Gait Classification in Unilateral Cerebral Palsy

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Patients & Methods
2.1. Patients
2.2. Clinical Classification
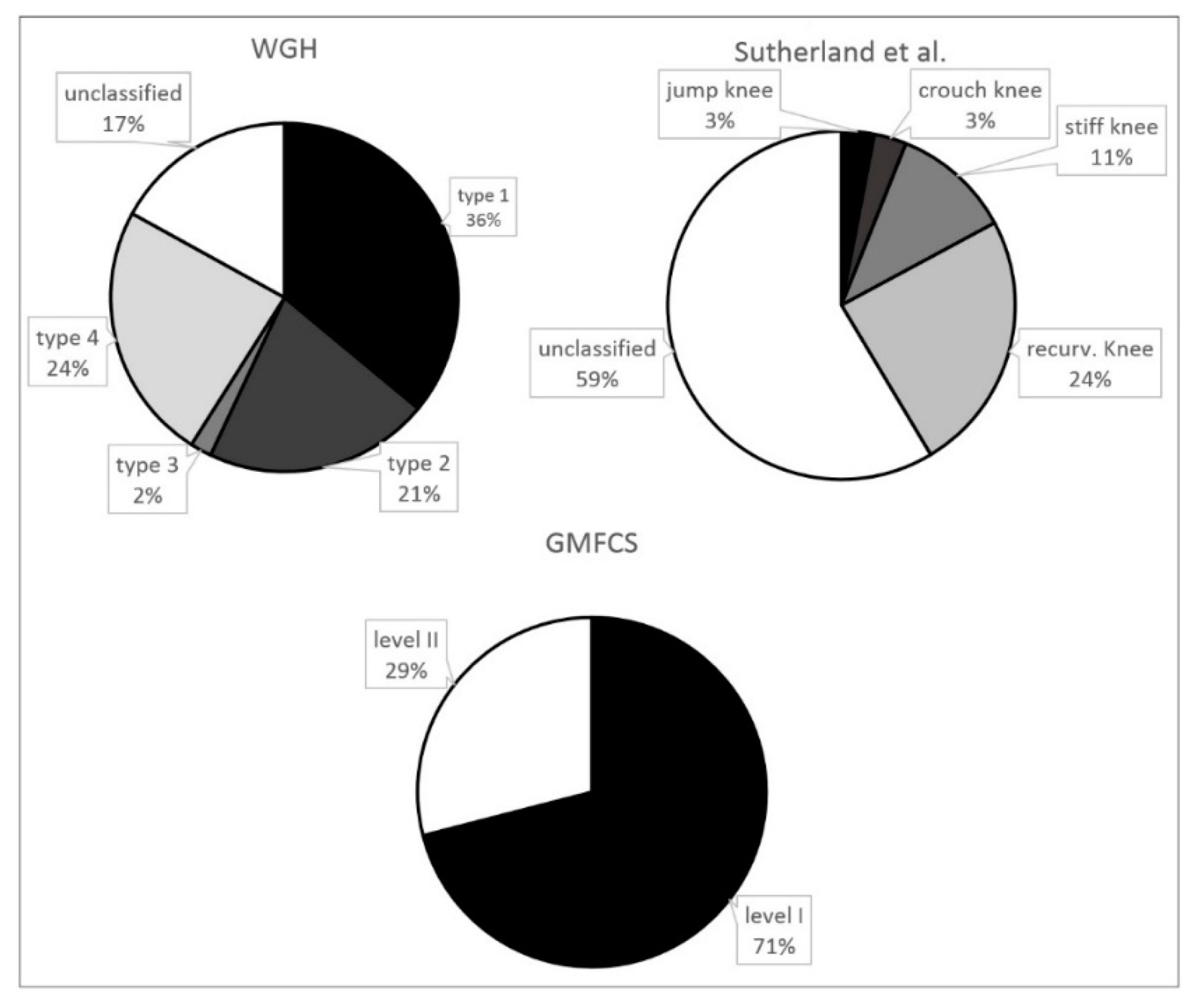
- Gross Motor Function Classification System (GMFCS) [26]
- level I: walking indoors/outdoors (including running and jumping), climbing stairs without support
- level II: walking indoors/outdoors, climbing stairs with a railing
- level III: walking indoors/outdoors with assistive mobility devices
- level IV: walking ability severely limited even with assistive devices; using wheelchairs most of the time
- level V: impaired in all areas of motor function
- the classification system of WGH [17]
- type I: plantar flexion of the ankle in the swing phase with equinus deformity at initial contact and adequate dorsiflexion in the stance phase
- type II: persistent plantar flexion of the ankle during the stance and swing phases
- type III: plantar flexion of the ankle, progression of proximal involvement, and more limited flexion of the knee during the swing phase
- type IV: plantar flexion of the ankle, restricted motion of the knee joint, and limited flexion–extension of the hip
- the classification system of Sutherland et al. [21]
- crouch gait: minimum knee flexion in stance phase > 30°
- jump knee gait: first peak knee flexion > 30° followed by minimum flexion in single support from 10° to 20°
- stiff knee gait: peak knee flexion in swing phase limited to a maximum of 45° or late peak knee flexion in more than 30% of the swing phase
- recurvatum knee gait: knee extension > 0° in stance phase
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.P.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral palsy. Nat. Rev. Dis. Primers 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- Colver, A.; Fairhurst, C.; Pharoah, P.O. Cerebral palsy. Lancet 2014, 383, 1240–1249. [Google Scholar] [CrossRef]
