Regeneration of Transected Recurrent Laryngeal Nerve Using Hybrid-Transplantation of Skeletal Muscle-Derived Stem Cells and Bioabsorbable Scaffold

 ,
,
Abstract
1. Introduction
2. Experimental Section
2.1. Animals
2.2. Cell Purification
2.3. Preparation of RLN Transected Model and Application of Hybrid-Transplantation
2.4. Measurement of Vocal Cord Movement
2.5. Macroscopic Observation and Immunostaining
2.6. Quantitative Real-Time PCR for Peripheral Nerve-Related Growth Factors
3. Results
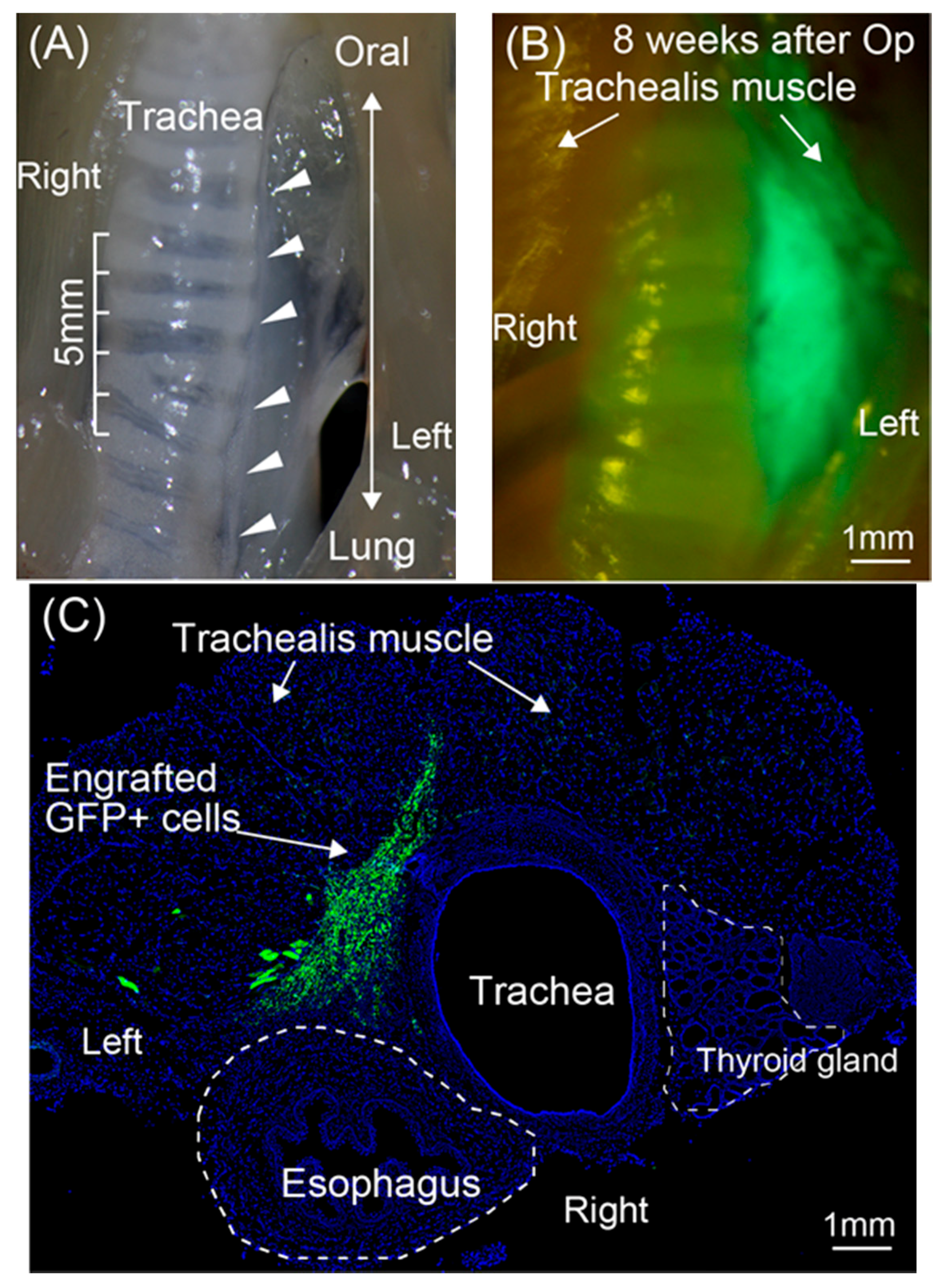
3.1. Engraftment of GFP+ Cells/Tissue around the RLN
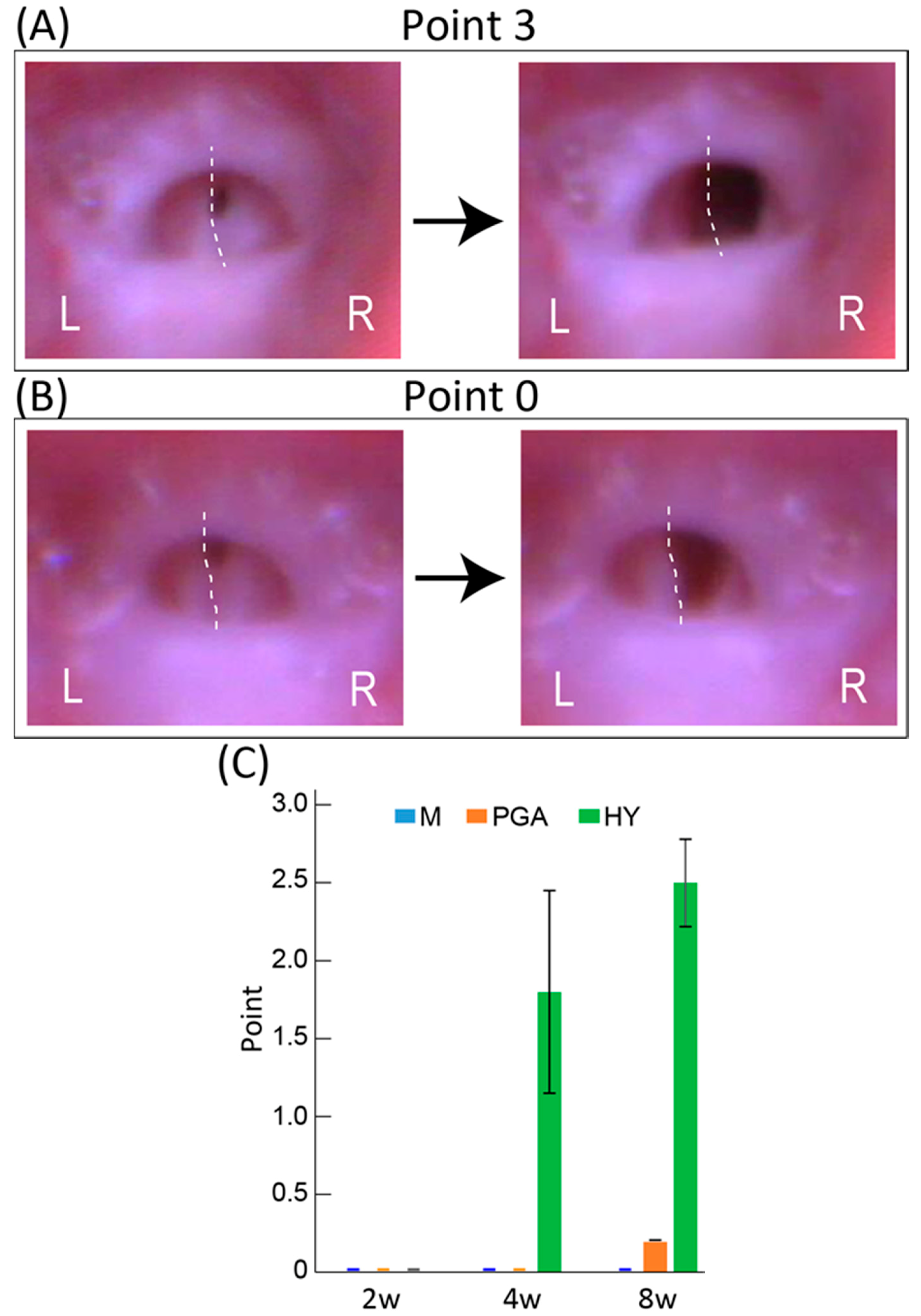
3.2. Functional Recovery of Vocal Cord Movement
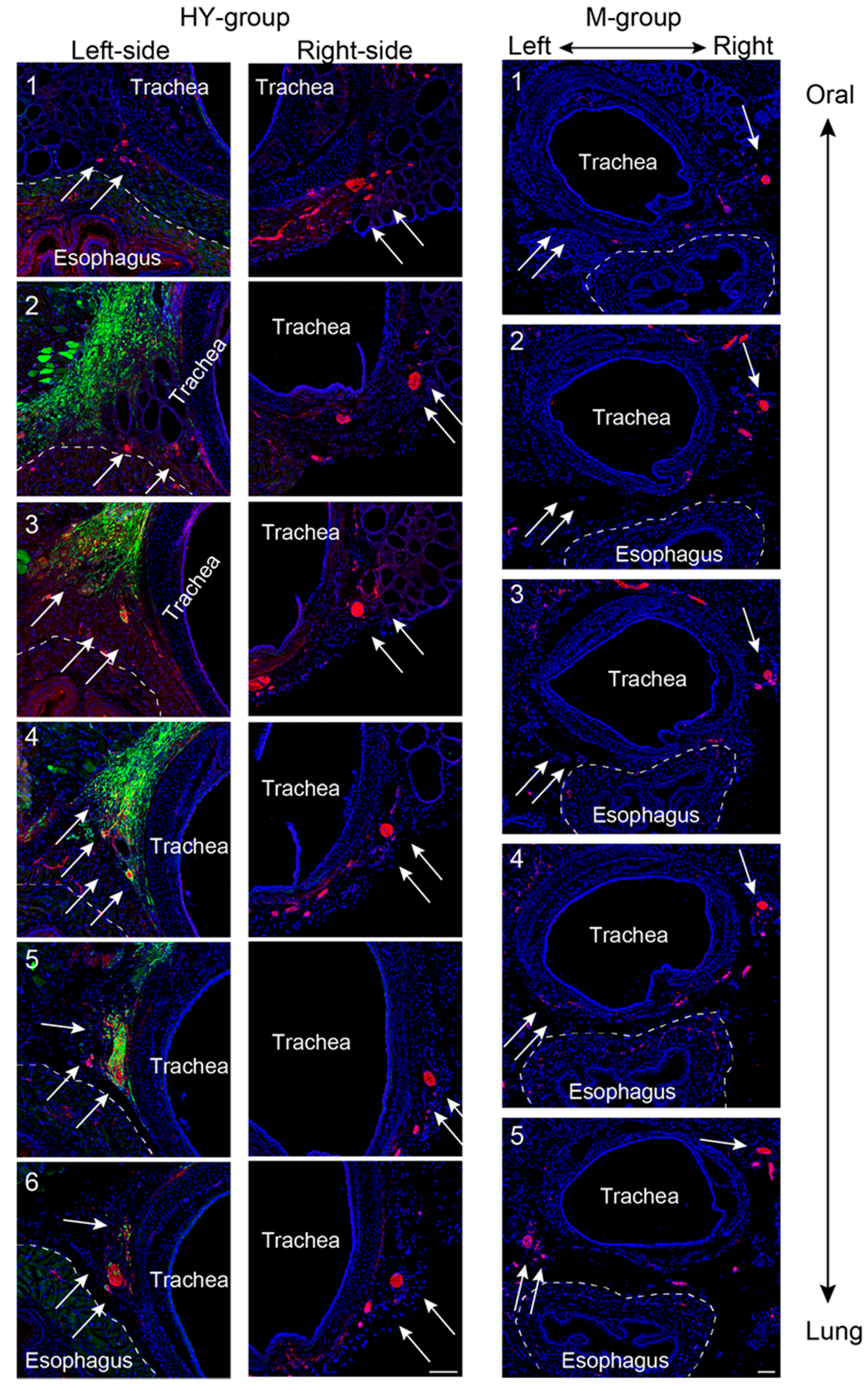
3.3. Morphological Regeneration of the RLN Demonstrated Using Serial Histological Sections
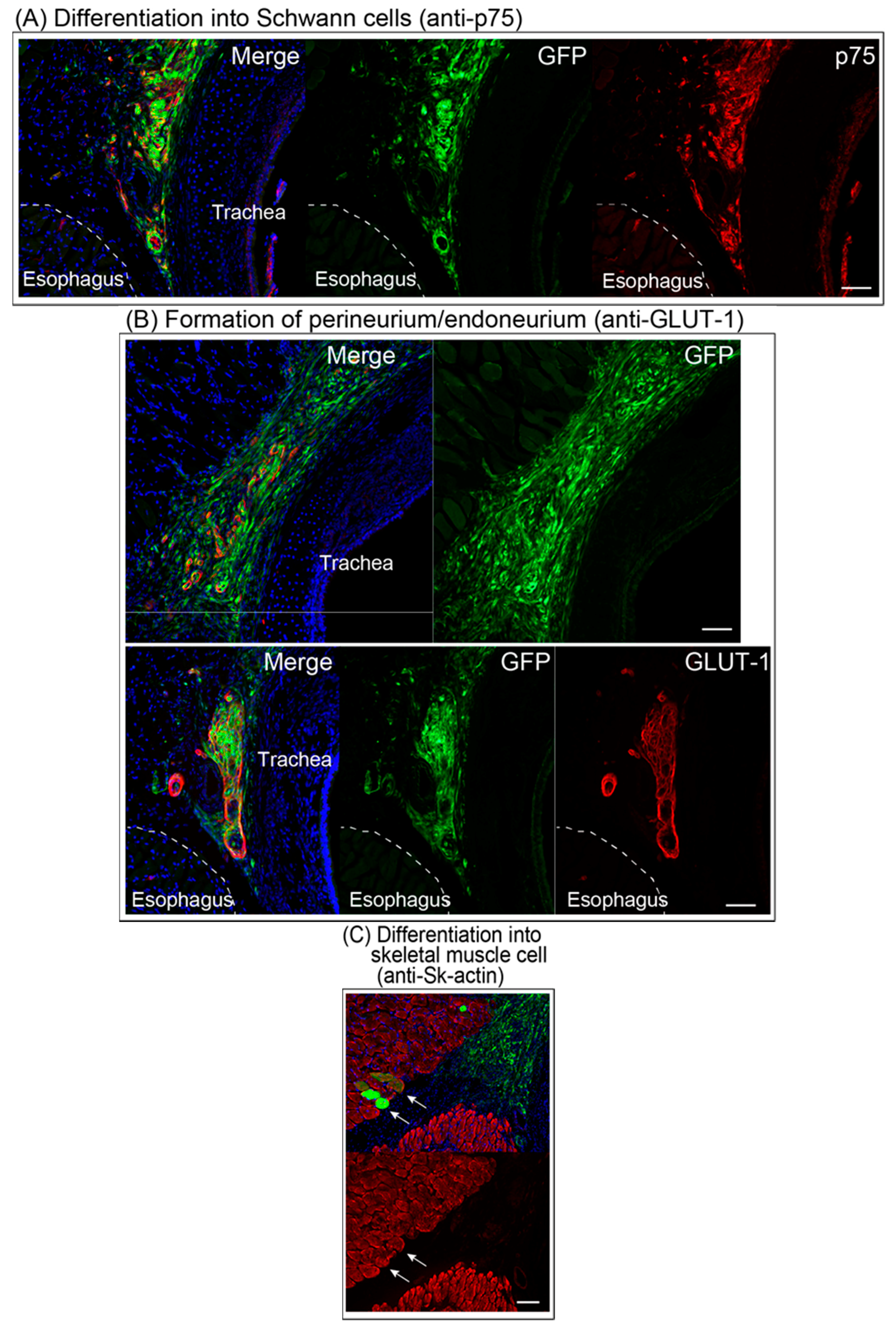
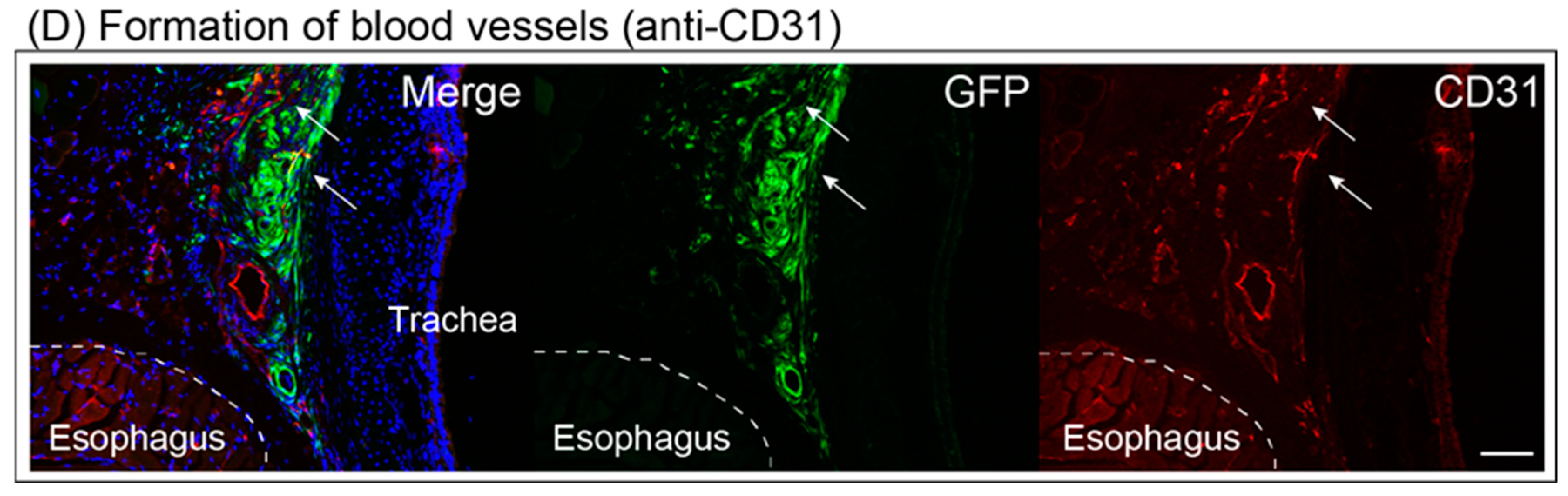
3.4. Differentiation of Engrafted Sk-MSCs
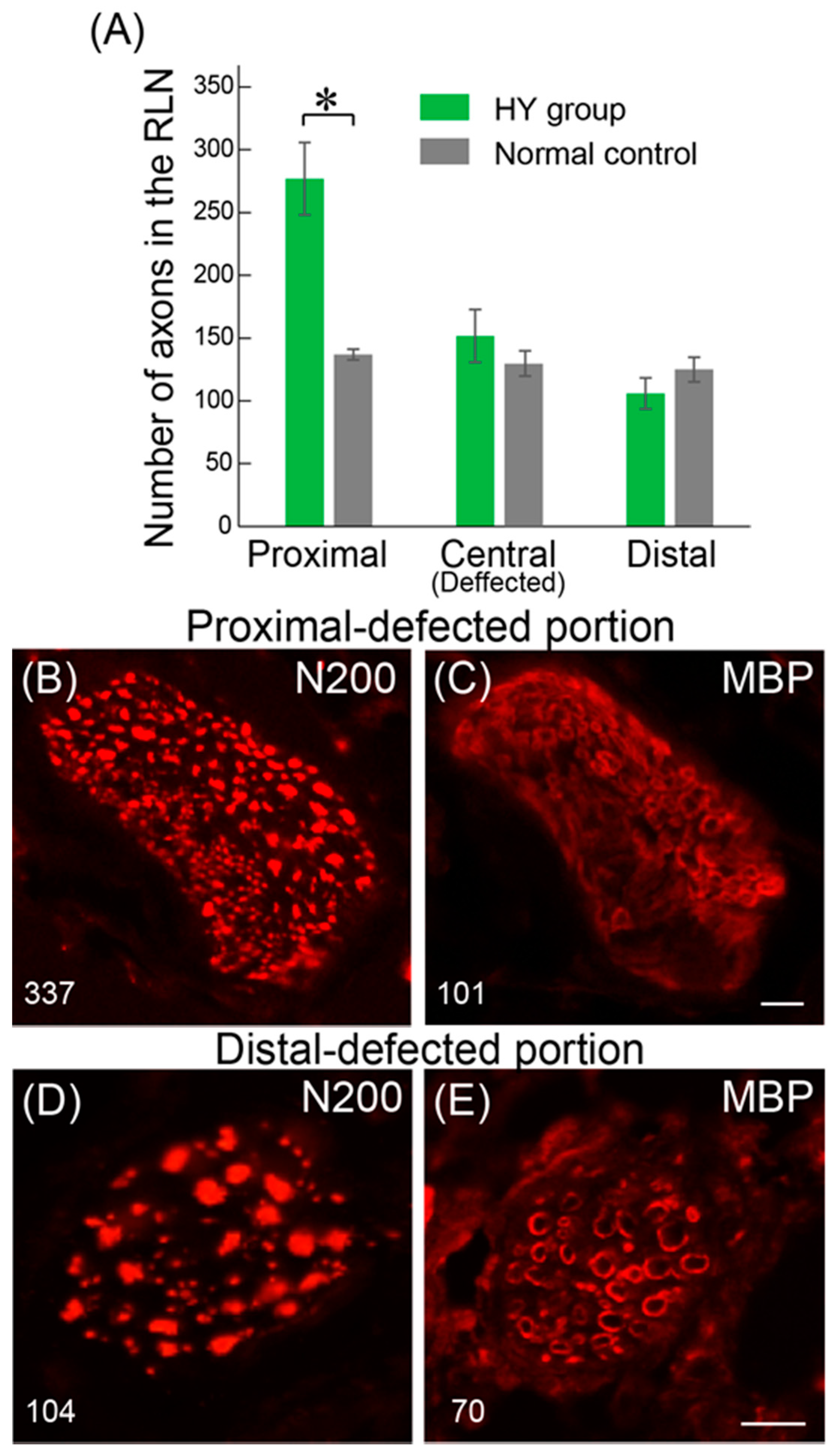
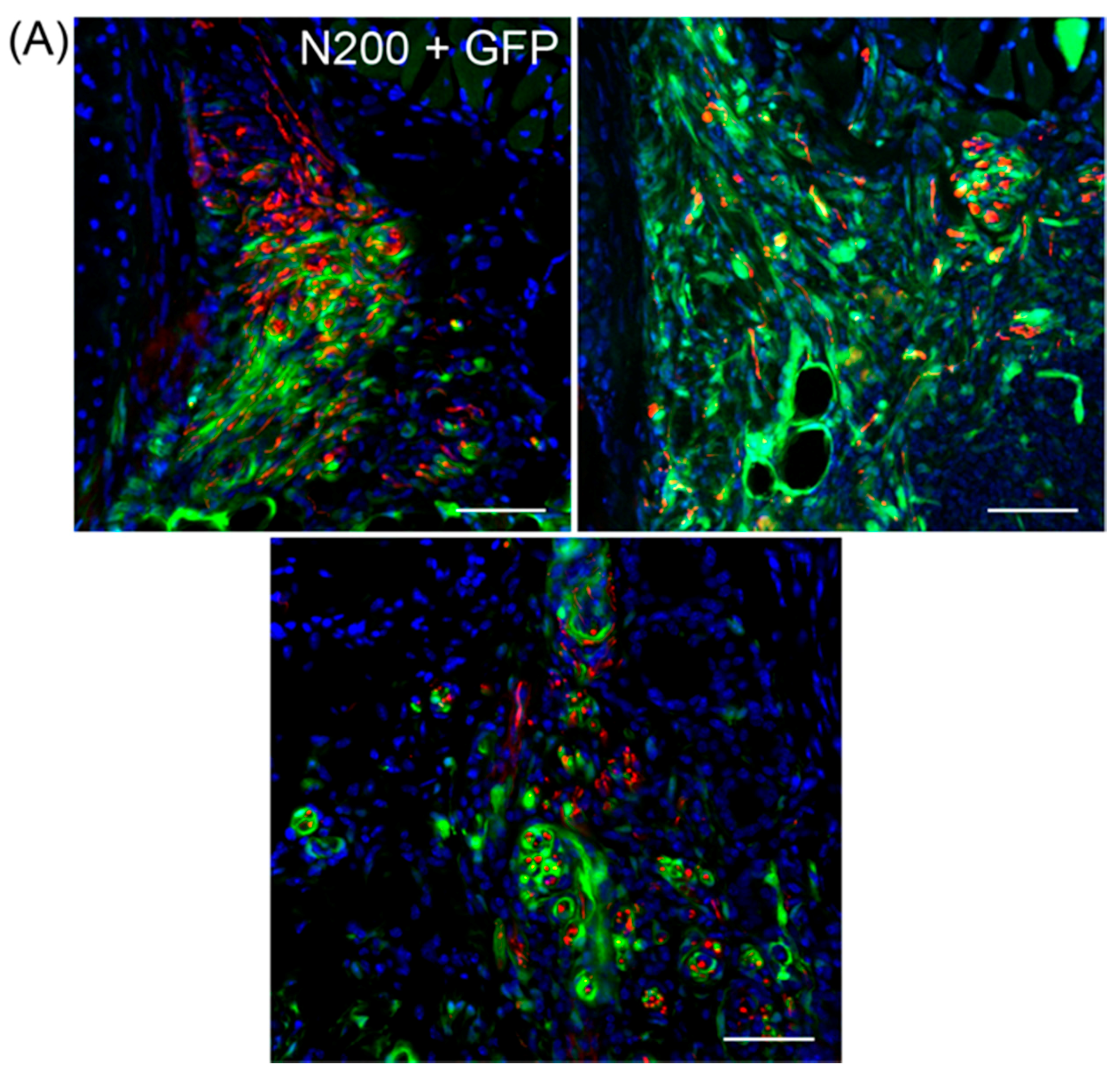
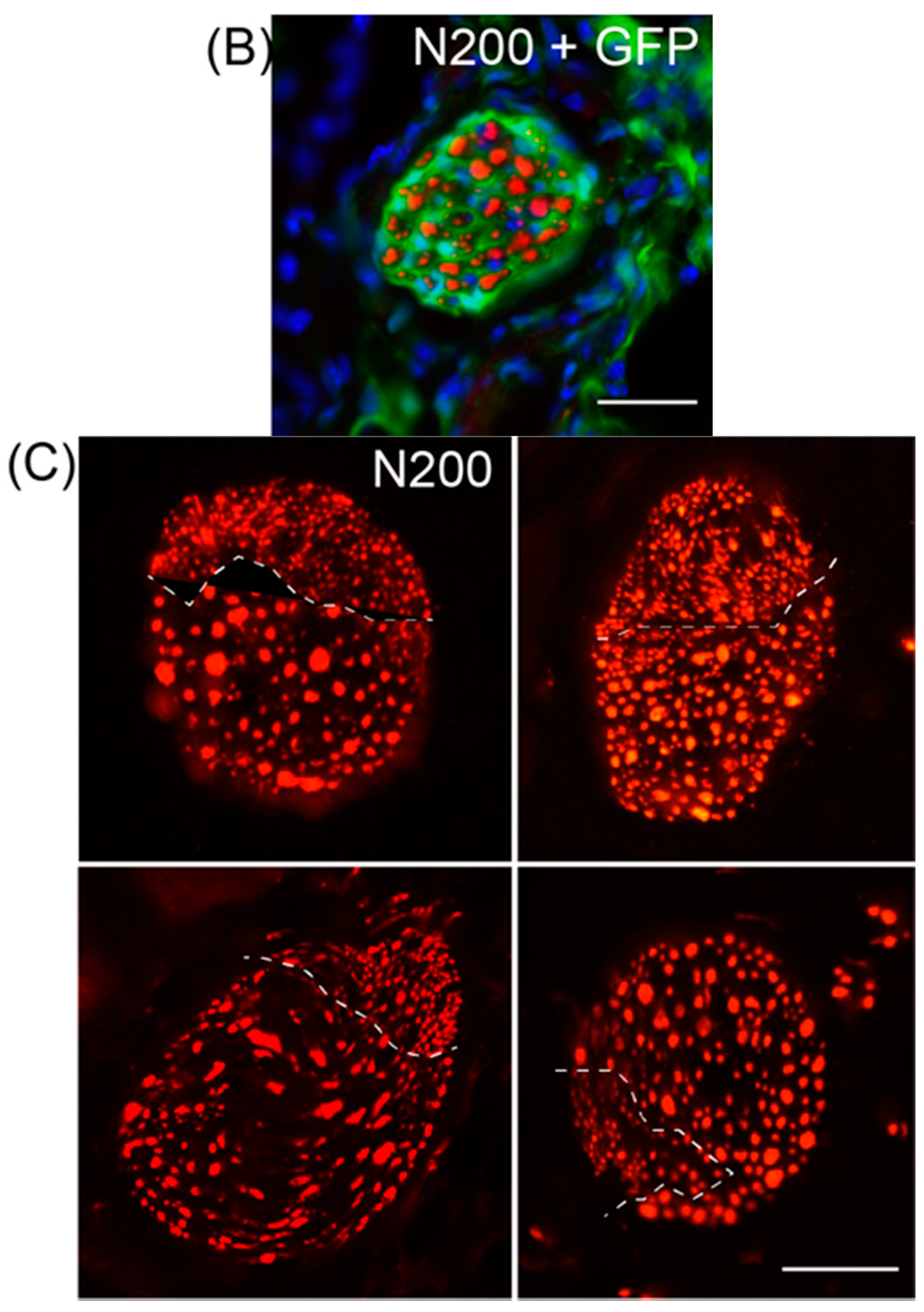
3.5. Variations in Axonal Regeneration in the Nerve Defect Central- and Pre-Portions
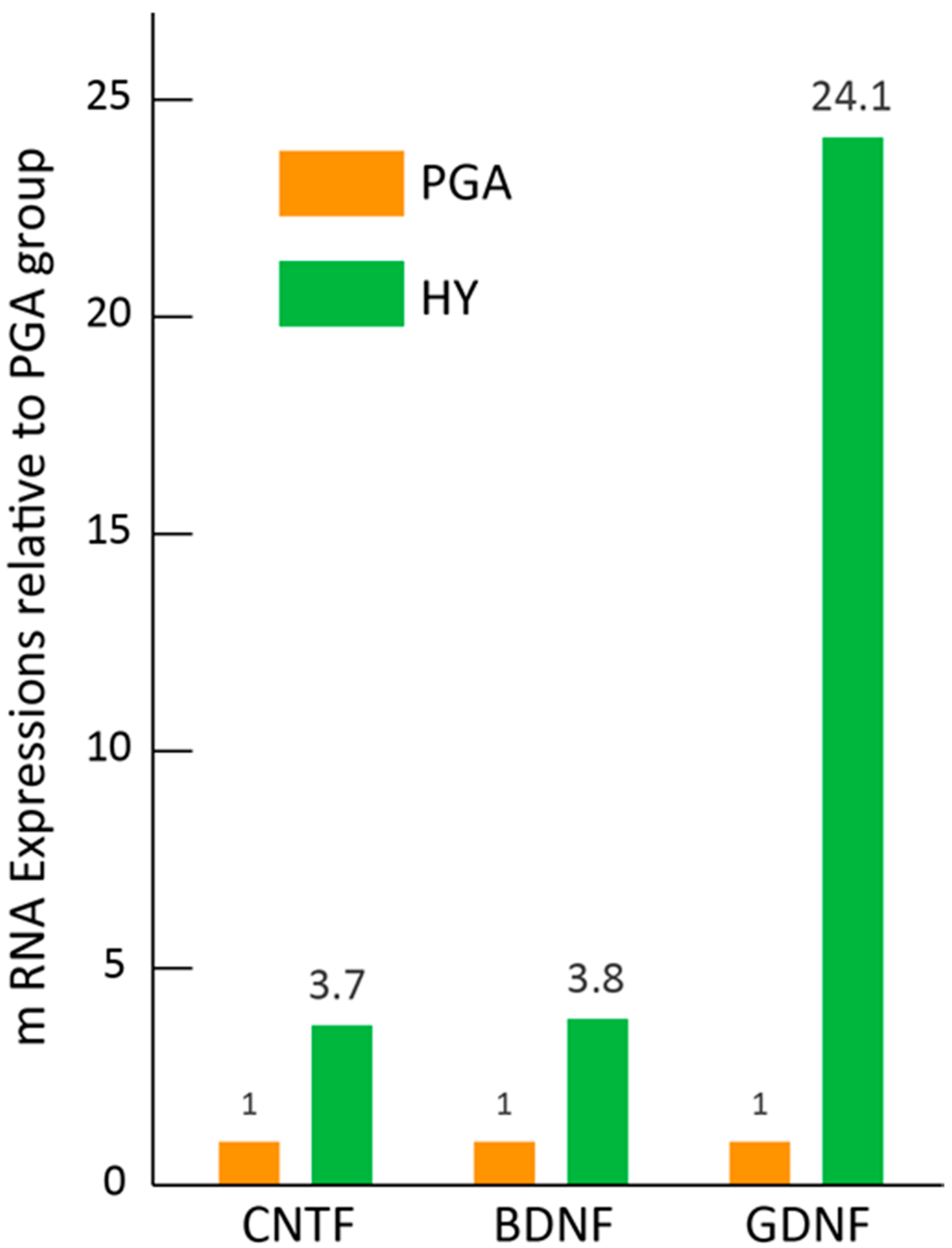
3.6. Paracrine Effect of HY Transplantation in Vivo
