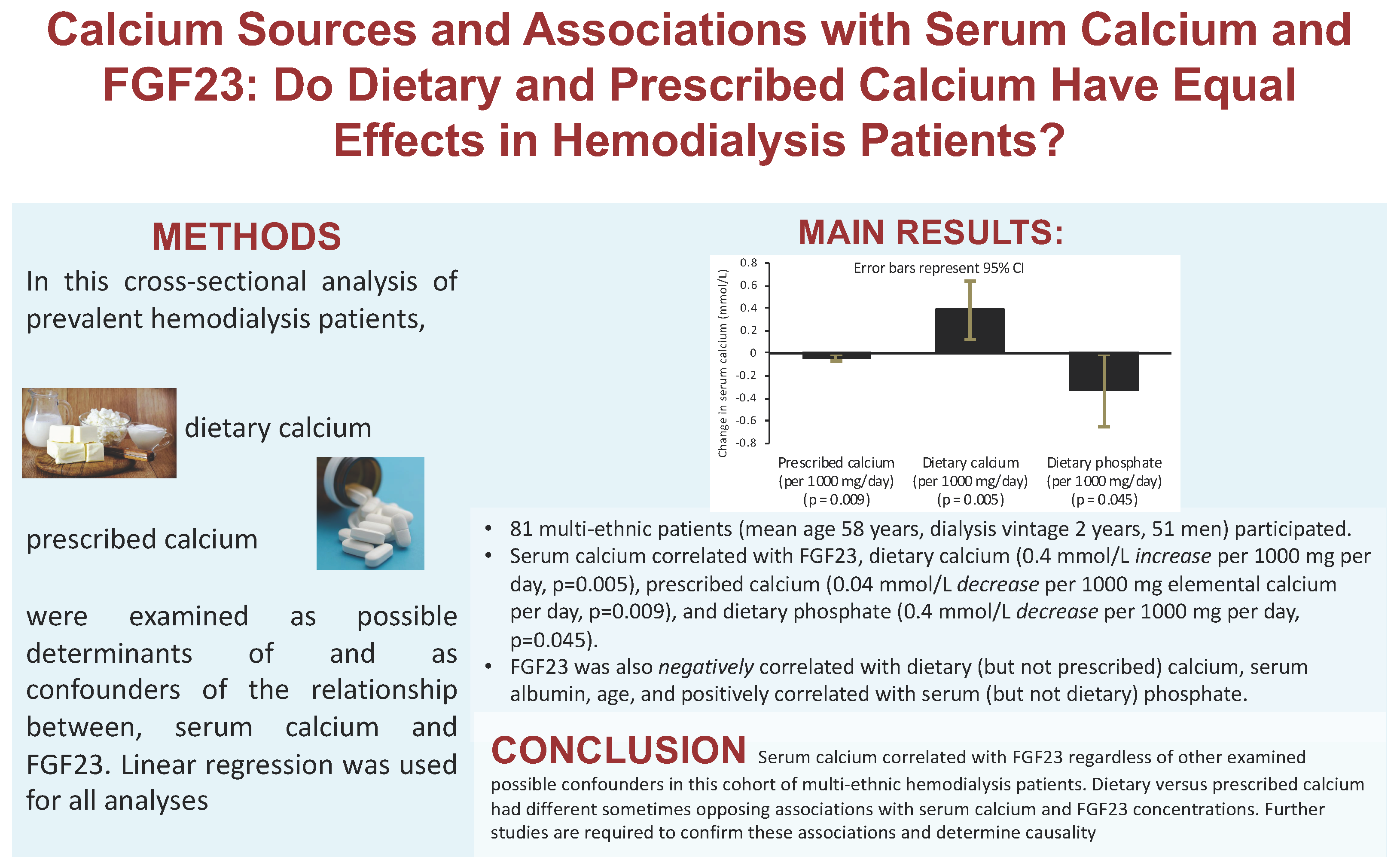
Associations of Calcium from Food Sources versus Phosphate Binders with Serum Calcium and FGF23 in Hemodialysis Patients

 , , and
, , and
Abstract

1. Introduction
2. Methods
2.1. Ethical Statement
2.2. Selection Criteria and Study Design
2.3. Outcome Measurements
2.4. Statistical Analysis
3. Results
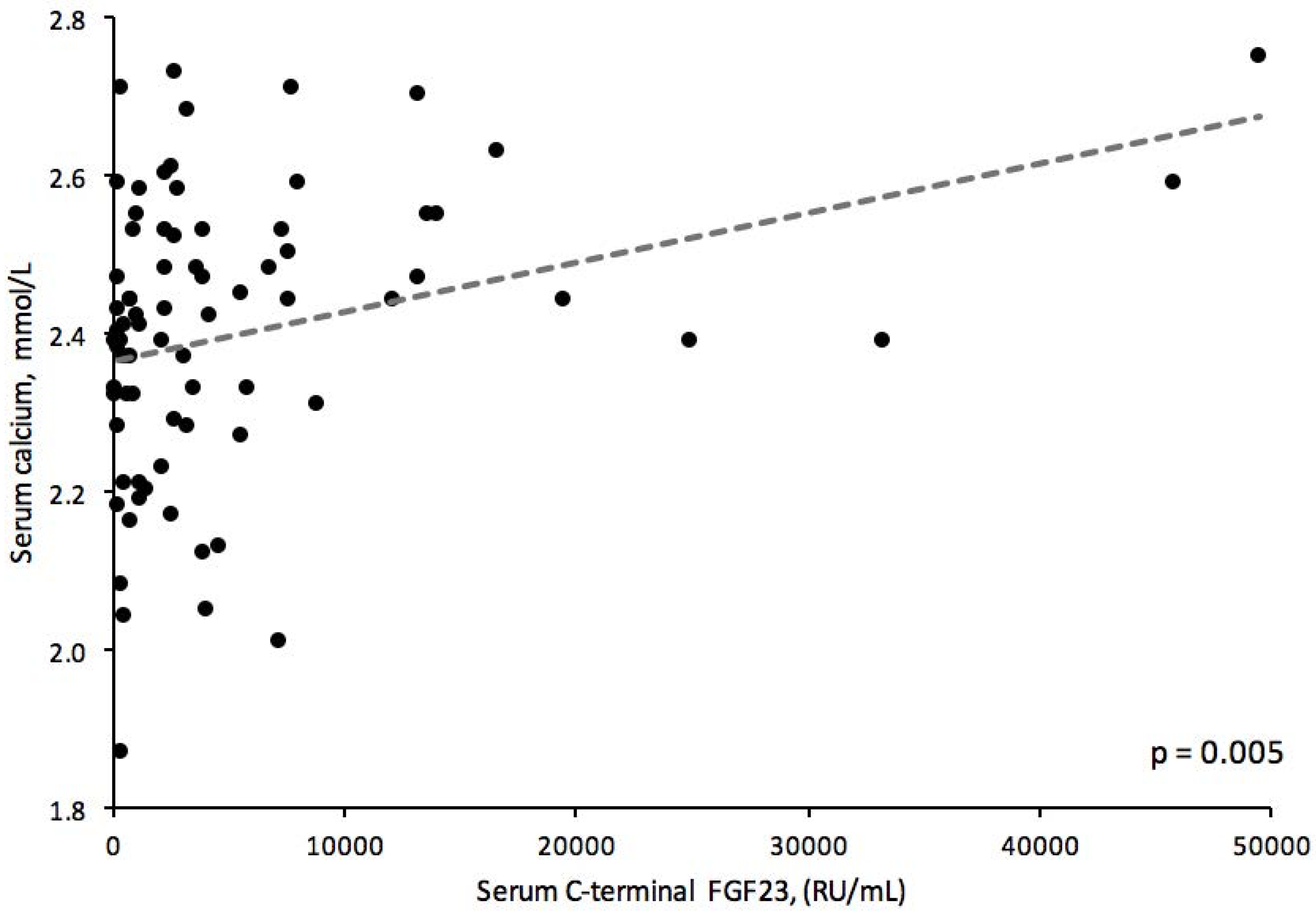
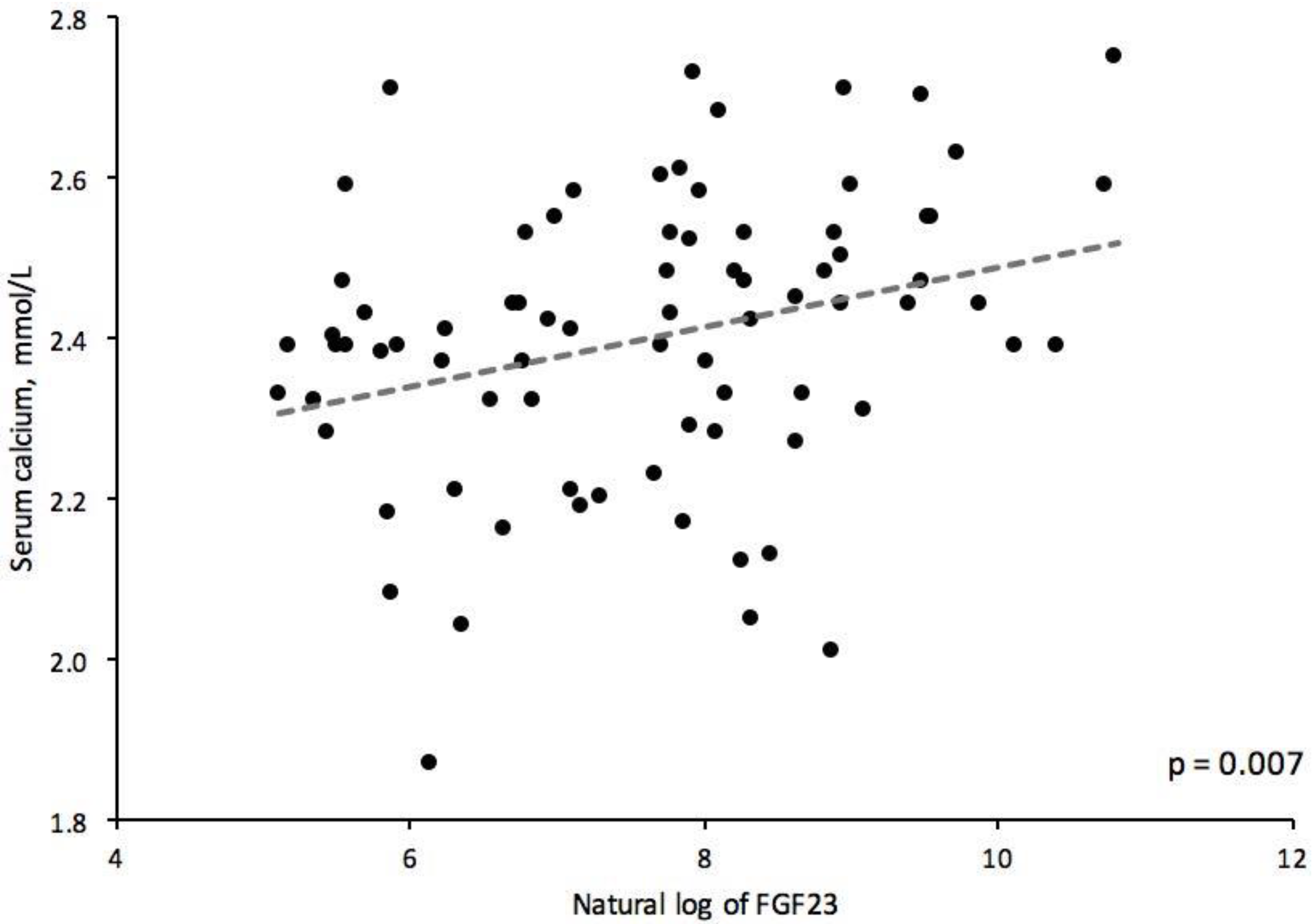
3.1. Bivariable Analyses
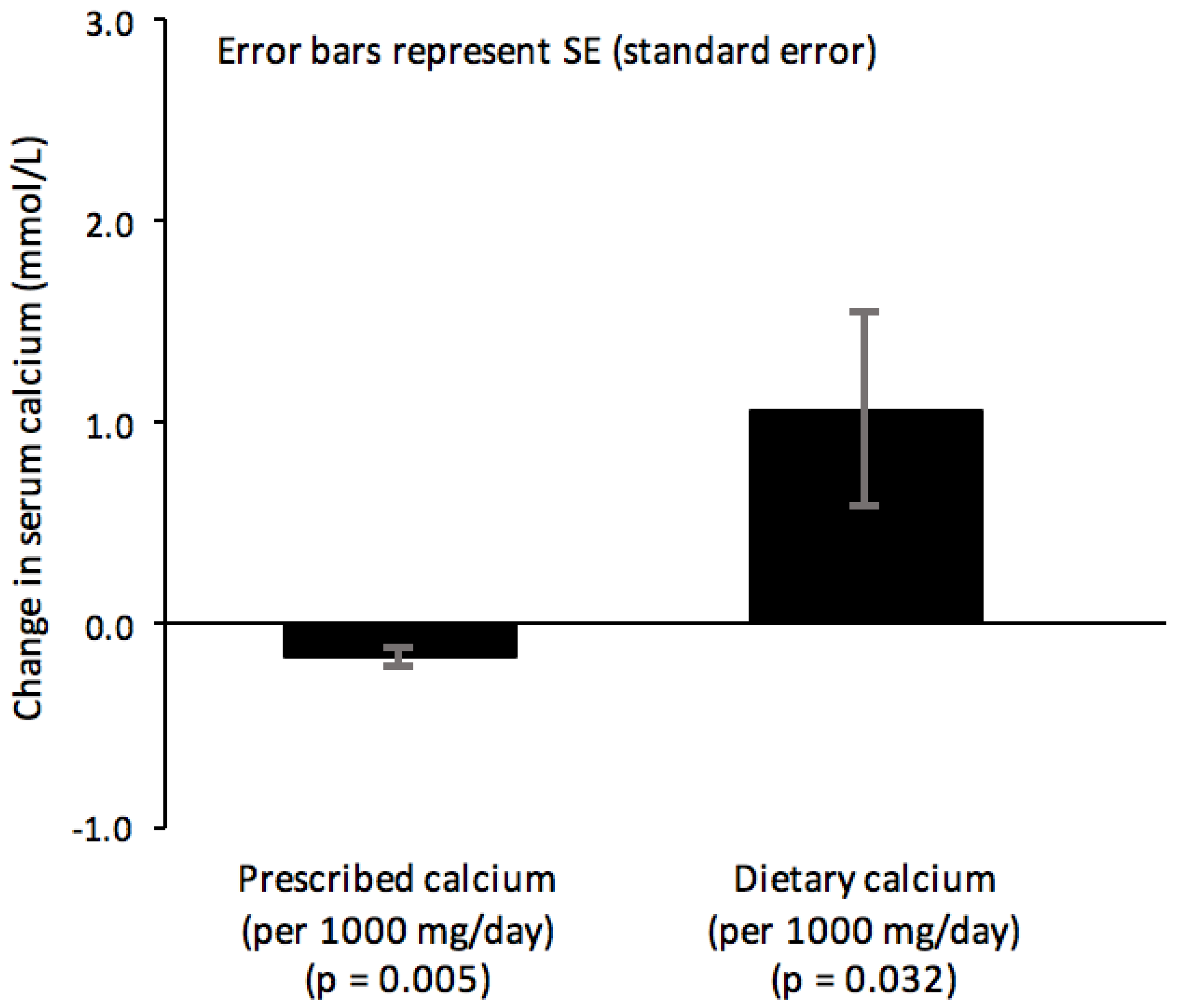
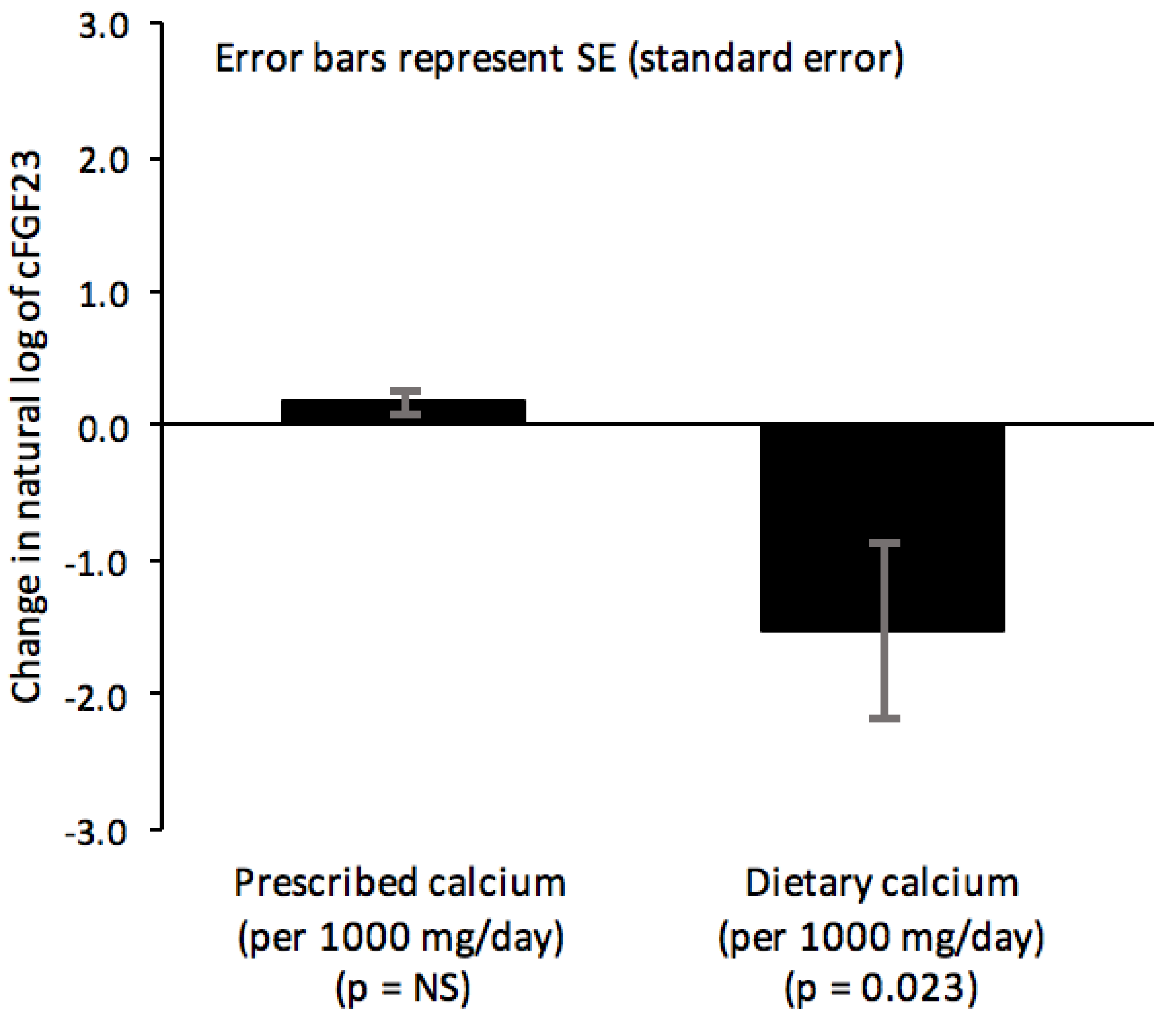
3.2. Multivariable Models
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- O’Neill, W.C. Targeting serum calcium in chronic kidney disease and end-stage renal disease: Is normal too high? Kidney Int. 2016, 89, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Isakova, T.; Xie, H.; Yang, W.; Xie, D.; Anderson, A.H.; Scialla, J.; Wahl, P.; Gutiérrez, O.M.; Steigerwalt, S.; He, J.; et al. Chronic Renal Insufficiency Cohort (CRIC) Study Group. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 2011, 305, 2432–2439. [Google Scholar] [CrossRef] [PubMed]
- Imanishi, Y.; Inaba, M.; Nakatsuka, K.; Nagasue, K.; Okuno, S.; Yoshihara, A.; Miura, M.; Miyauchi, A.; Kobayashi, K.; Miki, T.; et al. FGF23 in patients with end-stage renal disease on hemodialysis. Kidney Int. 2004, 65, 1943–1946. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ortiz, M.E.; Lopez, I.; Muñoz-Castañeda, J.R.; Martinez-Moreno, J.M.; Ramírez, A.P.; Pineda, C.; Canalejo, A.; Jaeger, P.; Aguilera-Tejero, E.; Rodriguez, M.; et al. Calcium deficiency reduces circulating levels of FGF23. J. Am. Soc. Nephrol. 