Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL)

 , ,
, , 
Abstract
1. Introduction
2. Section A. Selected Etiological Factors in Crestal Bone Loss
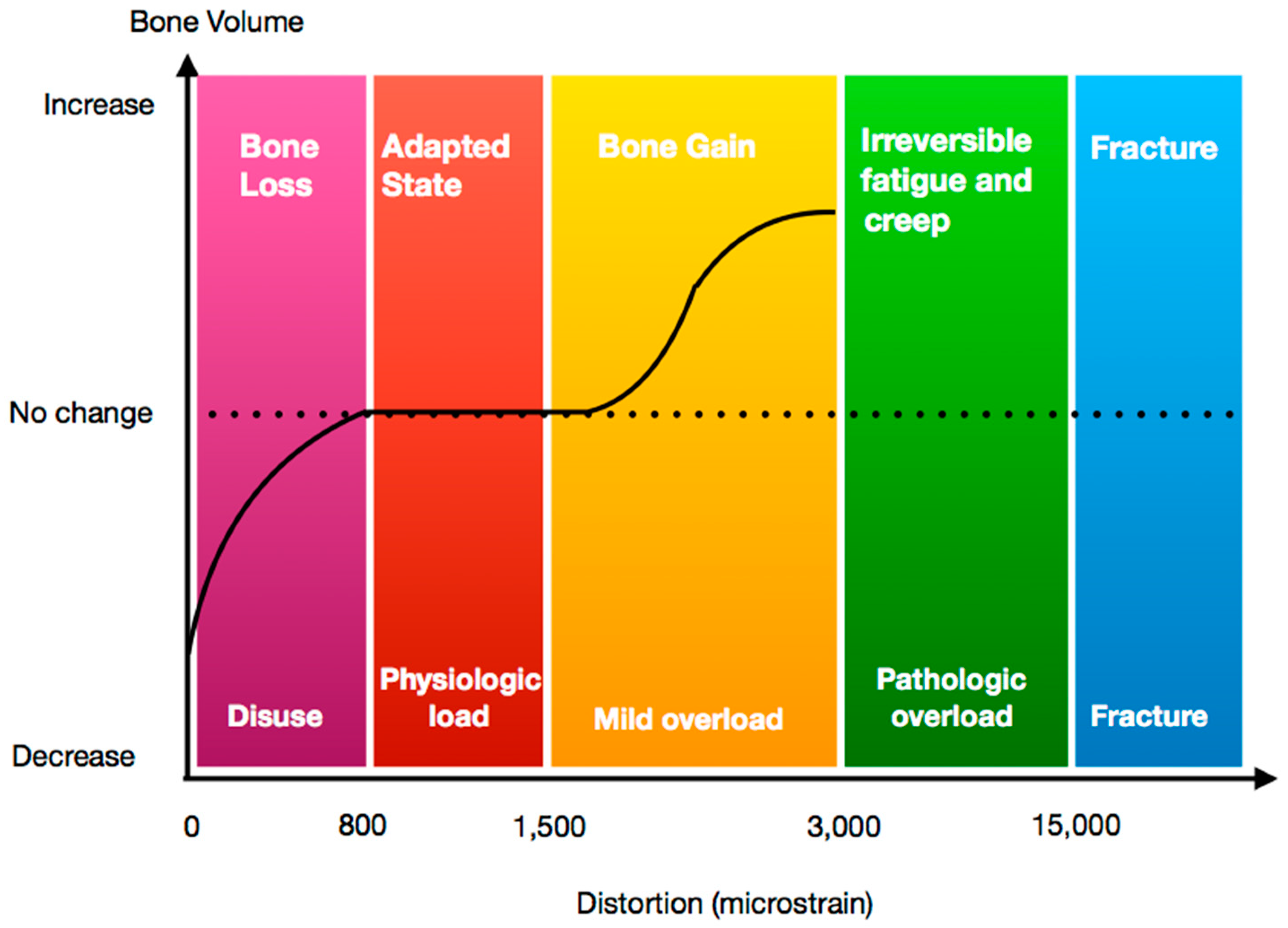
2.1. Overloading
2.2. Peri-Implant CBL and Periodontal Pathogens
2.3. Bone and the Immune System—Foreign Body Reaction
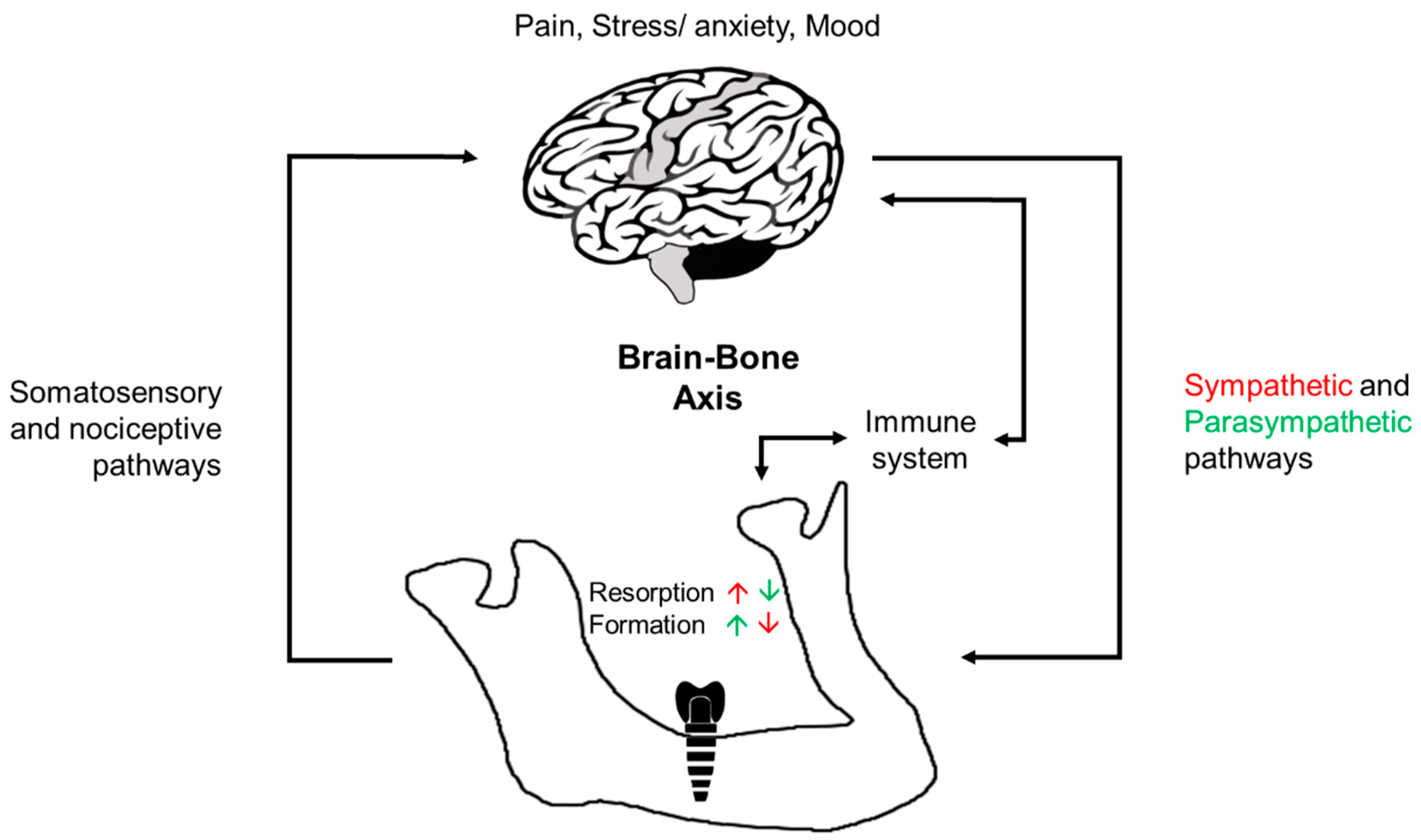
2.4. The Role of the Brain in Modulating Osseointegration: Brain–Bone Axis
3. Section B. Methods of Measuring Crestal Bone Loss
3.1. Current Methods
3.1.1. Standardized Intraoral Radiographs (SIR)
Accuracy
Sensitivity and Specificity
Pros and Cons
3.1.2. Cone Beam Computerized Tomography (CBCT)
Accuracy
Sensitivity and Specificity
Pros & Cons
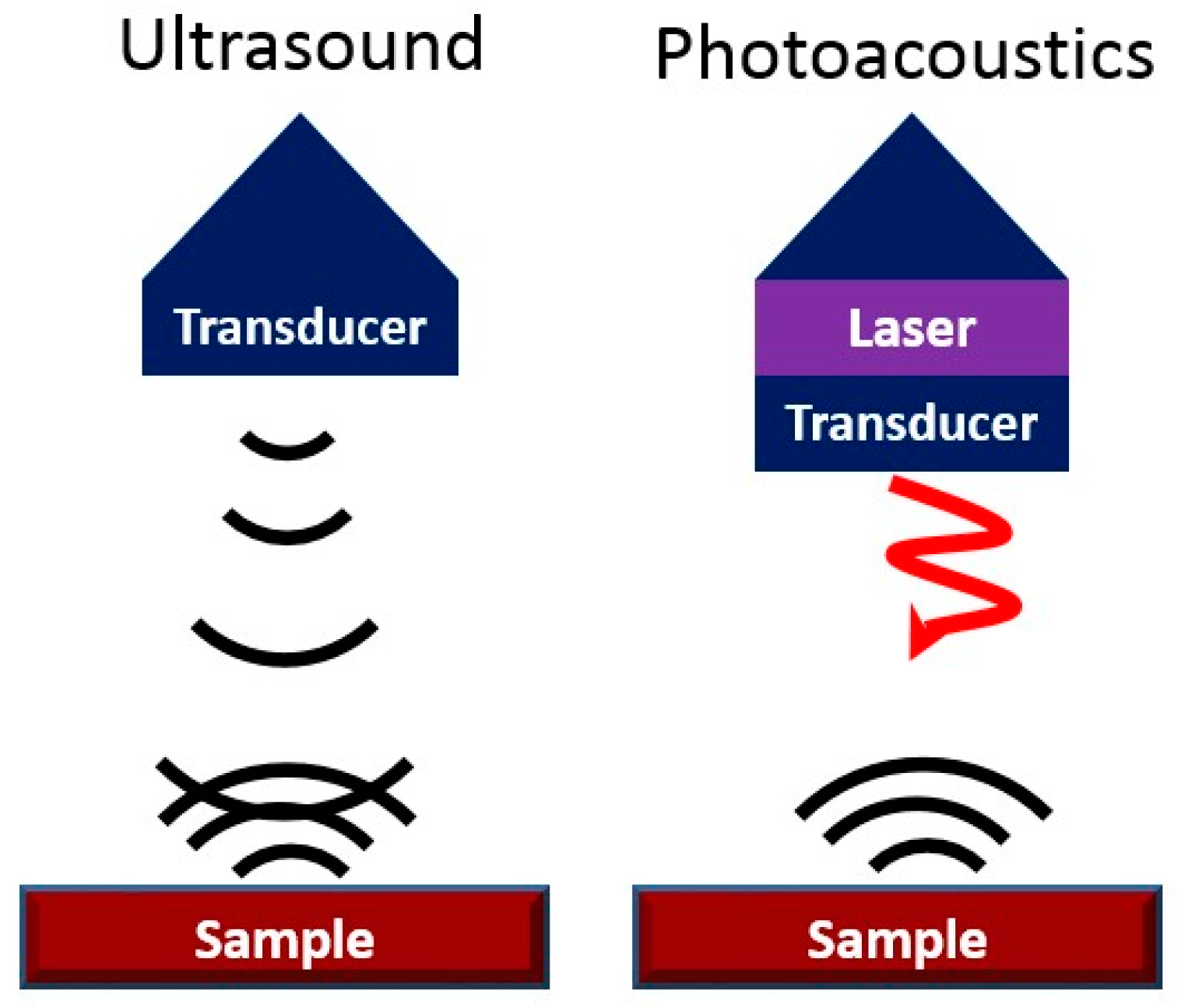
3.2. Novel Method: Photoacoustic Ultrasound as an Innovative Method to Measure Peri-Implant Pocket Depths and Bone Loss over Time
Imaging the Periodontal Pocket with Photoacoustic Ultrasound
4. Summary
Author Contributions
Conflicts of Interest
References
- Koka, S.; Zarb, G.A. On osseointegration: The healing adaptation principle in the context of osseosufficiency, osseoseparation, and dental implant failure. Int. J. Prosthodont. 2012, 25, 48–52. [Google Scholar] [PubMed]
- Bryant, S.R. Oral Implant Outcomes Predicted by Age- and Site-Specific Aspects of Bone Condition. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, 2001. [Google Scholar]
- Linkevicius, T.; Puisys, A.; Vindasuite, E.; Linkeviciene, L.; Apse, P. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin. Oral Implants Res. 2013, 24, 1179–1184. [Google Scholar] [CrossRef] [PubMed]
- Roos-Jansaker, A.M. Long time follow up of implant therapy and treatment of peri-implantitis. Swed. Dent. J. Suppl. 2007, 188, 7–66. [Google Scholar]
- Fransson, C.; Lekholm, U.; Jemt, T.; Berglundh, T. Prevalence of subjects with progressive bone loss. Clin. Oral Implants Res. 2005, 16, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef] [PubMed]
- Frost, H.M. A 2003 update of bone physiology and Wolff’s Law for clinicians. Angle Orthod. 2004, 74, 3–15. [Google Scholar] [PubMed]
- Naert, I.; Duyck, J.; Vandamme, K. Occlusal overload and bone/implant loss. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 95–107. [Google Scholar] [CrossRef]
- Isidor, F. Loss of osseointegration caused by occlusal load of oral implants. Clin. Oral Implants Res. 1996, 7, 143–152. [Google Scholar] [CrossRef]
- Miyata, T.; Kobayashi, Y.; Araki, H.; Ohto, T.; Shin, K. The influence of controlled occlusal overload on peri-implant tissue. Part 3: A histologic study in monkeys. Int. J. Oral Maxillofac. Implants 2000, 15, 425–431. [Google Scholar]
- Esaki, D.; Matsushita, Y.; Ayukawa, Y.; Sakai, N.; Sawae, Y.; Koyano, K. Relationship between magnitude of immediate loading and peri-implant osteogenesis in dogs. Clin. Oral Implants Res. 2012, 23, 1290–1296. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Schmid, B.; Weigel, C.; Gerber, S.; Bosshardt, D.D.; Jonsson, J.; Lang, N.P.; Jönsson, J. Does excessive occlusal load affect osseointegration? Exp. Study Dog Clin. Oral Implants Res. 2004, 15, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Tsourdi, E.; Jahn, K.; Rauner, M.; Busse, B.; Bonewald, L.F. Physiological and pathological osteocytic osteolysis. J. Musculoskelet. Neuronal Interact. 2018, 18, 292–303. [Google Scholar] [PubMed]
- Klein-Nulend, J.; van der Plas, A.; Semeins, C.M.; Ajubi, N.E.; Frangos, J.A.; Nijweide, P.J.; Burger, E.H. Sensitivity of osteocytes to biomechanical stress in vitro. FASEB J. 1995, 9, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Van Bezooijen, R.L.; Roelen, B.A.; Visser, A.; van der Wee-Pals, L.; de Wilt, E.; Karperien, M.; Hamersma, H.; Papapoulos, S.E.; ten Dijke, P.; Löwik, C.W. Sclerostin is an osteocyte-expressed negative regulator of bone formation, but not a classical BMP antagonist. J. Exp. Med. 2004, 199, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, T.; Hayashi, M.; Fukunaga, T.; Kurata, K.; Oh-Hora, M.; Feng, J.Q.; Bonewald, L.F.; Kodama, T.; Wutz, A.; Wagner, E.F.; et al. Evidence for osteocyte regulation of bone homeostasis through RANKL expression. Nat. Med. 2011, 17, 1231–1234. [Google Scholar] [CrossRef] [PubMed]