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Spector, B.C.; Netterville, J.L.; Billante, C.; Clary, J.; Reinisch, L.; Smith, T.L. Quality-of-life assessment in patients with unilateral vocal cord paralysis. Otolaryngol. Head Neck Surg. 2001, 125, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Pei, Y.C.; Fang, T.J.; Hsin, L.J.; Li, H.Y.; Wong, A.M. Early hyaluronate injection improves quality of life but not neural recovery in unilateral vocal fold paralysis: An open-label randomized controlled study. Restor. Neurol. Neurosci. 2015, 33, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Yuan, J.; Chen, X.; Xu, J.; Li, Y.; Dong, P. Functional regeneration of the transected recurrent laryngeal nerve using a collagen scaffold loaded with laminin and laminin-binding BDNF and GDNF. Sci. Rep. 2016, 6, 32292. [Google Scholar] [CrossRef] [PubMed]
- Halum, S.L.; McRae, B.; Bijangi-Vishehsaraei, K.; Hiatt, K. Neurotrophic factor-secreting autologous muscle stem cell therapy for the treatment of laryngeal denervation injury. Laryngoscope 2012, 122, 2482–2496. [Google Scholar] [CrossRef] [PubMed]
- Lerner, M.Z.; Matsushita, T.; Lankford, K.L.; Radtke, C.; Kocsis, J.D.; Young, N.O. Intravenous mesenchymal stem cell therapy after recurrent laryngeal nerve injury: A preliminary study. Laryngoscope 2014, 124, 2555–2560. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, T.; Hirata, M.; Soeda, S.; Nakajima, N.; Saito, K.; Nakazato, K.; Okada, Y.; Hashimoto, H.; Uchiyama, Y.; Mochida, J. Preferential and comprehensive reconstitution of severely damaged sciatic nerve using murine skeletal muscle-derived multipotent stem cells. PLoS ONE 2014, 9, e91257. