Cell Blood Count Alterations and Patterns of Anaemia in Autoimmune Atrophic Gastritis at Diagnosis: A Multicentre Study

 , ,
, ,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
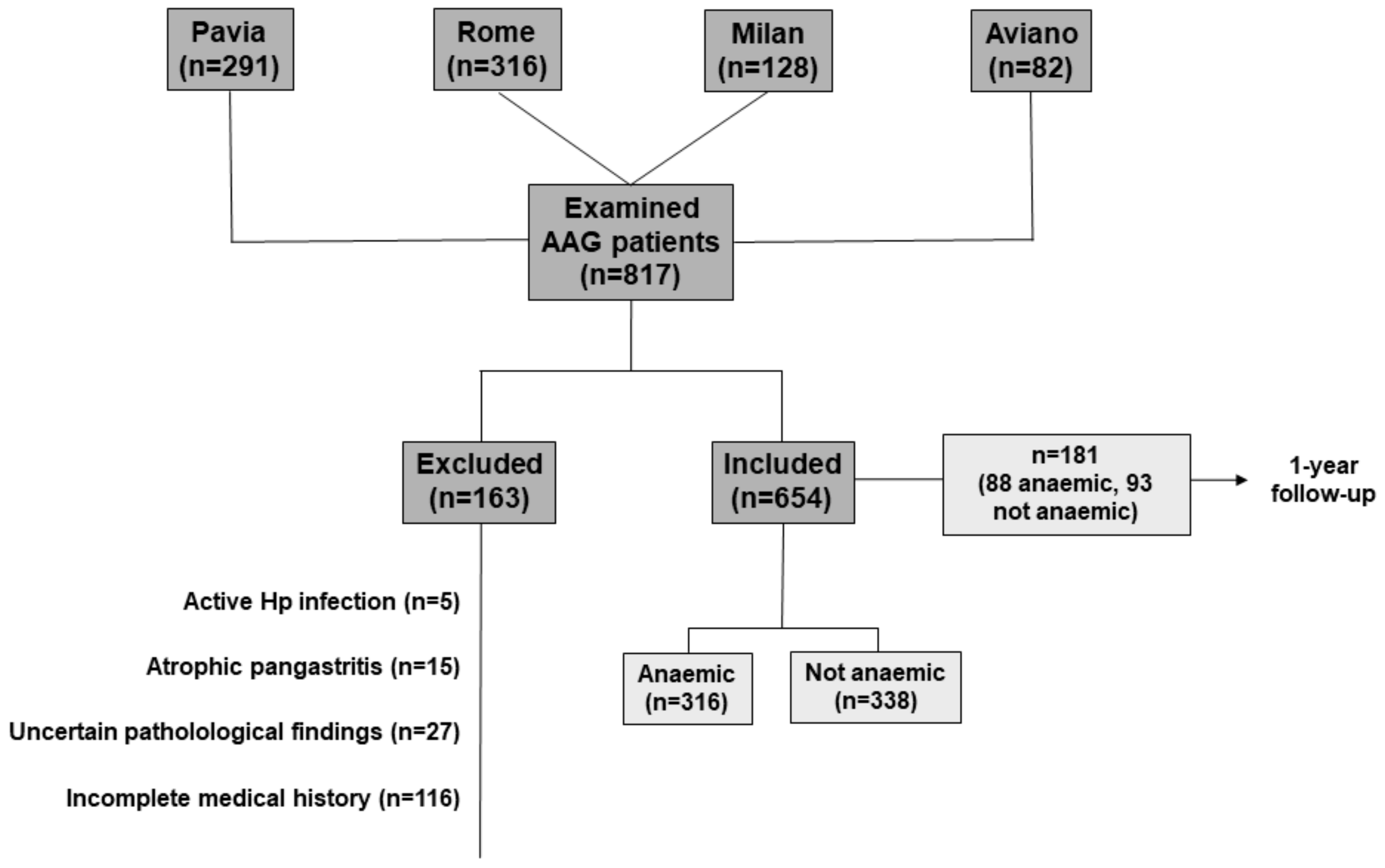
2.1. Participating Centres, Patient Selection, and Definition of Anaemia
2.2. Statistical Analysis
3. Results
3.1. Demographic, Clinical, and Histopathological Characteristics
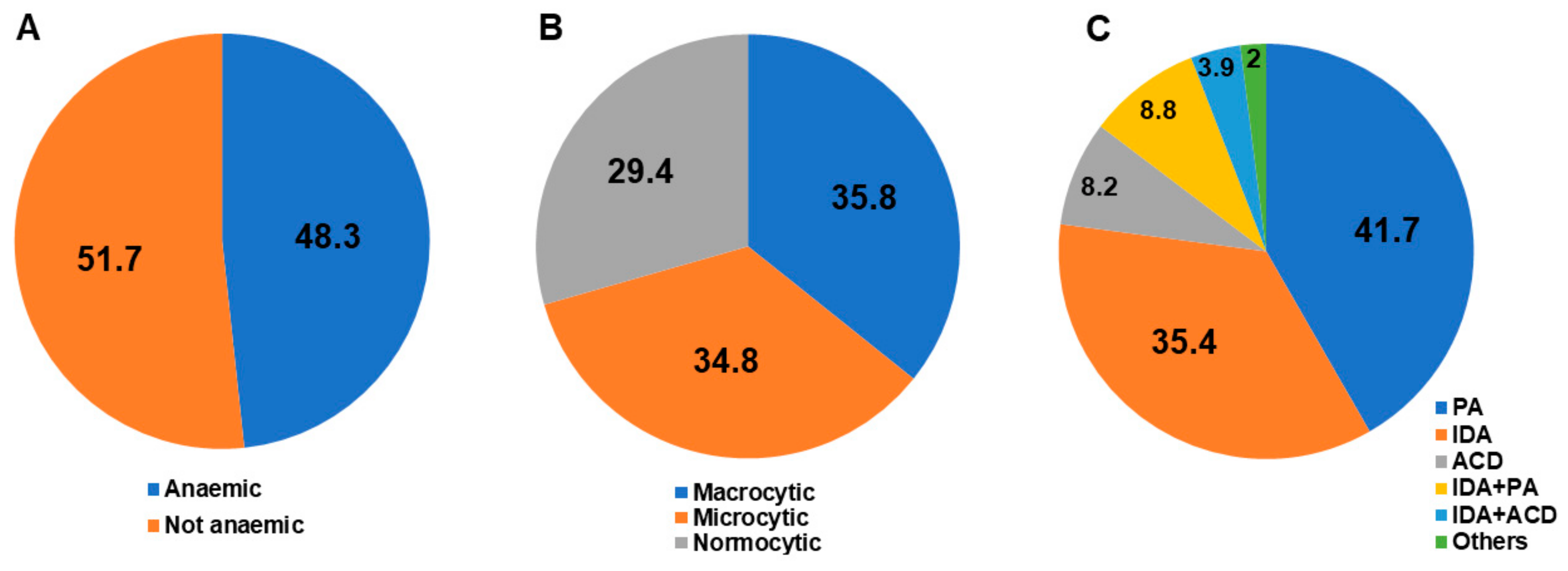
3.2. Haematological Alterations
3.3. Micronutrient Deficiencies
3.4. Haematological Alterations with Regard to Gender
3.5. Haematological Alterations with Regard to Age (as a Continuous Variable)
3.6. Clinical Predictors of Anaemia
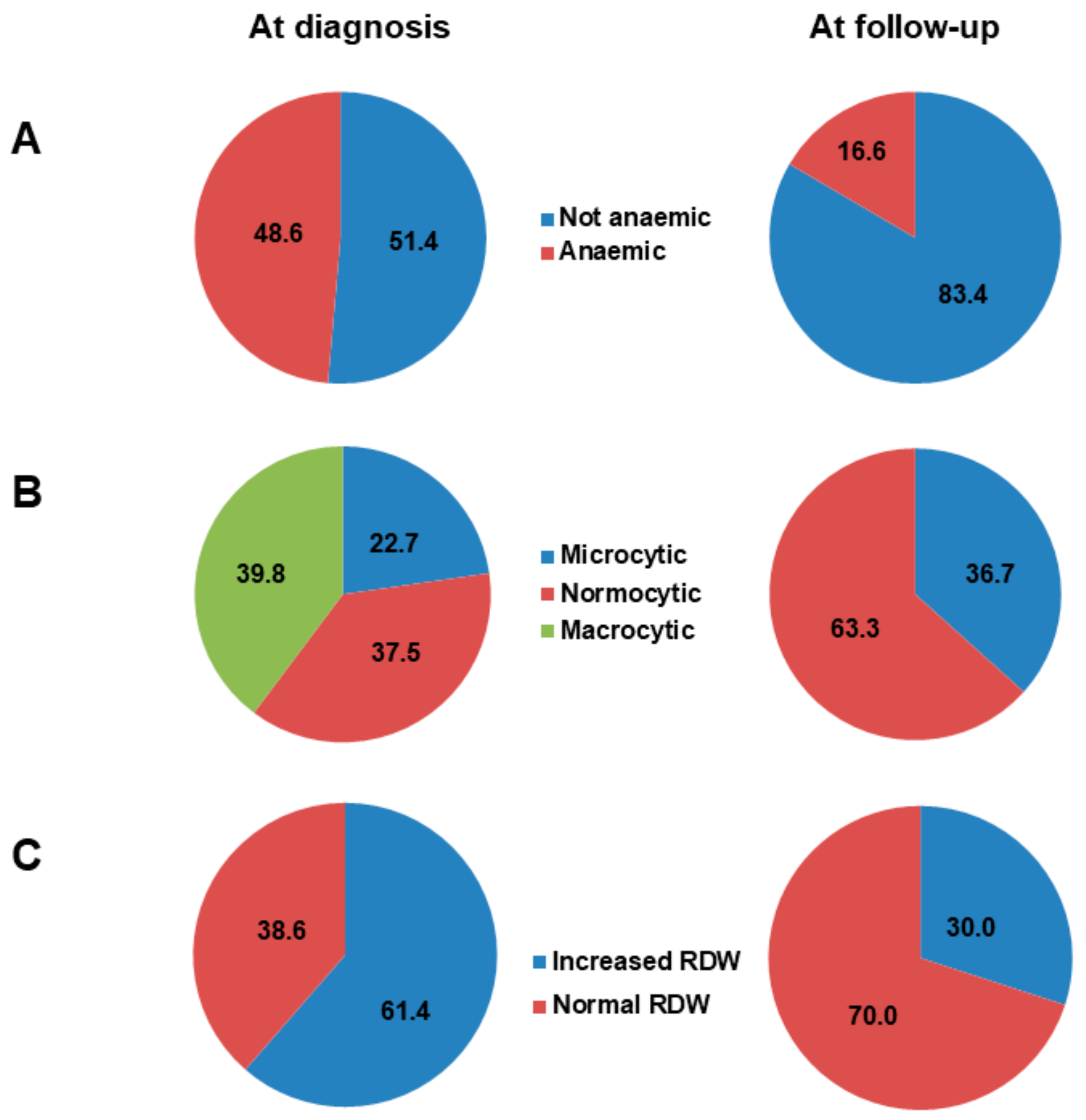
3.7. Follow-Up of Anaemia
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Neumann, W.L.; Coss, E.; Rugge, M.; Genta, R.M. Autoimmune atrophic gastritis: Pathogenesis, pathology and management. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Di Sabatino, A.; Lenti, M.V.; Giuffrida, P.; Vanoli, A.; Corazza, G.R. New insights into immune mechanisms underlying autoimmune diseases of the gastrointestinal tract. Autoimmun. Rev. 2015, 14, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Carmel, R. Prevalence of undiagnosed pernicious anemia in the elderly. Arch. Intern. Med. 1996, 156, 1097–1100. [Google Scholar] [CrossRef] [PubMed]
- Miceli, E.; Lenti, M.V.; Padula, D. Common features of patients with autoimmune atrophic gastritis. Clin. Gastroenterol. Hepatol. 2012, 10, 812–814. [Google Scholar] [CrossRef]
- Massironi, S.; Zilli, A.; Elvevi, A.; Invernizzi, P. The changing face of chronic autoimmune atrophic gastritis: An updated comprehensive perspective. Autoimmun. Rev. 2019, 18, 215–222. [Google Scholar] [CrossRef]
- Hershko, C.; Ronson, A.; Souroujon, M.; Maschler, I.; Heyd, J.; Patz, J. Variable hematologic presentation of autoimmune gastritis: Age-related progression from iron deficiency to cobalamin depletion. Blood 2006, 107, 1673–1679. [Google Scholar] [CrossRef]
- Green, R.; Allen, L.H.; Bjørke-Monsen, A.L.; Guéant, J.L.; Miller, J.W.; Molloy, A.M.; Nexo, E.; Stabler, S.; Toh, B.H.; Ueland, P.M.; et al. Vitamin B12 deficiency. Nat. Rev. Dis. Primers 2017, 3, 17040. [Google Scholar] [CrossRef]
