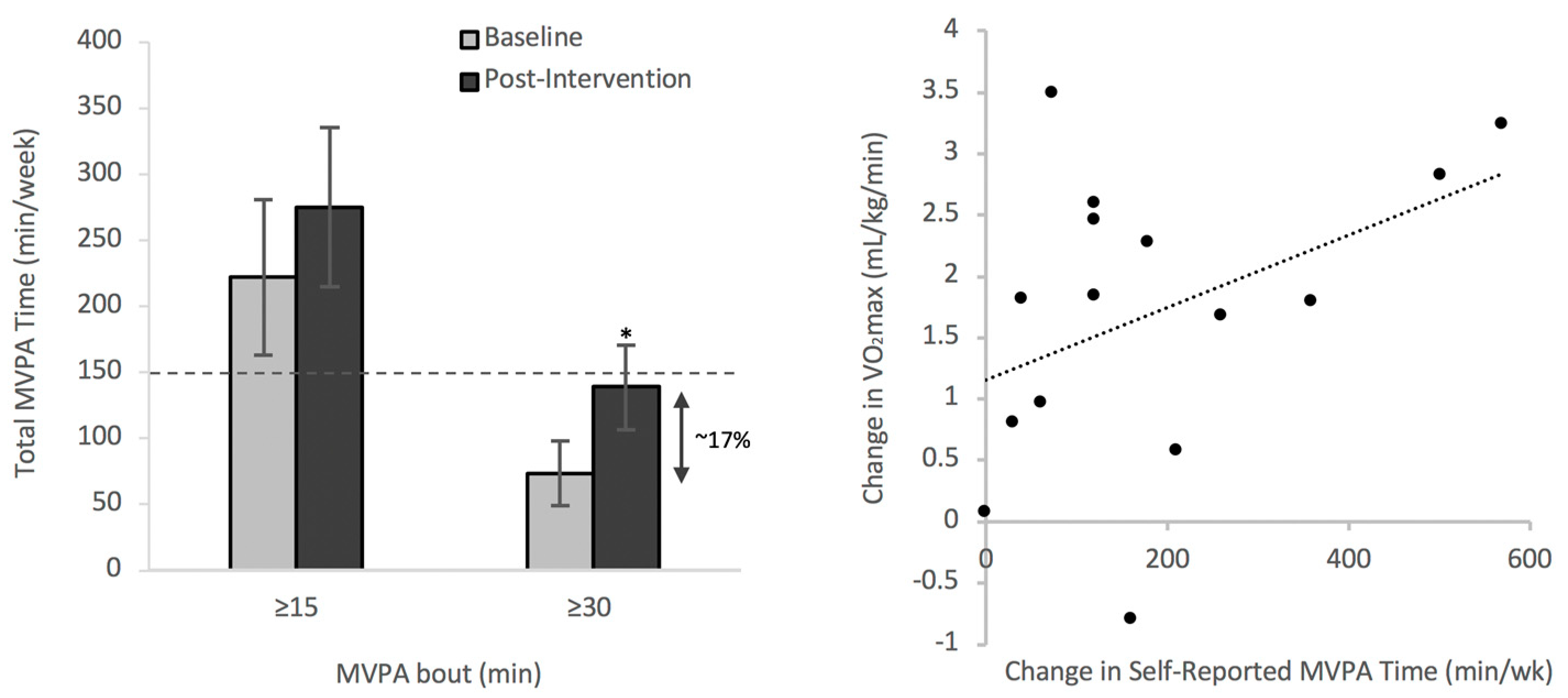
3.3. Physical Activity Levels Meeting International Recommendations
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.R.; Bredin, S.S.D. Lost in translation: What does the physical activity and health evidence actually tell us? In Lifestyle in Heart Health and Disease; Zibadi, S., Watson, R.R., Eds.; Elsevier: San Diego, CA, USA, 2018; pp. 175–186. [Google Scholar]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Warburton, D.E.; Bredin, S.S. Reflections on physical activity and health: What should we recommend? Can. J. Cardiol. 2016, 32, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicole, C.W.; Bredin, S.S. Prescribing exercise as a preventive therapy. CMAJ 2006, 174, 961–974. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Warburton, D.E.; Janssen, I.; Paterson, D.H.; Latimer, A.E.; Rhodes, R.E.; Kho, M.E.; Hicks, A.; Leblanc, A.G.; Zehr, L.; et al. New Canadian physical activity guidelines. Appl. Physiol. Nutr. Metab. 2011, 36, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Foulds, H.J.; Bredin, S.S.; Warburton, D.E. The effectiveness of community based physical activity interventions with Aboriginal peoples. Prev. Med. 2011, 53, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Katzmarzyk, P.T.; Rhodes, R.E.; Shephard, R.J. Evidence-informed physical activity guidelines for Canadian adults. Can. J. Public Health 2007, 98, 16–18. [Google Scholar]
- Pang, M.Y.; Charlesworth, S.A.; Lau, R.W.; Chung, R.C. Using aerobic exercise to improve health outcomes and quality of life in stroke: Evidence-based exercise prescription recommendations. Cerebrovasc. Dis. 2013, 35, 7–22. [Google Scholar] [CrossRef]
- Gordon, N.F.; Gulanick, M.; Costa, F.; Fletcher, G.; Franklin, B.A.; Roth, E.J.; Shephard, T. Physical activity and exercise recommendations for stroke survivors: An American Heart Association scientific statement from the Council on Clinical Cardiology, Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention; the Council on Cardiovascular Nursing; the Council on Nutrition, Physical Activity, and Metabolism; and the Stroke Council. Circulation 2004, 109, 2031–2041. [Google Scholar]
- Jones, L.W.; Alfano, C.M. Exercise-oncology research: Past, present, and future. Acta Oncol. 2013, 52, 195–215. [Google Scholar] [CrossRef]
- Myers, J.; Kaykha, A.; George, S.; Abella, J.; Zaheer, N.; Lear, S.; Yamazaki, T.; Froelicher, V. Fitness versus physical activity patterns in predicting mortality in men. Am. J. Med. 2004, 117, 912–918. [Google Scholar] [CrossRef]