2012, 23, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, X.; Zhou, Y.; Li, S.; Chen, Y.; Wang, Y.; Lou, T. New Conclusions Regarding Comparison of Sevelamer and Calcium-based phosphate binders in Coronary-Artery Calcification for Dialysis Patients: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2015, 10, e0133938. [Google Scholar] [CrossRef] [PubMed]
- Soriano, S.; Ojeda, R.; Rodríguez, M.; Almadén, Y.; Rodríguez, M.; Martín-Malo, A.; Aljama, P. The effect of phosphate binders, calcium and lanthanum carbonate on FGF23 levels in chronic kidney disease patients. Clin. Nephrol. 2013, 80, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Grahame, J.E. Calcium-based phosphate binders; down, but not out. Nephrol. Dial. Transplant. 2017, 32, 5–8. [Google Scholar] [CrossRef][Green Version]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A Malnutrition-Inflammation Score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [PubMed]
- Hirotugu, A. A new look at the statistical model identification. IEEE Trans. Autom. Control 1974, 19, 716–723. [Google Scholar] [CrossRef]
- Singh, R.J.; Kumar, R. Fibroblast growth factor 23 concentrations in humoral hypercalcemia of malignancy and hyperparathyroidism. Mayo Clin. Proc. 2003, 78, 826–829. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Imanishi, Y.; Miyauchi, A.; Onoda, N.; Kawata, T.; Tahara, H.; Goto, H.; Miki, T.; Ishimura, E.; Sugimoto, T.; et al. Regulation of plasma fibroblast growth factor 23 by calcium in primary hyperparathyroidism. Eur. J. Endocrinol. 