Effects of Progressive Resistance Training on Post-Surgery Incontinence in Men with Prostate Cancer

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
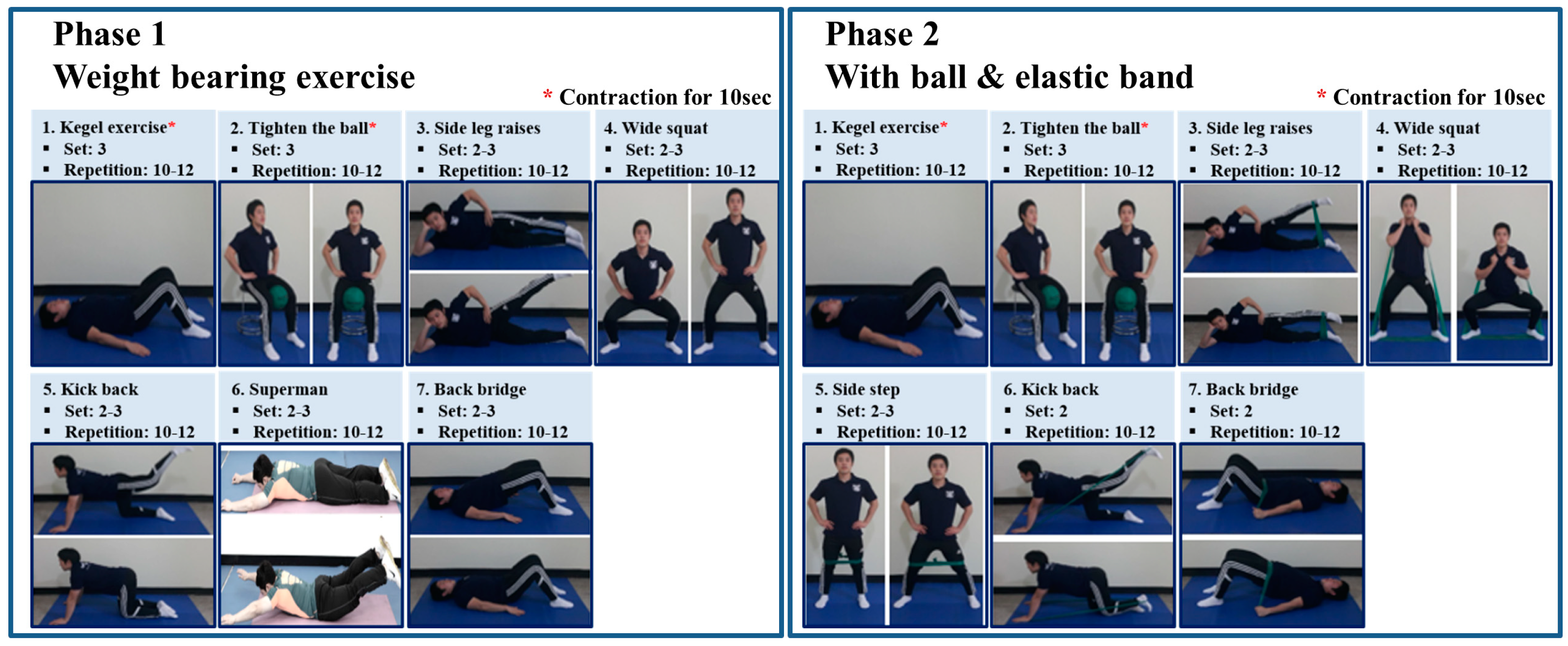
2.1. Pelvic Floor Muscle Exercise Program
2.2. Lower Muscle Strength and Endurance
2.3. Outcome Assessment
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Authors Contribution
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Oh, C.M.; Cho, H.; Lee, D.H.; Lee, K.H. Cancer statistics in korea: Incidence, mortality, survival, and prevalence in 2012. Cancer Res. Treat. 2015, 47, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Heo, J.E.; Ahn, H.K.; Kim, J.; Chung, B.H.; Lee, K.S. Changes in clinical characteristics of patients with an initial diagnosis of prostate cancer in korea: 10-year trends reported by a tertiary center. J. Korean Med. Sci. 2018, 33. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Choi, D.; Lim, J.H.; Yoon, J.H.; Jeong, I.G.; You, D.; Hong, J.H.; Ahn, H.; Kim, C.S. Changes in prostate cancer aggressiveness over a 12-year period in korea. Korean J. Urol. 2012, 53, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Trabulsi, E.J.; Gomella, L.G. Is there an optimal management for localized prostate cancer? Clin. Interv. Aging 2010, 5, 187–197. [Google Scholar] [PubMed]
- Ilic, D.; Evans, S.M.; Allan, C.A.; Jung, J.H.; Murphy, D.; Frydenberg, M. Laparoscopic and robot-assisted vs open radical prostatectomy for the treatment of localized prostate cancer: A cochrane systematic review. BJU Int. 2017, 6, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Borregales, L.D.; Berg, W.T.; Tal, O.; Wambi, C.; Kaufman, S.; Gaya, J.M.; Urzua, C.; Badani, K.K. ‘Trifecta’ after radical prostatectomy: Is there a standard definition? BJU Int. 2013, 112, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.; Fiori, C.; Amparore, D.; Checcucci, E.; Porpiglia, F. Technical details to achieve perfect early continence after radical prostatectomy. Minerva Chir. 2018. [Google Scholar] [CrossRef]
- Kretschmer, A.; Hubner, W.; Sandhu, J.S.; Bauer, R.M. Evaluation and management of postprostatectomy incontinence: A systematic review of current literature. Eur. Urol. Focus 2016, 2, 245–259. [Google Scholar] [CrossRef] [PubMed]
- Radadia, K.D.; Farber, N.J.; Shinder, B.; Polotti, C.F.; Milas, L.J.; Tunuguntla, H. Management of postradical prostatectomy urinary incontinence: A review. Urology 2017, 113, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Newman, D.K.; Guzzo, T.; Lee, D.; Jayadevappa, R. An evidence-based strategy for the conservative management of the male patient with incontinence. Curr. Opin. Urol. 2014, 24, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Trofimenko, V.; Myers, J.B.; Brant, W.O. Post-prostatectomy incontinence: How common and bothersome is it really? Sex. Med. Rev. 2017, 5, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Baker, H.; Wellman, S.; Lavender, V. Functional quality-of-life outcomes reported by men treated for localized prostate cancer: A systematic literature review. Oncol. Nurs. Forum 2016, 43, 199–218. [Google Scholar] [CrossRef] [PubMed]
