Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study



 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
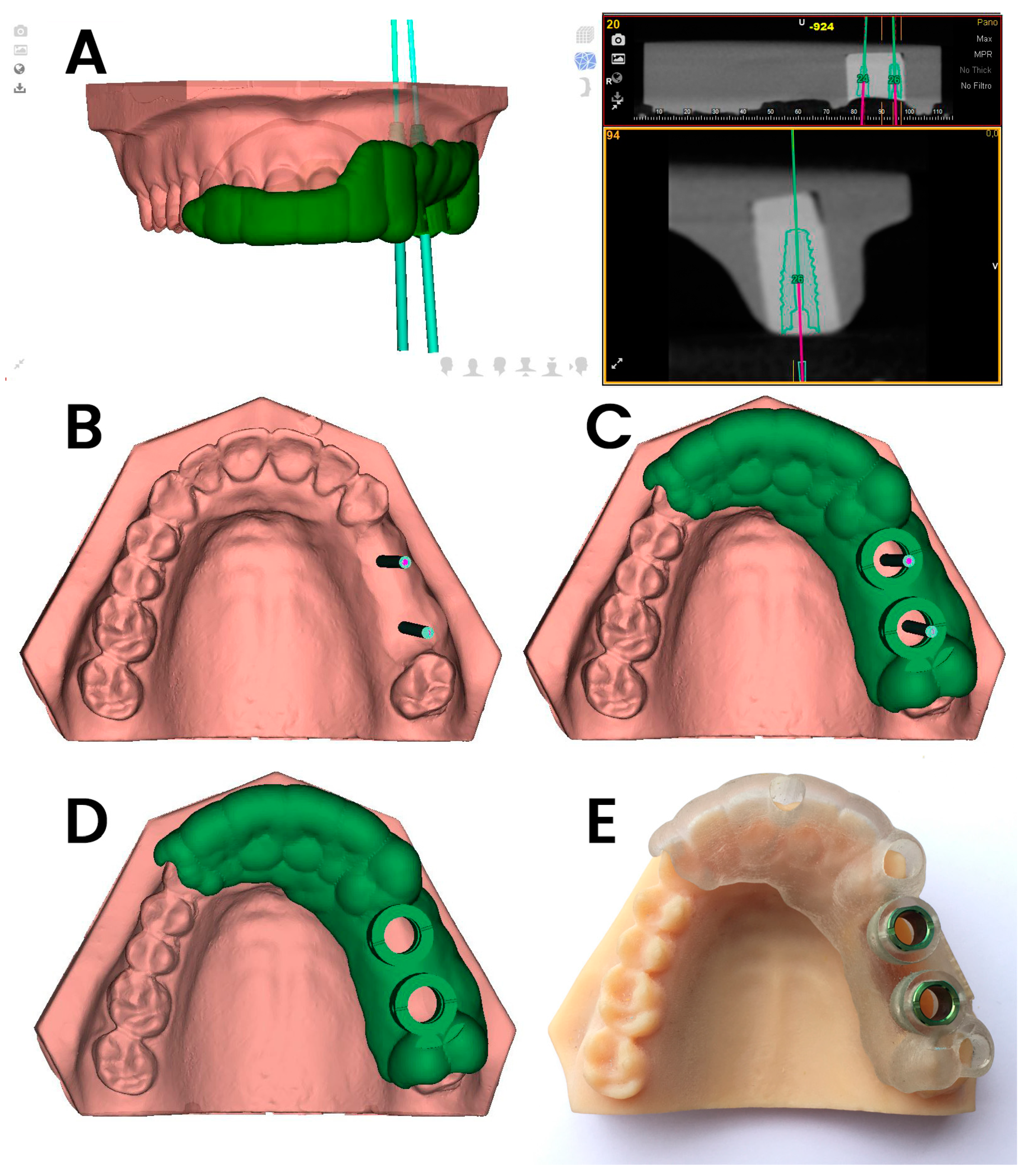
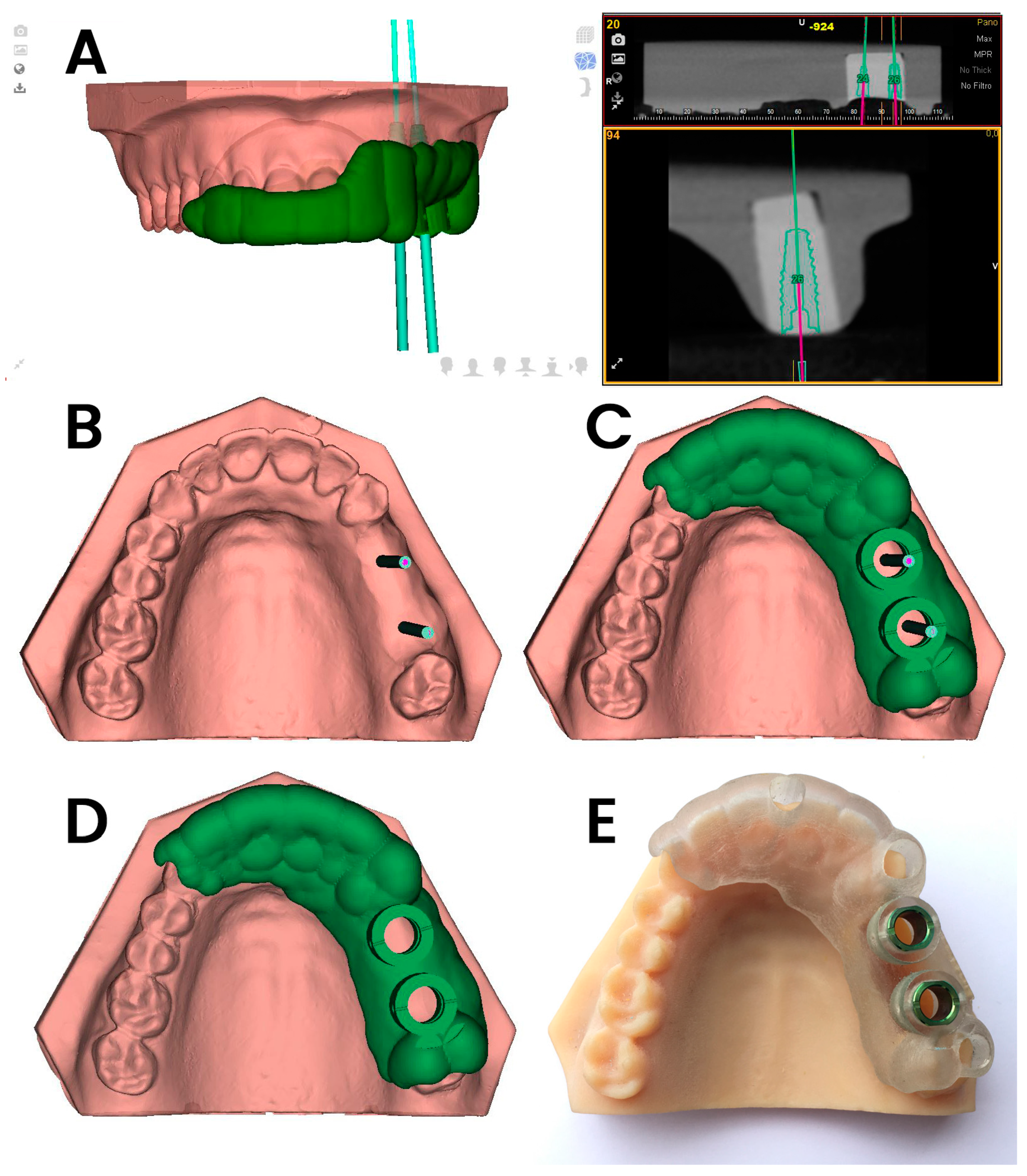
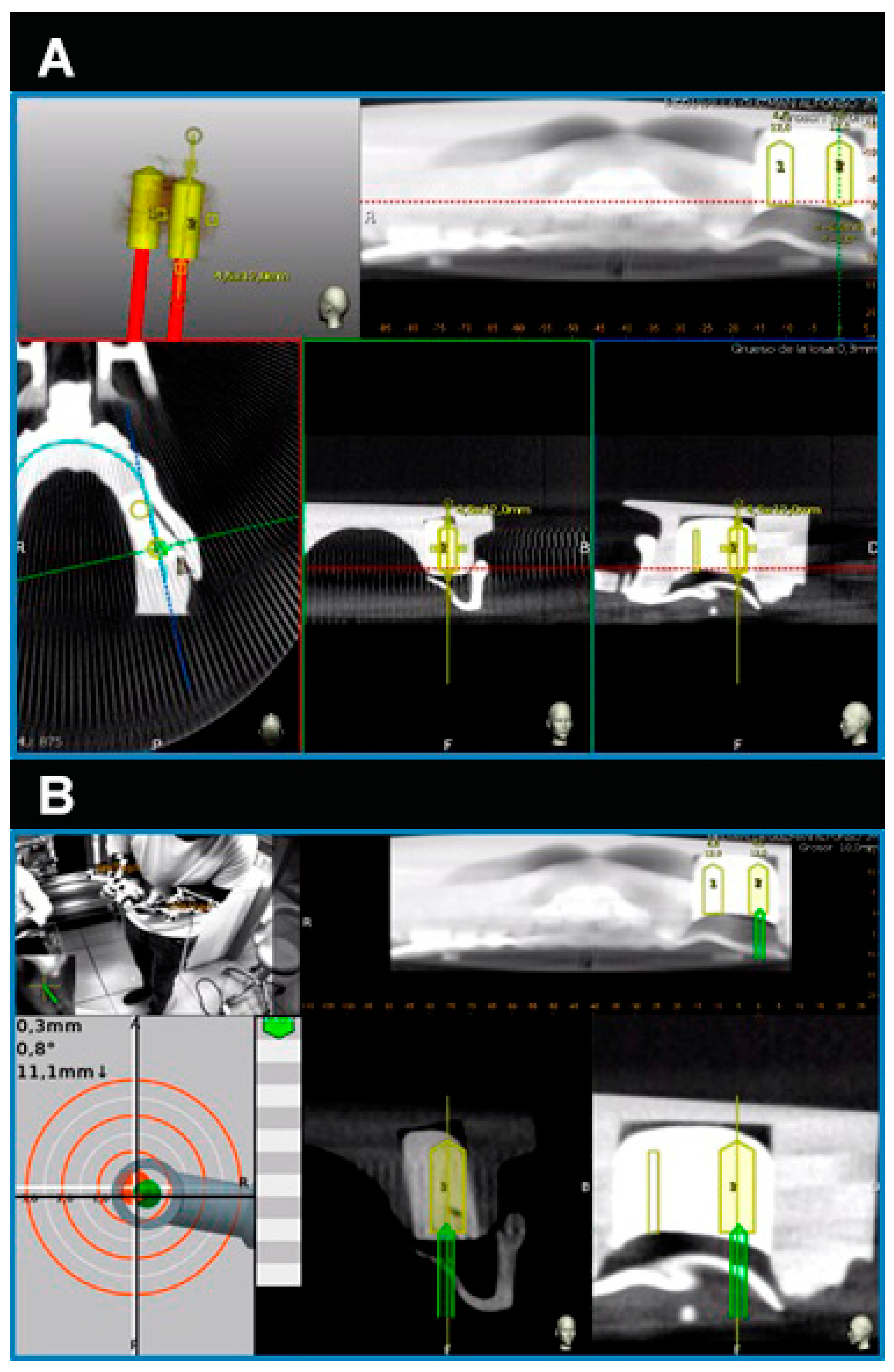
2.1. Study Design
2.2. Experimental Procedure
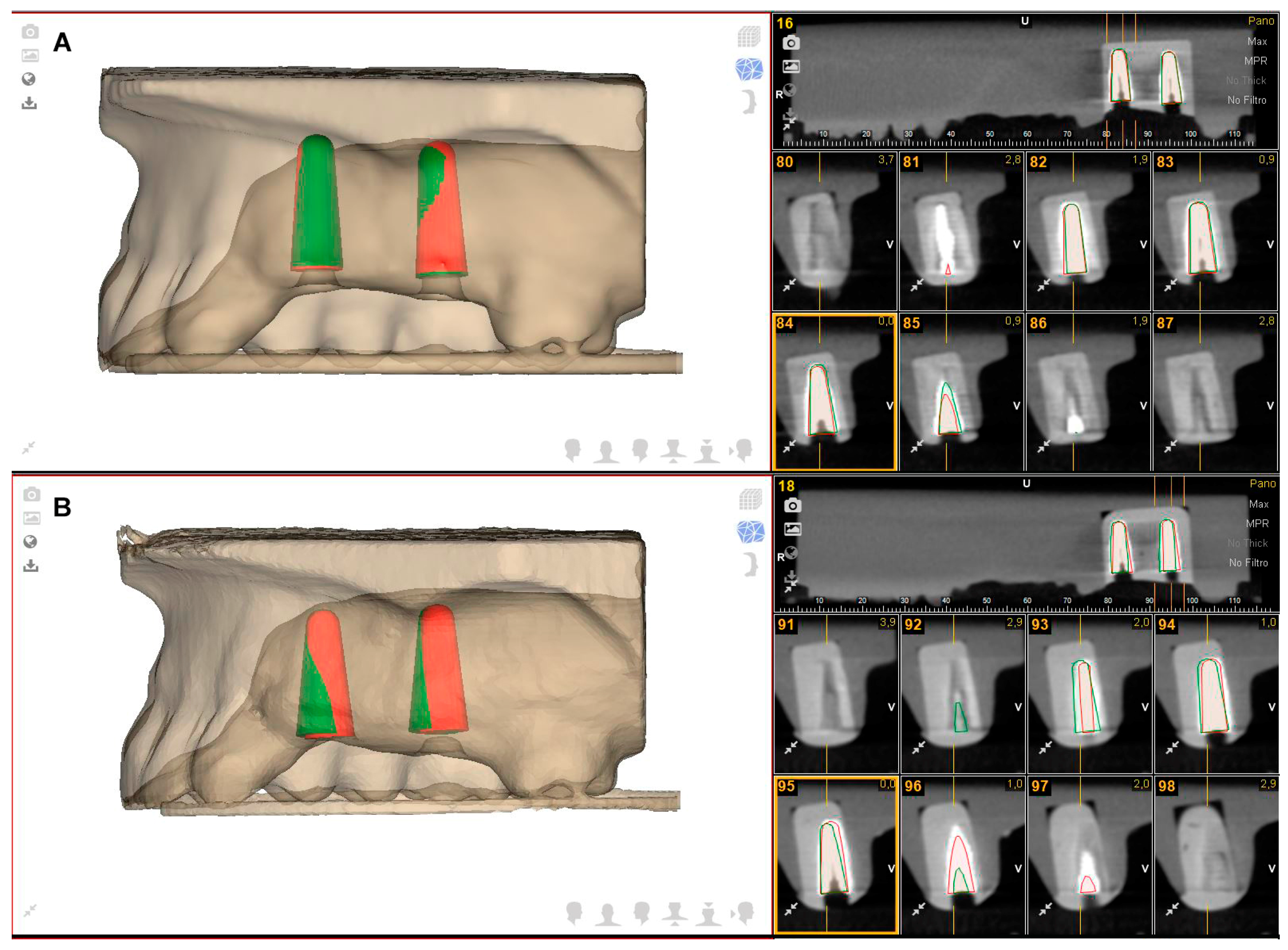
2.3. Measurement Procedure
2.4. Statistical Analysis
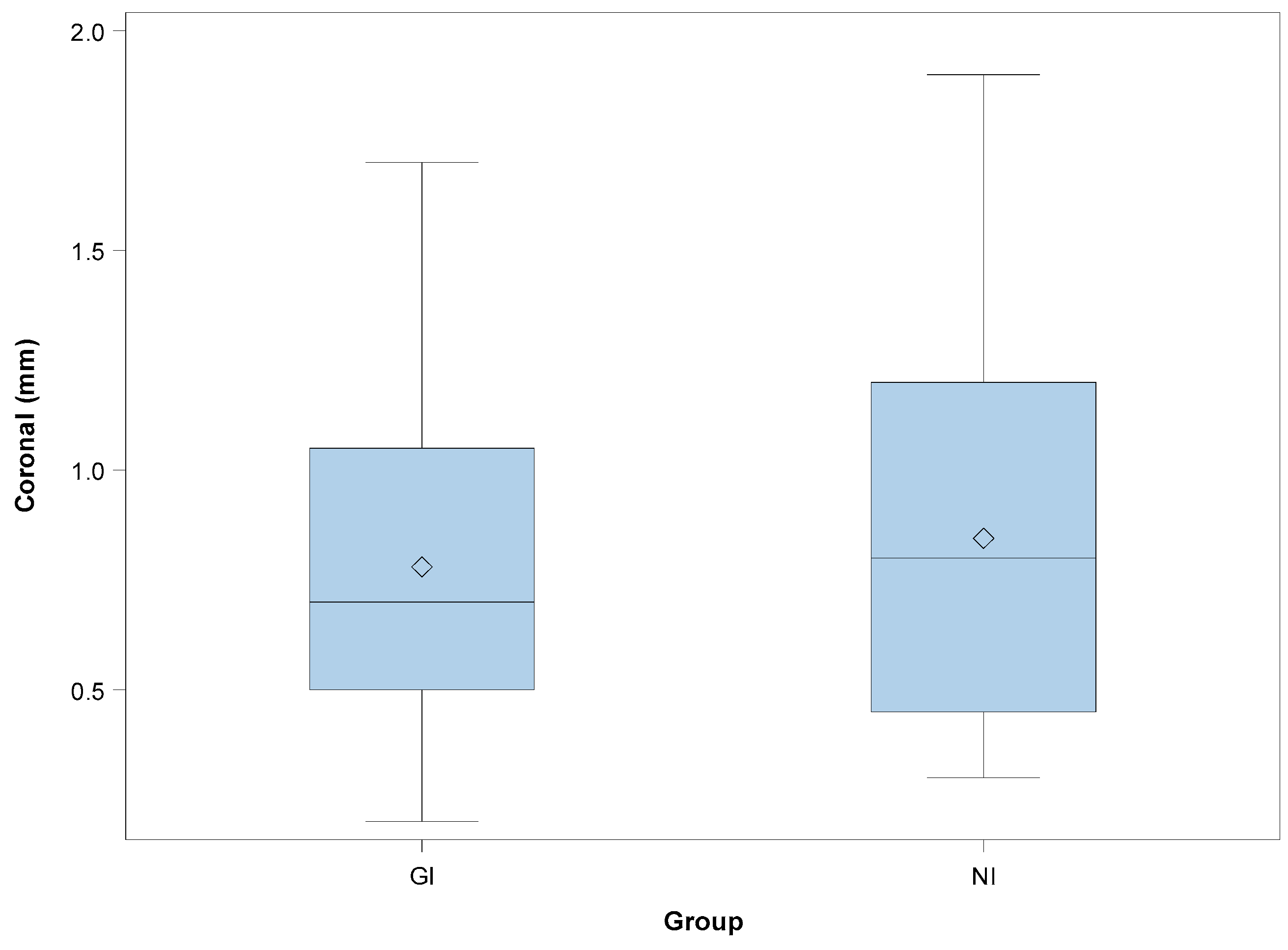
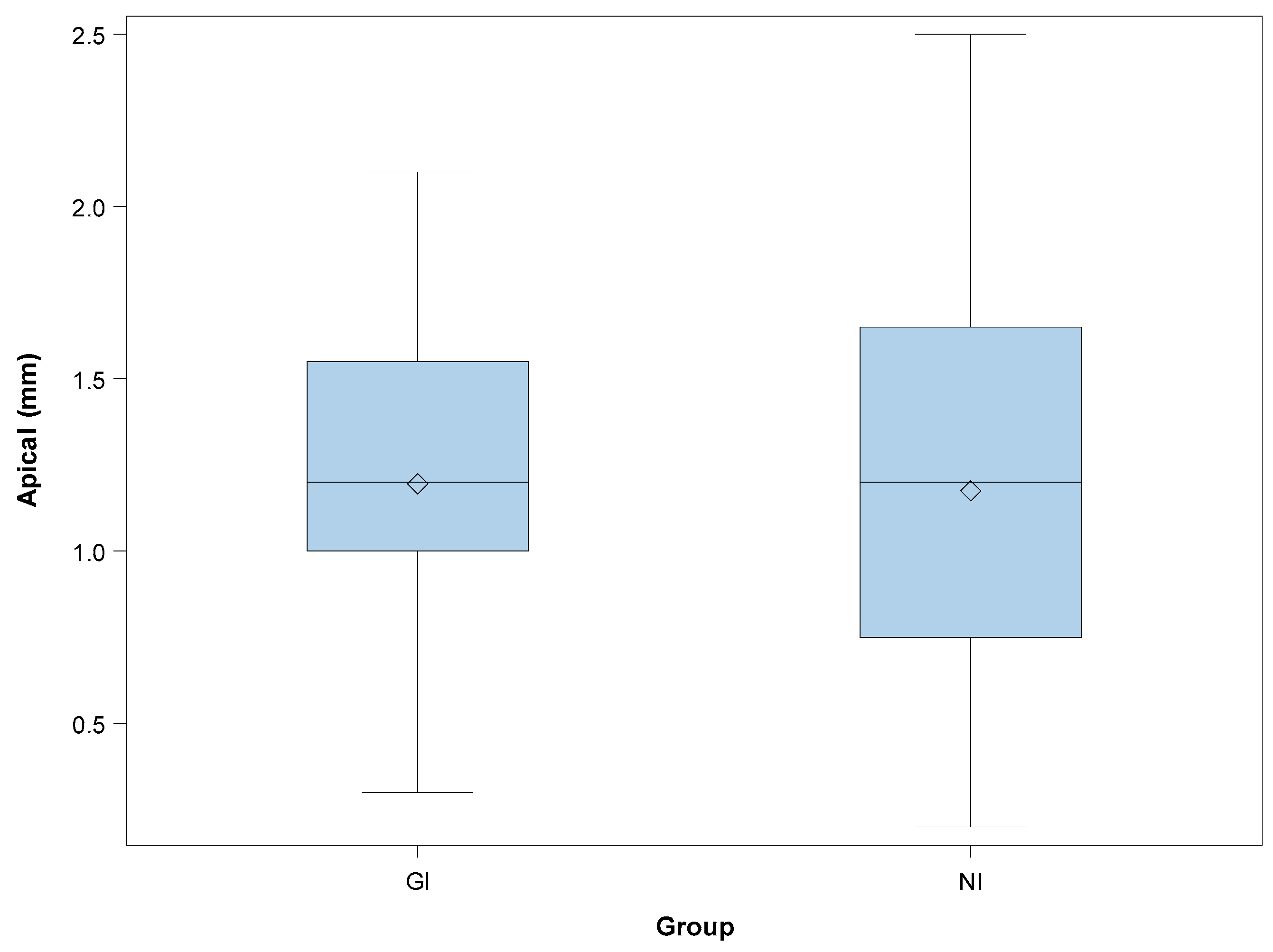
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaewsiri, D.; Panmekiate, S.