1. Introduction
Campylobacters are among the most prevalent bacteria involved in acute diarrhea [
1]. The culture of
Campylobacter sp. can unfortunately be falsely negative in 10% to 30% of cases [
2] due to preanalytical and analytical factors. Clinical laboratories equipped with syndromic polymerase chain reaction (PCR) systems in the context of a bacterial infectious diarrhea diagnosis are tempted to use only selective agar for the pathogen(s) detected by PCR. The French National Reference Center for Campylobacters and Helicobacters (NRCCH) set up a collaboration with two diagnostic laboratories participating in its surveillance network, located in the French departments 25 (Doubs) (Laboratory CBM25) and 67 (Bas-Rhin) (Laboratory Bio67), using the BD MAX
TM Enteric Bacterial Panel PCR (Becton Dickinson, Le Pont de Claix, France) as a screening method before culture. These two laboratories perform
Campylobacter culture only on stools that are detected positive on the BD MAX
TM, leading to a negative culture in a few cases. Thus, the objective of the study was to verify the positive
Campylobacter sp. status of the stools negative by culture for the period from 4 January to 23 August 2018 and from 18 December 2017 to 30 June 2018 for Laboratories CBM25 and Bio67, respectively.
2. Materials and Methods
The two laboratories sent 77 samples to the NRCCH (53 Cary Blair transport medium tubes previously inoculated with rectal swabs received from Bio67 and 24 stools from CBM25) (patients with a sex ratio 0.52 and a mean age 46.9 year ± 24.9) that were found positive for
Campylobacter sp. on BD MAX
TM but negative by culture (see
Table 1 for culture conditions in each laboratory).
The presence of diarrhea and/or abdominal pain was reported for only 25 cases (32.5%). For the 52 remaining cases, no clinical symptoms were reported by the two participating laboratories. The aspect of the stools was reported for 48 samples (62.3%), among them 28 were loose stools, 15 liquid, 3 glairy and 3 bloody. Only 4 of the 77 patients (5.2%) were already on antibiotic treatment at the time of stool collection. Simultaneous detection of other enteropathogens was found for 5 patients only (6.5%): 1 Yersinia sp., 3 pathogenic Escherichia coli (1 enterotoxinogen, 2 enterohemorragic) and 1 threadworm.
All of the samples were stored at −80 °C and transported to the NRCCH on dry ice. Upon reception, samples were cultured directly on Campylosel agar (bioMérieux, Marcy l’Etoile, France) (50 µL of Cary Blair transport medium or 50 µL from stools diluted in 9 mL of saline water) and incubated for 72 h at 35 °C in a microaerobic atmosphere, as previously described [
3,
4], and after enrichment in Preston broth inoculated with either a nut of stools or 100 µL of liquid stool or Cary Blair transport medium (24 h at 35 °C before subculturing on trypticase soy agar enriched with horse blood (bioMérieux)). They did not undergo other freeze–thaw cycles.
DNA extraction was performed on the stored samples (500 µL of Cary Blair transport medium or 1 mL of a stool suspension in GXT Stool Stabilizer provided with the GXT Stool Extraction kit) (Hain Lifesciences, Nehren, Germany) at the NRCCH using an Arrow automation (NorDiag, Diasorin, Saluggia, Italy). Real-time PCR was then carried out to identify
Campylobacter jejuni, Campylobacter coli and
Campylobacter fetus using a LightCycler 2.0 (Roche Life Science, Indianapolis, IN, USA), as previously described [
5]. Further testing was performed with the commercially available RIDAGENE Bacterial Stool Panel (r-Biopharm, Darmstadt, Germany) on CFX96 (Biorad, Marnes-la-Coquette, France) according to the manufacturer’s protocol.
The data obtained using these two PCR formats were evaluated with respect to the cycle threshold (Ct) and fluorescence intensity values (FI) obtained on BD MAX
TM. The total number of BD MAX
TM Campylobacter sp. positives for each laboratory is indicated in
Table 1. The Ct and FI values obtained for 80 positive
Campylobacter sp. cases by culture were also provided by the two laboratories.