- Bridgeman, B.; Roberts, S.G. The 4-3-2 method for kegel exercises. Am. J. Men’s Health 2010, 4, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Centemero, A.; Rigatti, L.; Giraudo, D.; Lazzeri, M.; Lughezzani, G.; Zugna, D.; Montorsi, F.; Rigatti, P.; Guazzoni, G. Preoperative pelvic floor muscle exercise for early continence after radical prostatectomy: A randomised controlled study. Eur. Urol. 2010, 57, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Parekh, A.R.; Feng, M.I.; Kirages, D.; Bremner, H.; Kaswick, J.; Aboseif, S. The role of pelvic floor exercises on post-prostatectomy incontinence. J. Urol. 2003, 170, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Tienforti, D.; Sacco, E.; Marangi, F.; D’Addessi, A.; Racioppi, M.; Gulino, G.; Pinto, F.; Totaro, A.; D’Agostino, D.; Bassi, P. Efficacy of an assisted low-intensity programme of perioperative pelvic floor muscle training in improving the recovery of continence after radical prostatectomy: A randomized controlled trial. BJU Int. 2012, 110, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Di Benedetto, P.; Coidessa, A.; Floris, S. Rationale of pelvic floor muscles training in women with urinary incontinence. Miner. Ginecol. 2008, 60, 529–541. [Google Scholar]
- Martuscello, J.M.; Nuzzo, J.L.; Ashley, C.D.; Campbell, B.I.; Orriola, J.J.; Mayer, J.M. Systematic review of core muscle activity during physical fitness exercises. J. Strength Cond. Res. 2013, 27, 1684–1698. [Google Scholar] [CrossRef] [PubMed]
- Rosier, P.; Schaefer, W.; Lose, G.; Goldman, H.B.; Guralnick, M.; Eustice, S.; Dickinson, T.; Hashim, H. International continence society good urodynamic practices and terms 2016: Urodynamics, uroflowmetry, cystometry, and pressure-flow study. Neurourol. Urodyn. 2017, 36, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Kang, D.; Kim, H.J.; Kim, J.S.; Song, H.S.; Song, W. Effect of elastic band-based high-speed power training on cognitive function, physical performance and muscle strength in older women with mild cognitive impairment. Geriatr. Gerontol. Int. 2017, 17, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.L.; American College of Sports Medicine. Acsm’s Guide to Exercise and Cancer Survivorship; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- Krhut, J.; Zachoval, R.; Smith, P.P.; Rosier, P.F.; Valansky, L.; Martan, A.; Zvara, P. Pad weight testing in the evaluation of urinary incontinence. Neurourol. Urodyn. 2014, 33, 507–510. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.I.; Lam, V.; Patel, M.I. Preoperative pelvic floor muscle exercise and postprostatectomy incontinence: A systematic review and meta-analysis. Eur. Urol. 2016, 69, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Oh, S.A.; Kim, S.H.; Oh, S.-J. Patient satisfaction after holmium laser enucleation of the prostate (holep): A prospective cohort study. PLoS ONE 2017, 12, e0182230. [Google Scholar] [CrossRef] [PubMed]