- Bergamaschi, G.; Di Sabatino, A.; Corazza, G.R. Pathogenesis, diagnosis and treatment of anaemia in immune-mediated gastrointestinal disorders. Br. J. Haematol. 2018, 182, 319–329. [Google Scholar] [CrossRef]
- Toh, B.H.; van Driel, I.R.; Gleeson, P.A. Pernicious anemia. N. Engl. J. Med. 1997, 337, 1441–1448. [Google Scholar] [CrossRef]
- Lahner, E.; Annibale, B. Pernicious anemia: New insights from a gastroenterological point of view. World J. Gastroenterol. 2009, 15, 5121–5128. [Google Scholar] [CrossRef]
- Burman, P.; Karlsson, F.A.; Lööf, L.; Axelsson, C.K.; Szesci, P.B.; Borch, K. H+,K+-ATPase antibodies in autoimmune gastritis: Observations on the development of pernicious anemia. Scand. J. Gastroenterol. 1991, 26, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Norman, G.L.; Severi, C.; Encabo, S.; Shums, Z.; Vannella, L.; Delle Fave, G.; Annibale, B. Reassessment of intrinsic factor and parietal cell autoantibodies in atrophic gastritis with respect to cobalamin deficiency. Am. J. Gastroenterol. 2009, 104, 2071–2079. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Gentile, G.; Purchiaroni, F.; Mora, B.; Simmaco, M.; Annibale, B. Single nucleotide polymorphisms related to vitamin B12 serum levels in autoimmune gastritis patients with or without pernicious anaemia. Dig. Liver Dis. 2015, 47, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Jin, Z.; Cui, R.; Ding, S.; Huang, Y.; Zhou, L. Autoimmune metaplastic atrophic gastritis in chinese: A study of 320 patients at a large tertiary medical center. Scand. J. Gastroenterol. 2017, 52, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Kalkan, Ç.; Soykan, I. Differences between older and young patients with autoimmune gastritis. Geriatr. Gerontol. Int. 2017, 17, 1090–1095. [Google Scholar] [CrossRef]
- Carabotti, M.; Lahner, E.; Esposito, G.; Sacchi, M.C.; Severi, C.; Annibale, B. Upper gastrointestinal symptoms in autoimmune gastritis: A cross-sectional study. Medicine (Baltim.) 2017, 96, e5784. [Google Scholar] [CrossRef]
