Association between Bladder Outlet Obstruction and Bladder Cancer in Patients with Aging Male

 , ,
, , 

Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Patient Identification and Definition of Exposure
2.3. Covariates
2.4. Outcome Detection
2.5. Statistics
3. Results
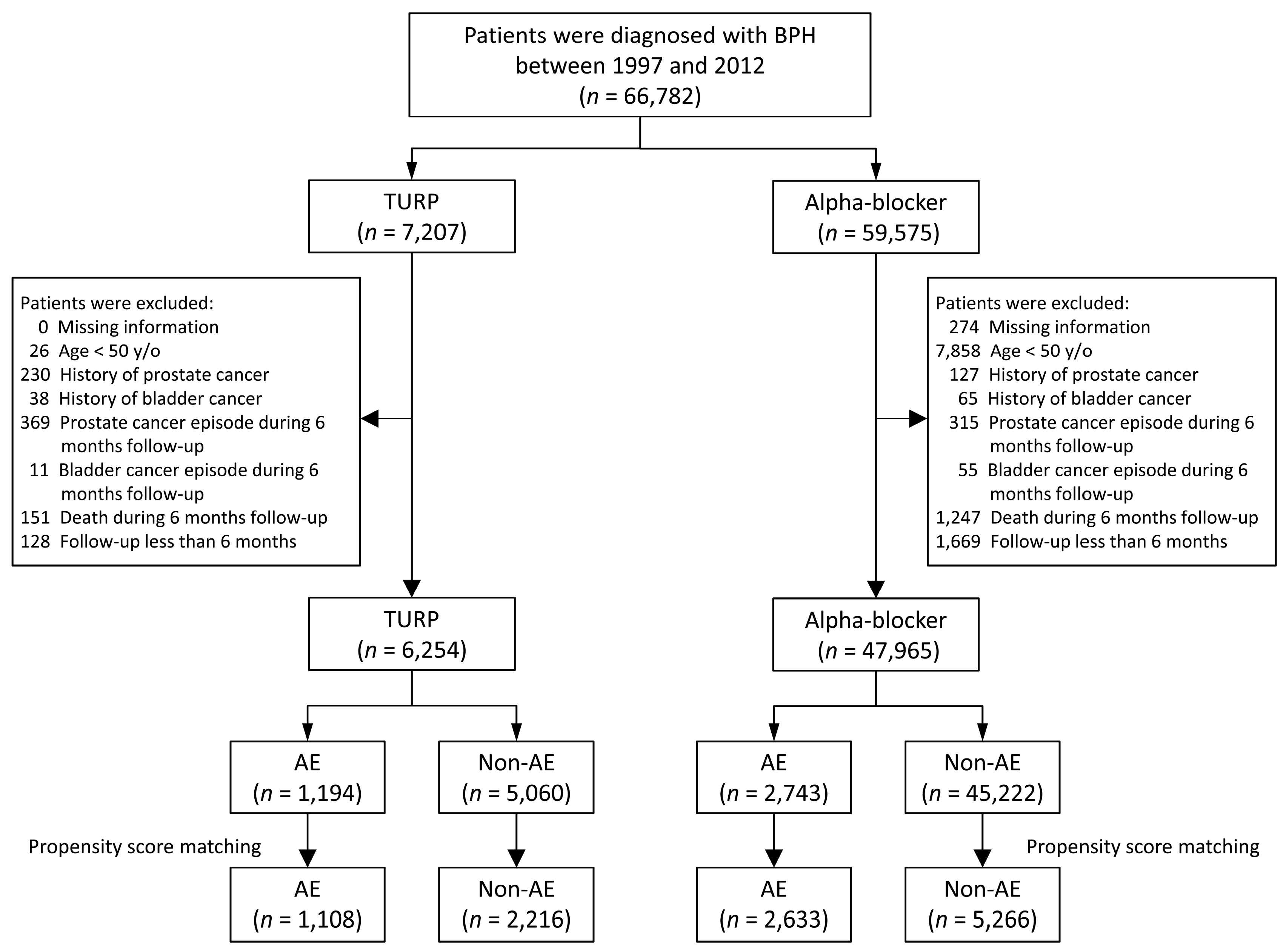
3.1. Study Population
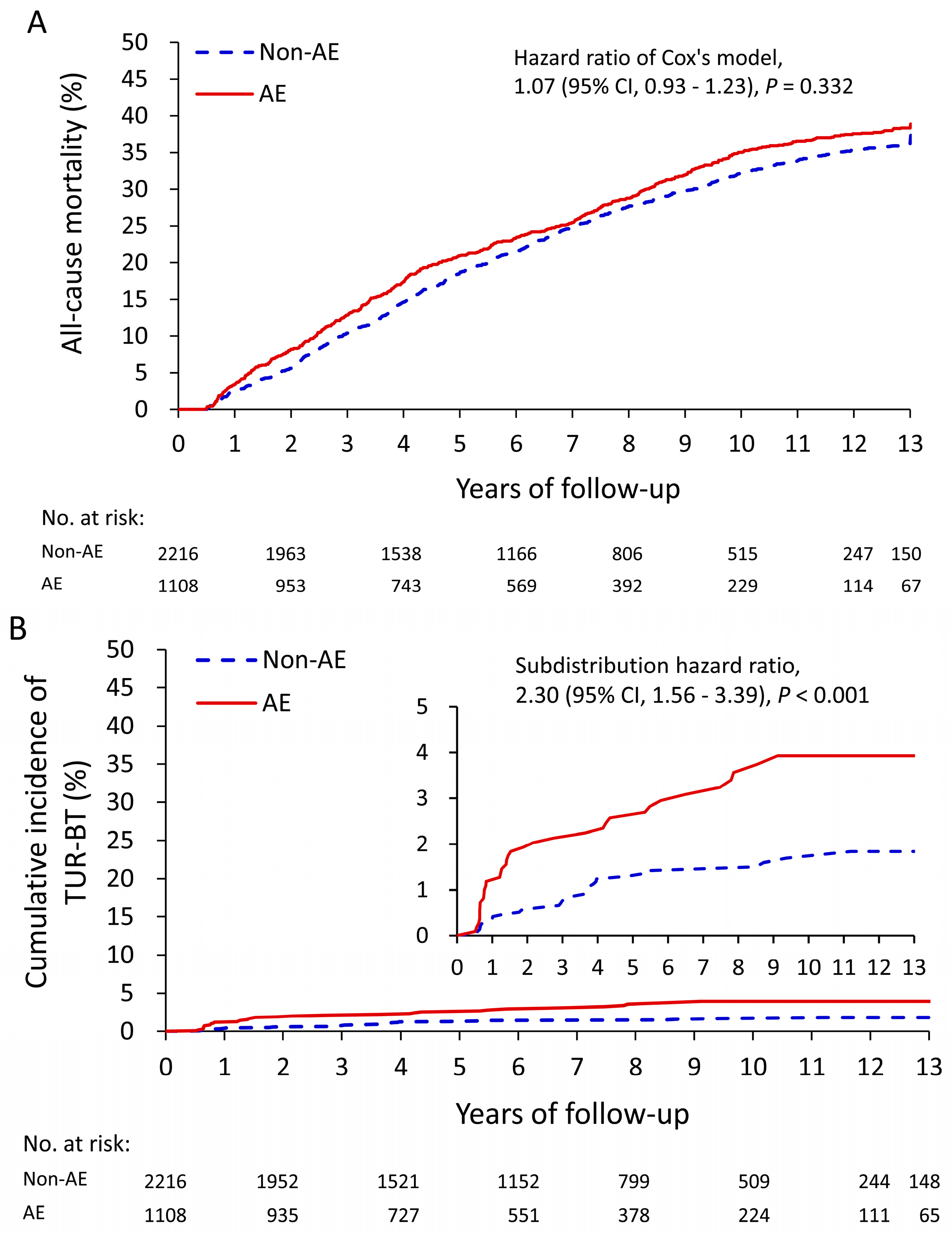
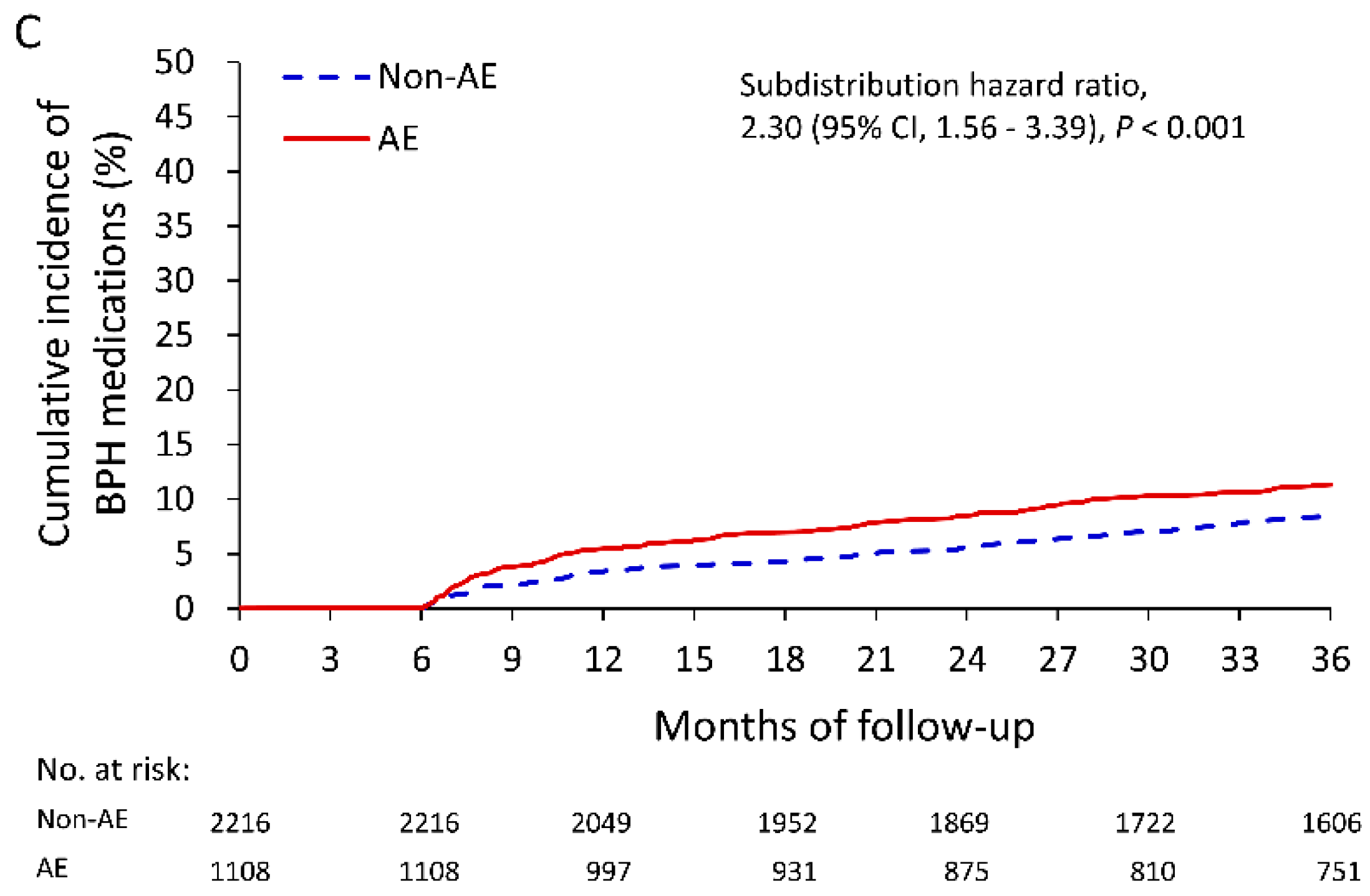
3.2. Association between AEs and Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Verhamme, K.M.C.; Dieleman, J.P.; Bleumink, G.S.; van der Lei, J.; Sturkenboom, M.C.J.M.; Triumph Pan European Expert Panel. Incidence and prevalence of lower urinary tract symptoms suggestive of benign prostatic hyperplasia in primary care—the Triumph project. Eur. Urol. 2002, 42, 323–328. [Google Scholar] [CrossRef]
- Berry, S.J.; Coffey, D.S.; Walsh, P.C.; Ewing, L.L. The development of human benign prostatic hyperplasia with age. J. Urol. 1984, 132, 474–479. [Google Scholar] [CrossRef]
- Irwin, D.E.; Kopp, Z.S.; Agatep, B.; Milsom, I.; Abrams, P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011, 108, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, S.J.; Jacobson, D.J.; Girman, C.J.; Ewing, L.L. Natural history of prostatism: Risk factors for acute urinary retention. J. Urol. 1997, 158, 481–487. [Google Scholar] [CrossRef]