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, T.; Hirata, M.; Nakajima, N.; Saito, K.; Hashimoto, H.; Soeda, S.; Uchiyama, Y.; Watanabe, M. A long-gap peripheral nerve injury therapy using human skeletal muscle-derived stem cells (Sk-SCs): An achievement of significant morphological, numerical and functional recovery. PLoS ONE 2016, 11, e0166639. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, T.; Uchiyama, Y.; Okada, Y.; Ishikawa, T.; Sato, M.; Akatsuka, A.; Asahara, T. Functional recovery of damaged skeletal muscle through synchronized vasculogenesis, myogenesis, and neurogenesis by muscle-derived stem cells. Circulation 2005, 112, 2857–2866. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, T.; Okada, Y.; Uchiyama, Y.; Tono, K.; Masuda, M.; Wada, M.; Hoshi, A.; Akatsuka, A. Synchronized reconstitution of muscle fibers, peripheral nerves and blood vessels by murine skeletal muscle-derived CD34−/45− cells. Histochem. Cell Biol. 2007, 128, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, T.; Uchiyama, Y.; Hirata, M.; Hashimoto, H.; Nakajima, N.; Saito, K.; Terachi, T.; Mochida, J. Therapeutic isolation and expansion of human skeletal muscle-derived stem cells for the use of muscle-nerve-blood vessel reconstitution. Front. Physiol. 