Safety and Effectiveness of Shoulder Arthroplasties in Spain: A Systematic Review

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
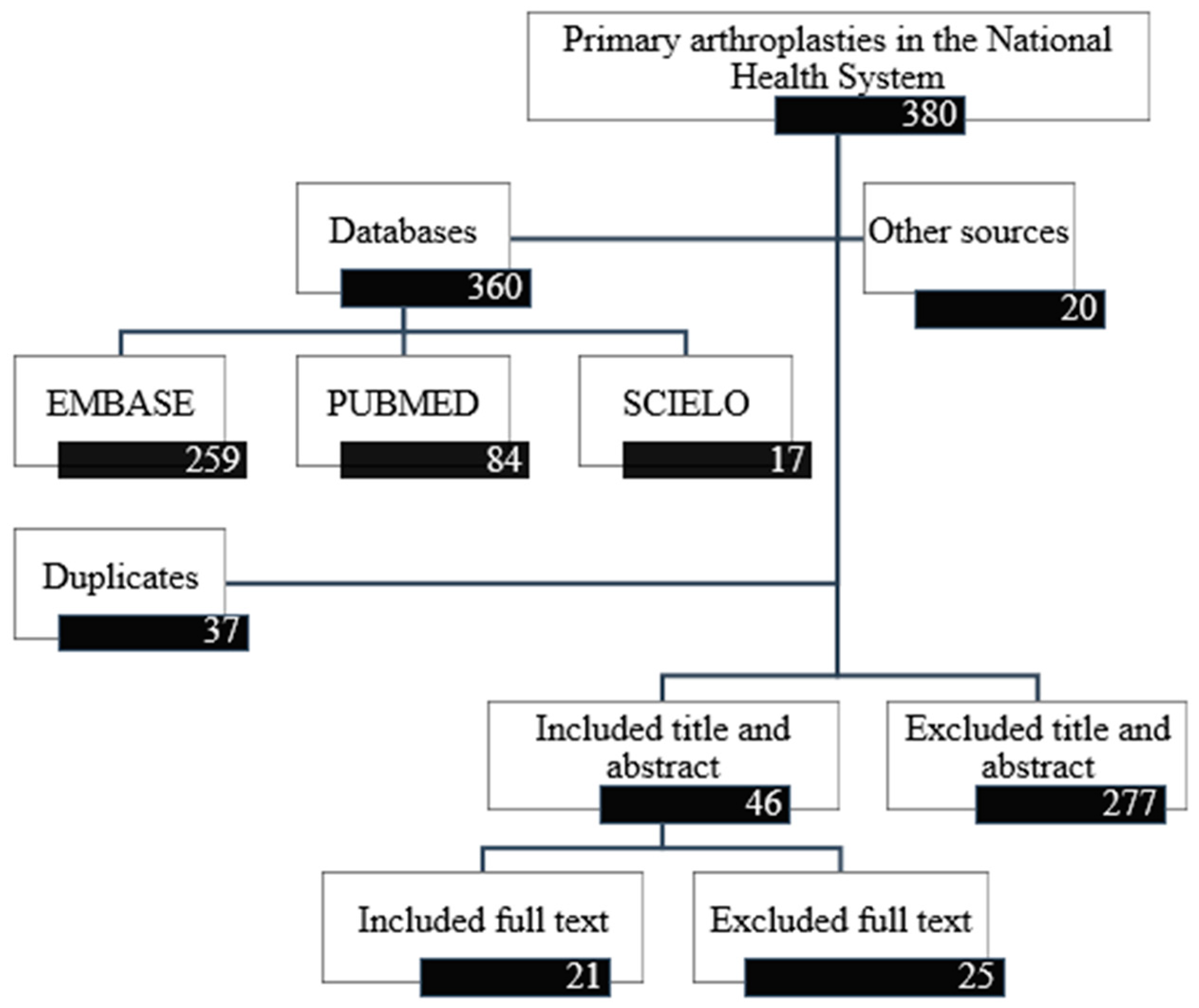
2.1. Inclusion and Exclusion Criteria and the Revision Process
2.2. Quality of Studies Included
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. PubMed Filter
References
- Boileau, P.; Sinnerton, R.J.; Chuinard, C.; Walch, G. Arthroplasty of the shoulder. J. Bone Jt. Surg. Br. 2006, 88, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Rangan, A.; Handoll, H.; Brealey, S.; Jefferson, L.; Keding, A.; Martin, B.; Goodchild, L.; Chuang, L.; Hewitt, C.; Torgerson, D. Surgical vs. nonsurgical treatment of adults with displaced fractures of the proximal humerus. Ned. Tijdschr. Traumachir. 2016, 24, 18. [Google Scholar] [CrossRef]
- Handoll, H.; Brealey, S.; Rangan, A.; Keding, A.; Corbacho, B.; Jefferson, L.; Chuang, L.-H.; Goodchild, L.; Hewitt, C.; Torgerson, D. The ProFHer (PROximal fracture of the humerus: Evaluation by randomisation) trial—A pragmatic multicentre randomized controlled trial evaluating the clinical effectiveness and cost-effectiveness of surgical compared with non-surgical treatment for proxi. Health Technol. Assess. 2015, 19, 1–279. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Sperling, J.; Buchbinder, R.; McMaken, K. Surgery for shoulder osteoarthritis. Cochrane Database Syst. Rev. 2010, 6, CD008089. [Google Scholar] [CrossRef] [PubMed]
- Sumrein, B.O.; Huttunen, T.T.; Launonen, A.P.; Berg, H.E.; Fellander-Tsai, L.; Mattila, V.M. Proximal humeral fractures in Sweden—A registry-based study. Osteoporos. Int. 2017, 28, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Ryösä, A.; Laimi, K.; Äärimaa, V.; Lehtimäki, K.; Kukkonen, J.; Saltychev, M. Surgery or conservative treatment for rotator cuff tear: A meta-analysis. Disabil. Rehabil. 2017, 39, 1357–1363. [Google Scholar] [CrossRef]
- Sharma, S.; Dreghorn, C.R. Registry of shoulder arthroplasty—The Scottish experience. Ann. R. Coll. Surg. Engl. 2006, 88, 122–126. [Google Scholar] [CrossRef]
- Handoll, H.H.; Brorson, S. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst. Rev. 2015, 11, CD000434. [Google Scholar] [CrossRef]
- Lubbeke, A.; Rees, J.L.; Barea, C.; Combescure, C.; Carr, A.J.; Silman, A.J. International variation in shoulder arthroplasty. Acta Orthop. 2017, 88, 592–599. [Google Scholar] [CrossRef]
- Arias-de la Torre, J.; Capdevila, A.; Martínez, O.; Domingo, L.; Marinelli, M.; Robles, N.; Nardi, J.; Puig-Verdié, L.; Pallisó, F.; Espallargues, M.; et al. A decade of the Catalonian Arthroplasty Register (RACat): Variability, exhaustivity, and survival of prostheses between 2005 and 2014. Rev. Esp. Cir. Ortop. Traumatol. 2017, 61, 70–81. [Google Scholar] [CrossRef]
- Portal estadístico Ministerio de Sanidad, Servicios Sociales e Igualdad Conjunto Mínimo Básico de Datos al Alta Hospitalria.