- Perchon, L.F.; Pintarelli, V.L.; Bezerra, E.; Thiel, M.; Dambros, M. Quality of life in elderly men with aging symptoms and lower urinary tract symptoms (LUTS). Neurourol. Urodyn. 2011, 30, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Oesterling, J.E. Benign prostatic hyperplasia: A review of its histogenesis and natural history. prostate. 1996, 29, 67–73. [Google Scholar] [CrossRef]
- Saigal, C.S.; Joyce, G. Economic costs of benign prostatic hyperplasia in the private sector. J. Urol. 2005, 173, 1309–1313. [Google Scholar] [CrossRef]
- Nickel, J.C.; Méndez-Probst, C.E.; Whelan, T.F.; Paterson, R.F.; Razvi, H. 2010 Update: Guidelines for the management of benign prostatic hyperplasia. Can. Urol. Assoc. J. 2010, 4, 310. [Google Scholar] [CrossRef] [PubMed]
- Fusco, F.; Palmieri, A.; Ficarra, V.; Giannarini, G.; Novara, G.; Longo, N.; Verze, P.; Creta, M.; Mirone, V. α1-blockers improve benign prostatic obstruction in men with lower urinary tract symptoms: A systematic review and meta-analysis of urodynamic studies. Eur. Urol. 2016, 69, 1091–1101. [Google Scholar] [CrossRef]
- Mayer, E.K.; Kroeze, S.G.; Chopra, S.; Bottle, A.; Patel, A. Examining the ‘gold standard’: A comparative critical analysis of three consecutive decades of monopolar transurethral resection of the prostate (TURP) outcomes. BJU Int. 2012, 110, 1595–1601. [Google Scholar] [CrossRef]
- Lin, Y.H.; Hou, C.P.; Chen, T.H.; Juang, H.H.; Chang, P.L.; Yang, P.S.; Tsui, K.H. Transurethral resection of the prostate provides more favorable clinical outcomes compared with conservative medical treatment in patients with urinary retention caused by benign