2015, 6, 165. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Tamaki, T.; Hirata, M.; Hashimoto, H.; Nakazato, K.; Nakajima, N.; Kazuno, A.; Sakai, A.; Iida, M.; Okami, K. Reconstruction of multiple facial nerve branches using skeletal muscle-derived multipotent stem cell sheet-pellet transplantation. PLoS ONE 2015, 10, e0138371. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, A.; Tamaki, T.; Tono, K.; Okada, Y.; Akatsuka, A.; Usui, Y.; Terachi, T. Reconstruction of radical prostatectomy-induced urethral damage using skeletal muscle-derived multipotent stem cells. Transplantation 2008, 85, 1617–1624. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, N.; Tamaki, T.; Hirata, M.; Soeda, S.; Nitta, M.; Hoshi, A.; Terachi, T. Purified human skeletal muscle-derived stem cells enhance the repair and regeneration in the damaged urethra. Transplantation 2017, 101, 2312–2320. [Google Scholar] [CrossRef] [PubMed]
- Soeda, S.; Tamaki, T.; Hashimoto, H.; Saito, K.; Sakai, A.; Nakajima, N.; Nakazato, K.; Masuda, M.; Terachi, T. Functional nerve-vascular reconstitution of the bladder-wall; application of patch transplantation of skeletal muscle-derived multipotent stem cell sheet-pellets. J. Stem Cell Res. Ther 2013, 3, 142. [Google Scholar] [CrossRef]