- Dallas, S.L.; Prideaux, M.; Bonewald, L.F. The osteocyte: An endorine cell… and more. Endocr. Rev. 2013, 34, 658–690. [Google Scholar] [CrossRef] [PubMed]
- Van Steenberghe, D.; Klinge, B.; Lindén, U.; Quirynen, M.; Herrmann, I.; Garpland, C. Periodontal indices around natural and titanium abutments: A longitudinal multicenter study. J. Periodontol. 1993, 64, 538–541. [Google Scholar] [CrossRef]
- Charalampakis, G.; Abrahamsson, I.; Carcuac, O.; Dahlén, G.; Berglundh, T. Microbiota in experimental periodontitis and peri-implantitis in dogs. Clin. Oral Implants Res. 2014, 25, 1094–1098. [Google Scholar] [CrossRef]
- Berglundh, T.; Gotfredsen, K.; Zitzmann, N.U.; Lang, N.P.; Lindhe, J. Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: An experimental study in dogs. Clin. Oral Implants Res. 2007, 18, 655–661. [Google Scholar] [CrossRef]
- Carcuac, O.; Abrahamsson, I.; Albouy, J.P.; Linder, E.; Larsson, L.; Berglundh, T. Experimental periodontitis and peri-implantitis in dogs. Clin. Oral Implants Res. 2013, 24, 363–371. [Google Scholar] [CrossRef]
- Anderson, J.M. Inflammation, wound healing, and the foreign-body response. In Biomaterials Science: An Introduction to Materials, 3rd ed.; Academic Press: Cambridge, UK, 2013; pp. 503–512. [Google Scholar]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Zohdi, H.; Fujioka-Kobayashi, M.; Bosshardt, D.D. Giant cells around bone biomaterials: Osteoclasts or multi-nucleated giant cells? Acta Biomater. 2016, 46, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, Z.; Sima, C.; Glogauer, M. Bone replacement materials and techniques used for achieving vertical alveolar bone augmentation. Materials 2015, 8, 2953–2993. [Google Scholar] [CrossRef]
- Donath, K.; Laass, M.; Gunzl, H.J. The histopathology of different foreign-body reactions in oral soft tissue and bone tissue. Virchows Archiv. A 1992, 420, 131–137. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Molne, J.; Wennerberg, A. Foreign body reactions, marginal bone loss and allergies in relation to titanium implants. Eur. J. Oral Implantol. 2018, 11 (Suppl. 1), S37–S46. [Google Scholar]
- Albrektsson, T.; Dahlin, C.; Jemt, T.; Sennerby, L.; Turri, A.; Wennerberg, A. Is marginal bone loss around oral implants the result of a provoked foreign body reaction? Clin. Implant Dent. Relat. Res. 2014, 16, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Bielemann, A.M.; Marcello-Machado, R.M.; Del Bel Cury, A.A.; Faot, F. Systematic review of wound healing biomarkers in peri-implant crevicular fluid during osseointegration. Arch. Oral Biol. 2018, 89, 107–128. [Google Scholar] [CrossRef]
- Kzhyshkowska, J.; Gudima, A.; Riabov, V.; Dollinger, C.; Lavalle, P.; Vrana, N.E. Macrophage responses to implants: Prospects for personalized medicine. J. Leukoc. Biol. 2015, 98, 953–962. [Google Scholar] [CrossRef]
- Takayanagi, H. Osteoimmunology: Shared mechanisms and crosstalk between the immune and bone systems. Nat. Rev. Immunol. 2007, 7, 292–304. [Google Scholar] [CrossRef]
- Takayanagi, H. New developments in osteoimmunology. Nat. Rev. Rheumatol. 2012, 8, 684–689. [Google Scholar] [CrossRef]
- Trindade, R.; Albrektsson, T.; Galli, S.; Prgomet, Z.; Tengvall, P.; Wennerberg, A. Osseointegration and foreign body reaction: Titanium implants activate the immune system and suppress bone resorption during the first 4 weeks after implantation. Clin. Implants Dent. Relat Res. 2018, 20, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Trindade, R.; Albrektsson, T.; Tengvall, P.; Wennerberg, A. Foreign body reaction to biomaterials: On mechanisms for buildup and breakdown of osseointegration. Clin. Implants Dent. Relat. Res. 2016, 18, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Chrcanovic, B.; Jacobsson, M.; Wennerberg, A. Osseointegration of implants—A biological and clinical overview. JSM Dent. Surg 2017, 2, 1022–1027. [Google Scholar]