- Hupin, D.; Roche, F.; Gremeaux, V.; Chatard, J.C.; Oriol, M.; Gaspoz, J.M.; Barthélémy, J.C.; Edouard, P. Even a low-dose of moderate-to-vigorous physical activity reduces mortality by 22% in adults aged ≥60 years: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; Lavie, C.J.; Johannsen, N.M.; Arena, R.; Earnest, C.P.; O’Keefe, J.H.; Milani, R.V.; Blair, S.N.; Church, T.S. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circ. J. 2013, 77, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Hedayat, L.M.A.; Murchison, C.C.; Foulds, H.J.A. A systematic review and meta-analysis of cardiorespiratory fitness among Indigenous populations in North America and circumpolar Inuit populations. Prev. Med. 2018, 109, 71–81. [Google Scholar] [CrossRef]
- Pelletier, C.A.; Smith-Forrester, J.; Klassen-Ross, T. A systematic review of physical activity interventions to improve physical fitness and health outcomes among Indigenous adults living in Canada. Prev. Med. Rep. 2017, 8, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.S.; Davis, A.D.; Ahmed, R.; Jacobs, R.; Xie, C.; Hill, A.; Sowden, J.; Atkinson, S.; Blimkie, C.; Brouwers, M.; et al. A family-based intervention to promote healthy lifestyles in an Aboriginal community in Canada. Can. J. Public Health 2007, 98, 447–452. [Google Scholar] [PubMed]
- Lytton First Nation. Available online: http://www.lyttonfirstnations.com (accessed on 21 May 2018).
- Felton-Busch, C.; Maza, K.; Ghee, M.; Mills, F.; Mills, J.; Hitchins, M.; Park, T.; Chamberlain-Salaun, J. Using mentoring circles to support Aboriginal and Torres Strait Islander nursing students: Guidelines for sharing and learning. Contemp. Nurse 2013, 46, 135–138. [Google Scholar] [CrossRef]
- Wisener, K.; Shapka, J.; Jarvis-Selinger, S. Sustaining health education research programs in Aboriginal communities. Glob. Health Promot. 2017, 24, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rollnick, S. Chapter 3: Motivational interviewing as a counselling style. In Enhancing Motivation for Change in Substance Abuse Treatment: Treatment Improvement Protocol (TIP) Series 35; Allen, K., Brown, R.L., Czechowicz, D., Foley, L.S., Glover, W.A., Greer, P.J., Hester, T.W., Hill, J.G., Kamerow, D.B., Long, S.W., et al., Eds.; U.S. Department of Health and Human Services: Rockville, MD, USA, 1999. [Google Scholar]
- Miller, S.T.; Akohoue, S.A. Two-year follow-up study of a group-based diabetes medical nutrition therapy and motivational interviewing intervention among African American women. Patient Relat. Outcome Meas. 2017, 8, 57–61. [Google Scholar] [CrossRef]
- Miller, L.S.; Gramzow, R.H. A self-determination theory and motivational interviewing intervention to decrease racial/ethnic disparities in physical activity: Rationale and design. BMC Public Health 2016, 16, 768. [Google Scholar] [CrossRef]
- Miller, N.H. Motivational interviewing as a prelude to coaching in healthcare settings. J. Cardiovasc. Nurs. 2010, 25, 247–251. [Google Scholar] [CrossRef]
- Miller, W.R.; Rollnick, S. Meeting in the middle: Motivational interviewing and self-determination theory. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 25. [Google Scholar] [CrossRef]
- The First Nations Principles of OCAP. Available online: https://fnigc.ca/ocapr.html (accessed on 21 May 2018).
