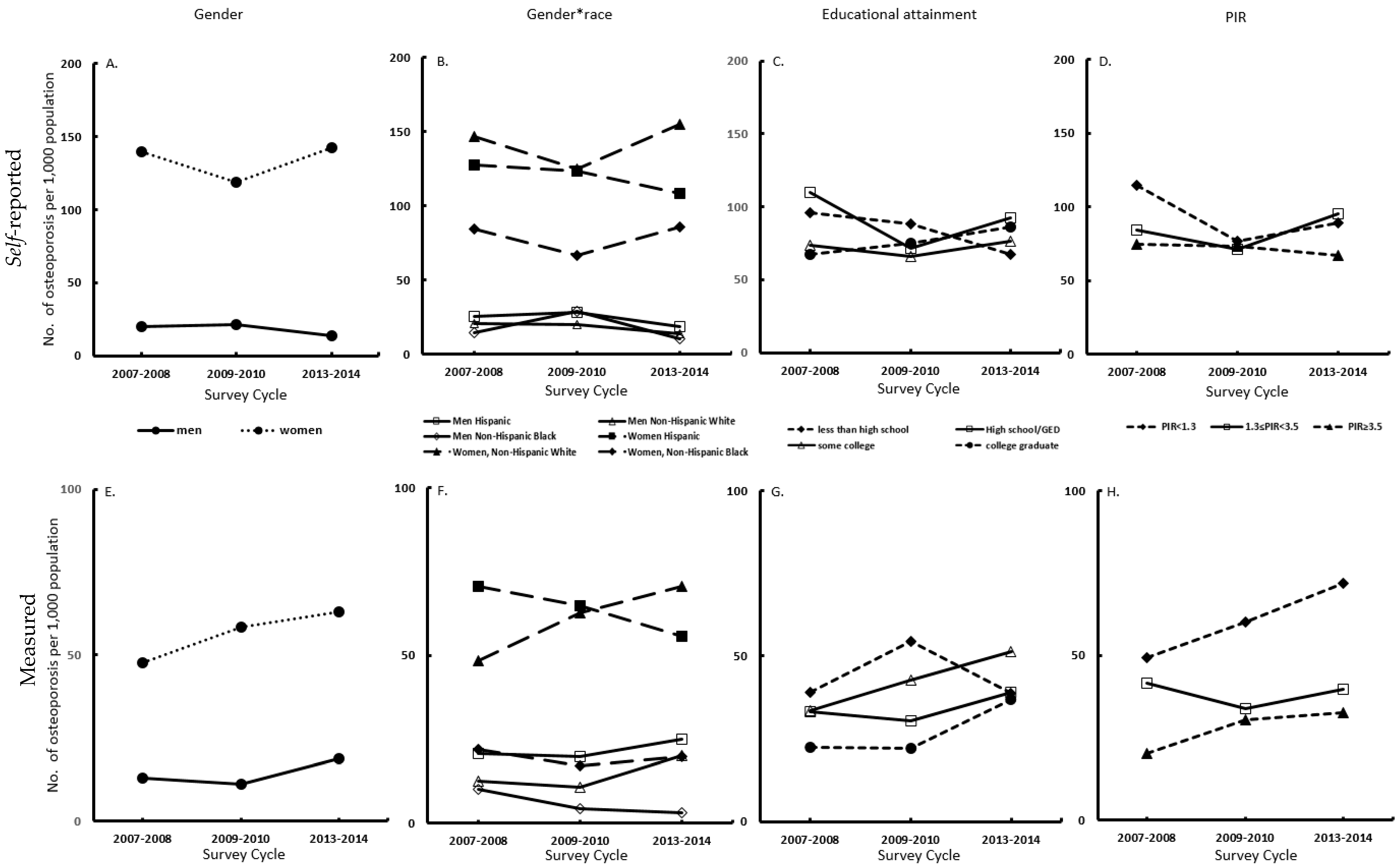
We used continuous NHANES, a nationally representative sample of the US civilian, noninstitutionalized population, to assess trends and disparities in measured and self-reported osteoporosis. Between 2007 and 2014, the age-adjusted prevalence of measured osteoporosis was on the rise among 40 year or older people in the United States, and this increase is not distributed uniformly across gender, race/ethnicity, and socioeconomic groups. Our findings regarding distinct trends and widening gaps by race/ethnicity and economic status are the concern, especially considering the significantly increased trend of measured osteoporosis among individuals with low family income (PIR < 1.3). Meanwhile, we found that the self-reported prevalence of osteoporosis was higher than the measured prevalence of osteoporosis.