- Nitta, M.; Tamaki, T.; Tono, K.; Okada, Y.; Masuda, M.; Akatsuka, A.; Hoshi, A.; Usui, Y.; Terachi, T. Reconstitution of experimental neurogenic bladder dysfunction using skeletal muscle-derived multipotent stem cells. Transplantation 2010, 89, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, K.; Tamaki, T.; Hirata, M.; Kazuno, A.; Kohno, M.; Masuda, R.; Iwazaki, M. Three-dimensional reconstitution of nerve blood vessel units on damaged trachea and bronchial stump using hybrid-transplantation of skeletal muscle-derived stem cells and bioabsorbable polyglyconate felt. J. Regen. Med. 2015, 4. [Google Scholar]
- Suzuki, H.; Araki, K.; Matsui, T.; Tomifuji, M.; Yamashita, T.; Kobayashi, Y.; Shiotani, A. Value of a novel PGA-collagen tube on recurrent laryngeal nerve regeneration in a rat model. Laryngoscope 2016, 126, E233–E239. [Google Scholar] [CrossRef] [PubMed]
- Okabe, M.; Ikawa, M.; Kominami, K.; Nakanishi, T.; Nishimune, Y. ‘Green mice’ as a source of ubiquitous green cells. FEBS Lett. 1997, 407, 313–319. [Google Scholar] [CrossRef]
- Tamaki, T.; Akatsuka, A.; Ando, K.; Nakamura, Y.; Matsuzawa, H.; Hotta, T.; Roy, R.R.; Edgerton, V.R. Identification of myogenic-endothelial progenitor cells in the interstitial spaces of skeletal muscle. J. Cell Biol. 2002, 157, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, T.; Akatsuka, A.; Okada, Y.; Matsuzaki, Y.; Okano, H.; Kimura, M. Growth and differentiation potential of main- and side-population cells derived from murine skeletal muscle. Exp. Cell Res. 2003, 291, 83–90. [Google Scholar] [CrossRef]