- Truth and Reconciliation Commission of Canada: Calls to Action. Available online: http://www.trc.ca/websites/trcinstitution/File/2015/Findings/Calls_to_Action_English2.pdf (accessed on 21 May 2018).
- The Physical Activity and Readiness Questionnaire for Everyone. Available online: http://eparmedx.com/wp-content/uploads/2013/03/January2018PARQPlusImage.pdf (accessed on 21 May 2018).
- Health and Fitness Federation of Canada. Available online: http://www.thehffc.ca/home.html (accessed on 21 May 2018).
- Warburton, D.E.; McKenzie, D.C.; Haykowsky, M.J. Effectiveness of high-intensity interval training for the rehabilitation of patients with coronary artery disease. Am. J. Cardiol. 2005, 95, 1080–1084. [Google Scholar] [CrossRef]
- Warburton, D.E.; Sheel, A.W.; Hodges, A.N. Effects of upper extremity exercise training on peak aerobic and anaerobic fitness in patients after transplantation. Am. J. Cardiol. 2004, 93, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Reed, J.L.; Pipe, A.L. Practical approaches to prescribing physical activity and monitoring exercise intensity. Can. J. Cardiol. 2016, 32, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.T. Twenty-five Indigenous projects. In Decolonizing Methodologies: Research and Indigenous Peoples; University of Otago Press: Dunedin, New Zealand, 1999; pp. 144–145. [Google Scholar]
- Archibald, J.-A. Learning about storywork from Stó:lō Elders. In Indigenous Storywork: Educating the Heart, Mind, Body, and Spirit; UBC Press: Vancouver, BC, Canada, 2008; pp. 59–83. [Google Scholar]
- Anderson, A.; Anderson, J.; Hare, J.; McTavish, M. Research with young children and their families in Indigenous, immigrant, and refugee communities. In Handbook of Research Methods in Early Childhood Education, Volume II; Saracho, O., Ed.; Information Age Publishing: Charlotte, NC, USA, 2015; pp. 115–145. [Google Scholar]
- Kovach, M. Indigenous Methodologies: Characteristics, Conversations and Contexts; University of Toronto Press: Toronto, ON, Canada, 2009. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behaviour change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Burr, J.F.; Bredin, S.S.; Faktor, M.D.; Warburton, D.E. The 6-minute walk test as a predictor of objectively measured aerobic fitness in healthy working-aged adults. Phys. Sportsmed. 2011, 39, 133–139. [Google Scholar] [CrossRef] [PubMed]
- The Revision of the Measurement of Waist Circumference in the CPAFLA. Available online: http://www.oshf.ca/cmfiles/measurementofwaistcircumference.pdf (accessed on 21 May 2018).