2006, 154, 93–99. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kovesdy, C.P.; Quarles, L.D. Fibroblast growth factor-23: What we know, what we don’t know, and what we need to know. Nephrol. Dial. Transplant. 2013, 28, 2228–2236. [Google Scholar] [CrossRef] [PubMed]
- David, V.; Dai, B.; Martin, A.; Huang, J.; Han, X.; Quarles, L.D. Calcium regulates FGF23 expression in bone. Endocrinology 2013, 154, 4469–4482. [Google Scholar] [CrossRef] [PubMed]
- Raggi, P.; Vukicevic, S.; Moysés, R.M.; Wesseling, K.; Spiegel, D.M. Ten-year experience with sevelamer and calcium salts as phosphate binders. Clin. J. Am. Soc. Nephrol. 2010, 1, S31–S40. [Google Scholar] [CrossRef] [PubMed]
- Bristow, S.M.; Gamble, G.D.; Stewart, A.; Kalluru, R.; Horne, A.M.; Reid, I.R. Acute effects of calcium citrate with or without a meal, calcium-fortified juice and a dairy product meal on serum calcium and phosphate: A randomized cross-over trial. Br. J. Nutr. 2015, 113, 1585–1594. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.J.; Kruszka, B.; Delaney, J.A.; He, K.; Burke, G.L.; Alonso, A.; Bild, D.E.; Budoff, M.; Michos, E.D. Calcium Intake from Diet and Supplements and the Risk of Coronary Artery Calcification and its Progression Among Older Adults: 10-Year Follow-up of the Multi-Ethnic Study of Atherosclerosis (MESA). J. Am. Heart Assoc. 2016, 11, 5. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age, mean ± SD, years | 58.28 ± 14.09 |
| Female, number (%) | 30 (37%) |