prostatic obstruction. BMC Geriatr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hou, C.P.; Lin, Y.H.; Chen, T.H.; Chang, P.L.; Juang, H.H.; Chen, C.L.; Tsui, K.H. Transurethral resection of the prostate achieves favorable outcomes in stroke patients with symptomatic benign prostate hyperplasia. Aging Male 2018, 21, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Hou, C.P.; Chen, T.H.; Juang, H.H.; Chang, P.L.; Yang, P.S.; Tsui, K.H. Is diabetes mellitus associated with clinical outcomes in aging males treated with transurethral resection of prostate for bladder outlet obstruction: Implications from Taiwan Nationwide population-based cohort study. Clin. Interv. Aging 2017. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, F.Y.; Yang, C.L.; Huang, Y.T.; Huang, W.F. Using Taiwan’s National Health Insurance Research Databases for Pharmacoepidemiology Research. J. Food. Drug Anal. 2007, 15, 99–108. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; McKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chron. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Wu, C.S.; Lai, M.S.; Gau, S.S.; Wang, S.C.; Tsai, H.J. Concordance between patient self-reports and claims data on clinical diagnoses, medication use, and health system utilization in Taiwan. PLoS ONE 2014. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-Y.; Chen, Y.-J.; Ho, H.-J.; Hsu, Y.-C.; Kuo, K.N.; Wu, M.-S.; Lin, J.-T. Association between nucleoside analogues and risk of hepatitis B virus–related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1913. