Low Dose Low-Molecular-Weight Heparin for Thrombosis Prophylaxis: Systematic Review with Meta-Analysis and Trial Sequential Analysis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
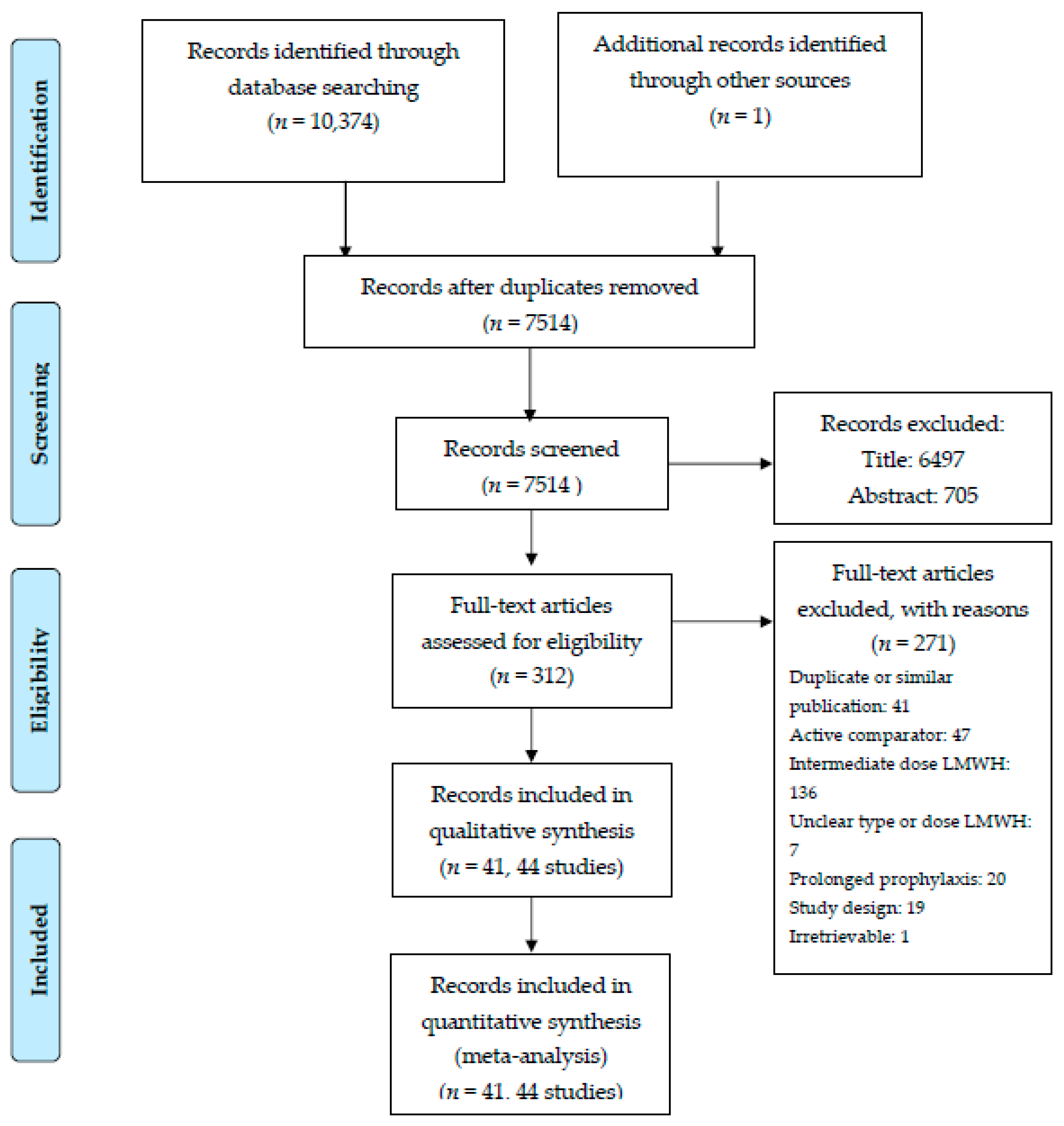
2.1. Study Selection
2.1.1. Patients
2.1.2. Interventions
2.1.3. Outcomes
2.2. Data Sources and Searches
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
2.4.1. Assessment of Significance