- Familiari, F.; Rojas, J.; Doral, M.N.; Huri, G.; McFarland, E.G. Reverse total shoulder arthroplasty. EFORT Open Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Gauci, M.-O.; Cavalier, M.; Gonzalez, J.-F.; Holzer, N.; Baring, T.; Walch, G.; Boileau, P. Revision of failed shoulder arthroplasty: Epidemiology, etiology, and surgical options. J. Shoulder Elb. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bohsali, K.I.; Bois, A.J.; Wirth, M.A. Complications of shoulder arthroplasty. J. Bone Jt. Surg. Am. 2017, 1, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Dillon, M.T.; Ake, C.F.; Burke, M.F.; Singh, A.; Yian, E.H.; Paxton, E.W.; Navarro, R.A. The kaiser permanente shoulder arthroplasty registry: Results from 6336 primary shoulder arthroplasties. Acta Orthop. 2015, 86, 286–292. [Google Scholar] [CrossRef]
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Annual Report 2016; AOANJRR: Adelaide, Australia, 2016. [Google Scholar]
- Hernandez, N.M.; Chalmers, B.P.; Wagner, E.R.; Sperling, J.W.; Cofield, R.H.; Sanchez-Sotelo, J. Revision to reverse total shoulder arthroplasty restores stability for patients with unstable shoulder prostheses. Clin. Orthop. Relat. Res. 2017, 475, 2716–2722. [Google Scholar] [CrossRef]
- Alcobia-Diaz, B.; Lopiz, Y.; Garcia-Fernandez, C.; Rizo de Alvaro, B.; Marco, F. Patient reported activities after reverse total shoulder arthroplasty in rotator cuff arthropathy patients. Rev. Esp. Cir. Ortop. Traumatol. 2017, 61, 273–280. [Google Scholar] [CrossRef]
- Andrés-Cano, P.; Galán, A.; Arenas, J.; Del Águila, B.; Guerado, E. Results of uncemented hemiarthroplasty as primary treatment of severe proximal humerus fractures in the elderly. Eur. J. Orthop. Surg. Traumatol. 2014, 25, 273–280. [Google Scholar] [CrossRef]
- Martinez, A.A.; Calvo, A.; Bejarano, C.; Carbonel, I.; Herrera, A. The use of the Lima reverse shoulder arthroplasty for the treatment of fracture sequelae of the proximal humerus. J. Orthop. Sci. 2012, 17, 141–147. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Arias-de la Torre, J.; Puigdomenech, E.; Valderas, J.M.; Evans, J.P.; Martín, V.; Molina, A.J.; Rodríguez, N.; Espallargues, M. Availability of specific tools to assess patient reported outcomes in hip arthroplasty in Spain. Identifying the best candidates to incorporate in an arthroplasty register: A systematic review and standardized assessment. PLoS ONE 2019, 14, e0214746. [Google Scholar] [CrossRef]
- Valderas, J.M.; Mendivil, J.; Parada, A.; Losada-Yáñez, M.; Alonso, J. Construcción de un filtro geográfico para la identificación en PubMed de estudios realizados en España. Rev. Española Cardiol. 2006, 59, 1244–1251. [Google Scholar] [CrossRef]
- Terwee, C.B.; Jansma, E.P.; Riphagen, I.I.; de Vet, H.C.W. Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual. Life Res. 2009, 18, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Northgate Orthopaedic Data Evaluation Panel (ODEP). Available online: http://www.odep.org.uk/ (accessed on 8 October 2019).