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.Y.; See, L.C.; Liu, J.R.; Chuang, C.K.; Pang, S.T.; Hsieh, I.C.; Wen, M.S.; Chen, T.H.; Lin, Y.C.; Liaw, C.C.; et al. Risk of Cardiovascular Ischemic Events After Surgical Castration and Gonadotropin-Releasing Hormone Agonist Therapy for Prostate Cancer: A Nationwide Cohort Study. J. Clin. Oncol. 2017, 35, 3697–3705. [Google Scholar] [CrossRef]
- Austin, P.C.; Fine, J.P. Propensity-score matching with competing risks in survival analysis. Stat. Med. 2019, 38, 751–777. [Google Scholar] [CrossRef]
- Davidian, M.H. Guidelines for the treatment of benign prostatic hyperplasia. US Pharm. 2016, 41, 36–40. [Google Scholar]
- Rassweiler, J.; Teber, D.; Kuntz, R.; Hofmann, R. Complications of transurethral resection of the prostate (TURP)—incidence, management, and prevention. Eur. Urol 2006, 50, 969–980. [Google Scholar] [CrossRef] [PubMed]
- Lepor, H. Alpha blockers for the treatment of benign prostatic hyperplasia. Rev. Urol. 2007, 9, 181–190. [Google Scholar] [CrossRef]
- Caliendo, M.; Kopeinig, S. Some practical guidance for the implementation of propensity score matching. J. Econ. Surv. 2008, 22, 31–72. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GLOBOCAN 2012 v1.0, cancer incidence and mortality worldwide. 2013, IARC CancerBase No. 11. Lyon, France: International Agency for Research on Cancer. Available online: http://globocan.iarc.fr. (accessed on 12 December 2013).