- Tamaki, T.; Okada, Y.; Uchiyama, Y.; Tono, K.; Masuda, M.; Nitta, M.; Hoshi, A.; Akatsuka, A. Skeletal muscle-derived CD34+/45− and CD34−/45− stem cells are situated hierarchically upstream of pax7+ cells. Stem Cells Dev. 2008, 17, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Krimm, R.F. Developmental expression of Bdnf, Ntf4/5, and TrkB in the mouse peripheral taste system. Dev. Dyn. 2010, 239, 2637–2646. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.H.; Hung, H.A.; Svaren, J. Epigenomic regulation of schwann cell reprogramming in peripheral nerve injury. J. Neurosci. 2016, 36, 9135–9147. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, S.K.; Hinkle, M.L.; Nicolini, J.; Rambo, L.N.; Rexwinkle, A.M.; Rose, S.J.; Sabatier, M.J.; Backus, D.; English, A.W. Misdirection of regenerating axons and functional recovery following sciatic nerve injury in rats. J. Comp. Neurol. 2011, 519, 21–33. [Google Scholar] [CrossRef] [PubMed]
- De Ruiter, G.C.; Spinner, R.J.; Verhaagen, J.; Malessy, M.J. Misdirection and guidance of regenerating axons after experimental nerve injury and repair. J. Neurosurg. 