- Harbour, R.; Miller, J. A new system for grading recommendations in evidence based guidelines. BMJ 2002, 323, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Sterne, J.A.C. Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2.0). Available online: https://www.bristol.ac.uk/media-library/sites/social-community-medicine/images/centres/cresyda/RoB2-0_indiv_main_guidance.pdf (accessed on 8 October 2019).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016. [Google Scholar] [CrossRef] [PubMed]
- Moga, C.; Guo, B.; Harstall, C. Development of a Quality Appraisal Tool for Case Series Studies Using a Modified Delphi Technique; Institute of Health Economics: Edmonton, AB, Canada, 2012. [Google Scholar]
- Torrens, C.; Guirro, P.; Santana, F. The minimal clinically important difference for function and strength in patients undergoing reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2016, 25, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Torrens, C.; Guirro, P.; Miquel, J.; Santana, F. Influence of glenosphere size on the development of scapular notching: A prospective randomized study. J. Shoulder Elb. Surg. 2016, 25, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- Sebastia-Forcada, E.; Cebrian-Gomez, R.; Lizaur-Utrila, A.; Gil-Guillen, V. Reverse shoulder arthroplasty versus hemiarthroplasty for acute proximal humeral fractures: A blinded, randomized, controlled, prospective study. J. Shoulder Elb. Surg. 2014, 23, 1419–1426. [Google Scholar] [CrossRef]
- Boyer, E.; Menu, G.; Loisel, F.; Saadnia, R.; Uhring, J.; Adam, A.; Rochet, S.; Clappaz, P.; Baudouin, E.; Lascar, T.; et al. Cementless and locked prosthesis for the treatment of 3-part and 4-part proximal humerus fractures: Prospective clinical evaluation of hemi- and reverse arthroplasty. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 301–308. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Guirro, P.; Santana, F.; Torrens, C. Treatment of fracture sequelae of the proximal humerus: Comparison of hemiarthroplasty and reverse total shoulder arthroplasty. Arch. Orthop. Trauma Surg. 2014, 134, 1545–1550. [Google Scholar] [CrossRef]
- Jorge-Mora, A.; Amhaz-Escanlar, S.; Fernández-Pose, S.; Lope-Del-Teso, C.; Pino-Mínguez, J.; Caeiro-Rey, J.R.; Pretell-Mazzini, J.; Gómez, R. Early outcomes of locked noncemented stems for the management of proximal humeral fractures: A comparative study. J. Shoulder Elb. Surg. 2019, 28, 48–55. [Google Scholar] [CrossRef]
- Sebastia-Forcada, E.; Lizaur-Utrilla, A.; Cebrian-Gomez, R.; Miralles-Muñoz, F.A.; Lopez-Prats, F.A. Outcomes of reverse total shoulder arthroplasty for proximal humeral fractures: Primary arthroplasty versus secondary arthroplasty after failed proximal humeral locking plate fixation. J. Orthop. Trauma 2017, 31, e236–e240. [Google Scholar] [CrossRef] [PubMed]
- Lopiz, Y.; García-Coiradas, J.; Serrano-Mateo, L.; García-Fernández, C.; Marco, F. Reverse shoulder arthroplasty for acute proximal humeral fractures in the geriatric patient: Results, health-related quality of life and complication rates. Int. Orthop. 2016, 40, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, J.C. Pròtesi Invertida d’Espatlla: Estudi Retrospectiu del Conflicte Escapular en 2 Models Diferents de Pròtesis; Universitat Autònoma de Barcelona, Departament de Cirurgia: Barcelona, Spain, 2012. [Google Scholar]
- Izquierdo-Fernández, A.; Minarro, J.C.; Carpintero-Lluch, R.; Estévez-Torres, E.M.; Carpintero-Benítez, P. Reverse shoulder arthroplasty in obese patients: Analysis of functionality in the medium-term. Arch. Orthop. Trauma Surg. 2017, 138, 5. [Google Scholar] [CrossRef] [PubMed]
- Cáceres-Sánchez, L.; Mesa-Mateo, A.; Barrionuevo-Sánchez, F.J.; García-Benítez, B.; Expósito-Triano, S. Total reverse shoulder replacement: Evaluation of the clinical results and complications in a series of 52 cases. Rev. Esp. Cir. Ortop. Traumatol. 2015, 59, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Zafra, M.; Uceda, P.; Flores, M.; Carpintero, P. Reverse total shoulder replacement for nonunion of a fracture of the proximal humerus. Bone Jt. J. 2014, 96, 1239–1243. [Google Scholar] [CrossRef] [PubMed]
- García-Fernández, C.; Lópiz-Morales, Y.; Rodríguez, A.; López-Durán, L.; Martínez, F.M. Periprosthetic humeral fractures associated with reverse total shoulder arthroplasty: Incidence and management. Int. Orthop. 2015, 39, 1965–1969. [Google Scholar] [CrossRef]
- Torrens, C.; Santana, F.; Marí, R.; Puig, L.; Alier, A. Serum C-reactive protein in patients undergoing elective shoulder arthroplasty: Prospective study. J. Orthop. Sci. 2017, 22, 858–861. [Google Scholar] [CrossRef]
- Torrens, C.; Alentorn-Geli, E.; Mingo, F.; Gamba, C.; Santana, F. Reverse shoulder arthroplasty for the treatment of acute complex proximal humeral fractures: Influence of greater tuberosity healing on the functional outcomes. J. Orthop. Surg. 2018, 26, 2309499018760132. [Google Scholar] [CrossRef]
- Delgado Rodriguez, J.A.; Moreno Palacios, J.A.; Pulido Poma, R.M.; Fernandez Leon, R.A.; Martin Maroto, M.P.; Miranda Vivas, M.T. Functional results of partial shoulder replacement in patients over 65 years. Rev. Esp. Geriatr. Gerontol. 2013, 48, 22–25. [Google Scholar]
- Hernández-Elena, J.; de la Red-Gallego, M.Á.; Garcés-Zarzalejo, C.; Pascual-Carra, M.A.; Pérez-Aguilar, M.D.; Rodríguez-López, T.; Alfonso-Fernández, A.; Pérez-Núñez, M.I. Treatment of proximal humeral fractures by reverse shoulder arthroplasty: Mid-Term evaluation of functional results and Notching. Rev. Esp. Cir. Ortop. Traumatol. 2015, 59, 413–420. [Google Scholar] [CrossRef]
- Villodre-Jiménez, J.; Estrems-Díaz, V.; Diranzo-García, J.; Bru-Pomer, A. Reverse shoulder arthroplasty in 3 and 4 part proximal humeral fractures in patients aged more than 65 years: Results and complications. Rev. Esp. Cir. Ortop. Traumatol. 2016, 61, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Sebastià-Forcada, E. Influencia de los Factores Anatómicos en el Resultado de las Prótesis de Hombro para el Tratamiento de las Fracturas Proximales de Húmero en Pacientes de Edad. 2014. Available online: https://dialnet.unirioja.es/servlet/cittes?codigo=68217 (accessed on 8 October 2019).