- Van Drongelen, S.; Dreher, T.; Heitzmann, D.W.; Wolf, S.I. Gait patterns in twins with cerebral palsy: Similarities and development over time after multilevel surgery. Res. Dev. Disabil. 2013, 34, 1595–1601. [Google Scholar] [CrossRef] [PubMed]
- Senst, S. Unilateral Spastic Cerebral Palsy (Hemiparesis). Der Orthopade 2014, 43, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Dobson, F.; Morris, M.E.; Baker, R.; Graham, H.K. Unilateral cerebral palsy: A population-based study of gait and motor function. Dev. Med. Child Neurol. 2011, 53, 429–435. [Google Scholar] [CrossRef]
- El-Shamy, S.M.; Abdelaal, A.A. WalkAide Efficacy on Gait and Energy Expenditure in Children with Hemiplegic Cerebral Palsy: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2016, 95, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Dequeker, G.; Van Campenhout, A.; Feys, H.; Molenaers, G. Evolution of self-care and functional mobility after single-event multilevel surgery in children and adolescents with spastic diplegic cerebral palsy. Dev. Med. Child Neurol. 2018, 60, 505–512. [Google Scholar] [CrossRef]
- Marconi, V.; Hachez, H.; Renders, A.; Docquier, P.L.; Detrembleur, C. Mechanical work and energy consumption in children with cerebral palsy after single-event multilevel surgery. Gait Posture 2014, 40, 633–639. [Google Scholar] [CrossRef]
- Tieman, B.; Palisano, R.J.; Gracely, E.J.; Rosenbaum, P.L. Variability in mobility of children with cerebral palsy. Pediatr. Phys. Ther. 2007, 19, 180–187. [Google Scholar] [CrossRef]
- Attias, M.; Chevalley, O.; Bonnefoy-Mazure, A.; De Coulon, G.; Cheze, L.; Armand, S. Effects of contracture on gait kinematics: A systematic review. Clin. Biomech. 2016, 33, 103–110. [Google Scholar] [CrossRef]