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 9859, 2095–2128. [Google Scholar] [CrossRef]
- Chiang, C.J.; Lo, W.C.; Yang, Y.W.; You, S.L.; Chen, C.J.; Lai, M.S. Incidence and survival of adult cancer patients in Taiwan, 2002–2012. J. Formos. Med. Assoc. 2016, 115, 1076–1088. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Furberg, H.; Zabor, E.C.; Xylinas, E.; Babjuk, M.; Pycha, A.; Montorsi, F. Impact of smoking and smoking cessation on oncologic outcomes in primary non–muscle-invasive bladder cancer. Eur. Urol. 2013, 63, 724–732. [Google Scholar] [CrossRef]
- Vincis, P.; Esteve, J.; Hartge, P.; Hoover, R.; Silverman, D.T.; Terracini, B. Effects of timing and type of tobacco in cigarette-induced bladder cancer. Cancer Res. 1998, 48, 3849–3852. [Google Scholar]
- Chu, H.; Wang, M.; Zhang, Z. Bladder cancer epidemiology and genetic susceptibility. J. Biomed. Res. 2013, 27, 170. [Google Scholar]
- Fang, C.W.; Liao, C.H.; Wu, S.C.; Muo, C.H. Association of benign prostatic hyperplasia and subsequent risk of bladder cancer: An Asian population cohort study. World J. Urol. 2018, 36, 931–938. [Google Scholar] [CrossRef]
- Burger, M.; Catto, J.W.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Lotan, Y. Epidemiology and risk factors of urothelial bladder cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef]
- Nesi, G.; Nobili, S.; Cai, T.; Caini, S.; Santi, R. Chronic inflammation in urothelial bladder cancer. Virchows Archiv 2015, 467, 623–633. [Google Scholar] [CrossRef]
- Platz, E.A.; Kulac, I.; Barber, J.R.; Drake, C.G.; Joshu, C.E.; Nelson, W.G.; Thompson, I.M. A prospective study of chronic inflammation in benign prostate tissue and risk of prostate cancer: Linked PCPT and SELECT cohorts. Cancer Epidemiol. Prev. Biomark. 2017, 26, 1549–1557. [Google Scholar] [CrossRef]
- Dai, X.; Fang, X.; Ma, Y.; Xianyu, J. Benign prostatic hyperplasia and the risk of prostate cancer and bladder cancer: A meta-analysis of observational studies. Medicine 2016. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, E.; White, J.R.; Yu, S.H.; Kulac, I.; Ertunc, O.; De Marzo, A.M.; Sfanos, K.S. Profiling the urinary microbiome in men with positive versus negative biopsies for prostate cancer. J. Urol. 2018, 199, 161–171. [Google Scholar] [CrossRef]
- Han, H.H.; Ko, W.J.; Yoo, T.K.; Oh, T.H.; Kim, D.Y.; Kwon, D.D.; Jung, T.Y. Factors associated with continuing medical therapy after transurethral resection of prostate. Urology 2014, 84, 675–680. [Google Scholar] [CrossRef]
- Lee, W.C.; Lin, Y.H.; Hou, C.P.; Chang, P.L.; Tsui, K.H. Prostatectomy using different lasers for the treatment of benign prostate hyperplasia in aging males. Clin. Interv. Aging 2013, 8, 1483–1488. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Code |
|---|---|
| Benign prostatic hyperplasia | 600.xx, A360 |
| Prostate cancer | 185.xx (Catastrophic illness certificate) |