- Reeves, F.; Preece, P.; Kapoor, J.; Everaerts, W.; Murphy, D.G.; Corcoran, N.M.; Costello, A.J. Preservation of the neurovascular bundles is associated with improved time to continence after radical prostatectomy but not long-term continence rates: Results of a systematic review and meta-analysis. Eur. Urol. 2015, 68, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Grasso, A.A.; Mistretta, F.A.; Sandri, M.; Cozzi, G.; De Lorenzis, E.; Rosso, M.; Albo, G.; Palmisano, F.; Mottrie, A.; Haese, A.; et al. Posterior musculofascial reconstruction after radical prostatectomy: An updated systematic review and a meta-analysis. BJU Int. 2016, 118, 20–34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Continent Group (n = 31) | Incontinent Group (n = 22) | p-Value | |
|---|---|---|---|
| Age (years) | 68.2 ± 6.1 | 68.3 ± 5.1 | 0.899 |
| Preoperative BMI (kg/m2) | 24.8 ± 2.8 | 26.6 ± 9.0 | 0.289 |
| Post-exercise 12-weeks BMI (kg/m2) | 24.5 ± 2.8 | 24.7 ± 3.3 | 0.827 |
| Prostate volume (mL) | 36.4 ± 19.1 | 37.8 ± 23.5 | 0.827 |
| PSA (ng/dL) | 23.6 ± 42.1 | 24.3 ± 42.8 | 0.953 |
| Op methods | 0.601 | ||
| RRP | 17 | 12 | |
| RALP | 14 | 10 | |
| Pathology Gleason Score Sum | 0.812 | ||
| 6 | 5 | 4 | |
| 7 (3 + 4) | 7 | 5 | |
| 7 (4 + 3) | 8 | 8 | |
| 8 | 7 | 4 | |
| 9 | 4 | 1 | |
| Pathologic T stage | 0.219 | ||
| T2 | 20 (64.5%) | 11 (50.0%) | |
| T3 | 11 (35.5%) | 11 (50.0%) | |
| Participation rate (%) | 42.0 ± 38.7 | 50.4 ± 36.0 | 0.428 |
| Preoperative MUCP (cmH2O) | 78.2 ± 18.8 | 64.8 ± 25.3 | 0.036 |
| Preoperative MCC (mL) | 355.3 ± 133.1 | 339.4 ± 139.2 | 0.685 |
| Preoperative PdetQmax (cm H2O) | 55.1 ± 21.0 | 48.7 ± 20.2 | 0.285 |
| Post-exercise 12-week MUCP (cm H2O) | 56.1 ± 25.3 | 53.6 ± 27.0 | 0.739 |
| Post-exercise 12-week MCC (mL) | 339.5 ± 89.7 | 297.1 ± 77.3 | 0.085 |
| Post-exercise 12-week DetQmax (cm H2O) | 38.5 ± 18.5 | 30.6 ± 15.6 | 0.123 |
| Change of MUCP (cm H2O) | 24.4 ± 29.4 | 12.9 ± 30.6 | 0.199 |
| Post-exercise 6-week pad (g) | 14.2 ± 45.6 | 18.7 ± 23.8 | 0.676 |
| Post-exercise 6-week pad number | 1.67 ± 2.1 | 4.2 ± 5.8 | 0.034 |
| Post-exercise 12-week pad (g) | 0 | 14.7 ± 25.1 | 0.002 |
| Post-exercise 12-week pad number | 0.4 ± 0.5 | 2.14 ± 2.4 | <0.001 |
| Continent Group (n = 31) | Incontinent Group (n = 22) | p-Value | |||
|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ||
| Isokinetic 60°/s peak torque/Bodyweight, muscle strength | |||||
| Hip Extensor (Nm) | |||||
| Pre/Post exercise muscle strength | 119.5 + 41.7 | 145.9 + 41.3 | 138.0 + 67.5 | 139.6 + 55.4 | |
| Change of muscle strength | 22.3 ± 39.7 | −9.5 ± 32.4 | 0.005 | ||
| Hip Flexor (Nm) | |||||
| Pre/Post exercise muscle strength | 78.1 + 25.9 | 92.2 + 26.1 | 85.0 + 34.1 | 90.6 + 19.3 | |
| Change of muscle strength | 11.5 ± 26.9 | 1.4 ± 27.2 | 0.204 | ||
| Hip Abductor (Nm) | |||||