2014, 120, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Mi, D.; Zhang, T.; Zhang, Y.; Yan, J.; Wang, Y.; Tan, X.; Yuan, Y.; Yang, Y.; Gu, X.; et al. Tubulation repair mitigates misdirection of regenerating motor axons across a sciatic nerve gap in rats. Sci. Rep. 2018, 8, 3443. [Google Scholar] [CrossRef] [PubMed]
- Montani, L.; Petrinovic, M.M. Targeting axonal regeneration: The growth cone takes the lead. J. Neurosci. 2014, 34, 4443–4444. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Medina, M.; Gregus, K.A.; Nichol, R.H.; O’Toole, S.M.; Gomez, T.M. Regulation of ecm degradation and axon guidance by growth cone invadosomes. Development 2015, 142, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Lundborg, G.; Rosen, B.; Dahlin, L.; Holmberg, J.; Rosen, I. Tubular repair of the median or ulnar nerve in the human forearm: A 5-year follow-up. J. Hand Surg. Br. 2004, 29, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Weber, R.A.; Breidenbach, W.C.; Brown, R.E.; Jabaley, M.E.; Mass, D.P. A randomized prospective study of polyglycolic acid conduits for digital nerve reconstruction in humans. Plast. Reconstr. Surg. 2000, 106, 1036–1045. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evaluation | 2w (n = 6) | 4w (n = 5) | 8w (n = 10) |
|---|---|---|---|
| Point 0 | 100% | 20% | 0% |
| Point 1 | 0% | 20% | 20% |
| Point 2 | 0% | 20% | 10% |