- Albrektsson, T.; Jämt, T.; Molne, J.; Tengvall, P.; Wennerberg, A. On inflammation-immunological balance theory—A critical apprehension of disease concepts around implants: Mucositis and marginal bone loss may represent normal conditions and not necessarily a state of disease. J. Clin. Implant Dent. Relat. Res. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, V.; Cavusoglu, Y.; Gruber, R.; Kuchler, U.; Buser, D.; Bosshardt, D.D. Osseointegration of zirconia in the presence of multinucleated giant cells. Clin. Implants Dent. Relat. Res. 2016, 18, 686–698. [Google Scholar] [CrossRef] [PubMed]
- Avivi-Arber, L.; Avivi, D.; Perez, M.; Arber, N.; Shapira, S. Impaired bone healing at tooth extraction sites in cd24-deficient mice: A pilot study. PLoS ONE 2018, 13, e0191665. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Giannobile, W.V. Investigational clinical research in implant dentistry: Beyond observational and descriptive studies. J. Dent. Res. 2013, 92 (Suppl. 12), 107s–108s. [Google Scholar] [CrossRef]
- Brånemark, P.I.; Zarb, G.A.; Albrektsson, T. Tissue-Integrated Prostheses. Osseointegration in Clinical Dentistry; Quintessence: Chicago, IL, USA, 1985. [Google Scholar]
- Nishimura, I. Genetic networks in osseointegration. J. Dent. Res. 2013, 92 (Suppl. 12), 109s–118s. [Google Scholar] [CrossRef]
- Wennerberg, A.; Ide-Ektessabi, A.; Hatkamata, S.; Sawase, T.; Johansson, C.; Albrektsson, T.; Martinelli, A.; Sodervall, U.; Odelius, H. Titanium release from implants prepared with different surface roughness. Clin. Oral Implants Res. 2004, 15, 505–512. [Google Scholar] [CrossRef]
- Delgado-Ruiz, R.; Romanos, G. Potential causes of titanium particle and ion release in implant dentistry: A systematic review. Int J. Mol. Sci. 2018, 19, 3585. [Google Scholar] [CrossRef]
- Franchi, M.; Bacchelli, B.; Martini, D.; Pasquale, V.D.; Orsini, E.; Ottani, V.; Fini, M.; Giavaresi, G.; Giardino, R.; Ruggeri, A. Early detachment of titanium particles from various different surfaces of endosseous dental implants. Biomaterials 2004, 25, 2239–2246. [Google Scholar] [CrossRef] [PubMed]
- Trindade, R.; Albrektsson, T.; Galli, S.; Prgomet, Z.; Tengvall, P.; Wennerberg, A. Bone Immune Response to Materials, Part I: Titanium, PEEK and Copper in Comparison to Sham at 10 Days in Rabbit Tibia. J. Clin. Med. 2018, 7, 526. [Google Scholar] [CrossRef] [PubMed]
- Lechner, J.; Noumbissi, S.; von Baehr, V. Titanium implants and silent inflammation in jawbone-a critical interplay of dissolved titanium particles and cytokines tnf-alpha and rantes/ccl5 on overall health? EPMA J. 2018, 9, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Noronha Oliveira, M.; Schunemann, W.V.H.; Mathew, M.T.; Henriques, B.; Magini, R.S.; Teughels, W.; Souza, J.C.M. Can degradation products released from dental implants affect peri-implant tissues? J. Periodontal. Res. 2018, 53, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, R.J. Metal Release from Implants and Its Effect on the Immune System. Ph.D. Thesis, Technical University of Denmark, DTU Mechanical Engineering, Lyngby, Denmark, 2016. [Google Scholar]
- Elefteriou, F. Regulation of bone remodeling by the central and peripheral nervous system. Arch. Biochem. Biophys. 2008, 473, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.G.; Sun, B.H.; Dietrich, M.O.; Koch, M.; Yao, G.Q.; Diano, S.; Insogna, K.; Horvath, T.L. AGRP neurons regulate bone mass. Cell Rep. 2015, 13, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Takeda, S.; Ducy, P. Regulation of bone remodeling by central and peripheral nervous signals. In Principles of Bone Biology; Bilezekian, J., Raisz, L.G., Martin, T.J., Eds.; Academic Press: Cambridge, MA, USA, 2008; pp. 1059–1068. [Google Scholar]
- Bajayo, A.; Bar, A.; Denes, A.; Bachar, M.; Kram, V.; Attar-Namdar, M.; Zallone, A.; Kovacs, K.J.; Yirmiya, R.; Bab, I. Skeletal parasympathetic innervation communicates central il-1 signals regulating bone mass accrual. Proc. Natl. Acad. Sci. USA 2012, 109, 15455–15460. [Google Scholar] [CrossRef]
- Ysander, M.; Branemark, R.; Olmarker, K.; Myers, R.R. Intramedullary osseointegration: Development of a rodent model and study of histology and neuropeptide changes around titanium implants. J. Rehabil. Res. Dev. 2001, 38, 183–190. [Google Scholar]
- Elefteriou, F. Neuronal signaling and the regulation of bone remodeling. Cell. Mol. Life Sci. 2005, 62, 2339–2349. [Google Scholar] [CrossRef]