| History of diabetes mellitus, number (%) | 31 (38%) |
| Dialysis vintage, mean ± SD, years | 2.51 ± 2.37 |
| Dry weight, mean ± SD, kg | 71.97 ± 17.37 |
| Ethnicity, number (%) White South Asian East Asian Black | 16 (20%) 24 (30%) 28 (35%) 12 (15%) |
| Serum cFGF23, median (IQR)[range], RU/mL | 2396 (586 to 5896) [468 to 49,479] |
| Natural log of FGF23 | 7.64 ± 1.44 |
| Serum calcium, mean ± SD, mmol/L | 2.40 ± 0.18 |
| Serum phosphate, mean ± SD, mmol/L | 1.60 ± 0.50 |
| Serum parathyroid hormone, median (IQR)[range], pmol/L | 34.30 (21.30 to 79.80) [1 to 363] |
| Serum albumin, mean ± SD, gm/L | 33.83 ± 3.32 |
| Serum 25-OH vitamin D, median (IQR)[range], pmol/L Serum hemoglobin, mean ± SD, mg/L Serum ferritin, median (IQR)[range], mcg/L Transferrin saturation, median (IQR)[range], % | 39 (25 to 56) [10 to 128] 114 ± 12.3 95.5 (40 to 346) [2 to 1097] 22 (15 to 31) [6 to 78] |
| Using calcium-based phosphate binder, number (%) | 59 (73%) |
| Prescribed CaCO3 dose, median (IQR)[range], mg/day | 1500 (800 to 2500) [0 to 6250] |
| Prescribed activated vitamin D dose, median (IQR)[range], mcg/day | 0.43 (0.13 to 0.57) [0 to 1.71] |
| Taking supplemental vitamin D, number (%) | 19 (24%) |
| Dietary calcium, median (IQR)[range], mg/day | 424.09 (301.13 to 626.12) [14.58 to 1037.04] |
| Dietary phosphate, median (IQR)[range], mg/day | 831.09 (606.84 to 1026.69) [337.90 to 1645.16] |
| Dietary vitamin D, median (IQR)[range], mcg/day | 1.66 (0.81 to 2.84) [0 to 22.74] |
| Dietary protein, median (IQR)[range], gm/day | 66.35 (53.01 to 92.85) [25.90 to 145.83] |