- Blomquist, J.; Solheim, E.; Liavaag, S.; Schroder, C.P.; Espehaug, B.; Havelin, L.I. Shoulder instability surgery in Norway: The first report from a multicenter register, with 1-year follow-up. Acta Orthop. 2012, 83, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Magosch, P.; Habermeyer, P.; Lichtenberg, S.; Tauber, M.; Gohlke, F.; Mauch, F.; Boehm, D.; Loew, M.; Zeifang, F.; Potzl, W. Results from the German shoulder- and elbow-arthroplasty register (SEPR): Anatomic or reverse shoulder arthroplasty in B2-glenoids? Orthopade 2017, 46, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Dutch Arthroplasty Register (LROI). Annual Repport, 2018; LROI: Hague, The Netherlands, 2018. [Google Scholar]
- Fevang, B.-T.S.; Lie, S.A.; Havelin, L.I.; Skredderstuen, A.; Furnes, O. Risk factors for revision after shoulder arthroplasty: 1825 shoulder arthroplasties from the Norwegian Arthroplasty Register. Acta Orthop. 2009, 80, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, J.V.; Olsen, B.S.; Fevang, B.-T.S.; Furnes, O.; Skytta, E.T.; Rahme, H.; Salomonsson, B.; Mohammed, K.D.; Page, R.S.; Carr, A.J. A review of national shoulder and elbow joint replacement registries. J. Shoulder Elb. Surg. 2012, 21, 1328–1335. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Clark, N.J.; Assenmacher, A.T.; Samuelsen, B.T.; Sanchez-Sotelo, J.; Cofield, R.H.; Sperling, J.W. What are the complications, survival, and outcomes after revision to reverse shoulder arthroplasty in patients older than 80 years? Clin. Orthop. Relat. Res. 2017, 475, 2744–2751. [Google Scholar] [CrossRef]
- Lehtimaki, K.; Rasmussen, J.V.; Mokka, J.; Salomonsson, B.; Hole, R.; Jensen, S.L.; Aarimaa, V. Risk and risk factors for revision after primary reverse shoulder arthroplasty for cuff tear arthropathy and osteoarthritis: A Nordic Arthroplasty Register Association study. J. Shoulder Elb. Surg. 2018, 27, 1596–1601. [Google Scholar] [CrossRef]
- Erickson, B.J.; Bohl, D.D.; Cole, B.J.; Verma, N.N.; Nicholson, G.; Romeo, A.A.; Harris, J.D. Reverse total shoulder arthroplasty: Indications and techniques across the world. Am. J. Orthop. 2018, 47. [Google Scholar] [CrossRef]
- Drake, G.N.; O’Connor, D.P.; Edwards, T.B. Indications for reverse total shoulder arthroplasty in rotator cuff disease. Clin. Orthop. Relat. Res. 2010, 468, 1526–1533. [Google Scholar] [CrossRef]
- Nolan, B.M.; Ankerson, E.; Wiater, J.M. Reverse total shoulder arthroplasty improves function in cuff tear arthropathy. Clin. Orthop. Relat. Res. 2011, 469, 2476–2482. [Google Scholar] [CrossRef]
- Jobin, C.M.; Galdi, B.; Anakwenze, O.A.; Ahmad, C.S.; Levine, W.N. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J. Am. Acad. Orthop. Surg. 2015, 23, 190–201. [Google Scholar] [CrossRef] [PubMed]
- National Joint Registry for England, Wales; Northern Ireland and the Isle of Man (NJR). UK National Jt. Registry 16th Annual Report; NJR: London, UK, 2018. [Google Scholar]
- Angst, F.; Schwyzer, H.-K.; Aeschlimann, A.; Simmen, B.R.; Goldhahn, J. Measures of adult shoulder function: Disabilities of the arm, shoulder, and hand questionnaire (DASH) and its short version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society standardized shoulder. Arthritis Care Res. 2011, 63, S174–S188. [Google Scholar] [CrossRef] [PubMed]
- Constant, C.R. An evaluation of the constant-murley shoulder assessment. J. Bone Jt. Surg. Br. 1997, 79, 695–696. [Google Scholar] [CrossRef]
- Bjornholdt, K.T.; Brandsborg, B.; Soballe, K.; Nikolajsen, L. Persistent pain is common 1–2 years after shoulder replacement. Acta Orthop. 2015, 86, 71–77. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | SIGN Level of Evidence | Risk of Bias (%) | Study Type (Time Period) | Average Patient Follow-Up in Months | Total Number of Cases |
|---|---|---|---|---|---|
| Torrens et al., 2016 | 1+ | 56 | Randomized controlled trial (2010–2012) | 24 | 81 |
| Sebastià Forcada et al., 2014 | 1+ | 56 | Randomized controlled trial (2009–2011) | 30 reverse and 28 partial | 61 |
| Boyer et al., 2017 | 2++ | 39 | Nonrandomized trial (2009–2011) | 15 reverse and 25 partial | 134 |
| Alentorn-Geli et al., 2014 | 2++ | 50 | Nonrandomized trial (2005–2012). | 40 reverse and 72 partial | 32 |
| Jorge-Mora et al., 2018 | 2+ | 43 | Retrospective observational (2012–2017) | 26 | 114 |
| Sebastià Forcada et al. 2017 | 2+ | 54 | Retrospective observational (2009–2011) | 40 plate failure and 37 acute fracture | 60 |
| Lopiz et al., 2016 | 2+ | 54 | Retrospective observational (2009–2012) | 33 | 42 |
| Bonilla et al., 2012 | 2- | 54 | Retrospective observational (2003–2011) | 25 Delta and 9 Comprehensive | 43 |
| Izquierdo-Fernández et al., 2017 | 2- | 46 | Prospective observational (2012) | 48 | 29 |
| Cáceres-Sánchez et al., 2015 | 3 | 50 | Retrospective observational (2004–2012) | 36 | 52 |
| Martinez et al., 2012 | 3 | 43 | Prospective observational (2003–2007) | 48 | 44 |
| Zafra et al., 2014 | 3 | 43 | Prospective observational (2003–2011) | 51 | 35 |
| García-Fernandez et al., 2015 | 3 | 39 | Retrospective observational (2003–2014) | 79 | 163 |
| Alcobía-Díaz et al., 2017 | 3 | 43 | Retrospective observational (2009–2011) | 53 | 116 |
| Torrens et al., 2016 | 3 | 43 | Prospective observational (NS) | 12 | 60 |
| Torrens et al., 2017 | 3 | 36 | Prospective observational (NS) | 24 | 58 |
| Torrens et al., 2018 | 3 | 36 | Retrospective observational (2010–2012) | 29 | 41 |