Statistical analyses were performed with GraphPad Prism 5.01 (GraphPad Software, Inc., La Jolla, CA, USA). The Mann–Whitney test was used as a nonparametric test to compare the distributions of two unmatched groups. Differences were considered significant when p was inferior to 0.05.
3. Results
The activity report and the analytical conditions used by the two laboratories for culturing
Campylobacters are summarized in
Table 1. In these laboratories the level of negative culture for a positive
Campylobacter PCR detection was 10.6% and 12.5% for CBM25 and Bio67 laboratories, respectively (
Table 1). During the time periods considered, the ratio of positive
Campylobacter sp. to positive PCR versus
Salmonella sp. was 423/7 and 227/13 for Bio67 and CMB25, respectively. These results confirm the wide prevalence of
Campylobacter sp. in acute community infectious diarrhea.
Culture of the 77 samples was also negative at the NRCCH. Thirty-three of the 77 samples (7 from stools and 26 from Cary Blair transport media) (42.9%) were positive with the two PCR formats tested (double-positive PCR cases) (30
C. jejuni and 3
C. coli), and 37 samples (15 from stools and 22 from Cary Blair transport media) (48%) remained negative with the two PCRs (double-negative PCR cases). Six samples were PCR positive with the RIDAGENE Bacterial Stool Panel only (7.8%) and 1 sample (1.3%) was positive with the in-house PCR only. No significant difference of Ct values was found between the stools and Cary Blair transport media (
Figure S1).
For the 33 double-positive samples, diarrhea was noticed in only 3 cases whereas no symptom was reported in the 30 remaining cases. Eight of these samples corresponded to loose stools, 1 glairy, 2 bloody, 8 liquid, and for the 14 remaining samples, the stool aspect was not reported.
For the 37 double-negative samples, diarrhea and/or abdominal pain were present in 17 patients whereas no symptom was reported in the 20 remaining cases. The majority of these samples corresponded to loose stools (n = 17), 1 glairy, 5 liquid, and for the 14 remaining samples, the stool aspect was not reported. None of the 37 double-negative samples corresponded to patients that were under antibiotic treatment.
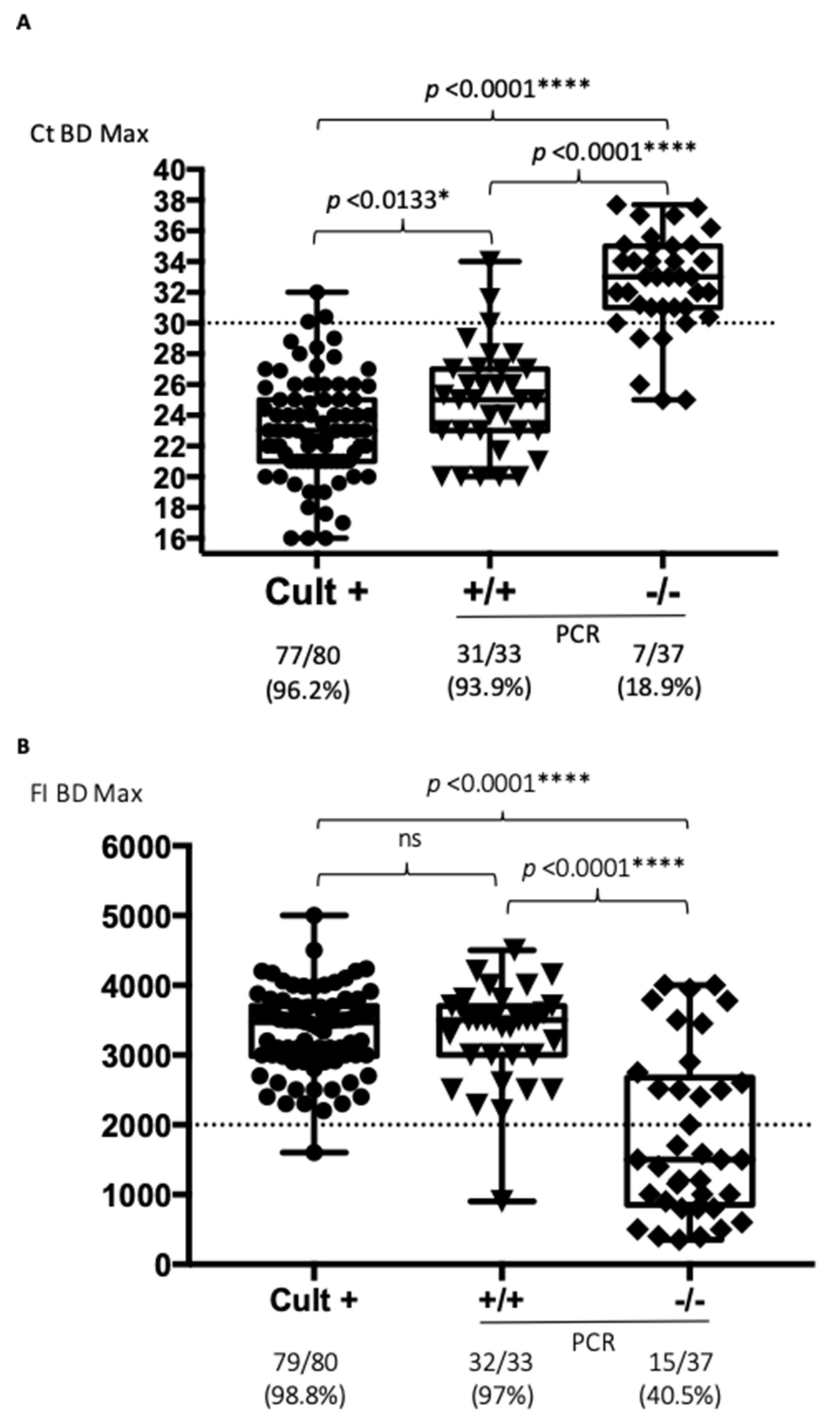