- Wren, T.A.; Rethlefsen, S.; Kay, R.M. Prevalence of specific gait abnormalities in children with cerebral palsy: Influence of cerebral palsy subtype, age, and previous surgery. J. Pediatr. Orthop. 2005, 25, 79–83. [Google Scholar] [PubMed]
- Dobson, F.; Morris, M.E.; Baker, R.; Graham, H.K. Gait classification in children with cerebral palsy: A systematic review. Gait Posture 2007, 25, 140–152. [Google Scholar] [CrossRef] [PubMed]
- Lundh, D.; Coleman, S.; Riad, J. Movement deviation and asymmetry assessment with three dimensional gait analysis of both upper and lower extremity results in four different clinical relevant subgroups in unilateral cerebral palsy. Clin. Biomech. 2014, 29, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Kratschmer, R.; Bohm, H.; Doderlein, L. Kinematic adaptation and changes in gait classification in running compared to walking in children with unilateral spastic cerebral palsy. Gait Posture 2019, 67, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, E.; Nieuwenhuys, A.; Vandekerckhove, I.; Van Campenhout, A.; Ortibus, E.; Desloovere, K. Systematic review on gait classifications in children with cerebral palsy: An update. Gait Posture 2019, 69, 209–223. [Google Scholar] [CrossRef]
- Rethlefsen, S.A.; Blumstein, G.; Kay, R.M.; Dorey, F.; Wren, T.A. Prevalence of specific gait abnormalities in children with cerebral palsy revisited: Influence of age, prior surgery, and Gross Motor Function Classification System level. Dev. Med. Child Neurol. 2017, 59, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Winters, T.F., Jr.; Gage, J.R.; Hicks, R. Gait patterns in spastic hemiplegia in children and young adults. J. Bone Joint Surg. Am. 1987, 69, 437–441. [Google Scholar] [PubMed]
- Riad, J.; Haglund-Akerlind, Y.; Miller, F. Classification of spastic hemiplegic cerebral palsy in children. J. Pediatr. Orthop. 2007, 27, 758–764. [Google Scholar] [CrossRef]