| Bladder cancer | 188.9x (Catastrophic illness certificate) |
| Diabetes mellitus | 250.xx |
| Hypertension | 401.xx–405.xx |
| Hyperlipidemia | 272.xx |
| Chronic obstructive pulmonary disease | 491.xx, 492.xx, 496.xx |
| Parkinsonism | 332.xx |
| Chronic kidney disease | 580.xx–589.xx, 403.xx–404.xx, 016.0x, 095.4x, 236.9x, 250.4x, 274.1x, 442.1x, 447.3x, 440.1x, 572.4x, 642.1x, 646.2x, 753.1x, 283.11, 403.01, 404.02, 446.21 |
| Ischemic heart disease | 410.xx–414.xx |
| Stroke | 430.xx–434.xx |
| Heart failure | 428.xx |
| Alcoholism | V113, 291.xx, 305.0x, 357.5, 425.5, 303.xx, 571.0, 571.1, 571.2, 571.3, 980.0 |
| Drug abuse | 303.xx–305.xx |
| Urinary tract infection | 599.0x, 595.0x |
| Hemorrhoids | 455.xx |
| Acute myocardial infarction | 410.xx |
| Hip fracture | 820.xx |
| Spine fracture | 805.xx, 806.xx |
| Variable | Before Matching | After Matching | ||||
|---|---|---|---|---|---|---|
| AE (n = 1194) | Non-AE (n = 5060) | STD | AE (n = 1108) | Non-AE (n = 2216) | STD | |
| Age (years) | 72.9 ± 8.0 | 71.6 ± 8.0 | 0.160 | 72.7 ± 8.0 | 72.5 ± 7.8 | 0.021 |
| Comorbidity | ||||||
| Diabetes mellitus | 227 (19.0) | 867 (17.1) | 0.049 | 203 (18.3) | 413 (18.6) | −0.008 |
| Hypertension | 596 (49.9) | 2106 (41.6) | 0.167 | 534 (48.2) | 1075 (48.5) | −0.006 |
| Hyperlipidemia | 142 (11.9) | 450 (8.9) | 0.098 | 124 (11.2) | 244 (11.0) | 0.006 |
| Chronic obstructive pulmonary disease | 229 (19.2) | 657 (13.0) | 0.169 | 191 (17.2) | 361 (16.3) | 0.025 |
| Parkinsonism | 34 (2.8) | 93 (1.8) | 0.067 | 24 (2.2) | 51 (2.3) | −0.009 |
| Chronic kidney disease | 124 (10.4) | 483 (9.5) | 0.028 | 117 (10.6) | 221 (10.0) | 0.019 |
| Ischemic heart disease | 236 (19.8) | 791 (15.6) | 0.108 | 196 (17.7) | 405 (18.3) | −0.015 |
| Stroke | 165 (13.8) | 408 (8.1) | 0.185 | 123 (11.1) | 252 (11.4) | −0.009 |
| Heart failure | 54 (4.5) | 166 (3.3) | 0.064 | 41 (3.7) | 92 (4.2) | −0.023 |
| Alcoholism | 6 (0.5) | 10 (0.2) | 0.052 | 1 (0.09) | 5 (0.23) | −0.034 |
| Drug abuse | 3 (0.3) | 13 (0.3) | −0.001 | 1 (0.09) | 4 (0.18) | −0.025 |
| CCI score | 1.5 ± 1.7 | 1.2 ± 1.5 | 0.218 | 1.4 ± 1.6 | 1.4 ± 1.7 | 0.002 |
| Tissue ablation | ||||||
| 5–15 g | 850 (71.2) | 3771 (74.5) | −0.075 | 791 (71.4) | 1576 (71.1) | 0.006 |
| 15–50 g | 288 (24.1) | 1086 (21.5) | 0.063 | 269 (24.3) | 538 (24.3) | 0.000 |
| >50 g | 56 (4.7) | 203 (4.0) | 0.033 | 48 (4.3) | 102 (4.6) | −0.013 |
| Urologic event in the previous three years | ||||||
| Urinary tract infection | 484 (40.5) | 1192 (23.6) | 0.370 | 401 (36.2) | 790 (35.6) | 0.011 |
| Urinary retention | 495 (41.5) | 1783 (35.2) | 0.128 | 445 (40.2) | 898 (40.5) | −0.007 |
| Bladder stone | 39 (3.3) | 137 (2.7) | 0.033 | 34 (3.1) | 67 (3.0) | 0.003 |
| Urologic drug use in the previous three months | ||||||
| Anti-muscarinic | 114 (9.5) | 488 (9.6) | −0.003 | 108 (9.7) | 221 (10.0) | −0.008 |