| Variable | Coefficient (95% CI) | p-Value | Adjusted r2 If Significant (%) |
|---|---|---|---|
| Natural log of FGF23 | 0.04 (0.01 to 0.06) | 0.007 | 7.8 |
| Female | 0.09 (0.01 to 0.17) | 0.037 | 4.2 |
| Non-black race | 0.10 (−0.01 to 0.21) | 0.064 | |
| Parathyroid hormone category | 0.04 (0.00 to 0.08) | 0.071 | |
| Age, years | 0.00 (0.00 to 0.01) | 0.119 | |
| Prescribed CaCO3, 1000 mg/day | −0.02 (−0.05 to 0.01) | 0.157 | |
| Dry weight, kg | 0.00 (0.00 to 0.00) | 0.2 | |
| Activated vitamin D, mcg/day | 0.07 (−0.04 to 0.18) | 0.208 | |
| Caloric intake, kcal/day | 0.00 (0.00 to 0.00) | 0.255 | |
| Dietary calcium, 1000 mg/day | 0.10 (−0.09 to 0.30) | 0.302 | |
| Serum 25-OH vitamin D, pmol/L | 0.03 (−0.04 to 0.11) | 0.368 | |
| Natural log of transferrin saturation | −0.03 (−0.12 to 0.05) | 0.419 | |
| Natural log of dietary vitamin D | 0.00 (−0.02 to 0.01) | 0.445 | |
| Use of a phosphate binder | 0.02 (−0.04 to 0.09) | 0.462 | |
| HD vintage, year | 0.01 (−0.01 to 0.02) | 0.494 | |
| Dietary protein, gm/day | 0.00 (0.00 to 0.00) | 0.508 | |
| Dietary phosphate, 1000 mg/day | 0.04 (−0.10 to 0.19) | 0.552 | |
| Serum phosphate, mmol/L | 0.01 (−0.007 to 0.09) | 0.755 | |
| Vitamin D supplementation | 0.01 (−0.08 to 0.11) | 0.756 | |
| Albumin, mg/L | 0.00 (−0.01 to 0.01) | 0.827 | |
| Natural log of serum ferritin | 0.00 (−0.03 to 0.03) | 0.909 | |
| Serum hemoglobin, mg/L | 0.00 (0.00 to 0.00) | 0.97 |
| Variable | Coefficient (95% CI) | p-Value | Adjusted r2 If Significant (%) |
|---|---|---|---|