- Chenu, C. Role of innervation in the control of bone remodeling. J. Musculoskelet. Neuronal Interact. 2004, 4, 132–134. [Google Scholar]
- Jiang, S.D.; Jiang, L.S.; Dai, L.Y. Mechanisms of osteoporosis in spinal cord injury. Clin. Endocrinol. 2006, 65, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Corpas Ldos, S.; Lambrichts, I.; Quirynen, M.; Collaert, B.; Politis, C.; Vrielinck, L.; Martens, W.; Struys, T.; Jacobs, R. Peri-implant bone innervation: Histological findings in humans. Eur J. Oral Implants 2014, 7, 283–292. [Google Scholar]
- Fujii, N.; Ohnishi, H.; Shirakura, M.; Nomura, S.; Ohshima, H.; Maeda, T. Regeneration of nerve fibres in the peri-implant epithelium incident to implantation in the rat maxilla as demonstrated by immunocytochemistry for protein gene product 9.5 (pgp9.5) and calcitonin gene-related peptide (cgrp). Clin. Oral Implants Res. 2003, 14, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.G.; Holland, G.R. The reinnervation of healing extraction sockets in the ferret. J. Dent. Res. 1993, 72, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Wada, S.; Kojo, T.; Wang, Y.H.; Ando, H.; Nakanishi, E.; Zhang, M.; Fukuyama, H.; Uchida, Y. Effect of loading on the development of nerve fibers around oral implants in the dog mandible. Clin. Oral Implants Res. 2001, 12, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-H.; Kojo, T.; Ando, H.; Nakanishi, E.; Yoshizawa, H.; Zhang, M.; Fukuyama, H.; Wada, S.; Uchida, Y. Nerve regeneration after implantation in peri-implant area. A histological study on different implant materials in dogs. In Osseoperception; Jacobs, R., Ed.; Catholic University Leuven: Leuven, Belgium, 1998; pp. 3–11. [Google Scholar]
- Elefteriou, F.; Campbell, P.; Ma, Y. Control of bone remodeling by the peripheral sympathetic nervous system. Calcif. Tissue Int. 2014, 94, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [PubMed]
- Kinjo, M.; Setoguchi, S.; Schneeweiss, S.; Solomon, D.H. Bone mineral density in subjects using central nervous system-active medications. Am. J. Med. 2005, 118, 1414.e7–1414.e12. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors influencing early dental implant failures. J. Dent. Res. 2016, 95, 995–1002. [Google Scholar] [CrossRef]
- Gupta, B.; Acharya, A.; Pelekos, G.; Gopalakrishnan, D.; Kolokythas, A. Selective serotonin reuptake inhibitors and dental implant failure-a significant concern in elders? Gerodontology 2017, 34, 505–507. [Google Scholar] [CrossRef]
- Wu, X.; Al-Abedalla, K.; Rastikerdar, E.; Abi Nader, S.; Daniel, N.G.; Nicolau, B.; Tamimi, F. Selective serotonin reuptake inhibitors and the risk of osseointegrated implant failure: A cohort study. J. Dent. Res. 2014, 93, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Olney, R.C. Regulation of bone mass by growth hormone. Med. Pediatric Oncol.. 2003, 41, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V. Bone healing the diamond concept. In European Instructional Lectures: 15th EFORT Congress, London, United Kingdom; Bentley, G., Ed.; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar] [CrossRef]
- Malloy, K.A.; Wadhwani, C.; McAllister, B.; Wang, M.; Katancik, J.A. Accuracy and reproducibility of radiographic images for assessing crestal bone height of implants using the precision implant X-ray locator (pixrl) device. Int J. Oral Maxillofac. Implants 2017, 32, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Bohner, L.O.L.; Mukai, E.; Oderich, E.; Porporatti, A.L.; Pacheco-Pereira, C.; Tortamano, P.; De Luca Canto, G. Comparative analysis of imaging techniques for diagnostic accuracy of peri-implant bone defects: A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, 432.e5–440.e5. [Google Scholar] [CrossRef] [PubMed]
- Wakoh, M.; Harada, T.; Otonari, T.; Otonari-Yamamoto, M.; Ohkubo, M.; Kousuge, Y.; Kobayashi, N.; Mizuta, S.; Kitagawa, H.; Sano, T. Reliability of linear distance measurement for dental implant length with standardized periapical radiographs. Bull. Tokyo Dent. Coll. 2006, 47, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Daros, P.; Carneiro, V.C.; Siqueira, A.P.; de-Azevedo-Vaz, S.L. Diagnostic accuracy of 4 intraoral radiographic techniques for misfit detection at the implant abutment joint. J. Prosthet. Dent. 2018, 120, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Duckworth, J.E.; Judy, P.F.; Goodson, J.M.; Socransky, S.S. A method for the geometric and densitometric standardization of intraoral radiographs. J. Periodontol. 1983, 54, 435–440. [Google Scholar] [CrossRef]