The Ct values initially obtained for
Campylobacter detection using the BD MAX
TM system for 31 of the 33 double-positive PCR samples were lower or equal to 30 cycles (93.9%), versus only 7 of the 37 double-negative PCR cases (18.9%) (
p < 0.0001) (
Figure 1A).
As a comparator, Ct values were also ≤30 in 77 out of 80 positive culture cases (96.2%) (
Figure 1A). It therefore seems that the Ct values may be a good indicator of the presence of
Campylobacter sp. detectable by culture or at least confirmed by two independent PCR formats. For the 80 positive culture cases, diarrhea was noticed in 58 cases; 1 patient had abdominal pain, whereas unfortunately no symptom was reported in the 21 remaining cases. Most of them (
n = 34) corresponded to liquid stools, 19 loose stools, 8 glairy samples; 2 bloody stools and for the 17 remaining samples, the stool aspect was not reported.
The same analyses were performed based on the FI values obtained on the BD MAX
TM system. The FI values were higher than 2000 units in 32 of the 33 double-positive cases (97%), but also in 15 of the 37 double-negative cases (40.5%) (
p < 0.0001) (
Figure 1B). Positive culture cases had an FI > 2000 in 79 out of 80 samples (98.8%). It therefore seems that FI values are less discriminatory than Ct values (
Figure 1B). No significant difference of FI values was found for the double-negative cases between the stools and Cary Blair transport media, whereas FI values were significantly higher in the 7 double-positive stools compared to the 22 Cary Blair transport media (
p = 0.0484) (
Figure S1).
4. Discussion
The BD MAX
TM Enteric Bacterial Panel PCR clearly improves the diagnosis of
Campylobacter sp. infections by enabling the laboratories to deliver fast and targeted results to their clinicians [
6,
7]. Syndromic approaches now replace the traditional research by culture. Culture is performed only in the case of a positive BD MAX
TM result. Thus, technicians examine only agar plates in which they are supposed to find the pathogen detected by PCR, which probably reinforces their vigilance in identifying suspicious colonies. This selective culture is, however, at the expense of pathogens not targeted by the chosen syndromic PCR kit.