2.4.2. Meta-Analysis
2.4.3. Trial Sequential Analysis
2.4.4. Assessment of Heterogeneity
2.4.5. Subgroup Analysis
2.4.6. Sensitivity Analysis
2.5. GRADE
3. Results
3.1. Characteristics of the Included Studies
3.2. Bias Risk Assessment
3.3. Co-Primary Outcomes
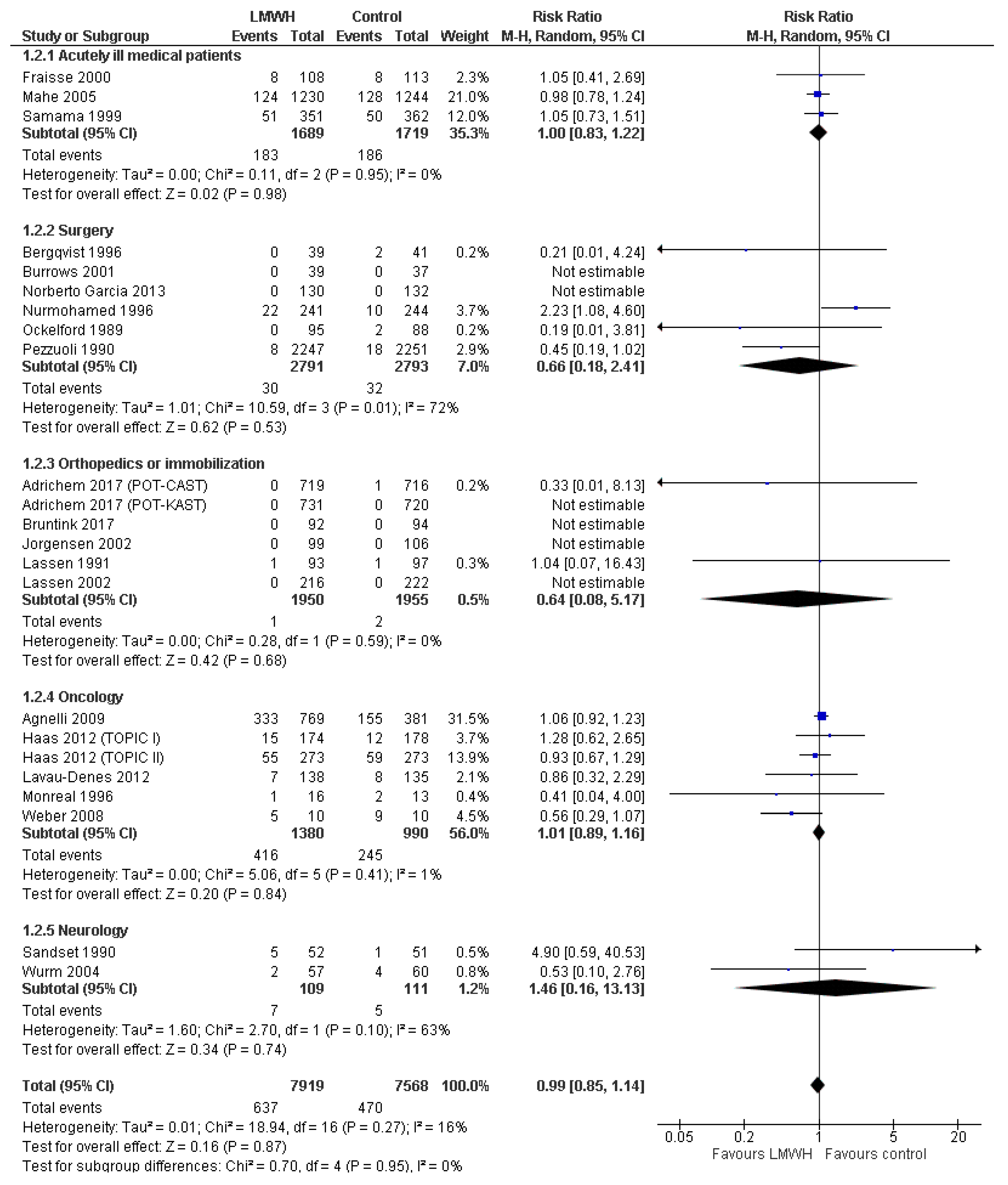
3.3.1. All-Cause Mortality
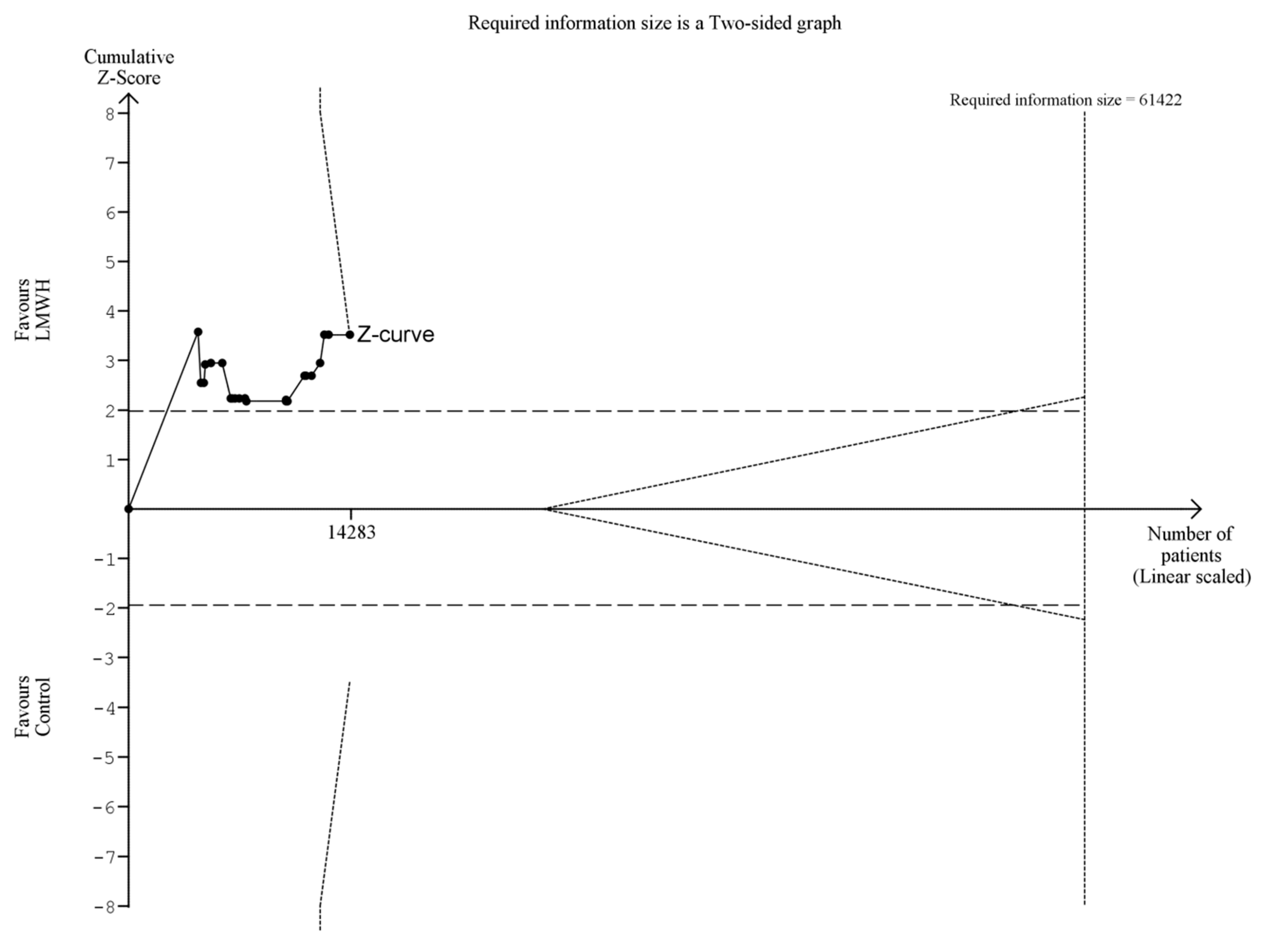