- Lin, K.C.; Wadhwani, C.P.; Cheng, J.; Sharma, A.; Finzen, F. Assessing fit at the implant-abutment junction with a radiographic device that does not require access to the implant body. J. Prosthet. Dent. 2014, 112, 817–823. [Google Scholar] [CrossRef]
- Grondahl, K.; Sunden, S.; Grondahl, H.G. Inter- and intraobserver variability in radiographic bone level assessment at Branemark fixtures. Clin. Oral Implants Res. 1998, 9, 243–250. [Google Scholar] [CrossRef]
- Morner-Svalling, A.C.; Tronje, G.; Andersson, L.G.; Welander, U. Comparison of the diagnostic potential of direct digital and conventional intraoral radiography in the evaluation of peri-implant conditions. Clin. Oral Implants Res. 2003, 14, 714–719. [Google Scholar] [CrossRef]
- Kamburoglu, K.; Gulsahi, A.; Genc, Y.; Paksoy, C.S. A comparison of peripheral marginal bone loss at dental implants measured with conventional intraoral film and digitized radiographs. J. Oral Implants 2012, 38, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Sewerin, I.P.; Gotfredsen, K.; Stoltze, K. Accuracy of radiographic diagnosis of peri-implant radiolucencies--an in vitro experiment. Clin. Oral Implants Res. 1997, 8, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Dave, M.; Davies, J.; Wilson, R.; Palmer, R. A comparison of cone beam computed tomography and conventional periapical radiography at detecting peri-implant bone defects. Clin. Oral Implants Res. 2013, 24, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Pini Prato, G.; Williams, R.C.; Cortellini, P. Periodontal regeneration of human infrabony defects. Iii. Diagnostic strategies to detect bone gain. J. Periodontol. 1993, 64, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Eickholz, P.; Hausmann, E. Accuracy of radiographic assessment of interproximal bone loss in intrabony defects using linear measurements. Eur. J. Oral Sci. 2000, 108, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, M.; Mir-Mari, J.; Benic, G.I.; Figueiredo, R.; Valmaseda-Castellon, E. Accuracy of periapical radiography in assessing bone level in implants affected by peri-implantitis: A cross-sectional study. J. Clin. Periodontol. 2016, 43, 85–91. [Google Scholar] [CrossRef]
- Hermann, J.S.; Schoolfield, J.D.; Nummikoski, P.V.; Buser, D.; Schenk, R.K.; Cochran, D.L. Crestal bone changes around titanium implants: A methodologic study comparing linear radiographic with histometric measurements. Int. J. Oral Maxillofac. Implants 2001, 16, 475–485. [Google Scholar]
- Schwarz, F.; Herten, M.; Sager, M.; Bieling, K.; Sculean, A.; Becker, J. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. Clin. Oral Implants Res. 2007, 18, 161–170. [Google Scholar] [CrossRef]
- Schwarz, F.; Sahm, N.; Schwarz, K.; Becker, J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J. Clin. Periodontol. 2010, 37, 449–455. [Google Scholar] [CrossRef]
- Demirturk Kocasarac, H.; Helvacioglu Yigit, D.; Bechara, B.; Sinanoglu, A.; Noujeim, M. Contrast-to-noise ratio with different settings in a cbct machine in presence of different root-end filling materials: An in vitro study. Dentomaxillofac. Radiol. 2016, 45, 20160012. [Google Scholar] [CrossRef]
- Sirin, Y.; Horasan, S.; Yaman, D.; Basegmez, C.; Tanyel, C.; Aral, A.; Guven, K. Detection of crestal radiolucencies around dental implants: An in vitro experimental study. J. Oral Maxillofac. Surg. 2012, 70, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Fienitz, T.; Schwarz, F.; Ritter, L.; Dreiseidler, T.; Becker, J.; Rothamel, D. Accuracy of cone beam computed tomography in assessing peri-implant bone defect regeneration: A histologically controlled study in dogs. Clin. Oral Implants Res. 2012, 23, 882–887. [Google Scholar] [CrossRef] [PubMed]