The BD MAX
TM PCR gives relevant results concerning the detection of Campylobacters. Without a perfect gold standard such as a positive
Campylobacter sp. culture, only double-positive cases by two independent PCRs could be considered as true
Campylobacter sp. positives in case of negative culture [
2,
8,
9]. We did not find a perfect correlation between the
Campylobacter PCR results obtained on BD MAX
TM and the two independent PCR formats. Several factors could explain this: the extraction of DNA is not identical, the targets used are different, the detection limits can vary between the methods (see below), and the DNA may have been degraded by the presence of DNAse in the stool sample. All of these factors should be evaluated in a future study. According to the manufacturer, the mean detection limit of
Campylobacter detection by the RIDAGENE PCR is 2.1 × 10
4 CFU/mL and 8.5 × 10
5 CFU/mL for
C. jejuni and
C. coli, respectively (manufacturer data). For the BD MAX
TM system the mean detection limit for
C. jejuni is around 6.3 × 10
3 CFU/mL, and 1.5 × 10
3 CFU/mL for stools and Cary Blair, respectively. For
C. coli, it is around 1.4 × 10
4 CFU/mL, and 8.2 × 10
3 CFU/mL for stools and Cary Blair, respectively (manufacturer’s data). Our in-house
gyrA PCR was originally designed to identify
Campylobacter [
5]. Its ability to detect
Campylobacter in stools has never been evaluated.
The nature of the samples tested in the present study (either stools or swabs in Cary Blair transport media) has no influence on the
Campylobacter sp. detection, confirming that there is no influence of inoculum or inhibitory issues as suggested by others [
6]. Even if the preanalytical conditions were different between the two laboratories, the Ct values were significantly lower in the positive stools in culture. The most likely hypothesis is that these patients had a more abundant bacterial load in their digestive tract. This has already been suggested by the data published by Wholwend et al., where the authors showed that the median Ct values of culture-positive specimens were significantly lower than those of culture-negative specimens. [
10].
Nonetheless, PCRs only obtained using the BD MAX™ remained low, with 5.7% (37 samples) of all 650 samples tested in the two laboratories during the time period of the present study.
A limit of this study is its retrospective design, which did not allow to obtain clinical data for 52 of the 77 samples included in the analyses. Even if there were more loose stools in the double-negative cases compared to the double-positive cases, it could not be a good indicator of the presence of Campylobacter sp.
However, this study shows that 95.6% (108/113) of the Campylobacter sp. cases detected by culture or with the two reference PCRs were also positive on BD MAXTM with a Ct value ≤ 30; hence, stools that were positive on BD MAXTM with a Ct > 30 may possibly be false positives. In our study, this cut-off had a sensitivity of 93.9% and a specificity of 81%. The fact that the Ct threshold proposed in our study was valid for two independent laboratories is representative of its robustness. The integration of a quantitative control for adjusting Ct values to chromosomal equivalents could be of major interest.
5. Conclusions
In conclusion, it could be interesting to propose that laboratories using the BD MAXTM strategy for Campylobacter sp. diagnosis before culture, include a comment concerning the clinical interpretation and the therapeutic management of positive cases with Ct values > 30. This comment should alert the clinician of the risk of having no positive Campylobacter sp. culture, in which case the clinician should reconsider the need of giving empiric antimicrobial therapy. However, these results could be confirmed by a prospective study.
We recommend that this type of analysis should be carried out for other enteric pathogens and for other PCR formats.
Supplementary Materials
The following are available online at
https://www.mdpi.com/2077-0383/8/12/2138/s1, Figure S1: Stratification of Ct intensity and fluorescence values according to the nature of the samples (*
p < 0.05, ns: non-significant).
Author Contributions
Conceptualization, P.L.; Data curation, P.L.; Formal analysis, F.M., E.B. and P.L.; Methodology, T.G., M.C.P., A.B., J.M.R., M.L., L.B. and A.D.; Project administration, P.L.; Resources, T.G., M.C.P., A.T., M.L. and J.M.R.; Supervision, E.B., P.L.; Validation, E.B.; Writing—original draft, P.L.; Writing—review & editing, F.M., E.B. and P.L.