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. The accuracy of static vs. dynamic computer-assited implant surgery in single tooth space: A randomized controlled trial. Clin. Oral Implants Res. 2019, 30, 505–514. [Google Scholar] [PubMed]
- Herklotz, I.; Beuer, F.; Kunz, A.; Hildebrand, D.; Happe, A. Navigation in implantology. Int. J. Comput. Dent. 2017, 20, 9–19. [Google Scholar] [PubMed]
- Widmann, G.; Bale, R.J. Accuracy in Computer-Aided Implant Surgery—A review. Int. J. Oral Maxillofac. Implants 2006, 21, 305–313. [Google Scholar] [PubMed]
- Chasioti, E.; Sayed, M.; Drew, H. Novel Techniques with the Aid of a Staged CBCT Guided Surgical Protocol. Case. Rep. Dent. 2015, 2015, 439706. [Google Scholar] [CrossRef] [PubMed]
- Lal, K.; White, G.S.; Morea, D.N.; Wright, R.F. Use of stereolithographic templates for surgical and prosthodontic implant planning and placement. Part II. A clinical report. J. Prosthodont. 2006, 15, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Jorba-García, A.; Figueiredo, R.; González-Barnadas, A.; Camps-Font, O.; Valmaseda-Castellón, E. Accuracy and the role of experience in dynamic computer