| Alpha-blockers | 920 (77.1) | 3817 (75.4) | 0.038 | 851 (76.8) | 1706 (77.0) | −0.004 |
| Propensity score | 0.235 ± 0.105 | 0.181 ± 0.085 | 0.569 | 0.216 ± 0.082 | 0.215 ± 0.081 | 0.008 |
| Follow-up years | 6.3 ± 3.8 | 7.3 ± 4.3 | −0.225 | 6.5 ± 3.9 | 6.7 ± 3.9 | −0.050 |
| Variable | AE (n = 1108) | Non-AE (n = 2216) | AE vs. Non-AE | |
|---|---|---|---|---|
| HR/SHR (95% CI) | P | |||
| Primary Outcome at the End of Follow Up | ||||
| All-cause mortality | 431 (38.9) | 827 (37.3) | 1.07 (0.93, 1.23) | 0.332 |
| Prostate cancer | 31 (2.8) | 56 (2.5) | 1.20 (0.83, 1.74) | 0.337 |
| TUR-BT | 36 (3.2) | 32 (1.4) | 2.30 (1.56, 3.39) | <0.001 |
| Radical cystectomy | 5 (0.5) | 1 (0.0) | NA | NA |
| Secondary outcome during three-year follow-up | ||||
| Medication dependence | ||||
| Anti-muscarinic | 30 (2.7) | 26 (1.2) | 2.27 (1.48, 3.46) | <0.001 |
| Alpha-blocker | 112 (10.1) | 172 (7.8) | 1.31 (1.08, 1.59) | 0.006 |
| Inguinal hernia | 40 (3.6) | 59 (2.7) | 1.35 (0.98, 1.87) | 0.066 |
| Hemorrhoids | 132 (11.9) | 195 (8.8) | 1.39 (1.16, 1.66) | <0.001 |
| Stroke | 56 (5.1) | 118 (5.3) | 0.97 (0.74, 1.25) | 0.788 |
| AMI | 8 (0.7) | 19 (0.9) | 0.80 (0.40, 1.57) | 0.511 |
| Hip fracture | 21 (1.9) | 20 (0.9) | 2.26 (1.37, 3.71) | 0.001 |
| Variable | AE (n = 2633) | Non-AE (n = 5266) | AE vs. Non-AE | |
|---|---|---|---|---|
| HR/SHR (95% CI) | p | |||
| Primary Outcome at the End of Follow Up | ||||
| All-cause mortality | 1272 (48.3) | 2060 (39.1) | 1.63 (1.49, 1.78) | <0.001 |
| Prostate cancer | 44 (1.7) | 89 (1.7) | 1.16 (0.84, 1.61) | 0.354 |
| TUR-BT | 66 (2.5) | 49 (0.9) | 2.72 (1.99, 3.71) | <0.001 |
| Radical cystectomy | 15 (0.6) | 3 (0.1) | 7.68 (2.54, 23.28) | <0.001 |
| Secondary outcome during three-year follow-up | ||||
| Inguinal hernia | 55 (2.1) | 96 (1.8) | 1.12 (0.85, 1.47) | 0.418 |
| Hemorrhoids | 202 (7.7) | 403 (7.7) | 1.04 (0.90, 1.19) | 0.629 |
| Stroke | 143 (5.4) | 262 (5.0) | 1.06 (0.90, 1.26) | 0.475 |
| AMI | 30 (1.1) | 45 (0.9) | 1.33 (0.91, 1.92) | 0.137 |
| Hip fracture | 36 (1.4) | 82 (1.6) | 0.93 (0.67, 1.29) | 0.651 |
| Predictor | HR | 95% CI | p Value |
|---|---|---|---|
| Age ≥ 75 years | 1.29 | 1.07–1.56 | 0.008 |
| BPH duration (years) | 1.13 | 1.10–1.16 | <0.001 |
| Adverse event during the six-month follow up | 1.45 | 1.18–1.79 | <0.001 |
| Hypertension | 1.82 | 1.49–2.22 | <0.001 |
| Hyperlipidemia | 1.51 | 1.17–1.94 | 0.002 |
| Urinary tract infection in the previous three years | 1.23 | 1.01–1.49 | 0.039 |
| NSAIDs use in the previous year | 1.35 | 1.11–1.63 | 0.002 |
| Alpha-blocker use in the previous three months | 1.61 | 1.21–2.14 | 0.001 |
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Variable | AE (n = 2743) | Non-AE (n = 45,222) | STD | AE (n = 2633) | Non-AE (n = 5266) | STD |
| Age (years) | 70.1 ± 10.3 | 66.7 ± 9.9 | 0.335 | 69.8 ± 10.3 | 70.1 ± 10.8 | −0.023 |
| Comorbidity | ||||||