- Villanacci, V.; Casella, G.; Lanzarotto, F.; Di Bella, C.; Sidoni, A.; Cadei, M.; Salviato, T.; Dore, M.P.; Bassotti, G. Autoimmune gastritis: Relationships with anemia and Helicobacter pylori status. Scand. J. Gastroenterol. 2017, 52, 674–677. [Google Scholar] [CrossRef]
- Lenti, M.V.; Miceli, E.; Cococcia, S.; Klersy, C.; Staiani, M.; Guglielmi, F.; Giuffrida, P.; Vanoli, A.; Luinetti, O.; De Grazia, F.; et al. Determinants of diagnostic delay in autoimmune atrophic gastritis. Aliment. Pharmacol. Ther. 2019, 50, 167–175. [Google Scholar] [CrossRef]
- Lenti, M.V.; Miceli, E.; Padula, D.; Colleoni, R.; Beneventi, F.; Corazza, G.R.; Di Sabatino, A. Infertility and recurrent miscarriage in a patient with autoimmune atrophic gastritis. Intern. Emerg. Med. 2018, 13, 815–816. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef]
- Lenti, M.V.; Miceli, E.; Padula, D.; Di Sabatino, A.; Corazza, G.R. The challenging diagnosis of autoimmune atrophic gastritis. Scand. J. Gastroenterol. 2017, 52, 471–472. [Google Scholar] [CrossRef] [PubMed]
- Di Sabatino, A.; Biagi, F.; Lenzi, M.; Frulloni, L.; Lenti, M.V.; Giuffrida, P.; Corazza, G.R. Clinical usefulness of serum antibodies as biomarkers of gastrointestinal and liver diseases. Dig. Liver Dis. 2017, 49, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Tozzoli, R.; Kodermaz, G.; Perosa, A.R.; Tampoia, M.; Zucano, A.; Antico, A.; Bizzaro, N. Autoantibodies to parietal cells as predictors of atrophic body gastritis: A five-year prospective study in patients with autoimmune thyroid diseases. Autoimmun. Rev. 2010, 10, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Rugge, M.; Meggio, A.; Pennelli, G.; Piscioli, F.; Giacomelli, L.; De Pretis, G.; Graham, D.Y. Gastritis staging in clinical practice: The OLGA staging system. Gut 2007, 56, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Capelle, L.G.; de Vries, A.C.; Haringsma, J.; Ter Borg, F.; de Vries, R.A.; Bruno, M.J.; van Dekken, H.; Meijer, J.; van Grieken, N.C.; Kuipers, E.J. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest. Endosc. 2010, 71, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Toh, B.H. Pathophysiology and laboratory diagnosis of pernicious anemia. Immunol. Res. 2017, 65, 326–330. [Google Scholar] [CrossRef]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System; WHO/NMH/NHD/MNM/11.1; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Hershko, C.; Camaschella, C. How I treat unexplained refractory iron deficiency anemia. Blood 2014, 123, 326–333. [Google Scholar] [CrossRef]