- De-Azevedo-Vaz, S.L.; Alencar, P.N.; Rovaris, K.; Campos, P.S.; Haiter-Neto, F. Enhancement cone beam computed tomography filters improve in vitro periimplant dehiscence detection. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Neves, F.S.; Vasconcelos, T.V.; Campos, P.S.; Haiter-Neto, F.; Freitas, D.Q. Influence of scan mode (180 degrees/360 degrees) of the cone beam computed tomography for preoperative dental implant measurements. Clin. Oral Implants Res. 2014, 25, e155–e158. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, L.R.; Scarfe, W.C.; Augusto de Oliveira Sales, M.; Gaia, B.F.; Cortes, A.R.; Cavalcanti, M.G. Effect of cone-beam computed tomography field of view and acquisition frame on the detection of chemically simulated peri-implant bone loss in vitro. J. Periodontol. 2015, 86, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Al-Nuaimi, N.; Patel, S.; Foschi, F.; Mannocci, F. The detection of simulated periapical lesions in human dry mandibles with cone-beam computed tomography: A dose reduction study. Int. Endod. J. 2016, 49, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Pelekos, G.; Acharya, A.; Tonetti, M.S.; Bornstein, M.M. Diagnostic performance of cone beam computed tomography in assessing peri-implant bone loss: A systematic review. Clin. Oral Implants Res. 2018, 29, 443–464. [Google Scholar] [CrossRef]
- Mengel, R. Kruse, B. Flores-de-Jacoby, L. Digital volume tomography in the diagnosis of peri-implant defects: An in vitro study on native pig mandibles. J. Periodontol. 2006, 77, 1234–1241. [Google Scholar] [CrossRef]
- Ritter, L.; Elger, M.C.; Rothamel, D.; Fienitz, T.; Zinser, M.; Schwarz, F.; Zoller, J.E. Accuracy of peri-implant bone evaluation using cone beam ct, digital intra-oral radiographs and histology. Dentomaxillofac. Radiol. 2014, 43, 20130088. [Google Scholar] [CrossRef]
- Fleiner, J.; Hannig, C.; Schulze, D.; Stricker, A.; Jacobs, R. Digital method for quantification of circumferential periodontal bone level using cone beam ct. Clin. Oral Investig. 2013, 17, 389–396. [Google Scholar] [CrossRef]
- Kuhl, S.; Zurcher, S.; Zitzmann, N.U.; Filippi, A.; Payer, M.; Dagassan-Berndt, D. Detection of peri-implant bone defects with different radiographic techniques—A human cadaver study. Clin. Oral Implants Res. 2016, 27, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Tyndall, D.A.; Price, J.B.; Tetradis, S.; Ganz, S.D.; Hildebolt, C.; Scarfe, W.C. Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology with emphasis on cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Sinjab, K.; Li, J.; Chen, Z.; Wang, H.L.; Kripfgans, O.D. Ultrasonography for noninvasive and real-time evaluation of peri-implant tissue dimensions. J. Clin. Periodontol. 2018, 45, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Bloch, S.H.; Dayton, P.A.; Ferrara, K.W. Targeted imaging using ultrasound contrast agents. IEEE Eng. Med. Biol. Mag. 2004, 23, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Marotti, J.; Heger, S.; Tinschert, J.; Tortamano, P.; Chuembou, F.; Radermacher, K.; Wolfart, S. Recent advances of ultrasound imaging in dentistry—A review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 819–832. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.V.; Hu, S. Photoacoustic Tomography: In Vivo Imaging from Organelles to Organs. Science 2012, 335, 1458–1462. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Wang, L.V. Photoacoustic imaging in biomedicine. Rev. Sci. Instrum. 2006, 77, 041101. [Google Scholar] [CrossRef]
- Hariri, A.; Lemaster, J.; Wang, J.; Jeevarathinam, A.S.; Chao, D.L.; Jokerst, J.V. The characterization of an economic and portable LED-based photoacoustic imaging system to facilitate molecular imaging. Photoacoustics 2018, 9, 10–20. [Google Scholar] [CrossRef]
- Asao, Y.; Hashizume, Y.; Suita, T.; Nagae, K.-I.; Fukutani, K.; Sudo, Y.; Matsushita, T.; Kobayashi, S.; Tokiwa, M.; Yamaga, I.; et al. Photoacoustic mammography capable of simultaneously acquiring photoacoustic and ultrasound images. J. Biomed. Opt. 2016, 21, 116009. [Google Scholar] [CrossRef]
- Mozaffarzadeh, M.; Hariri, A.; Moore, C.; Jokerst, J.V. The double-stage delay-multiply-and-sum image reconstruction method improves imaging quality in a LED-based photoacoustic array scanner. Photoacoustics 2018, 12, 22–29. [Google Scholar] [CrossRef]