| Serum phosphate, mmol/L | 1.81 (1.17 to 2.45) | <0.001 | 28.5 |
| Serum hemoglobin, mg/L | −0.04 (−0.07 to −0.02) | 0.002 | 11.3 |
| Serum calcium, mmol/L | 2.42 (0.67 to 4.16) | 0.007 | 7.8 |
| Parathyroid hormone category | 0.37 (0.03 to 0.70) | 0.031 | 4.7 |
| Dietary calcium, 1000 mg/day | −1.60 (−3.16 to −0.05) | 0.044 | 4.6 |
| Natural log of serum ferritin | −0.23 (−0.46 to 0.01) | 0.059 | |
| Prescribed CaCO3, 1000 mg/day | 0.22 (−0.03 to 0.47) | 0.08 | |
| Activated vitamin D, mcg/day | 0.79 (−0.12 to 1.70) | 0.089 | |
| Natural log of dietary vitamin D | −0.22 (−0.54 to 0.11) | 0.192 | |
| Age, years | −0.02 (−0.04 to 0.01) | 0.211 | |
| Albumin, mg/L | −0.06 (−0.16 to 0.04) | 0.217 | |
| Dry weight, kg | 0.01 (−0.01 to 0.03) | 0.341 | |
| Caloric intake, kcal/day | 0.00 (0.00 to 0.00) | 0.448 | |
| Non-black race | 0.30 (−0.61 to 1.20) | 0.517 | |
| Use of a phosphate binder | 0.16 (−0.36 to 0.67) | 0.554 | |
| Natural log of transferrin saturation | −0.15 (−0.86 to 0.52) | 0.654 | |
| Dietary protein, gm/day | 0.00 (−0.01 to 0.02) | 0.656 | |
| Vitamin D supplementation | −0.15 (−0.94 to 0.64) | 0.706 | |
| HD vintage, years | −0.03 (−0.20 to 0.14) | 0.743 | |
| Natural log of serum 25-OH vitamin D | −0.09 (−0.72 to 0.54) | 0.772 | |
| Dietary phosphate, 1000 mg/day | 0.14 (−1.05 to 1.34) | 0.81 | |
| Female | 0.01 (−0.67 to 0.68) | 0.985 |
| Variable | Coefficient ± SE | ß Coefficient | p-Value |
|---|---|---|---|
| Natural log of FGF23 | 0.05 ± 0.01 | 0.39 | 0.002 |
| Prescribed CaCO3, per 1000 mg/day | −0.03 ± 0.01 | −0.27 | 0.021 |