- McDowell, B.C.; Kerr, C.; Kelly, C.; Salazar, J.; Cosgrove, A. The validity of an existing gait classification system when applied to a representative population of children with hemiplegia. Gait Posture 2008, 28, 442–447. [Google Scholar] [CrossRef]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Knaflitz, M. Multiple gait patterns within the same Winters class in children with hemiplegic cerebral palsy. Clin. Biomech. 2015, 30, 908–914. [Google Scholar] [CrossRef]
- Sutherland, D.H.; Davids, J.R. Common gait abnormalities of the knee in cerebral palsy. Clin. Orthop. Relat. Res. 1993, 288, 139–147. [Google Scholar]
- De Morais Filho, M.C.; Kawamura, C.M.; Lopes, J.A.; Neves, D.L.; Cardoso Mde, O.; Caiafa, J.B. Most frequent gait patterns in diplegic spastic cerebral palsy. Acta Ortop. Bras. 2014, 22, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Klotz, M.C.; Wolf, S.I.; Heitzmann, D.; Maier, M.W.; Braatz, F.; Dreher, T. The association of equinus and primary genu recurvatum gait in cerebral palsy. Res. Dev. Disabil. 2014, 35, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Domagalska, M.E.; Szopa, A.J.; Lembert, D.T. A descriptive analysis of abnormal postural patterns in children with hemiplegic cerebral palsy. Med. Sci. Monit. 2011, 17, CR110–CR116. [Google Scholar] [CrossRef] [PubMed]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Krzak, J.J.; Corcos, D.M.; Damiano, D.L.; Graf, A.; Hedeker, D.; Smith, P.A.; Harris, G.F. Kinematic foot types in youth with equinovarus secondary to hemiplegia. Gait Posture 2015, 41, 402–408. [Google Scholar] [CrossRef]
- Wren, T.A.; Gorton, G.E., III; Ounpuu, S.; Tucker, C.A. Efficacy of clinical gait analysis: A systematic review. Gait Posture 2011, 34, 149–153. [Google Scholar] [CrossRef]