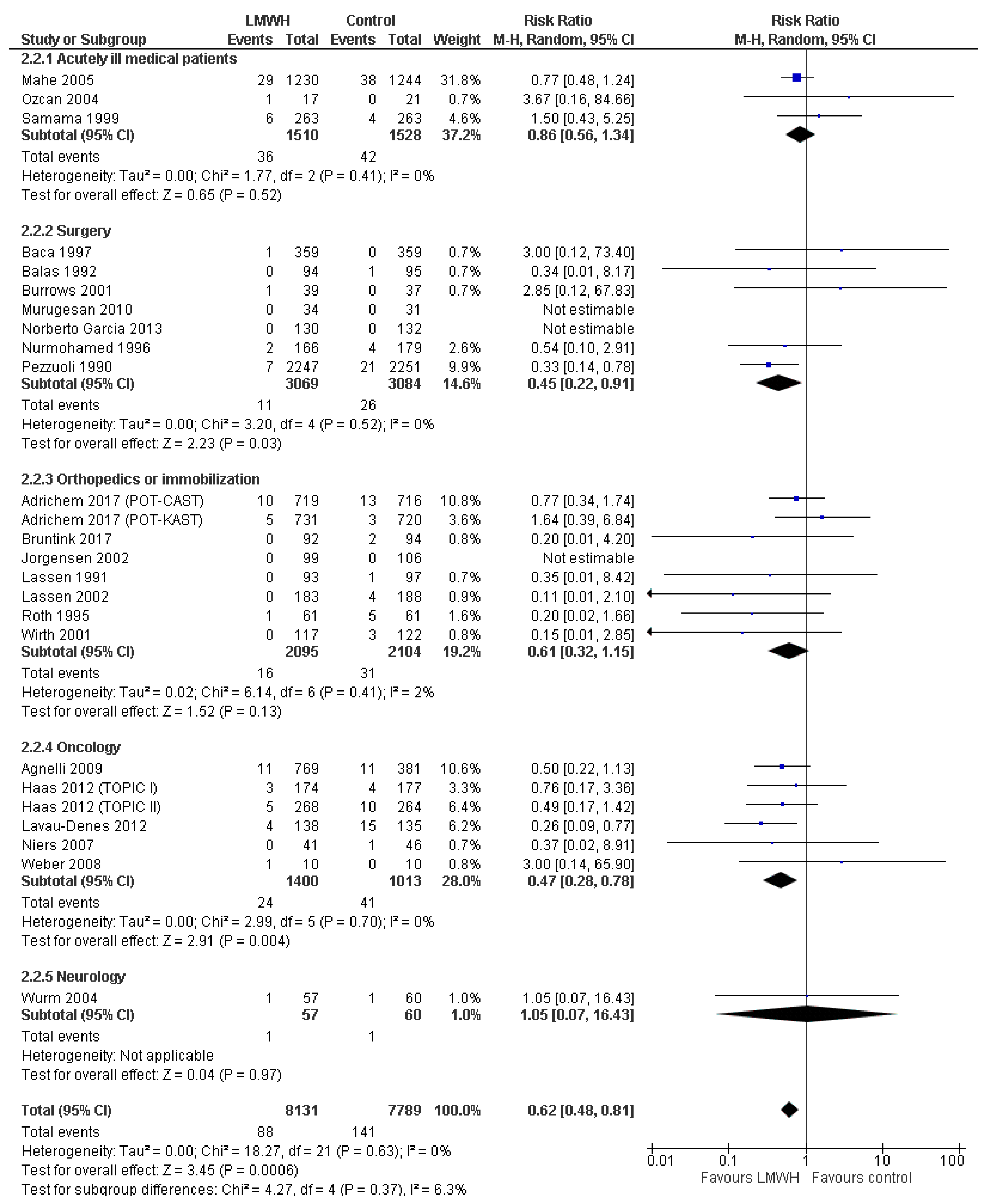
3.3.2. Symptomatic Venous Thromboembolism
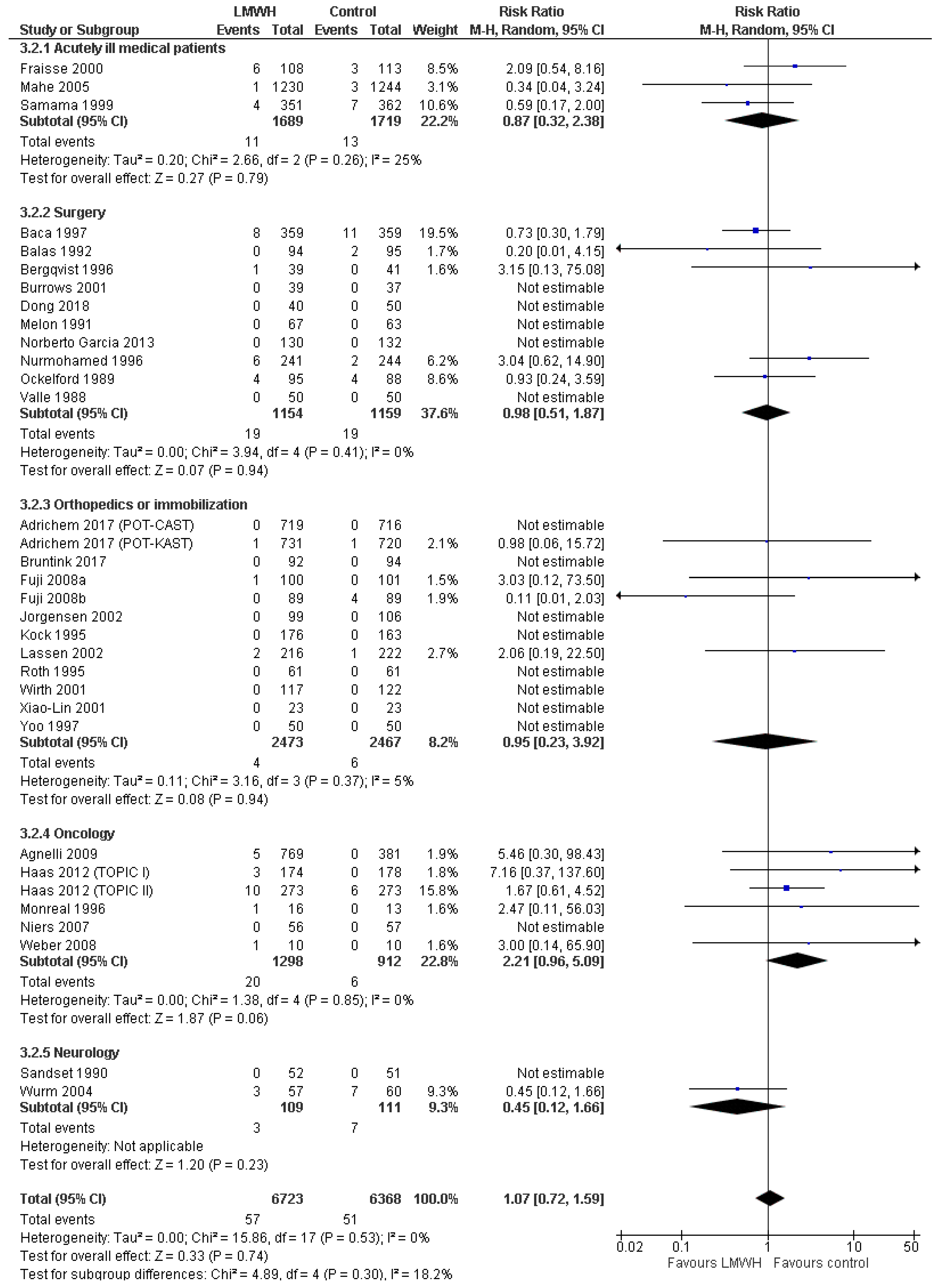
3.3.3. Major Bleeding
3.4. Secondary Outcomes
3.4.1. Serious Adverse Events
3.4.2. Clinically Relevant Non-Major Bleeding
3.4.3. Any Venous Thromboembolism
4. Discussion
4.1. Considerations on the Optimal Prophylactic Dose
4.2. Implications for Clinical Practice
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cohen, A.T.; Alikhan, R.; Arcelus, J.I.; Bergmann, J.-F.; Haas, S.; Merli, G.J.; Spyropoulos, A.C.; Tapson, V.F.; Turpie, A.G.G. Assessment of venous thromboembolism risk and the benefits of thromboprophylaxis in medical patients. Thromb. Haemost. 2005, 94, 750–759. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Cushman, M.; Burnett, A.E.; Kahn, S.R.; Beyer-Westendorf, J.; Spencer, F.A.; Rezende, S.M.; Zakai, N.A.; Bauer, K.A.; Dentali, F.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. 2018, 2, 3198–3225. [Google Scholar] [CrossRef] [PubMed]
- NICE Guideline Venous Thromboembolism in over 16s: Reducing the Risk of Hospital-Acquired Deep Vein Thrombosis or Pulmonary Embolism. 2018. Available online: https://www.nice.org.uk/guidance/ng89 (accessed on 31 January 2019).