- Bergamaschi, G.; Markopoulos, K.; Albertini, R.; Di Sabatino, A.; Biagi, F.; Ciccocioppo, R.; Arbustini, E.; Corazza, G.R. Anemia of chronic disease and defective erythropoietin production in patients with celiac disease. Haematologica 2008, 93, 1785–1791. [Google Scholar] [CrossRef]
- Bergamaschi, G.; Di Sabatino, A.; Albertini, R.; Ardizzone, S.; Biancheri, P.; Bonetti, E.; Cassinotti, A.; Cazzola, P.; Markopoulos, K.; Massari, A.; et al. Prevalence and pathogenesis of anemia in inflammatory bowel disease. Influence of anti-tumor necrosis factor-alpha treatment. Haematologica 2010, 95, 199–205. [Google Scholar] [CrossRef]
- Miceli, E.; Padula, D.; Lenti, M.V.; Gallia, A.; Albertini, R.; Di Stefano, M.; Klersy, C.; Corazza, G.R. A laboratory score in the diagnosis of autoimmune atrophic gastritis: A prospective study. J. Clin. Gastroenterol. 2015, 49, e1–e5. [Google Scholar] [CrossRef]
- Annibale, B.; Capurso, G.; Chistolini, A.; D’Ambra, G.; DiGiulio, E.; Monarca, B.; DelleFave, G. Gastrointestinal causes of refractory iron deficiency anemia in patients without gastrointestinal symptoms. Am. J. Med. 2001, 111, 439–445. [Google Scholar] [CrossRef]
- Miceli, E.; Vanoli, A.; Lenti, M.V.; Klersy, C.; Di Stefano, M.; Luinetti, O.; Dominioni, C.C.; Pisati, M.; Staiani, M.; Gentile, A.; et al. Natural history of autoimmune atrophic gastritis: A prospective, single-institution, long-term experience. Aliment. Pharmacol. Ther. 2019, 50, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Zagari, R.M.; Zullo, A.; Di Sabatino, A.; Meggio, A.; Cesaro, P.; Lenti, M.V.; Annibale, B.; Corazza, G.R. Chronic atrophic gastritis: Natural history, diagnosis and therapeutic management. A position paper by the Italian Society of Hospital Gastroenterologists and Digestive Endoscopists (AIGO), the Italian Society of Digestive Endoscopy (SIED), the Italian Society of Gastroenterology (SIGE), and the Italian Society of Internal Medicine (SIMI). Dig. Liver Dis. 2019. [Google Scholar] [CrossRef]