| Delgado-Rodríguez et al., 2013 | 3 | 54 | Retrospective observational (2006–2010) | 17 | 40 |
| Hernández-Elena et al., 2015 | 3 | 43 | Retrospective observational (2009–2013) | 18 | 37 |
| Villodre-Jiménez et al., 2016 | 3 | 43 | Prospective observational (2008–2014) | 34 | 30 |
| Andrés-Cano et al., 2014 | 3 | 43 | Retrospective observational (2009–2010) | 21 | 21 |
| Author, Year | Diagnosis | Patient Characteristics | Characteristics of the Intervention | Arthroplasty and Fixation | ODEP Model Rating |
|---|---|---|---|---|---|
| Torrens et al., 2016 | Rotator cuff arthropathy (82% G38 vs. 63% G42), Proximal humeral fracture (18% G38 vs. 26% G42) and fracture sequelae (13% G38 vs. 11% G42). | Average age, 75 years G38 (88% women) vs. 76 G42 (84% women). | Glenoid component fixed without retroversion, metaglene, flush. Deltopectoral approach for sequelae fractures and anterior superior in acute fractures, and pretension of the rotator cuff. Movement starting at 24 h, Sling: 3 weeks. | Reverse. | Delta Xtend - 10A; glenoid component size (38 vs. 42 mm). |
| Sebastià Forcada et al., 2014 | Proximal humeral fracture in three (16% reverse vs. 13% partial) and four fragmented (84% reverse vs. 87% partial). Rotator cuff arthropathy: 55% reverse vs. 63% partial. | Average age: 75 years, reverse (87% women, 61% lesion in dominant arm) vs. 73 years, partial (83% women). | Deltopectoral approach. Sling: 3 weeks. Average time between fracture and surgery: 5 days. Rehabilitation: beginning of active and passive movement at 2 weeks, active with resistance at 6 weeks. | Reverse vs. partial (non-cemented). | Lima SMR - 10A. |
| Boyer et al., 2017 | Three- and four-part proximal humeral fractures. | Average age: 78 years, reverse vs. 68 years partial. | Deltopectoral (88%) or superolateral (12%) approach. Average time between fracture and surgery: 7 days. | Reverse vs. partial. Non-cemented (using two screws). | - |
| Alentorn-Geli et al., 2014 | Fracture sequelae of the proximal humerus. | Average age: 79 years, reverse (80% women) vs. 83 years, partial (33% women). | Deltopectoral (84%) or superolateral (16%) approach. Tuberosity osteotomy type IV. Subscapularis repair in partial arthroplasties and in the reverse deltopectoral approach. | Reverse vs. partial. | Reverse - Delta Xtend - 10A vs. Partial: Global Advantage. |
| Jorge-Mora et al., 2018 | Proximal humeral fracture. | Average age: 78 years, cemented (100% women) vs. 76 years, non-cemented (91% women)/76 years union (95% women) vs. 78 years non-union (95% women). | Approach: deltopectoral cemented (92%) vs. non-cemented (94%)/deltopectoral union (92%) vs. nonunion (95%), the rest superolateral. Average time between fracture and surgery: 9 days cemented/8 days union vs. 8 days nonunion. | Total reverse: cemented vs. non-cemented. | Arrow shoulder fracture and anatomic shoulder reconstruction vs. Humelock II. |
| Sebastià Forcada et al., 2017 | Complex fracture sequela due to fixation failure of proximal humeral plate vs. proximal humeral fracture. | Average age: 73 years, sequela (63% women, 43% dominant arm) vs. 75 years, fracture (63% women). | Deltopectoral approach. Average of 2.311 days between fracture and intervention in the group with sequelae. Sling: 3 weeks. Rehabilitation: started at 3 weeks, lasted 4 weeks. | Total reverse, non-cemented. | Lima SMR - 10A. |
| Lopiz et al., 2016 | Humerus fracture: three (12% vs. 19%) and four (42% vs. 48%) fragmented and dislocated fractures (46% vs. 37.5%). | Over 80 years old vs. under 80 years old. 80% women. Dominant shoulder inured (62%). | Deltopectoral approach. Average of 6 days between fracture and intervention. Rehabilitation: passive movement from 24 h post intervention to 2 weeks, exercises for 3–4 weeks. | Reverse cemented. | Delta Xtend - 10A. |
| Bonilla et al., 2012 | Rotator cuff arthropathy or osteoarthritis secondary to rotator cuff tear. | Average age: 76 years, Delta vs. (87.5% women, 81% right arm) vs. 72 years Comprehensive (92% women) | Approach: Delta Xtend transdeltoid vs. Comprehensive deltopectoral. | Reverse. | Delta Xtend - 10A vs. Comprehensive Reverse Shoulder System - 5A. |
| Izquierdo-Fernández et al., 2017 | Rotator cuff arthropathy, fractures, or dislocations. | Average age: 78 years (80% women). Body mass index ≤35 vs. >35. | - | Reverse. | Delta Xtend - 10A. |
| Cáceres-Sánchez et al., 2015 | Proximal humeral fracture (10%), prosthetic revision (12%), fracture sequelae (19%), rotator cuff tear (60%). | Average age: 70 years (84% women). | Deltopectoral approach. Sling: 3 weeks. Rehabilitation: passive movements between the 1st and 3rd weeks, active movements between the 2nd and 4th weeks and muscle enhancement between the 3rd and 12th weeks. | Reverse. | Delta Xtend - 10A (58%) and Aequalis Reversed - 5A (42%). |
| Martinez et al., 2012 | Fracture sequelae of the proximal humerus. | Average age: 77 years (60% women). | Deltopectoral approach: Average time between fracture and surgery: 365 days. Rehabilitation: starting at 3 weeks. | Reverse cemented (45%) or non-cemented (55%). | Lima SMR - 10A. |
| Zafra et al., 2014 | Error in the treatment of proximal humeral fractures in two (40%), three (26%), and four parts (34%). | Average age: 69 years. Fracture in dominant arm (86%). | Deltopectoral approach. | Reverse cemented. | Delta III. |