- Alhazzani, W.; Lim, W.; Jaeschke, R.Z.; Murad, M.H.; Cade, J.; Cook, D.J. Heparin thromboprophylaxis in medical-surgical critically ill patients: A systematic review and meta-analysis of randomized trials. Crit. Care Med. 2013, 41, 2088–2098. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Bosch, J.; Cucherat, M.; Eikelboom, J.W. Nadroparin for the prevention of venous thromboembolism in nonsurgical patients: A systematic review and meta-analysis. J. Thromb. Thrombolysis 2016, 42, 90–98. [Google Scholar] [CrossRef]
- Di Nisio, M.; Porreca, E.; Candeloro, M.; De Tursi, M.; Russi, I.; Rutjes, A.W. Primary prophylaxis for venous thromboembolism in ambulatory cancer patients receiving chemotherapy. Cochrane Database Syst. Rev. 2016, 12, CD008500. [Google Scholar] [CrossRef]
- Kahale, L.A.; Tsolakian, I.G.; Hakoum, M.B.; Matar, C.F.; Barba, M.; Yosuico, V.E.; Terrenato, I.; Sperati, F.; Schünemann, H.; Akl, E.A. Anticoagulation for people with cancer and central venous catheters. Cochrane Database Syst. Rev. 2018, 6, CD006468. [Google Scholar] [CrossRef]
- Beitland, S.; Sandven, I.; Kjaervik, L.K.; Sandset, P.M.; Sunde, K.; Eken, T. Thromboprophylaxis with low molecular weight heparin versus unfractionated heparin in intensive care patients: A systematic review with meta-analysis and trial sequential analysis. Intensive Care Med. 2015, 41, 1209–1219. [Google Scholar] [CrossRef]
- Sanford, D.; Naidu, A.; Alizadeh, N.; Lazo-Langner, A. The effect of low molecular weight heparin on survival in cancer patients: An updated systematic review and meta-analysis of randomized trials. J. Thromb. Haemost. 2014, 12, 1076–1085. [Google Scholar] [CrossRef]
- Chapelle, C.; Rosencher, N.; Jacques Zufferey, P.; Mismetti, P.; Cucherat, M.; Laporte, S. Prevention of venous thromboembolic events with low-molecular-weight heparin in the non-major orthopaedic setting: Meta-analysis of randomized controlled trials. Arthroscopy 2014, 30, 987–996. [Google Scholar] [CrossRef]
- Eck, R.J.; Bult, W.; Wetterslev, J.; Gans, R.O.B.; Meijer, K.; Keus, F.; Van der Horst, I.C.C. Intermediate Dose low-molecular-weight heparin for thrombosis prophylaxis: Systematic review with meta-analysis and trial sequential analysis. Semin. Thromb. Hemost. 2019, 45, 810–824. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: Lonodn, UK, 2011; ISBN 9780470057964. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, J.C.; Wetterslev, J.; Winkel, P.; Lange, T.; Gluud, C. Thresholds for statistical and clinical significance in systematic reviews with meta-analytic methods. BMC Med. Res. Methodol. 2014, 14, 120. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schunemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef] [PubMed]
- International Conference on Harmonisation Expert Working Group International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use, ed. ICH Harmonised Tripartite Guideline; Guideline for Good Clinical Practice. Available online: www.ich.org/products/guidelines/efficacy/article/efficacy-guidelines.html (accessed on 31 January 2019).