- Capurso, G.; Marignani, M.; Delle Fave, G.; Annibale, B. Iron-deficiency anemia in premenopausal women: Why not consider atrophic body gastritis and Helicobacter pylori role? Am. J. Gastroenterol. 1999, 10, 3084–3085. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.V.; Ferrucci, L.; Ershler, W.B.; Longo, D.L.; Guralnik, J.M. Red blood cell distribution width and the risk of death in middle-aged and older adults. Arch. Intern. Med. 2009, 169, 515–523. [Google Scholar] [CrossRef]
- De Re, V.; Repetto, O.; De Zorzi, M.; Casarotto, M.; Tedeschi, M.; Giuffrida, P.; Lenti, M.V.; Magris, R.; Miolo, G.; Mazzon, C.; et al. Polymorphism in toll-like receptors and Helicobacter pylori motility in autoimmune atrophic gastritis and gastric cancer. Cancers 2019, 11, 648. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Setting | Patients (n) | Enrolled at AAG Diagnosis | Mean Age (years) | Overall Anaemia (%) | PA (%) | IDA (%) | Major Findings |
|---|---|---|---|---|---|---|---|---|---|
| Burman et al. [11] | 1991 | Internal medicine | 86 | Yes | 56 | 80.2 | 80.2 | NA | High PCA levels associated with PA |
| Hersko et al. [6] | 2006 | Haematology | 160 | NS | 59 | 75.0 | 18.1 | 51.8 | Microcytic anaemia more common in younger age |
| Lahner et al. [12] | 2009 | Gastroenterology | 165 | Yes | 54 | 94.5 | 49.0 | 45.5 | PCA and anti-intrinsic factor antibodies yield 73% accuracy PA diagnosis |
| Miceli et al. [4] | 2012 | Gastroenterology | 99 | Yes | 58 | 59.6 | 59.6 | 0 | PA was the most common cause of AAG diagnosis |
| Lahner et al. [13] | 2015 | Gastroenterology | 83 | Yes | 59 | 51.8 | 51.8 | NA | A genetic variant of transcobalamin 2 was related to PA |
| Zhang et al. [14] | 2017 | Gastroenterology | 275 | Yes | 61 | 19.3 | 5.4 | 8.4 | No clear gender differences; microcytic anaemia more common in younger age |
| Kalkan et al. [15] | 2017 | Gastroenterology | 355 | NS | 57 | 30.1 | 30.1 | NA | PA more common in older patients |
| Carabotti et al. [16] | 2017 | Gastroenterology | 379 | Yes | 55 | 88.4 | 53.6 | 34.8 | PA more frequent in patients without gastrointestinal symptoms |