- Kawamura, C.M.; de Morais Filho, M.C.; Barreto, M.M.; de Paula Asa, S.K.; Juliano, Y.; Novo, N.F. Comparison between visual and three-dimensional gait analysis in patients with spastic diplegic cerebral palsy. Gait Posture 2007, 25, 18–24. [Google Scholar] [CrossRef]
- Van Gestel, L.; De Laet, T.; Di Lello, E.; Bruyninckx, H.; Molenaers, G.; Van Campenhout, A.; Aertbelien, E.; Schwartz, M.; Wambacq, H.; De Cock, P.; et al. Probabilistic gait classification in children with cerebral palsy: A Bayesian approach. Res. Dev. Disabil. 2011, 32, 2542–2552. [Google Scholar] [CrossRef]
- Rathinam, C.; Bateman, A.; Peirson, J.; Skinner, J. Observational gait assessment tools in paediatrics—A systematic review. Gait Posture 2014, 40, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Armand, S.; Decoulon, G.; Bonnefoy-Mazure, A. Gait analysis in children with cerebral palsy. EFORT Open Rev. 2016, 1, 448–460. [Google Scholar] [CrossRef] [PubMed]
- De Laet, T.; Papageorgiou, E.; Nieuwenhuys, A.; Desloovere, K. Does expert knowledge improve automatic probabilistic classification of gait joint motion patterns in children with cerebral palsy? PLoS ONE 2017, 12, e0178378. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuys, A.; Ounpuu, S.; Van Campenhout, A.; Theologis, T.; De Cat, J.; Stout, J.; Molenaers, G.; De Laet, T.; Desloovere, K. Identification of joint patterns during gait in children with cerebral palsy: A Delphi consensus study. Dev. Med. Child Neurol. 2016, 58, 306–313. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Classification System | n | GMFCS I | GMFCS II | WGH I | WGH II | WGH III | WGH IV | WGH Unclass | Mean Age (years) | Sex Distribution f/m |
|---|---|---|---|---|---|---|---|---|---|---|
| GMFCS | ||||||||||
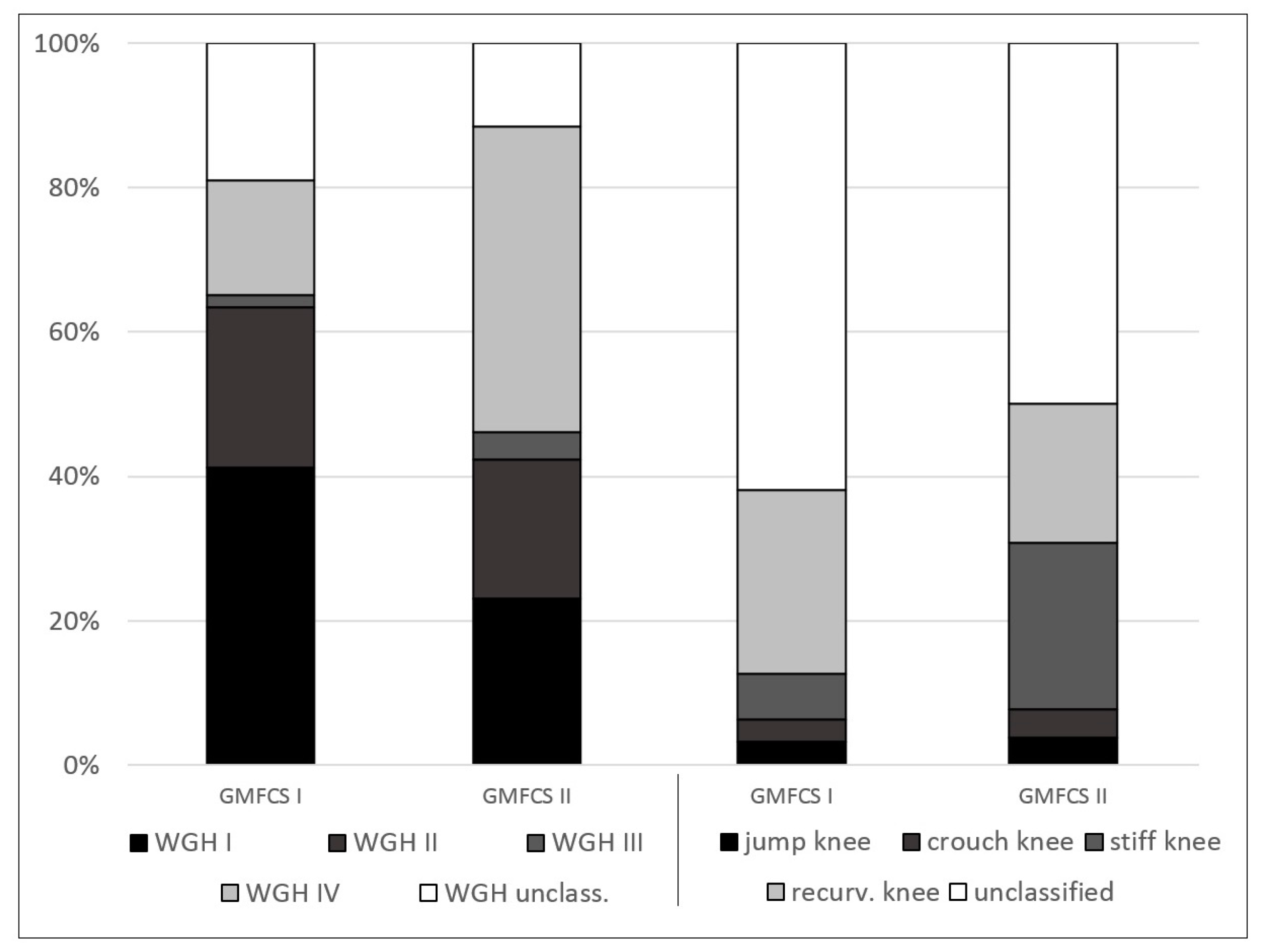
| I | 63 | - | - | / | / | / | / | / | 13.9 ± 7.3 | 29:34 |