| García-Fernandez et al., 2015 | Rotator cuff injury (30%), rotator cuff arthropathy (44%), proximal humeral fractures (26%). | Average age: 76 years (87.5% women) for the sample that included 40 additional revision arthroplasties. | Approach: deltopectoral (fractures) or superolateral (rotator cuff tears and arthropathies) | Reverse (cemented and non-cemented). | Delta III (9%), Delta Xtend (43%) - 10A, Lima SMR (29%). |
| Alcobía-Díaz et al., 2017 | Rotator cuff arthropathy. | Average age: 81 years (88% women) Charlson Comorbidity Index: 1.7 = low comorbidity. | Superolateral approach (76%) or deltopectoral (24%). Passive rehabilitation during hospital stay, exercises for 6 weeks. | Total. | - |
| Torrens et al., 2016 | Rotator cuff arthropathy. | Average age: 74.5 years (92% women). | Reverse. | Delta Xtend - 10A. | |
| Torrens et al., 2017 | Reverse (71%): 43% rotator cuff arthropathy, 28% proximal humeral fractures. Total: 22% primary osteoarthritis. Partial: 7% proximal humeral fractures. | Average age: fractures, 74 years; osteoarthritis, 78 years; arthropathy, 74 years (88% women). | Reverse: anterosuperior approach. Anatomic: deltopectoral approach. Average time between fracture and surgery: 11 days. | Total anatomic (23%), partial (7%) and reverse (70%). | Reverse: Delta Xtend - 7A, Total: Global AP - 5A, Partial: Global Unite. |
| Torrens et al., 2018 | Proximal humeral fracture in three (17%) or four parts (83%). | Average age: 78 years (87.5% women). Average BMI: 28. | Anterosuperior approach. Average time between fracture and surgery: 12 days. | Reverse cemented. | Delta Xtend - 10A. |
| Delgado-Rodríguez et al., 2013 | Proximal humeral fracture. | Average age: 76 years (87.5% women). | Rehabilitation: average start at 4 weeks. Average number of sessions = 39. | Partial. | |
| Hernández-Elena et al., 2015 | Proximal humeral fracture with risk of osteonecrosis of the humeral head. Type of fracture: four fragments (54%), three fragments (30%), fracture-dislocation (16%). | Average age: 77 years (97% women). | Deltopectoral approach. Rehabilitation: starting at 2 weeks with passive movement, resistance exercises starting at 6 weeks. | Reverse. | Aequalis® Reversed II - 5A. |
| Villodre-Jiménez et al., 2016 | Humerus fracture in three parts (27%) and four parts (73%). With non-reconstructible fractures, risk of avascular necrosis, severe osteoporosis and previous rotator cuff injuries. | Average age: 75 years (87% women). | Deltopectoral approach. Sling: 3 weeks. Rehabilitation: passive movement starting at 3 weeks, exercises starting at 6 weeks. | Reverse cemented. | Lima SMR - 10A. |
| Andrés-Cano et al., 2014 | Proximal humeral fracture in three (10%) or four parts (57%), fracture-dislocation (33%). | Average age: 72 years (90% women). Charlson Comorbidity: 0 or 1. | Deltopectoral approach. Average time between fracture and surgery: 17 days. Sling: 5 weeks. Rehabilitation starting at 4 weeks. | Partial non-cemented. | Epoca Shoulder Arthroplasty System. |
| Author, Year | Scapular Notching | Infection | Fractures, Tears and Ossifications | Complications in Tuberosities | Fixation, Dislocation or Stiffness Complications | Neurological, Vascular and/or Lymphatic Complications | Reinterventions and Revisions |
|---|---|---|---|---|---|---|---|
| Torrens et al., 2016 | Scapular neck notching (with intention to treat) 46% G38 vs. 30% G42. | 0% G38 vs. 3% G42 | - | - | Dislocation: 3% G38 vs. 2% G42. | - | Revision: 3% G38 vs. 2% G42. |
| Sebastià Forcada et al., 2014 | Scapular neck notching: 3% Reverse vs. 0% partial. | 3% reverse vs. 3% partial. | Intraoperative fracture: 0% reverse vs. 3% partial. Ossification: 16% reverse vs. 20% partial | Malunion: 19% reverse vs. 13% partial (p = 0.4). Resorption: 16% reverse vs. 30% partial (p = 0.4). | Rigidity: 0% reverse vs. 3% partial. Migration: 0% reverse vs. 20% partial. Radiolucency: 13% reverse vs. 10% partial. | Hematoma: 0% reverse vs. 4% partial. | Revision before the 40th month: 3% reverse vs. 20% partial. |
| Boyer et al., 2017 | Notching: Reverse (8%) vs. partial (0%). | - | Periprosthetic fracture: 3% reverse vs. 1% partial. Cuff tear: 0% reverse vs. 5% partial. | Lysis 6% reverse vs. 2% partial. | Poor fixation: 7% reverse vs. 2% partial. | Phlebitis: 3% reverse vs. 0% partial. Paralysis: 1% reverse vs. 1% partial. Lymphedema: 0% reverse vs. 2% partial. | Revision: 7% reverse vs. 2% partial. |
| Alentorn-Geli et al., 2014 | Glenoid erosion: 0% reverse vs. 8% partial. | 0% reverse vs. 8% partial. | - | - | - | - | Revision: 0% reverse vs. 25% partial. |
| Jorge-Mora et al., 2018 | - | Early infection: 0% cemented vs. 3% non-cemented. | Periprosthetic fracture: 0% cemented vs. 3% non-cemented. | Poor reinforcement: 33%, 54% cemented vs. 76% non-cemented (p = 0.07). | Dislocation: 0% cemented vs. 3% non-cemented. | Paralysis: 0% cemented vs. 3% non-cemented. | Revision: 0% cemented vs. 9% non-cemented. |
| Sebastià Forcada et al., 2017 | 0%. | - | Acromion fracture: 3% sequela vs. 0% acute. Intraoperative fracture: 0% sequelae vs. 3% acute. | - | Dislocation: 7% sequela vs. 0% acute. Loosening 3% sequela vs. 0% acute. Radiolucency: 7% sequela vs. 0% fracture. | - | Revision: 13% sequela vs. 0% fracture. |
| Lopiz et al., 2016 | Scapular notching: 14%. | Periprosthetic fracture: 2%. | Malunion: 19%. Resorption: 5%. | Dislocation: 2%. Radiolucency: 0%. | Hematoma: 4%. | Revision: 2%. | |