| Villanacci et al. [17] | 2017 | Pathology | 138 | NS | 48 | 54.7 | 25.0 | 29.7 | IDA more common than PA |
| Lenti et al. [18] | 2019 | Gastroenterology | 291 | Yes | 60 | 49.5 | 23.4 | 11.7 | Isolated MCV alterations associated with greater AAG diagnostic delay |
| Demographic Features | |
|---|---|
| Total AAG patients, n | 654 |
| Females, n (%) | 459 (70.2) |
| Age (years), median (range) | 61 (18–88) |
| Main clinical presentation at diagnosis, n (%) | |
| Haematological | 368 (56.3) |
| Gastrointestinal | 109 (16.7) |
| Neuropsychiatric | 105 (16.1) |
| Endocrinological | 23 (3.5) |
| Miscellaneous | 53 (8.1) |
| Other relevant clinical information, n (%) | |
| Current or past smoking | 246 (37.7) |
| Cardiovascular disease | 384 (58.7) |
| Autoimmune comorbidities | 305 (46.7) |
| Neuropsychiatric disorders | 180 (27.5) |
| Family history of AAG | 55 (8.4) |
| Family history of gastric cancer | 16 (2.4) |
| Proton pump inhibitor use prior to diagnosis | 237 (36.3) |
| Previously treated H. pylori infection | 97 (14.8) |
| Presence of Anaemia | Absence of Anaemia | p-Value | |
|---|---|---|---|
| Female gender | 220/459 (47.9) | 239/459 (52.1) | 0.8916 |
| Male gender | 96/195 (49.2) | 99/195 (50.8) | 0.9563 |
| Age (years) mean ± SD | 60.1 ± 15.8 | 59.3 ± 13.9 | 0.5061 |
| Age groups (years) | |||
| ≥80 | 31 (10.0) | 10 (3.0) | Trend 0.5463 |
| 70–79 | 74 (23.9) | 82 (24.8) | |
| 60–69 | 64 (20.6) | 89 (26.8) | |
| 50–59 | 47 (15.2) | 73 (22.0) | |
| 40–49 | 61 (19.7) | 41 (12.3) | |
| 30–39 | 24 (7.7) | 32 (9.6) | |
| ≤29 | 9 (2.9) | 5 (1.5) | |
| Current or past smoking | 103/300 (34.3) | 114/324 (35.2) | 0.8894 |
| Gastrointestinal symptoms | 32/302 (10.6) | 75/310 (24.2) | <0.0001 |
| Endocrinological disorders | 7/302 (2.3) | 16/312 (5.1) | 0.1050 |
| Cardiovascular disease | 178/301 (59.1) | 188/317 (59.3) | 0.9674 |
| Neuropsychiatric disorders | 80/297 (26.9) | 90/313 (28.7) | 0.6816 |
| Autoimmune comorbidities | 130/305 (42.6) | 165/325 (50.8) | 0.0491 |
| Autoimmune thyroid disease | 108/303 (35.6) | 143/325 (44.0) | 0.0399 |
| Family history of AAG | 19/296 (6.4) | 33/314 (10.5) | 0.1136 |
| Family history of gastric cancer | 6/296 (2.0) | 9/314 (2.9) | 0.6838 |