We found that the trend of age-adjusted prevalence of self-reporting is different and even opposite from that of measured osteoporosis during 2007–2014. Our finding was consistent with the study conducted by Dr. Stuart that the prevalence of self-reported osteoporosis tended to be higher than the prevalence of BMD defined osteoporosis [
19]. Furthermore, the observed trend in prevalence of measured osteoporosis in this study also corresponded to the study by Looker et al., which reported that the prevalence of osteoporosis had an increasing trend in older (50 years and above) US adults between 2005–2006 and 2013–2014 [
4]. These study findings are also consistent with our previous work in which we found a decreased trend of bone density in US adults 30 years and older between 2005 and 2014 [
20]. The higher prevalence of self-reported osteoporosis might indicate the perception of osteoporosis in the population. Not only patients with osteoporosis, but also individuals with osteopenia or even healthy individuals, also had a perception of osteoporosis and bone health. Notably, the prevalence of self-reported osteoporosis was significantly higher than that of measured osteoporosis among women in all survey years, suggesting that more women may have a perception of this disease. Studies showed that the level of perception about the disease might modify individual behavior [
21,
22]. The Health Belief Model has confirmed that high perceptions provide an impetus to adopting health-protective behaviors [
23]. Therefore, the perception of osteoporosis can positively impact people’s lifestyles and behavior. However, the perception could be one of the causes of a reduction in osteoporosis treatment as well. Related literature indicated that patients’ fear of adverse effects of bisphosphonates (medication for osteoporosis) might lead to the treatment crisis [
24]. Thus, the inaccurate perception of osteoporosis might have a negative impact on their bone health, especially for patients with this condition. In addition, except for individuals with less than high school education, those with high school/GED or higher educational attainments had an increased prevalence of measured osteoporosis between 2007 and 2014. Individuals with higher educational attainment are more likely to engage in white-collar jobs, which require prolonged time spent sitting in the workplace [
25]. Rapid advances in technology have led to increased numbers of employees with high education attainment being engaged in computerized tasks, which often require prolonged sedentary sitting; such sedentary behavior was associated with increased risk of osteoporosis. Studies found that full-time employees spent about half to two-thirds of their working hours sitting [
26,
27]. The increased number of white-collar employees affected by increased workplace sitting in the new technology era may explain the increased trend of osteoporosis in these groups with higher educational attainment. Workplace intervention to increase physical activity and to reduce sedentary time for white-collar workers may help to prevent osteoporosis in these groups. The prevalence of measured osteoporosis among participants with low family income (PIR < 1.3) increased significantly during the three survey cycles. Low income is always associated with disadvantaged SES [
28], and has been considered as a major barrier for health care access. Individuals with low SES often have limited access to not only the healthcare system but also experience a shortage of healthy food and a lack of knowledge about health, ultimately leading to poor bone health. Rapid increases in health care costs and insurance premiums may also have contributed to widening disparities by income and SES.
Our analyses have limitations. First, the cross-sectional nature of NHANES limited our ability to assess the trajectory of BMD change over time for individual participants and the corresponding impacts on our findings. Second, some of the NHANES participants were not eligible for BMD testing due to hip fracture, pregnancy, or other reasons, and were excluded from analysis, which may cause bias in the estimates. Furthermore, non-response bias is always a concern in NHANES data, as response rates have declined in federal surveys since 2000 [
29]. The decline in response rate could have a different impact on the accuracy of the estimated prevalence of self-reported osteoporosis across the different survey cycles we studied. However, the sample weights of NHANES have accounted for the non-response in the analysis. Third, the estimated prevalence of self-reported osteoporosis was subjected to recall bias. However, the NHANES survey was conducted in-person, which may be more accurate than a survey conducted by a different approach. Additionally, subjects were classified as self-reported osteoporosis in this study if they responded “yes” to either “Has a doctor ever told you that you had osteoporosis, sometimes called thin or brittle bones?” or “Were you ever treated for osteoporosis?” However, the difference between osteoporosis and osteopenia, and the detail osteoporosis treatment were not described in the NHANES questionnaires. Hence, the self-reported data were subject to bias. Finally, all of the NHANES participants were noninstitutionalized, as institutionalized persons may have lower bone mass [
30], and the prevalence of measured osteoporosis in this study may be slightly underestimated. Nevertheless, this limitation is unlikely to have altered the trends of measured osteoporosis we observed.


{kind=link}