| Bonilla et al., 2012 | Scapular notching: 31% Delta vs. 9%. Comprehensive. | 6% Delta vs. 0% Comprehensive | - | - | Migration: 3% Delta vs. 0% Comprehensive. | - | Revision: 9% Delta vs. 0% Comprehensive. |
| Izquierdo-Fernández et al., 2017 | Scapular notching: 47% BMI < 35 vs. 50% BMI > 35. | - | - | - | Radiolucency: 57% vs. 37.5% (p = 0.3). | - | - |
| Cáceres-Sánchez et al., 2015 | Scapular notching: 17%. | 4%. | Acromion fracture: 2%. Intraoperative fracture: 2%. | - | Radiolucency: 2% Instability: 4% Loosening: 4%. | - | Reintervention: 9%. |
| Martinez et al., 2012 | Glenoid notching: 41%. Scapular notching: 41%. | - | - | Resorption: 7%. | Radiolucency: 11%. Dislocation: 14%. Loosening: 2%. | Paralysis 1%. | Revision: 11%. |
| Zafra et al., 2014 | 60%. | - | Intraoperative fracture: 5%. Periprosthetic fracture: 2%. | - | Radiolucency: 65% humeral, 31.5% glenoid. | - | Other complications (20%). |
| García-Fernandez et al., 2015 | - | - | Periprosthetic humerus fracture: intraoperative with non-cemented Lima SMR (1%), postoperative with Lima SMR (1%). | - | - | - | - |
| Alcobía-Díaz et al., 2017 | - | - | - | - | - | - | 10% analgesic treatment 6 weeks after the intervention. |
| Torrens et al., 2016 | - | - | - | - | - | - | - |
| Torrens et al., 2017 | - | 0%. | - | - | - | - | - |
| Torrens et al., 2018 | Scapular notching: 15%. | - | Presence of osteophyte: 12%. | Malunion: 32%. Resorption: 10%. Poorer union, depending on comorbidity. | - | Paraesthesia: 15%. | Revision: 2%. |
| Delgado-Rodríguez et al., 2013 | - | - | - | - | - | - | - |
| Hernández-Elena et al., 2015 | Scapular notching (29%). Relationship between notching and age. | - | Intraoperative fracture: 2%. | - | - | Hematoma: 5%. Neuropraxia: 3%. | - |
| Villodre-Jiménez et al., 2016 | Scapular notching (46%). | - | Intraoperative fracture: 7%. | Malunion: 33%. | - | - | Other complications: 46%. |
| Andrés-Cano et al., 2014 | - | - | - | Malunion: 5%. Resorption: 24%. | Radiolucency: 5%. | - | - |
| Author, Year | Constant–Murley Score | Joint Assessment, by Constant–Murley Score | Other Results |
|---|---|---|---|
| Torrens et al., 2016 | Global score: 29 before—57 after G38 vs. 26 before—55 after G42. Pain: 5 before—11 after G38 vs. 5 before—11 after G42. Daily activities: 8 before—14 after G38 vs. 7 before—14 after G42. | Flexion = 4 before vs. 7 after G38 vs. 3 before—7 after G42. Abduction = 4 before vs. 6 after G38 vs. 3 before—6 after G42. External rotation = 2 before—5 after G38 vs. 2 before—4 after G42 (among groups after, p = 0.06). Internal rotation = 4 before G38—5 after vs. 4 before—7 after G42. Strength = 2 before—8 after G38 vs. 2 before—7 after G42. | - |
| Sebastià Forcada et al., 2014 | Global score: 80 reverse vs. 56 partial. Pain: 14 reverse vs. 9 partial. Activity: 17 reverse vs. 12 partial*. | Flexion = 120° reverse 80° partial*. Abduction = 113° reverse vs. 79° partial. External rotation = 5 reverse vs. 3 partial. Internal rotation= 3 reverse vs. 3 partial (p = 0.9). | UCLA score: 29 reverse vs. 21 partial. DASH score: 17 reverse vs. 24 partial. |
| Boyer et al., 2017 | Standard global score: 72 reverse vs. 72 partial. | Flexion = 109° reverse vs. 99.5° partial. Abduction = 99° reverse vs. 90° partial. External rotation = 21° reverse vs. 28° partial. | QuickDASH: 36 reverse vs. 78 partial. |
| Alentorn-Geli et al., 2014 | Standard global score: 35 before vs. 57 after, no improvement in internal rotation. Greater difference before vs. after in reverse arthroplasties (standard global, front flexion and activity level)*. | - | Score SF-36 (quality of life): No difference. |
| Jorge-Mora et al., 2018 | Global score: 53 cemented vs. 60 non-cemented/63 union vs. 45 non-union (difference of 15 points improvement). | Abduction = 92° cemented vs. 104° non-cemented/115° union vs. 68° non-union. Flexion = 92° cemented vs. 106° non-cemented/115° union vs. 69° non-union. Internal rotation = 35° cemented vs. 36° non-cemented/38° union vs. 31° non-union. External rotation = 17° cemented vs. 23° non-cemented/28° union vs. 5° non-union. | - |
| Sebastià Forcada et al., 2017 | Last standard global assessment: 67 sequela vs. 78 fracture. | Strength = 2 sequela vs. 4 fracture. Flexion = 114° sequela vs. 127° fracture. Abduction = 104° sequela vs. 120° fracture. External rotation = 4 sequela vs. 5 fracture (p = 0.3). Internal rotation = 3 sequela vs. 3 fracture (p = 0.7). | Last assessment: Pain VAS 8 sequela vs. 8 fracture (p = 0.9), UCLA score: 26 sequela vs. fracture 29 fracture, QuickDASH score: 21.5 sequela vs. 25 fracture. Satisfied patients: 93%. |
| Lopiz et al., 2016 | Global score: Lower in the older group. | No differences among groups at 24 months post intervention. | DASH score: 27 older group vs. 31 younger group (p = 0.1). Problems reported in EQ-5D: anxiety (38% older vs. 12% younger), pain/discomfort (23% vs. 12%), activity (38% vs. 0%), self-care (46% vs. 0%) and mobility (46% vs. 12%). Health status and quality of life EQ-VAS: 63 younger vs. 74 older. |
| Bonilla et al., 2012 | Global score: 32 before—57.5 after Delta vs. 31 before—60 after Comprehensive. | Flexion (before—after) = 95°–130° Delta vs. 102°–132° Comprehensive. Abduction (before—after) = 86°–123° Delta vs. 98°–118° Comprehensive. Internal rotation (before—after) = 46%–44% Delta vs. 49%–61% Comprehensive. External rotation (before—after) = 43%–64% Delta vs. 51%–61% Comprehensive. | - |