- Sterne, J.; Savović, J.; Page, M.; Elbers, R.; Blencowe, N.; Boutron, I.; Cates, C.; Cheng, H.-Y.; Corbett, M.; Eldridge, S.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Savović, J.; Turner, R.M.; Mawdsley, D.; Jones, H.E.; Beynon, R.; Higgins, J.P.T.; Sterne, J.A.C. Association between risk-of-bias assessments and results of randomized trials in cochrane reviews: The ROBES meta-epidemiologic study. Am. J. Epidemiol. 2018, 187, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial sequential analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Brok, J.; Thorlund, K.; Wetterslev, J.; Gluud, C. Apparently conclusive meta-analyses may be inconclusive—Trial sequential analysis adjustment of random error risk due to repetitive testing of accumulating data in apparently conclusive neonatal meta-analyses. Int. J. Epidemiol. 2009, 38, 287–298. [Google Scholar] [CrossRef]
- Thorlund, K.; Devereaux, P.J.; Wetterslev, J.; Guyatt, G.; Ioannidis, J.P.A.; Thabane, L.; Gluud, L.-L.; Als-Nielsen, B.; Gluud, C. Can trial sequential monitoring boundaries reduce spurious inferences from meta-analyses? Int. J. Epidemiol. 2009, 38, 276–286. [Google Scholar] [CrossRef]
- Pogue, J.M.; Yusuf, S. Cumulating evidence from randomized trials: Utilizing sequential monitoring boundaries for cumulative meta-analysis. Control. Clin. Trials 1997, 18, 580–586. [Google Scholar] [CrossRef]
- Pogue, J.; Yusuf, S. Overcoming the limitations of current meta-analysis of randomised controlled trials. Lancet 1998, 351, 47–52. [Google Scholar] [CrossRef]
- Wetterslev, J.; Thorlund, K.; Brok, J.; Gluud, C. Estimating required information size by quantifying diversity in random-effects model meta-analyses. BMC Med. Res. Methodol. 2009, 9, 86. [Google Scholar] [CrossRef] [PubMed]
- Alikhan, R.; Bedenis, R.; Cohen, A.T. Heparin for the prevention of venous thromboembolism in acutely ill medical patients (excluding stroke and myocardial infarction). Cochrane Database Syst. Rev. 2014, 5, CD003747. [Google Scholar] [CrossRef] [PubMed]
- Hostler, D.C.; Marx, E.S.; Moores, L.K.; Petteys, S.K.; Hostler, J.M.; Mitchell, J.D.; Holley, P.R.; Collen, J.F.; Foster, B.E.; Holley, A.B. Validation of the international medical prevention registry on venous thromboembolism bleeding risk score. Chest 2016, 149, 372–379. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LMWH Type | A Priori Defined as Low-Dose LMWH | Dose Used in Included Trials |
|---|---|---|
| Bemiparin | <3500 IU | 2500 IU |
| Certoparin | <5000 IU | 3000 IU |
| Dalteparin | <5000 IU | 2500 IU a |
| Enoxaparin | <40 mg | 20 mg |
| Nadroparin | <5700 IU | 2850–3800 IU b,c |
| Parnaparin | <4250 IU | 3200 IU |
| Reviparin | <3436 IU | 1750 IU |
| Tinzaparin | <4500 IU | 3500 IU d |
| Outcome | Included Trials | Trials (Patients) | Conventional Meta-Analysis a | Primary TSA a α 2.5%; ß 90%; RRR 20%; D2 Model Variance Based | Sensitivity TSA a α 2.5%; ß 90%; RRR Based on Low Risk Trials; D2 Model Variance Based | Sensitivity TSA a α 2.5%; ß 90%; RRR 20%; D2 25% | Certainty of Evidence |
|---|---|---|---|---|---|---|---|