- Hoelen, C.; de Mul, F.; Pongers, R.; Dekker, A. Three-dimensional photoacoustic imaging of blood vessels in tissue. Opt. Lett. 1998, 23, 648–650. [Google Scholar] [CrossRef] [PubMed]
- Köstli, K.P.; Beard, P.C. Two-dimensional photoacoustic imaging by use of Fourier-transform image reconstruction and a detector with an anisotropic response. Appl. Opt. 2003, 42, 1899–1908. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Wang, L.V. Universal back-projection algorithm for photoacoustic computed tomography. Phys. Rev. E 2005, 71, 016706. [Google Scholar] [CrossRef] [PubMed]
- Lovell, J.F.; Liu, T.W.; Chen, J.; Zheng, G. Activatable photosensitizers for imaging and therapy. Chem. Rev. 2010, 110, 2839–2857. [Google Scholar] [CrossRef] [PubMed]
- Hariri, A.; Wang, J.; Kim, Y.; Jhunjhunwala, A.; Chao, D.L.; Jokerst, J.V. In vivo photoacoustic imaging of chorioretinal oxygen gradients. J. Biomed. Opt. 2018, 23, 036005. [Google Scholar] [CrossRef] [PubMed]
- Luke, G.P.; Emelianov, S.Y. Label-free Detection of Lymph Node Metastases with US-guided Functional Photoacoustic Imaging. Radiology 2015, 277, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Kircher, M.F.; de la Zerda, A.; Jokerst, J.V.; Zavaleta, C.L.; Kempen, P.J.; Mittra, E.; Pitter, K.; Huang, R.; Campos, C.; Habte, F.; et al. A Brain Tumor Molecular Imaging Strategy Using A New Triple-Modality MRI-Photoacoustic-Raman Nanoparticle. Nat. Med. 2012, 18, 829–834. [Google Scholar] [CrossRef]
- Guan, T.; Shang, W.; Li, H.; Yang, X.; Fang, C.; Tian, J.; Wang, K. From Detection to Resection: Photoacoustic Tomography and Surgery Guidance with Indocyanine Green Loaded Gold Nanorod@liposome Core–Shell Nanoparticles in Liver Cancer. Bioconjugate Chem. 2017, 28, 1221–1228. [Google Scholar] [CrossRef]
- Wang, J.; Chen, F.; Arconada-Alvarez, S.J.; Hartanto, J.; Yap, L.-P.; Park, R.; Wang, F.; Vorobyova, I.; Dagliyan, G.; Conti, P.S. A Nanoscale Tool for Photoacoustic-based Measurements of Clotting Time and Therapeutic Drug Monitoring of Heparin. Nano Lett. 2016, 16, 6265–6271. [Google Scholar] [CrossRef]
- Cash, K.J.; Li, C.; Xia, J.; Wang, L.V.; Clark, H.A. Optical Drug Monitoring: Photoacoustic Imaging of Nanosensors to Monitor Therapeutic Lithium in Vivo. ACS Nano 2015, 9, 1692–1698. [Google Scholar] [CrossRef]
- Zackrisson, S.; van de Ven, S.; Gambhir, S. Light in and sound out: Emerging translational strategies for photoacoustic imaging. Cancer Res. 2014, 74, 979–1004. [Google Scholar] [CrossRef] [PubMed]
- Luke, G.P.; Yeager, D.; Emelianov, S.Y. Biomedical applications of photoacoustic imaging with exogenous contrast agents. Ann. Biomed. Eng. 2012, 40, 422–437. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, A.; Hefti, A.F. Defining periodontal health. BMC Oral Health 2015, 15, S6. [Google Scholar] [CrossRef] [PubMed]
- Perry, D.A.; Beemsterboer, P.; Essex, G. Periodontology for the Dental Hygienist, 4th ed.; Elsevier/Saunders: St. Louis, MO, USA, 2014. [Google Scholar]
- Araujo, M.W.; Benedek, K.M.; Benedek, J.R.; Grossi, S.G.; Dorn, J.; Wactawski-Wende, J.; Genco, R.J.; Trevisan, M. Reproducibility of probing depth measurements using a constant-force electronic probe: Analysis of inter-and intraexaminer variability. J. Periodontol. 2003, 74, 1736–1740. [Google Scholar] [CrossRef]
- Larsen, C.; Barendregt, D.S.; Slot, D.E.; van der Velden, U.; van der Weijden, F. Probing pressure, a highly undervalued unit of measure in periodontal probing: A systematic review on its effect on probing pocket depth. J. Clin. Periodontol. 2009, 36, 315–322. [Google Scholar] [CrossRef]
- Biddle, A.J.; Palmer, R.M.; Wilson, R.F.; Watts, T.L. Comparison of the validity of periodontal probing measurements in smokers and non-smokers. J. Clin. Periodontol. 2001, 28, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Listgarten, M.A. Periodontal probing: What does it mean? J. Clin. Periodontol. 1980, 7, 165–176. [Google Scholar] [CrossRef]
- Holtfreter, B.; Albandar, J.M.; Dietrich, T.; Dye, B.A.; Eaton, K.A.; Eke, P.I.; Papapanou, P.N.; Kocher, T. Standards for reporting chronic periodontitis prevalence and severity in epidemiologic studies: Proposed standards from the Joint EU/USA Periodontal Epidemiology Working Group. J. Clin. Periodontol. 2015, 42, 407–412. [Google Scholar] [CrossRef]