| PPI use prior to diagnosis | 63/216 (29.2) | 97/223 (43.5) | 0.0025 |
| Previous H. pylori infection | 26/276 (9.4) | 61/311 (19.6) | 0.0008 |
| Macrocytosis | 108/303 (35.6) | 48/317 (15.1) | <0.0001 |
| Microcytosis | 105/303 (34.6) | 28/317 (8.8) | <0.0001 |
| Normocytosis | 90/303 (29.7) | 241/317 (76.0) | <0.0001 |
| Vitamin B12 deficiency | 167/278 (60.1) | 124/303 (40.9) | <0.0001 |
| Iron deficiency | 163/280 (58.2) | 164/286 (57.3) | 0.9007 |
| Folate deficiency | 24/165 (14.5) | 10/201 (4.9) | 0.0031 |
| Vitamin B12 and iron deficiency | 72/263 (27.4) | 64/279 (22.9) | 0.2749 |
| Increased RDW | 227/277 (81.9) | 113/289 (39.1) | <0.0001 |
| Thrombocytopenia | 69/294 (23.5) | 23/310 (7.4) | <0.0001 |
| Thrombocytosis | 6/294 (2.0) | 7/310 (2.2) | 0.9231 |
| Intestinal metaplasia | 246/310 (79.3) | 258/332 (77.7) | 0.6814 |
| Pseudopyloric metaplasia | 196/301 (65.1) | 194/317 (61.2) | 0.3547 |
| OLGA 1 OLGA 2 | 22/269 (8.2) 247/269 (91.8) | 30/280 (10.7) 250/280 (89.3) | Trend 0.3851 |
| OLGIM 0 OLGIM 1 OLGIM 2 OLGIM 3 | 56/269 (20.8) 102/269 (37.9) 111/269 (41.3) 0 (0) | 56/280 (20.0) 106/280 (37.9) 114/280 (40.7) 4/280 (1.4) | Trend 0.6349 |
| Variables | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Autoimmune comorbidities | 0.67 | 0.2306–1.9532 | 0.4644 |
| No history of H. pylori infection | 1.48 | 0.7288–3.0118 | 0.2775 |
| Thrombocytopenia | 3.27 | 1.4596–7.3507 | 0.0040 |
| Increased RDW | 10.65 | 6.1381–18.5012 | <0.0001 |
| Absence of gastrointestinal symptoms | 2.26 | 1.1048–4.6312 | 0.0256 |
| Autoimmune thyroid disease | 0.92 | 0.3127–2.7167 | 0.8825 |
| Vitamin B12 deficiency | 1.09 | 0.6359–1.8960 | 0.7371 |
| No PPI use prior to diagnosis | 1.98 | 1.1071–3.5423 | 0.0213 |
| PCA positivity | 0.92 | 0.4873–1.7438 | 0.8024 |
| Age < 50 years | 0.67 | 0.3830–1.1922 | 0.1760 |
| Family history of gastric cancer | 0.45 | 0.0823–2.5594 | 0.3744 |
| No family history of AAG | 1.77 | 0.7096-4.4185 | 0.2207 |
| Current or past smoking | 0.78 | 0.4638-1.3122 | 0.3494 |
| Autoimmune comorbidities | 0.51 | 0.1683-1.5950 | 0.2517 |
| No history of H. pylori infection | 1.69 | 0.8029-3.5970 | 0.1657 |