| Mortality | Low bias risk | 5 (4.960) | RR 1.03 (0.92 to 1.16) | RR 1.03 (0.88 to 1.20) | Insufficient data (<5% of DIS) | RR 1.03 (0.86 to 1.23) | Low d, e, f |
| All | 23 (15.487) | RR 0.99 (0.85 to 1.14) | RR 1.02 (0.89 to 1.16) b | Insufficient data (<5% of DIS) | RR 1.02 (0.90 to 1.15) | Low d, g | |
| Symptomatic VTE | Low bias risk | 5 (4.878) | RR 0.65 (0.45 to 0.94) | RR 0.67 (0.15 to 3.05) | RR 0.67 (0.32 to 1.38) | 0.67 (0.15 to 3.05) | Moderate e |
| All | 25 (15.920) | RR 0.62 (0.48 to 0.81) | RR 0.62 (0.44 to 0.89) c | RR 0.62 (0.42 to 0.92) | RR 0.62 (0.20 to 1.95) | Moderate g | |
| Major bleeding | Low bias risk | 5 (4.960) | RR 1.70 (0.77 to 3.74) | Insufficient data (<5% of DIS) | Insufficient data (<5% of DIS) | Insufficient data (<5% of DIS) | Moderate f |
| All | 33 (13.091) | RR 1.07 (0.72 to 1.59) | RR 1.01 (0.18 to 5.73) c | RR 1.01 (0.52 to 1.93) | RR 1.09 (0.75 to 1.60) | Low e, f, g | |
| SAE | Low bias risk | 1 (1.150) | RR 0.89 (0.68 to 1.17) | RR 0.89 (0.41 to 1.96) | RR 0.89 (0.27 to 2.96) | RR 0.89 (0.36 to 2.23) | Low e, f, h |
| All | 8 (5.180) | RR 0.98 (0.78 to 1.25) | RR 0.98 (0.37 to 2.58) | Insufficient data (<5% of DIS) | RR 0.98 (0.77 to 1.24) | Very low d, e, f, g | |
| Clinically relevant non-major bleeding | Low bias risk | 0 (0) | - | - | - | - | - |
| All | 5 (3.372) | RR 1.50 (0.72 to 3.12) | Insufficient data (<5% of DIS) | Insufficient data (<5% of DIS) | Insufficient data (<5% of DIS) | Very low d, e, f, g | |
| Any VTE | Low bias risk | 3 (1.254) | RR 0.57 (0.38 to 0.84) | RR 0.57 (0.11 to 2.82) | RR 0.57 (0.32 to 1.01) | Not performed (D2 >25%) | Moderate e, i, k |
| All | 30 (5.849) | RR 0.61 (0.50 to 0.75) | RR 0.63 (0.49 to 0.82) | RR 0.63 (0.50 to 0.80) | Not performed (D2 >25%) | Low e, i, j, k |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eck, R.J.; Bult, W.; Wetterslev, J.; Gans, R.O.B.; Meijer, K.; van der Horst, I.C.C.; Keus, F. Low Dose Low-Molecular-Weight Heparin for Thrombosis Prophylaxis: Systematic Review with Meta-Analysis and Trial Sequential Analysis. J. Clin. Med. 2019, 8, 2039. https://doi.org/10.3390/jcm8122039
Eck RJ, Bult W, Wetterslev J, Gans ROB, Meijer K, van der Horst ICC, Keus F. Low Dose Low-Molecular-Weight Heparin for Thrombosis Prophylaxis: Systematic Review with Meta-Analysis and Trial Sequential Analysis. Journal of Clinical Medicine. 2019; 8(12):2039. https://doi.org/10.3390/jcm8122039
Chicago/Turabian StyleEck, Ruben J., Wouter Bult, Jørn Wetterslev, Reinold O. B. Gans, Karina Meijer, Iwan C.C. van der Horst, and Frederik Keus. 2019. "Low Dose Low-Molecular-Weight Heparin for Thrombosis Prophylaxis: Systematic Review with Meta-Analysis and Trial Sequential Analysis" Journal of Clinical Medicine 8, no. 12: 2039. https://doi.org/10.3390/jcm8122039
APA StyleEck, R. J., Bult, W., Wetterslev, J., Gans, R. O. B., Meijer, K., van der Horst, I. C. C., & Keus, F. (2019). Low Dose Low-Molecular-Weight Heparin for Thrombosis Prophylaxis: Systematic Review with Meta-Analysis and Trial Sequential Analysis. Journal of Clinical Medicine, 8(12), 2039. https://doi.org/10.3390/jcm8122039