| Point 3 | 0% | 40% | 70% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazuno, A.; Maki, D.; Yamato, I.; Nakajima, N.; Seta, H.; Soeda, S.; Ozawa, S.; Uchiyama, Y.; Tamaki, T. Regeneration of Transected Recurrent Laryngeal Nerve Using Hybrid-Transplantation of Skeletal Muscle-Derived Stem Cells and Bioabsorbable Scaffold. J. Clin. Med. 2018, 7, 276. https://doi.org/10.3390/jcm7090276
Kazuno A, Maki D, Yamato I, Nakajima N, Seta H, Soeda S, Ozawa S, Uchiyama Y, Tamaki T. Regeneration of Transected Recurrent Laryngeal Nerve Using Hybrid-Transplantation of Skeletal Muscle-Derived Stem Cells and Bioabsorbable Scaffold. Journal of Clinical Medicine. 2018; 7(9):276. https://doi.org/10.3390/jcm7090276
Chicago/Turabian StyleKazuno, Akihito, Daisuke Maki, Ippei Yamato, Nobuyuki Nakajima, Hiroya Seta, Shuichi Soeda, Soji Ozawa, Yoshiyasu Uchiyama, and Tetsuro Tamaki. 2018. "Regeneration of Transected Recurrent Laryngeal Nerve Using Hybrid-Transplantation of Skeletal Muscle-Derived Stem Cells and Bioabsorbable Scaffold" Journal of Clinical Medicine 7, no. 9: 276. https://doi.org/10.3390/jcm7090276
APA StyleKazuno, A., Maki, D., Yamato, I., Nakajima, N., Seta, H., Soeda, S., Ozawa, S., Uchiyama, Y., & Tamaki, T. (2018). Regeneration of Transected Recurrent Laryngeal Nerve Using Hybrid-Transplantation of Skeletal Muscle-Derived Stem Cells and Bioabsorbable Scaffold. Journal of Clinical Medicine, 7(9), 276. https://doi.org/10.3390/jcm7090276