| II | 26 | - | - | / | / | / | / | / | 18.9 ± 12.9 | 11:15 |
| WGH | ||||||||||
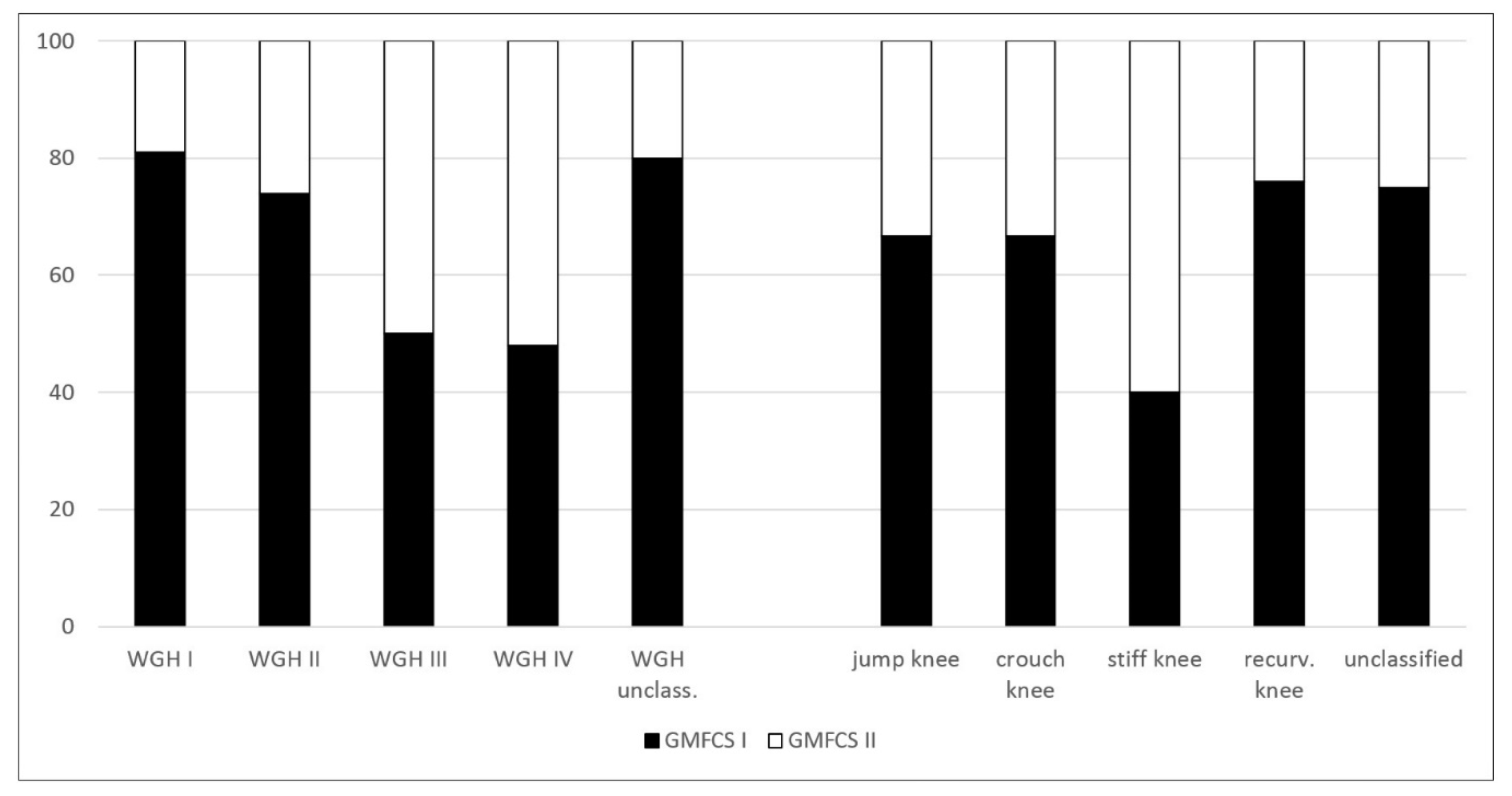
| I | 32 | 26 | 6 | - | - | - | - | - | 16.1 ± 9.6 | 17:15 |
| II | 19 | 14 | 5 | - | - | - | - | - | 11.4 ± 6.3 | 10:9 |
| III | 2 | 1 | 1 | - | - | - | - | - | 12.0 ± 0.0 | 1:1 |
| IV | 21 | 10 | 11 | - | - | - | - | - | 17.6 ± 12.3 | 7:14 |
| unclassified | 15 | 12 | 3 | - | - | - | - | - | 16.1 ± 7.6 | 5:10 |
| Sutherland | ||||||||||
| jump knee | 3 | 2 | 1 | 1 | 0 | 0 | 1 | 1 | 10.7 ± 4.6 | 2:1 |
| crouch knee | 3 | 2 | 1 | 0 | 0 | 0 | 3 | 0 | 8.0 ± 5.3 | 1:2 |
| stiff knee | 10 | 4 | 6 | 2 | 1 | 1 | 4 | 2 | 17.8 ± 14.4 | 2:8 |
| recurv. knee | 21 | 16 | 5 | 4 | 12 | 0 | 2 | 3 | 16.5 ± 8.5 | 11:10 |
| unclassified | 52 | 39 | 13 | 25 | 6 | 1 | 11 | 9 | 15.1 ± 9.3 | 24:28 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsitlakidis, S.; Horsch, A.; Schaefer, F.; Westhauser, F.; Goetze, M.; Hagmann, S.; Klotz, M.C.M. Gait Classification in Unilateral Cerebral Palsy. J. Clin. Med. 2019, 8, 1652. https://doi.org/10.3390/jcm8101652
Tsitlakidis S, Horsch A, Schaefer F, Westhauser F, Goetze M, Hagmann S, Klotz MCM. Gait Classification in Unilateral Cerebral Palsy. Journal of Clinical Medicine. 2019; 8(10):1652. https://doi.org/10.3390/jcm8101652
Chicago/Turabian StyleTsitlakidis, Stefanos, Axel Horsch, Felix Schaefer, Fabian Westhauser, Marco Goetze, Sebastien Hagmann, and Matthias C. M. Klotz. 2019. "Gait Classification in Unilateral Cerebral Palsy" Journal of Clinical Medicine 8, no. 10: 1652. https://doi.org/10.3390/jcm8101652
APA StyleTsitlakidis, S., Horsch, A., Schaefer, F., Westhauser, F., Goetze, M., Hagmann, S., & Klotz, M. C. M. (2019). Gait Classification in Unilateral Cerebral Palsy. Journal of Clinical Medicine, 8(10), 1652. https://doi.org/10.3390/jcm8101652