| Non-black race | 0.10 ± 0.05 | 0.24 | 0.042 |
| Age, per year | 0.00 ± 0.00 | 0.10 | 0.394 |
| Female | 0.03 ± 0.04 | 0.08 | 0.479 |
| Parathyroid hormone category | 0.00 ± 0.02 | 0.01 | 0.951 |
| Variable | Coefficient ± SE | ß Coefficient | p-Value |
|---|---|---|---|
| Serum phosphate, per mmol/L | 1.42 ± 0.33 | 0.43 | <0.001 |
| Serum calcium, per mmol/L | 2.22 ± 0.84 | 0.25 | 0.011 |
| Natural log of serum ferritin | −0.23 ± 0.10 | –0.22 | 0.02 |
| Serum hemoglobin, per mg/L | −0.02 ± 0.01 | –0.22 | 0.023 |
| Dietary CaCO3, per 1000 mg/day | −1.32 ± 0.62 | –0.20 | 0.038 |
| Parathyroid hormone category | 0.07 ± 0.15 | 0.04 | 0.661 |
| Variable | Coefficient ± SE | ß Coefficient | p-Value |
|---|---|---|---|
| Natural log of FGF23 | 0.05 ± 0.01 | 0.46 | 0.001 |
| Prescribed CaCO3, per 1000 mg/day | −0.04 ± 0.01 | −0.35 | 0.005 |
| Dietary calcium, per 1000 mg/day | 0.27 ± 0.12 | 0.35 | 0.032 |
| Dietary phosphate, per 1000 mg/day | −0.26 ± 0.14 | −0.47 | 0.084 |
| Dietary protein, per gm/day | 0.00 ± 0.00 | 0.62 | 0.008 |
| Non-black race | 0.05 ± 0.05 | 0.14 | 0.282 |
| Dry weight, per kg | 0.00 ± 0.00 | −0.18 | 0.137 |
| Serum hemoglobin, per mg/L | 0.00 ± 0.00 | 0.10 | 0.429 |
| Variable | Coefficient ± SE | ß Coefficient | p-Value |
|---|---|---|---|
| Serum phosphate, per mmol/L | 1.77 ± 0.30 | 0.54 | <0.001 |
| Natural log of serum ferritin | −0.33 ± 0.08 | −0.34 | <0.001 |
| Serum calcium, per mmol/L | 2.18 ± 0.80 | 0.24 | 0.01 |
| Dietary calcium, per 1000 mg/day | −1.53 ± 0.65 | −0.24 | 0.023 |