| Izquierdo-Fernández et al., 2017 | - | - | ASES score: 75 vs. 63. Length of stay: 5 vs. 6 days (p = 0.3). |
| Cáceres-Sánchez et al., 2015 | Global score: 23 before—67 at 12 months. | External rotation = 26° before—67° after. Flexion = 74° before—135° after | There are no metrics for fractures before the intervention. EQ-VAS: 8 before vs. 2 at one-year follow-up. Satisfied patients: 100%. |
| Martinez et al., 2012 | Global score: 28 before—58 after. | Flexion = 40° before vs. 100° after. Abduction = 41° before vs. 95° after. External rotation = 15° before vs. 35 after. Internal rotation = 25° before vs. 60° after. | Estimation of proximity to a normal back: 13% before to 56% after. Patient satisfaction: 86% satisfied or very satisfied. |
| Zafra et al., 2014 | Global score: 23 before—65.5 after. | Flexion = 45° before vs. 117° after. Abduction = 39° before vs. 96° after*. Internal rotation (no difference). External rotation = 5° before vs. 15.5° after. | Cofield pain rating: 4.8 before vs. 1.77 after. Patient perception of improvement after the intervention: 95%. |
| García-Fernandez et al., 2015 | Patients with periprosthetic fracture satisfied at the end of follow-up: 61%. | ||
| Alcobía-Díaz et al., 2017 | Standardized Constant score: 36 before vs. 81 after. | Differences before vs. after: improved flexion (+15°/5°) and abduction (+10°/5°), not in rotation (-2°/0°). Goutallier classification: >2 grade. | Daily activity questionnaire: 20% limitation in shoulder function with low-demand tasks, 51% limitation with high-demand tasks. VAS pain = 3.5. |
| Torrens et al., 2016 | Global score: 30 before—58 at one year. Pain: 5 before vs. 10 at one-year follow-up. Daily activities: 8 before vs. 14 at one-year follow-up. | Flexion = 4 before vs. 7 at one-year follow-up. Abduction = 4 before vs. 6 at one-year follow-up. External rotation = 3 before vs. 5 at one-year follow-up. Internal rotation = 4 before vs. 5 at one-year follow-up (p = 0.1). Strength = 2 before vs. 10 at one-year follow-up. | Patient perception of improvement: General = 80%, (minimum 8 points), Strength = 62 % (minimum 11 points), Anterior elevation = 73% (minimum 6 points), Lateral rotation = 73% (minimum 2 points), Internal rotation = 38% (minimum 2 points). |
| Torrens et al., 2017 | Global score at 2-year follow-up: 54. Pain = 12. Daily activity = 15. | Flexion = 7, Abduction = 6, Lateral rotation = 5, Internal rotation =5, Strength = 5. | C-reactive protein; increase after surgery, peak on the 2nd day, recovery on the 14th. |
| Torrens et al., 2018 | Global score at the end of follow-up: 61, 66 younger than 75 years vs. 57 older than 75 years. Pain: 12. | Metrics at the end of follow-up. Flexion = 7, Abduction = 6 Lateral rotation = 5. Internal rotation = 5, Strength = 7. | - |
| Delgado-Rodríguez et al., 2013 | Flexion = 39° before vs. 84° after. External rotation = 13° before vs. 33° after. Internal rotation = 11° before vs. 31° after. Abduction = 32° before vs. 75° after. | QuickDASH score: 36% after. Pain VAS: 3. | |
| Hernández-Elena et al., 2015 | Global score: 63. Pain:14. | Abduction = 104°. Flexion = 106°. Internal rotation = 40°. External rotation = 46°. | |
| Villodre-Jiménez et al., 2016 | Global score: 65. Best results in patients with arm lengthening intervention <20 mm. | Flexion = 124°. External rotation = 13°. Abduction = 95°. | UCLA scale: 27 points. QuickDASH: 32. Best results in QuickDASH in patients with arm lengthening intervention <20 mm. Patients with moderate to severe pain: 20%. Patients satisfied: 95%. |
| Andrés-Cano et al., 2014 | Global score at the end of follow-up: 44 points. | Active abduction = 50°. Flexion = 70°. External rotation: 50°. Internal rotation: up to the lumbosacral joint. | QuickDASH: 24 points. Higher number of rehabilitation sessions = QuickDASH. Less operating time = QuickDASH. Pain EVA = 1 of 8. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arias-de la Torre, J.; Garcia, X.; Smith, K.; Romero-Tamarit, A.; Puigdomenech, E.; Muñoz-Ortiz, L.; Evans, J.P.; Martín, V.; Molina, A.J.; Torrens, C.; et al. Safety and Effectiveness of Shoulder Arthroplasties in Spain: A Systematic Review. J. Clin. Med. 2019, 8, 2063. https://doi.org/10.3390/jcm8122063
Arias-de la Torre J, Garcia X, Smith K, Romero-Tamarit A, Puigdomenech E, Muñoz-Ortiz L, Evans JP, Martín V, Molina AJ, Torrens C, et al. Safety and Effectiveness of Shoulder Arthroplasties in Spain: A Systematic Review. Journal of Clinical Medicine. 2019; 8(12):2063. https://doi.org/10.3390/jcm8122063
Chicago/Turabian StyleArias-de la Torre, Jorge, Xavier Garcia, Kayla Smith, Arantxa Romero-Tamarit, Elisa Puigdomenech, Laura Muñoz-Ortiz, Jonathan P. Evans, Vicente Martín, Antonio J. Molina, Carles Torrens, and et al. 2019. "Safety and Effectiveness of Shoulder Arthroplasties in Spain: A Systematic Review" Journal of Clinical Medicine 8, no. 12: 2063. https://doi.org/10.3390/jcm8122063
APA StyleArias-de la Torre, J., Garcia, X., Smith, K., Romero-Tamarit, A., Puigdomenech, E., Muñoz-Ortiz, L., Evans, J. P., Martín, V., Molina, A. J., Torrens, C., Pons-Cabrafiga, M., Pallisó, F., Valderas, J. M., & Espallargues, M. (2019). Safety and Effectiveness of Shoulder Arthroplasties in Spain: A Systematic Review. Journal of Clinical Medicine, 8(12), 2063. https://doi.org/10.3390/jcm8122063