- Payne, N.; Gledhill, N.; Katzmarzyk, P.T.; Jamnik, V.K.; Keir, P.J. Canadian musculoskeletal fitness norms. Can. J. Appl. Physiol. 2000, 25, 430–442. [Google Scholar] [CrossRef]
- Godin, G.; Shephard, R.J. A simple method to assess exercise behaviour in the community. Can. J. Appl. Sport Sci. 1985, 10, 141–146. [Google Scholar] [PubMed]
- Staudenmayer, J.; He, S.; Sasaki, J.; Freedson, P. Methods to estimate aspects of physical activity and sedentary behaviour from high-frequency wrist accelerometer measurements. J. Appl. Physiol. 2015, 119, 396–403. [Google Scholar] [CrossRef]
- Skender, S.; Ose, J.; Chang-Claude, J.; Paskow, M.; Brühmann, B.; Siegel, E.M.; Steindorf, K.; Ulrich, C.M. Accelerometry and physical activity questionnaires: A systematic review. BMC Public Health 2016, 16, 515. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Nyström, C.D.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practice considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- American College of Sports Medicine. ACSM position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; McAuley, P.; Lavie, C.J.; Despres, J.P.; Arena, R.; Kokkinos, P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: Their independent and interwoven importance to health status. Prog. Cardiovasc. Dis. 2015, 57, 306–314. [Google Scholar] [CrossRef]
- Zhang, D.; Shen, X.; Qi, X. Resting heart rate and all-cause and cardiovascular mortality in the general population: A meta-analysis. CMAJ 2015, 188, E53–E63. [Google Scholar] [CrossRef]
- Hypertension Canada’s 2018 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children. Available online: https://www.onlinecjc.ca/article/S0828-282X(18)30183-1/fulltext (accessed on 23 May 2018).
- Elliot, S.A.; Baxter, K.A.; Davies, P.S.; Truby, H. Accuracy of self-reported physical activity levels in obese adolescents. J. Nutr. Metab. 2014. [Google Scholar] [CrossRef]
- Leatherdale, S.T.; Laxer, R.E.; Faulkner, G. Reliability and validity of the physical activity and sedentary behaviour measures in the COMPASS study. Compass Tech. Rep. Ser. 2014, 2, 1–17. [Google Scholar]
- Classification and Risks of Overweight and Obesity. Available online: https://www.nhlbi.nih.gov/health-topics/overweight-and-obesity (accessed on 18 August 2018).
- Foulds, H.; Bredin, S.S.D.; Warburton, D.E.R. The relationship between diabetes and obesity across different ethnicities. J. Diabetes Metab. 2012, 3, 228. [Google Scholar] [CrossRef]
- Foulds, H.J.; Bredin, S.S.; Warburton, D.E. The prevalence of overweight and obesity in British Columbian Aboriginal adults. Obes. Rev. 2011, 12, e4–e11. [Google Scholar] [CrossRef] [PubMed]
- Foulds, H.J.; Bredin, S.S.; Warburton, D.E. An evaluation of the physical activity and health status of British Columbian Aboriginal populations. Appl. Physiol. Nutr. Metab. 2012, 37, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.D.; Wilks, R.; McCaw-Binns, A. Effect of aerobic exercise (walking) training on functional status and health-related quality of life in chronic stroke survivors. Stroke 2013, 44, 1179–1181. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Bartali, B.; Cavazzini, C.; Di lorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L. Age-associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J. Appl. Physiol. 