| Diabetes mellitus | 641 (23.4) | 7414 (16.4) | 0.175 | 589 (22.4) | 1193 (22.7) | −0.007 |
| Hypertension | 1264 (46.1) | 17292 (38.2) | 0.159 | 1192 (45.3) | 2424 (46.0) | −0.015 |
| Hyperlipidemia | 309 (11.3) | 5598 (12.4) | −0.035 | 300 (11.4) | 604 (11.5) | −0.002 |
| Chronic obstructive pulmonary disease | 466 (17.0) | 4752 (10.5) | 0.189 | 412 (15.6) | 853 (16.2) | −0.015 |
| Parkinsonism | 85 (3.1) | 539 (1.2) | 0.132 | 75 (2.8) | 155 (2.9) | −0.006 |
| Chronic kidney disease | 324 (11.8) | 3010 (6.7) | 0.179 | 296 (11.2) | 603 (11.5) | −0.007 |
| Ischemic heart disease | 484 (17.6) | 5985 (13.2) | 0.122 | 450 (17.1) | 936 (17.8) | −0.018 |
| Stroke | 533 (19.4) | 3580 (7.9) | 0.340 | 460 (17.5) | 934 (17.7) | −0.007 |
| Heart failure | 173 (6.3) | 1067 (2.4) | 0.195 | 143 (5.4) | 312 (5.9) | −0.021 |
| Alcoholism | 33 (1.2) | 347 (0.8) | 0.044 | 32 (1.22) | 74 (1.41) | −0.017 |
| Drug abuse | 19 (0.7) | 238 (0.5) | 0.021 | 19 (0.72) | 40 (0.76) | −0.004 |
| CCI score | 1.6 ± 1.9 | 1.0 ± 1.5 | 0.385 | 1.5 ± 1.8 | 1.6 ± 1.9 | −0.021 |
| Urology event in the previous three years | ||||||
| Urinary tract infection | 893 (32.6) | 4408 (9.7) | 0.582 | 783 (29.7) | 1541 (29.3) | 0.010 |
| Urinary retention | 529 (19.3) | 1693 (3.7) | 0.502 | 419 (15.9) | 780 (14.8) | 0.031 |
| Bladder stone | 39 (1.4) | 223 (0.5) | 0.095 | 32 (1.2) | 52 (1.0) | 0.022 |
| Urologic drug use in the previous three months | ||||||
| Anti-muscarinic | 79 (2.9) | 675 (1.5) | 0.095 | 74 (2.8) | 162 (3.1) | −0.016 |
| Alpha-blockers | — | — | — | — | — | — |
| Propensity score | 0.121 ± 0.126 | 0.053 ± 0.053 | 0.705 | 0.105 ± 0.096 | 0.104 ± 0.095 | 0.003 |
| Follow-up years | 5.1 ± 3.8 | 6.7 ± 4.3 | −0.404 | 5.1 ± 3.8 | 5.9 ± 3.9 | −0.200 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-H.; Hou, C.-P.; Juang, H.-H.; Chang, P.-L.; Chen, T.-H.; Chen, C.-L.; Tsui, K.-H. Association between Bladder Outlet Obstruction and Bladder Cancer in Patients with Aging Male. J. Clin. Med. 2019, 8, 1550. https://doi.org/10.3390/jcm8101550
Lin Y-H, Hou C-P, Juang H-H, Chang P-L, Chen T-H, Chen C-L, Tsui K-H. Association between Bladder Outlet Obstruction and Bladder Cancer in Patients with Aging Male. Journal of Clinical Medicine. 2019; 8(10):1550. https://doi.org/10.3390/jcm8101550
Chicago/Turabian StyleLin, Yu-Hsiang, Chen-Pang Hou, Horng-Heng Juang, Phei-Lang Chang, Tien-Hsing Chen, Chien-Lun Chen, and Ke-Hung Tsui. 2019. "Association between Bladder Outlet Obstruction and Bladder Cancer in Patients with Aging Male" Journal of Clinical Medicine 8, no. 10: 1550. https://doi.org/10.3390/jcm8101550
APA StyleLin, Y.-H., Hou, C.-P., Juang, H.-H., Chang, P.-L., Chen, T.-H., Chen, C.-L., & Tsui, K.-H. (2019). Association between Bladder Outlet Obstruction and Bladder Cancer in Patients with Aging Male. Journal of Clinical Medicine, 8(10), 1550. https://doi.org/10.3390/jcm8101550