guided dental implant surgery: An in-vitro study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, 76–83. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 16, 416–435. [Google Scholar] [CrossRef]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implants 2019, 34, 205–213. [Google Scholar] [CrossRef]
- Hoffmann, J.; Westendorff, C.; Gomez-Roman, G.; Reinert, S. Accuracy of navigation- guided socket drilling before implant installation compared to the conventional free-hand method in a synthetic edentulous lower jaw model. Clin. Oral Implants Res. 2005, 16, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Yuh, D.Y.; Huang, R.Y.; Fu, E.; Tsai, C.F.; Chiang, C.Y. Accuracy of implant placement with a navigation system, a laboratory guide, and freehand drilling. Int. J. Oral Maxillofac. Implants 2018, 33, 1213–1218. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Mangano, C.; Mangano, R.; Ferri, A.; Taraschi, V.; Marchetti, C. Augmented reality for dental implantology: A pilot clinical report of two cases. BMC Oral Health 2019, 19, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Gargallo-Albiol, J.; Barootchi, S.; Salomó-Coll, O.; Wang, H. Advantages and disadvantages of implant navigation surgery. A systematic review. Ann. Anat. 2019, 225, 1–10. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|
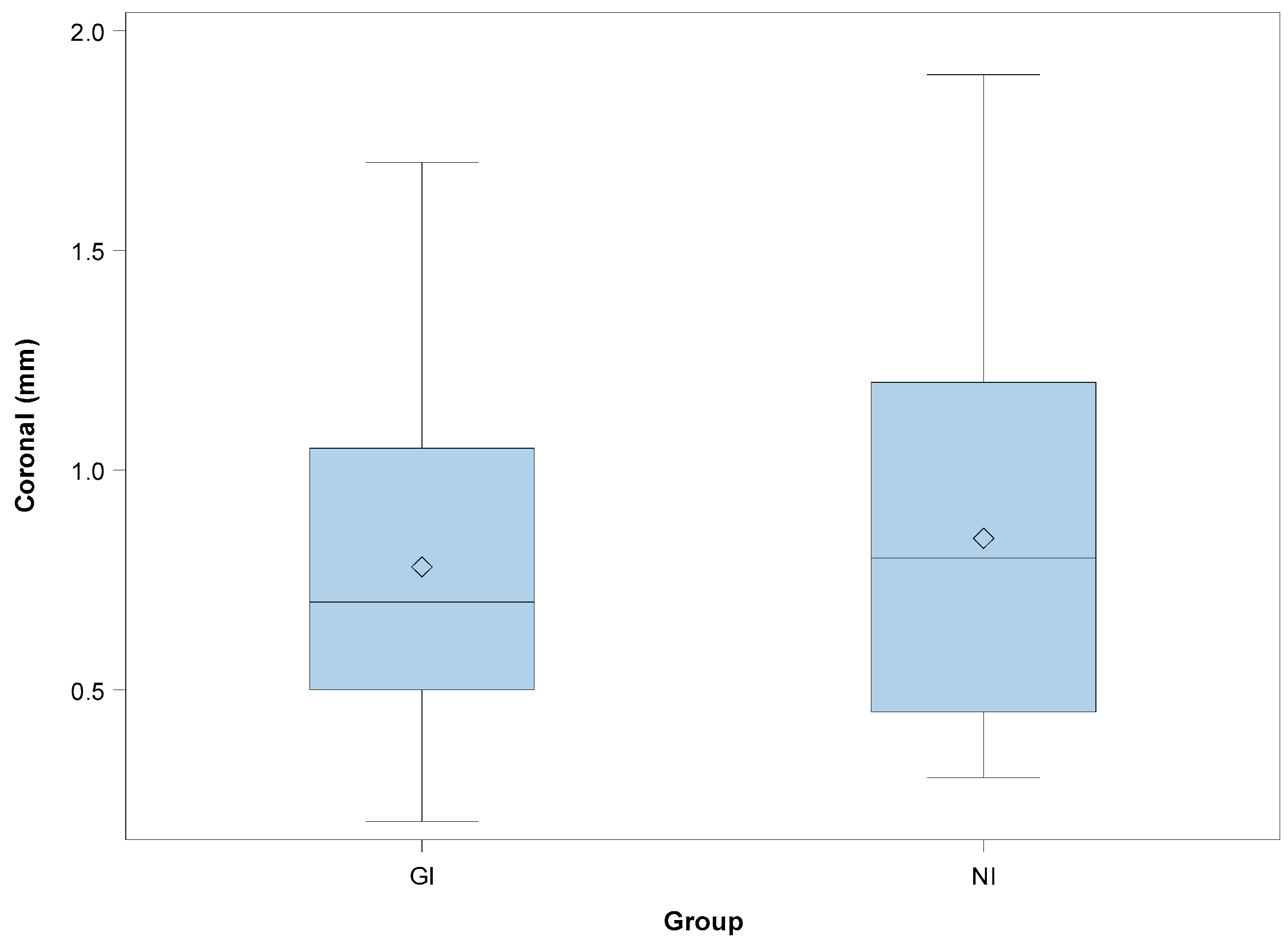
| CORONAL | GI | 20 | 0.78 | 0.43 | 0.20 | 1.70 |
| NI | 20 | 0.85 | 0.48 | 0.30 | 1.90 | |
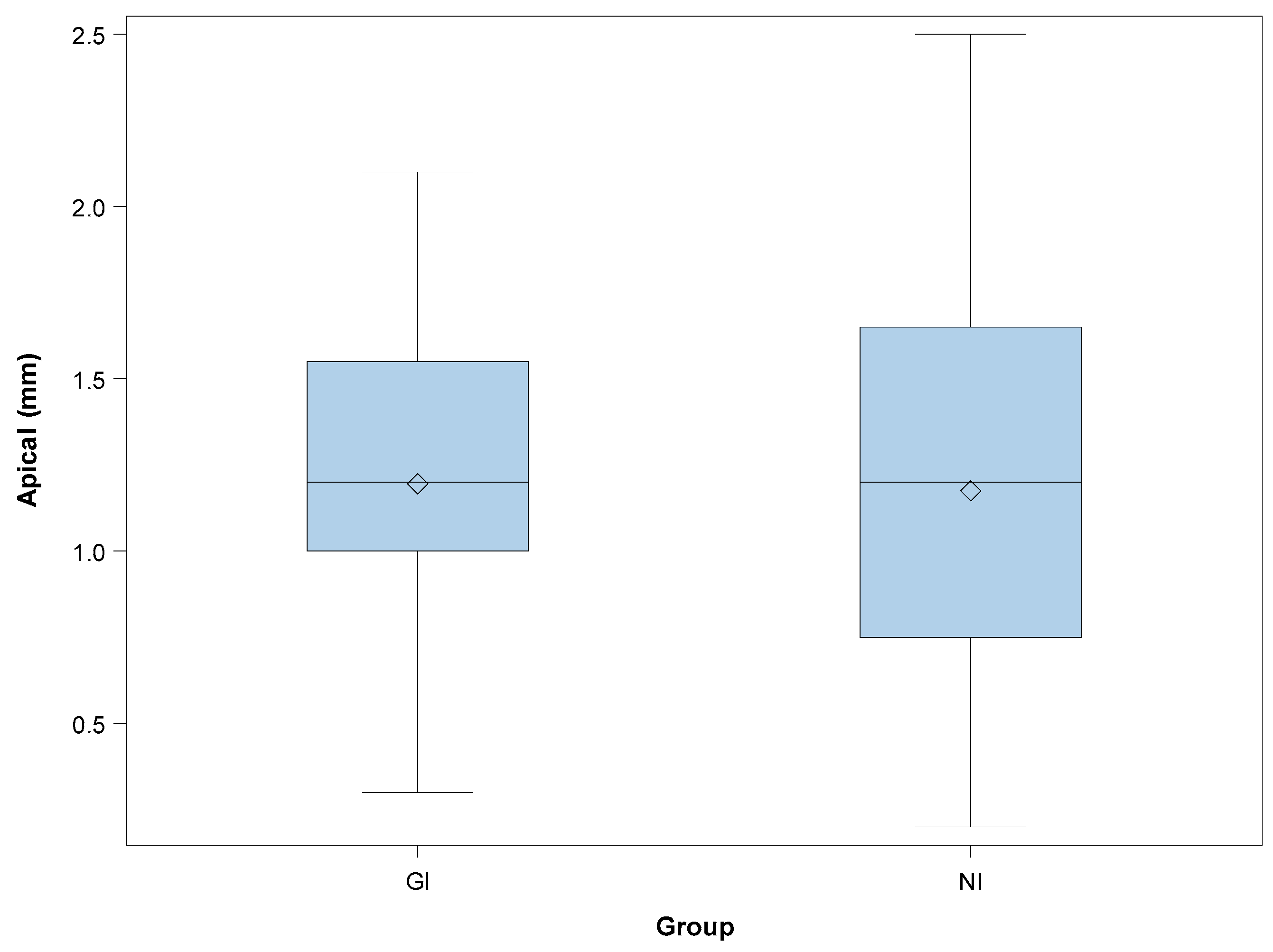
| APICAL | GI | 20 | 1.20 | 0.48 | 0.30 | 2.10 |
| NI | 20 | 1.18 | 0.60 | 0.20 | 2.50 | |
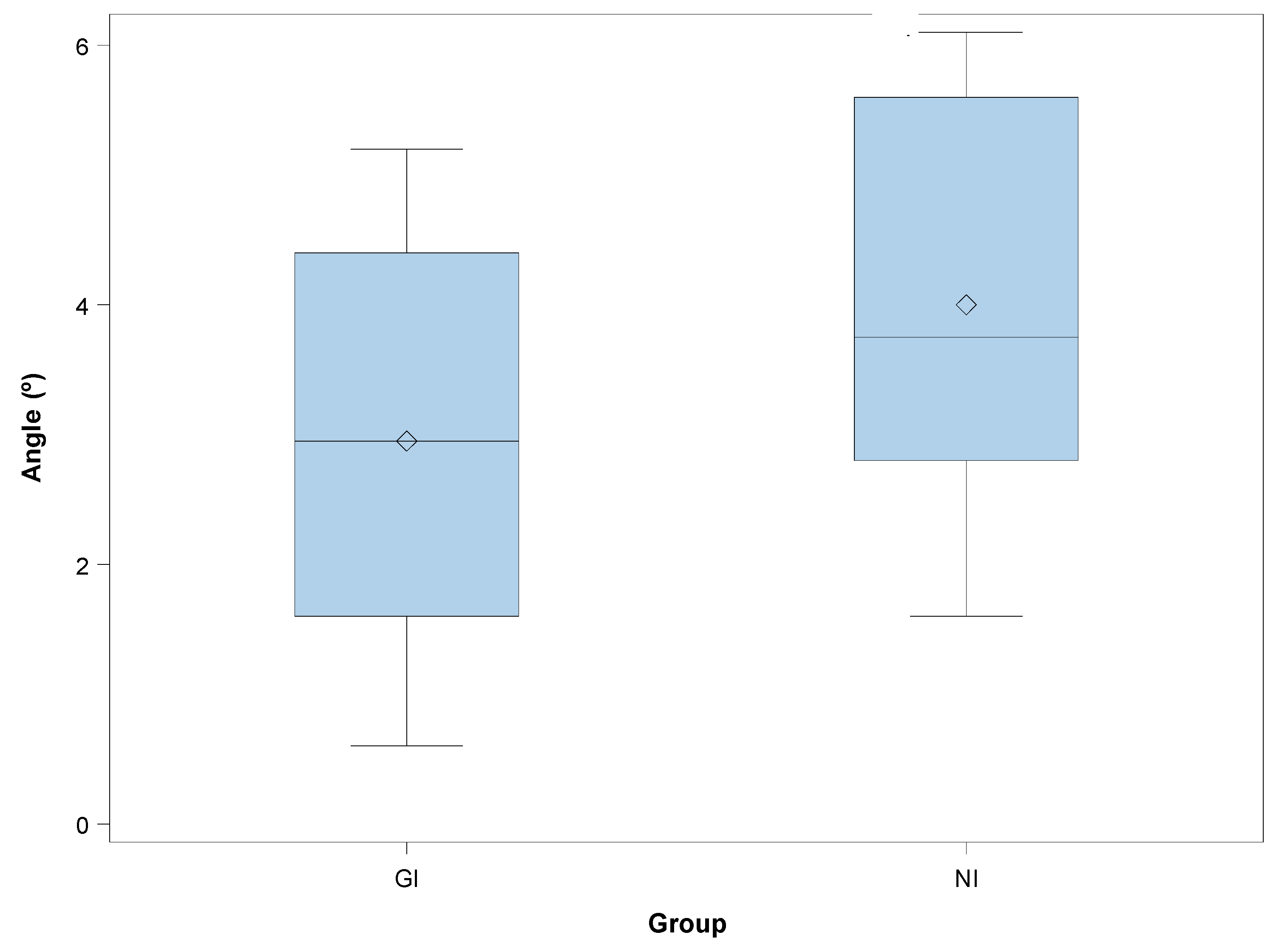
| ANGULAR | GI | 20 | 2.95 | 1.48 | 0.60 | 5.20 * |
| NI | 20 | 4.00 | 1.41 | 1.60 | 6.10 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mediavilla Guzmán, A.; Riad Deglow, E.; Zubizarreta-Macho, Á.; Agustín-Panadero, R.; Hernández Montero, S. Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study. J. Clin. Med. 2019, 8, 2123. https://doi.org/10.3390/jcm8122123
Mediavilla Guzmán A, Riad Deglow E, Zubizarreta-Macho Á, Agustín-Panadero R, Hernández Montero S. Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study. Journal of Clinical Medicine. 2019; 8(12):2123. https://doi.org/10.3390/jcm8122123
Chicago/Turabian StyleMediavilla Guzmán, Alfonso, Elena Riad Deglow, Álvaro Zubizarreta-Macho, Rubén Agustín-Panadero, and Sofía Hernández Montero. 2019. "Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study" Journal of Clinical Medicine 8, no. 12: 2123. https://doi.org/10.3390/jcm8122123
APA StyleMediavilla Guzmán, A., Riad Deglow, E., Zubizarreta-Macho, Á., Agustín-Panadero, R., & Hernández Montero, S. (2019). Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study. Journal of Clinical Medicine, 8(12), 2123. https://doi.org/10.3390/jcm8122123