| Absence of thrombocytopenia | 2.20 | 1.0789-4.5053 | 0.0301 |
| Increased RDW | 4.83 | 2.7097-8.6409 | <0.0001 |
| Female gender | 1.47 | 0.8227-2.6430 | 0.1921 |
| PCA positivity | 1.39 | 0.6535-2.9741 | 0.3900 |
| Age < 50 years | 0.66 | 0.3372-1.3286 | 0.2511 |
| No family history of AAG | 1.26 | 0.4861-3.3118 | 0.6266 |
| Current or past smoking | 1.13 | 0.6082-2.1290 | 0.6860 |
| Autoimmune comorbidities | 0.60 | 0.1775-2.0391 | 0.4145 |
| No history of H. pylori infection | 2.98 | 1.1249-7.9012 | 0.0280 |
| Thrombocytopenia | 3.51 | 1.7113-7.2044 | 0.0006 |
| Increased RDW | 6.40 | 3.1210-13.1643 | <0.0001 |
| Female gender | 0.33 | 0.38 to 1.42 | 0.3663 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenti, M.V.; Lahner, E.; Bergamaschi, G.; Miceli, E.; Conti, L.; Massironi, S.; Cococcia, S.; Zilli, A.; Caprioli, F.; Vecchi, M.; et al. Cell Blood Count Alterations and Patterns of Anaemia in Autoimmune Atrophic Gastritis at Diagnosis: A Multicentre Study. J. Clin. Med. 2019, 8, 1992. https://doi.org/10.3390/jcm8111992
Lenti MV, Lahner E, Bergamaschi G, Miceli E, Conti L, Massironi S, Cococcia S, Zilli A, Caprioli F, Vecchi M, et al. Cell Blood Count Alterations and Patterns of Anaemia in Autoimmune Atrophic Gastritis at Diagnosis: A Multicentre Study. Journal of Clinical Medicine. 2019; 8(11):1992. https://doi.org/10.3390/jcm8111992
Chicago/Turabian StyleLenti, Marco Vincenzo, Edith Lahner, Gaetano Bergamaschi, Emanuela Miceli, Laura Conti, Sara Massironi, Sara Cococcia, Alessandra Zilli, Flavio Caprioli, Maurizio Vecchi, and et al. 2019. "Cell Blood Count Alterations and Patterns of Anaemia in Autoimmune Atrophic Gastritis at Diagnosis: A Multicentre Study" Journal of Clinical Medicine 8, no. 11: 1992. https://doi.org/10.3390/jcm8111992
APA StyleLenti, M. V., Lahner, E., Bergamaschi, G., Miceli, E., Conti, L., Massironi, S., Cococcia, S., Zilli, A., Caprioli, F., Vecchi, M., Maiero, S., Cannizzaro, R., Corazza, G. R., Annibale, B., & Di Sabatino, A. (2019). Cell Blood Count Alterations and Patterns of Anaemia in Autoimmune Atrophic Gastritis at Diagnosis: A Multicentre Study. Journal of Clinical Medicine, 8(11), 1992. https://doi.org/10.3390/jcm8111992