Funding
This work was supported by internal funding of the French National Reference Center for Campylobacters and Helicobacters.
Acknowledgments
The authors thank all the staff from the clinical laboratories, Bio67, Strasbourg, France and CBM25, Besançon, France.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kaakoush, N.O.; Castaño-Rodríguez, N.; Mitchell, H.M.; Man, S.M. Global Epidemiology of Campylobacter Infection. Clin. Microbiol. Rev. 2015, 28, 687–720. [Google Scholar] [CrossRef] [PubMed]
- Bessède, E.; Asselineau, J.; Perez, P.; Valdenaire, G.; Richer, O.; Lehours, P.; Mégraud, F. Evaluation of the Diagnostic Accuracy of Two Immunochromatographic Tests Detecting Campylobacter in Stools and Their Role in Campylobacter Infection Diagnosis. J. Clin. Microbiol. 2018, 56, e01567-17. [Google Scholar] [CrossRef] [PubMed]
- Bénéjat, L.; Sifré, E.; Domingues Martins, C.; Ducournau, A.; Buissonnière, A.; Bessède, E.; Mégraud, F.; Lehours, P. Epidemiologic cutoff values to separate wild-type from non-wild-type Campylobacter fetus to ciprofloxacin. Diagn. Microbiol. Infect. Dis. 2018, 92, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Sifré, E.; Salha, B.A.; Ducournau, A.; Floch, P.; Chardon, H.; Mégraud, F.; Lehours, P. EUCAST recommendations for antimicrobial susceptibility testing applied to the three main Campylobacter species isolated in humans. J. Microbiol. Methods 2015, 119, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Ménard, A.; Dachet, F.; Prouzet-Mauleon, V.; Oleastro, M.; Mégraud, F. Development of a real-time fluorescence resonance energy transfer PCR to identify the main pathogenic Campylobacter spp. Clin. Microbiol. Infect. 2005, 11, 281–287. [Google Scholar] [CrossRef] [PubMed][Green Version]
- DeBurger, B.; Hanna, S.; Powell, E.A.; Ventrola, C.; Mortensen, J.E. Utilizing BD MAXTM Enteric Bacterial Panel to Detect Stool Pathogens from Rectal Swabs. BMC Clin. Pathol. 2017, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Park, J.; Lee, H.K.; Yu, J.K.; Lee, G.D.; Park, K.G.; Oak, H.C.; Park, Y.-J. Comparative Evaluation of Seegene Allplex Gastrointestinal, Luminex xTAG Gastrointestinal Pathogen Panel, and BD MAX Enteric Assays for Detection of Gastrointestinal Pathogens in Clinical Stool Specimens. Arch. Pathol. Lab. Med. 2019, 143, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Asselineau, J.; Paye, A.; Bessède, E.; Perez, P.; Proust-Lima, C. Different latent class models were used and evaluated for assessing the accuracy of Campylobacter diagnostic tests: Overcoming imperfect reference standards? Epidemiol. Infect. 2018, 146, 1556–1564. [Google Scholar] [CrossRef] [PubMed]
- Harrington, S.M.; Buchan, B.W.; Doern, C.; Fader, R.; Ferraro, M.J.; Pillai, D.R.; Rychert, J.; Doyle, L.; Lainesse, A.; Karchmer, T.; et al. Multicenter evaluation of the BD max enteric bacterial panel PCR assay for rapid detection of Salmonella spp., Shigella spp., Campylobacter spp. (C. jejuni and C. coli), and Shiga toxin 1 and 2 genes. J. Clin. Microbiol. 2015, 53, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Wohlwend, N.; Tiermann, S.; Risch, L.; Risch, M.; Bodmer, T. Evaluation of a Multiplex Real-Time PCR Assay for Detecting Major Bacterial Enteric Pathogens in Fecal Specimens: Intestinal Inflammation and Bacterial Load Are Correlated in Campylobacter Infections. J. Clin. Microbiol. 2016, 54, 2262–2266. [Google Scholar] [CrossRef] [PubMed][Green Version]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).





{kind=link}