2003, 95, 1851–1860. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, T. Muscle strength, disability and mortality. Scand. J. Med. Sci. Sports 2003, 13, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Sallinen, J.; Stenholm, S.; Rantanen, T.; Heliovaara, M.; Sainio, P.; Koskinen, S. Hand-grip strength cut points to screen older persons at risk for mobility limitation. J. Am. Geriatr. Soc. 2010, 58, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.S.; Lo, K.M.; McDowall, M.; West, T. Fractures after stroke: Frequency, types, and associations. Stroke 2002, 33, 728–734. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Lear, S.A. Physical activity for obese individuals: A systematic review of effects on chronic disease risk factors. Obes. Rev. 2012, 13, 95–105. [Google Scholar] [CrossRef]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; Berrington de Gonzalez, A.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Program Stage | Week | Frequency (days/week) | Intensity | Duration (min) | ||
|---|---|---|---|---|---|---|
| %HRR | RPE | Breathing Rate | ||||
| Initial Stage: Mild to moderate intensity aerobic exercise | 1 | 3 | 40–50 | 3–4 | Slightly increased | 15–20 |
| 2 | 3 | 40–50 | 3–4 | Slightly increased | 20–25 | |
| 3 | 3 | 50–60 | 3–5 | Noticeably increased | 20–25 | |
| 4 | 3 | 50–60 | 3–5 | Noticeably increased | 25–30 | |
| Improvement: Exercise intensity and duration increase with fitness | 5–7 | 4 | 60–70 | 3–4 | Noticeably increased | 25–30 |
| 8–10 | 4 | 60–70 | 3–4 | Noticeably increased | 30–35 | |
| 11–13 | 3–5 | 65–75 | 3–5 | Noticeably increased | 30–35 | |
| Fitness Group | Age (year) | 6MWT Distance (m) | VO2max (mL/kg/min) | ΔVO2max (%) | ||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||
| Least Fit (n = 5) | 46.8 ± 5.5 | 439.0 ± 31.5 | 470.2 ± 18.1 | 20.7 ± 3.5 | 23.1 ± 3.6 ** | 13.3 ± 2.4 ** |
| Unfit (n = 5) | 36.2 ± 5.0 | 569.0 ± 24.1 | 545.0 ± 24.1 | 34.9 ± 2.0 | 35.9 ± 2.4 | 2.7 ± 1.7 |
| Moderately Fit (n = 5) | 48.6 ± 7.1 | 487.4 ± 19.8 | 496.2 ± 27.3 | 32.4 ± 1.6 | 34.1 ± 1.7 | 5.3 ± 1.8 |
| Overall (n = 15) | 43.9 ± 3.5 | 498.5 ± 19.8 | 503.8 ± 15.0 | 29.3 ± 2.1 | 31.0 ± 2.1 * | 7.1 ± 1.6 * |
| Fitness Group | Resting Heart Rate (bpm) | Resting SBP (mmHg) | Resting DBP (mmHg) | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |
| Least Fit (n = 5) | 84.8 ± 4.3 | 76.4 ± 5.6 * | 135.0 ± 8.3 | 126.8 ± 5.4 | 85.6 ± 4.1 | 76.2 ± 5.9 |
| Unfit (n = 5) | 79.4 ± 5.7 | 69.2 ± 3.7 * | 127.2 ± 5.7 | 113.2 ± 3.1 | 79.8 ± 3.7 | 74.2 ± 2.3 |
| Moderately Fit (n = 5) | 77.2 ± 3.8 | 70.4 ± 2.4 * | 110.8 ± 3.3 | 109.8 ± 2.7 | 67.8 ± 2.9 | 63.0 ± 4.2 |
| Overall (n = 15) | 80.5 ± 2.6 | 72.0 ± 2.4 * | 124.3 ± 4.2 | 116.6 ± 2.9 * | 77.7 ± 2.8 | 71.1 ± 2.8 * |
| Fitness Group | Weight (kg) | Body Mass Index (kg/m2) | Waist Circumference (cm) | |||
| Pre | Post | Pre | Post | Pre | Post | |
| Least Fit (n = 5) | 99.5 ± 5.7 | 99.2 ± 5.7 | 37.2 ± 2.0 | 37.1 ± 2.0 | 119.2 ± 5.2 | 117.8 ± 3.9 |
| Unfit (n = 5) | 79.7 ± 4.2 | 81.2 ± 4.0 | 28.4 ± 3.0 | 28.9 ± 3.0 | 101.0 ± 5.0 | 103.1 ± 4.7 |
| Moderately Fit (n = 5) | 65.2 ± 4.2 | 64.6 ± 4.2 | 26.2 ± 1.1 | 25.9 ± 1.2 | 94.9 ± 3.3 | 93.0 ± 2.6 |
| Overall (n = 15) | 81.5 ± 4.5 | 81.7 ± 4.5 | 30.6 ± 1.7 | 30.7 ± 1.7 | 105.0 ± 3.7 | 104.6 ± 3.4 |