| Pre/Post exercise muscle strength | 75.5 + 19.4 | 87.5 + 28.2 | 70.5 + 24.7 | 71.9 + 32.7 | |
| Change of muscle strength | 12.0 ± 26.4 | 10.2 ± 26.3 | 0.811 | ||
| Hip Adductor (Nm) | |||||
| Pre/Post exercise muscle strength | 109.1 + 37.7 | 122.2 + 40.5 | 116.1 + 43.5 | 130.7 + 41.5 | |
| Change of muscle strength | 21.7 ± 48.4 | 3.9 ± 31.0 | 0.153 | ||
| Isokinetic 180°/s peak torque / Bodyweight, muscle endurance | |||||
| Hip Extensor (Nm) | |||||
| Pre/Post exercise muscle endurance | 85.3 + 65.4 | 106.9 + 38.8 | 102.5 + 53.9 | 105.1 + 42.6 | |
| Change of muscle endurance | 18.8 ± 43.6 | −5.6 ± 33.1 | 0.038 | ||
| Hip Flexor (Nm) | |||||
| Pre/Post exercise muscle endurance | 65.1 + 65.4 | 62.1 + 17.4 | 58.8 + 25.2 | 66.5 + 18.1 | |
| Change of muscle endurance | −5.2 ± 61.9 | 4.2 ± 20.1 | 0.517 | ||
| Hip Abductor (Nm) | |||||
| Pre/Post exercise muscle endurance | 63.0 + 21.0 | 70.9 + 24.0 | 64.8 + 23.0 | 66.5 + 18.1 | |
| Change of muscle endurance | 7.9 ± 25.6 | 3.1 ± 14.3 | 0.449 | ||
| Hip Adductor (Nm) | |||||
| Pre/Post exercise muscle endurance | 79.3 + 36.3 | 89.3 + 29.9 | 82.4 + 30.4 | 89.1 + 36.2 | |
| Change of muscle endurance | 10.0 ± 32.2 | 5.7 ± 27.7 | 0.624 | ||
| Univariate | Multivariate | |||
|---|---|---|---|---|
| p-Value | OR (95% CI) | p Value | OR (95% CI) | |
| Age | 0.897 | 0.994 (0.901–1.096) | 0.686 | 0.965 (0.811–1.148) |
| BMI | 0.354 | 0.943 (0.833–1.067) | 0.800 | 0.963 (0.719–1.289) |
| Prostate volume | 0.822 | 0.997 (0.968–1.026) | 0.454 | 0.984 (0.942–1.027) |
| Pathologic T stage | 0.293 | 0.550 (0.181–1.675) | 0.773 | 1.369 (0.162–11.535) |
| Operative Methods (RRP vs. RALP) | 0.983 | 0.988 (0.330–2.962) | 0.553 | 1.811 (0.280–11.703) |
| MUCP | 0.045 | 1.031 (1.001–1.061) | 0.097 | 1.046 (0.992–1.103) |
| Change of hip extensor muscle strength (Nm) | 0.010 | 1.029 (1.007–1.053) | 0.045 | 1.039 (1.001–1.080) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Yoon, D.H.; Yoo, S.; Cho, S.Y.; Cho, M.C.; Han, G.-Y.; Song, W.; Jeong, H. Effects of Progressive Resistance Training on Post-Surgery Incontinence in Men with Prostate Cancer. J. Clin. Med. 2018, 7, 292. https://doi.org/10.3390/jcm7090292
Park J, Yoon DH, Yoo S, Cho SY, Cho MC, Han G-Y, Song W, Jeong H. Effects of Progressive Resistance Training on Post-Surgery Incontinence in Men with Prostate Cancer. Journal of Clinical Medicine. 2018; 7(9):292. https://doi.org/10.3390/jcm7090292
Chicago/Turabian StylePark, Juhyun, Dong Hyun Yoon, Sangjun Yoo, Sung Yong Cho, Min Chul Cho, Ga-Young Han, Wook Song, and Hyeon Jeong. 2018. "Effects of Progressive Resistance Training on Post-Surgery Incontinence in Men with Prostate Cancer" Journal of Clinical Medicine 7, no. 9: 292. https://doi.org/10.3390/jcm7090292
APA StylePark, J., Yoon, D. H., Yoo, S., Cho, S. Y., Cho, M. C., Han, G.-Y., Song, W., & Jeong, H. (2018). Effects of Progressive Resistance Training on Post-Surgery Incontinence in Men with Prostate Cancer. Journal of Clinical Medicine, 7(9), 292. https://doi.org/10.3390/jcm7090292