- Karadottir, H.; Lenoir, L.; Barbierato, B.; Bogle, M.; Riggs, M.; Sigurdsson, T.; Crigger, M.; Egelberg, J. Pain experienced by patients during periodontal maintenance treatment. J. Periodontol. 2002, 73, 536–542. [Google Scholar] [CrossRef]
- Van Wijk, A.; Hoogstraten, J. Experience with dental pain and fear of dental pain. J. Dent. Res. 2005, 84, 947–950. [Google Scholar] [CrossRef]
- Cole, A.; McMichael, A. Audit of dental practice record-keeping: A PCT-coordinated clinical audit by Worcestershire dentists. Prim. Dent. Care 2009, 16, 85–93. [Google Scholar] [CrossRef] [PubMed]
- McFall, W.T., Jr.; Bader, J.D.; Rozier, R.G.; Ramsey, D. Presence of periodontal data in patient records of general practitioners. J. Periodontol. 1988, 59, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.G. Quality evaluation of clinical records of a group of general dental practitioners entering a quality assurance programme. Br. Dent. J. 2001, 191, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Schou, S.; Holmstrup, P.; Stoltze, K.; Hjørting-Hansen, E.; Fiehn, N.E.; Skovgaard, L.T. Probing around implants and teeth with healthy or inflamed peri-implant mucosa/gingiva: A histologic comparison in cynomolgus monkeys (Macaca fascicularis). Clin. Oral Implants Res. 2002, 13, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Koka, S. The implant-mucosal interface and its role in the long-term success of endosseous oral implants: A review of the literature. Int. J. Prosthodont. 1998, 11, 421–432. [Google Scholar] [PubMed]
- Rakic, M.; Galindo-Moreno, P.; Monje, A.; Radovanovic, S.; Wang, H.-L.; Cochran, D.; Sculean, A.; Canullo, L. How frequent does peri-implantitis occur? A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Giraldo, V.M.; Duque, A.; Aristizabal, A.G.; Hernández, R.D.M. Prevalence of Peri-implant Disease According to Periodontal Probing Depth and Bleeding on Probing: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implants 2018, 33, e89–e105. [Google Scholar] [CrossRef]
- Lin, C.; Chen, F.; Hariri, A.; Chen, C.; Wilder-Smith, P.; Takesh, T.; Jokerst, J. Photoacoustic Imaging for Noninvasive Periodontal Probing Depth Measurements. J. Dent. Res. 2018, 97, 23–30. [Google Scholar] [CrossRef]
- Moore, C.; Bai, Y.; Hariri, A.; Sanchez, J.B.; Lin, C.-Y.; Koka, S.; Sedghizadeh, P.; Chen, C.; Jokerst, J.V. Photoacoustic imaging for monitoring periodontal health: A first human study. Photoacoustics 2018, 12, 67–74. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Animal Model | Loading Pattern | Bone Resorption | Healing Period | Loading Period | Implant System |
|---|---|---|---|---|---|---|
| Isidor [9] | Monkey mandible | 10–300 N330 N/s for 5 days | Yes | 6 months | 4–15 months | Astra |
| Miyata et al. [10] | Monkey mandible | Supra-occlusal contact | Yes | 3.5 months | 4 weeks | Intra-mobile element (IMZ) |
| Heitz-Mayfield et al. [12] | Dog mandible | Supra-occlusal contact | No | 6 months | 8 months | Straumann |
| Esaki et al. [11] | Dog mandible | Immediate load | Yes | None | 3 weeks | Branemark |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naveau, A.; Shinmyouzu, K.; Moore, C.; Avivi-Arber, L.; Jokerst, J.; Koka, S. Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL). J. Clin. Med. 2019, 8, 166. https://doi.org/10.3390/jcm8020166
Naveau A, Shinmyouzu K, Moore C, Avivi-Arber L, Jokerst J, Koka S. Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL). Journal of Clinical Medicine. 2019; 8(2):166. https://doi.org/10.3390/jcm8020166
Chicago/Turabian StyleNaveau, Adrien, Kouhei Shinmyouzu, Colman Moore, Limor Avivi-Arber, Jesse Jokerst, and Sreenivas Koka. 2019. "Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL)" Journal of Clinical Medicine 8, no. 2: 166. https://doi.org/10.3390/jcm8020166
APA StyleNaveau, A., Shinmyouzu, K., Moore, C., Avivi-Arber, L., Jokerst, J., & Koka, S. (2019). Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL). Journal of Clinical Medicine, 8(2), 166. https://doi.org/10.3390/jcm8020166