| Fitness Group | Grip Strength (kg) | Sit-and-Reach (cm) | Bioelectrical Impedance (%) | |||
| Pre | Post | Pre | Post | Pre | Post | |
| Least Fit (n = 5) | 60.6 ± 7.1 | 59.8 ± 7.0 | 24.0 ± 3.1 | 23.3 ± 3.6 | 49.2 ± 1.6 | 49.4 ± 1.4 |
| Unfit (n = 5) | 71.2 ± 5.9 | 73.6 ± 3.3 | 26.1 ± 3.2 | 27.8 ± 2.5 | 34.6 ± 6.0 | 35.7 ± 5.9 |
| Moderately Fit (n = 5) | 52.4 ± 7.3 | 47.6 ± 6.5 | 31.3 ± 1.7 | 31.0 ± 3.0 | 34.7 ± 2.4 | 34.2 ± 2.4 |
| Overall (n = 15) | 61.4 ± 4.2 | 60.3 ± 4.2 | 25.7 ± 1.7 | 27.1 ± 1.8 | 39.8 ± 2.7 | 40.1 ± 2.6 |
| Fitness Group | Frequency of MVPA Bouts ≥ 15 min (#/week) | MVPA Time ≥ 15 min (min/week) | Change in MVPA Time ≥ 15 min Bouts (min/day) | ||
| Pre | Post | Pre | Post | ||
| Least Fit (n = 3) | 16.0 ± 11.1 | 15.7 ± 8.8 | 240.0 ± 167.0 | 235.0 ± 132.5 | -0.7 ± 5.0 |
| Unfit (n = 3) | 13.7 ± 4.3 | 22.0 ± 9.6 | 205.0 ± 63.8 | 330.0 ± 144.1 | 17.9 ± 11.5 |
| Moderately Fit (n = 5) | 14.8 ± 6.4 | 17.8 ± 5.9 | 222.0 ± 95.7 | 267.0 ± 87.9 | 6.4 ± 8.6 |
| Overall (n = 11) | 14.8 ± 3.9 | 18.4 ± 4.0 | 222.3 ± 58.5 | 275.5 ± 60.2 | 7.6 ± 5.2 |
| Fitness Group | Frequency of MVPA Bouts ≥ 30 min (#/week) | MVPA Time ≥ 30 min (min/week) | Change in MVPA Time ≥ 30 min Bouts (min/day) | ||
| Pre | Post | Pre | Post | ||
| Least Fit (n = 3) | 2.3 ± 1.9 | 5.0 ± 3.1 | 70.0 ± 55.7 | 150.0 ± 91.7 | 11.4 ± 5.2 |
| Unfit (n = 3) | 3.3 ± 0.3 | 5.0 ± 2.0 | 100.0 ± 10.0 | 150.0 ± 60.0 | 7.1 ± 7.1 |
| Moderately Fit (n = 5) | 2.0 ± 1.5 | 4.2 ± 1.5 | 60.0 ± 46.5 | 126.0 ± 43.9 | 9.4 ± 8.1 |
| Overall (n = 11) | 2.4 ± 0.8 | 4.6 ± 1.1 * | 73.6 ± 24.4 | 139.1 ± 31.9 * | 9.4 ± 4.0 * |
| Fitness Group | MVPA Time (min/week) | |
|---|---|---|
| Pre | Post | |
| Least Fit (n = 5) | 89 ± 17 | 184 ± 19 * |
| Unfit (n = 5) | 316 ± 55 | 508 ± 70 * |
| Moderately Fit (n = 5) | 118 ± 27 | 392 ± 73 |
| Overall (n = 15) | 174 ± 52 | 361 ± 79 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, H.P.H.; Miles, R.M.; Bredin, S.S.D.; Kaufman, K.L.; Chua, C.Z.Y.; Hare, J.; Norman, M.E.; Rhodes, R.E.; Oh, P.; Warburton, D.E.R. “With Every Step, We Grow Stronger”: The Cardiometabolic Benefits of an Indigenous-Led and Community-Based Healthy Lifestyle Intervention. J. Clin. Med. 2019, 8, 422. https://doi.org/10.3390/jcm8040422
Lai HPH, Miles RM, Bredin SSD, Kaufman KL, Chua CZY, Hare J, Norman ME, Rhodes RE, Oh P, Warburton DER. “With Every Step, We Grow Stronger”: The Cardiometabolic Benefits of an Indigenous-Led and Community-Based Healthy Lifestyle Intervention. Journal of Clinical Medicine. 2019; 8(4):422. https://doi.org/10.3390/jcm8040422
Chicago/Turabian StyleLai, Henry P.H., Rosalin M. Miles, Shannon S.D. Bredin, Kai L. Kaufman, Charlie Z.Y. Chua, Jan Hare, Moss E. Norman, Ryan E. Rhodes, Paul Oh, and Darren E.R. Warburton. 2019. "“With Every Step, We Grow Stronger”: The Cardiometabolic Benefits of an Indigenous-Led and Community-Based Healthy Lifestyle Intervention" Journal of Clinical Medicine 8, no. 4: 422. https://doi.org/10.3390/jcm8040422
APA StyleLai, H. P. H., Miles, R. M., Bredin, S. S. D., Kaufman, K. L., Chua, C. Z. Y., Hare, J., Norman, M. E., Rhodes, R. E., Oh, P., & Warburton, D. E. R. (2019). “With Every Step, We Grow Stronger”: The Cardiometabolic Benefits of an Indigenous-Led and Community-Based Healthy Lifestyle Intervention. Journal of Clinical Medicine, 8(4), 422. https://doi.org/10.3390/jcm8040422