| Age, per year | −0.02 ± 0.01 | −0.19 | 0.039 |
| Serum hemoglobin, per mg/L | −0.02 ± 0.01 | −0.18 | 0.049 |
| Prescribed CaCO3, per 1000 mg/day | 0.17 ± 0.09 | 0.17 | 0.071 |
| Dietary phosphate, per 1000 mg/day | 0.74 ± 0.47 | 0.16 | 0.118 |
| Albumin, per mg/L | −0.05 ± 0.05 | −0.11 | 0.26 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahdavi, S.; Bellasi, A.; Nagra, K.; Johnston, L.; Tam, P.; Di Iorio, B.; Sikaneta, T. Associations of Calcium from Food Sources versus Phosphate Binders with Serum Calcium and FGF23 in Hemodialysis Patients. J. Clin. Med. 2019, 8, 1680. https://doi.org/10.3390/jcm8101680
Mahdavi S, Bellasi A, Nagra K, Johnston L, Tam P, Di Iorio B, Sikaneta T. Associations of Calcium from Food Sources versus Phosphate Binders with Serum Calcium and FGF23 in Hemodialysis Patients. Journal of Clinical Medicine. 2019; 8(10):1680. https://doi.org/10.3390/jcm8101680
Chicago/Turabian StyleMahdavi, Sara, Antonio Bellasi, Karan Nagra, Luke Johnston, Paul Tam, Biagio Di Iorio, and Tabo Sikaneta. 2019. "Associations of Calcium from Food Sources versus Phosphate Binders with Serum Calcium and FGF23 in Hemodialysis Patients" Journal of Clinical Medicine 8, no. 10: 1680. https://doi.org/10.3390/jcm8101680
APA StyleMahdavi, S., Bellasi, A., Nagra, K., Johnston, L., Tam, P., Di Iorio, B., & Sikaneta, T. (2019). Associations of Calcium from Food Sources versus Phosphate Binders with Serum Calcium and FGF23 in Hemodialysis Patients. Journal of Clinical Medicine, 8(10), 1680. https://doi.org/10.3390/jcm8101680