
Kidney Transplantation in the Diabetic Patient

Abstract
:1. Introduction
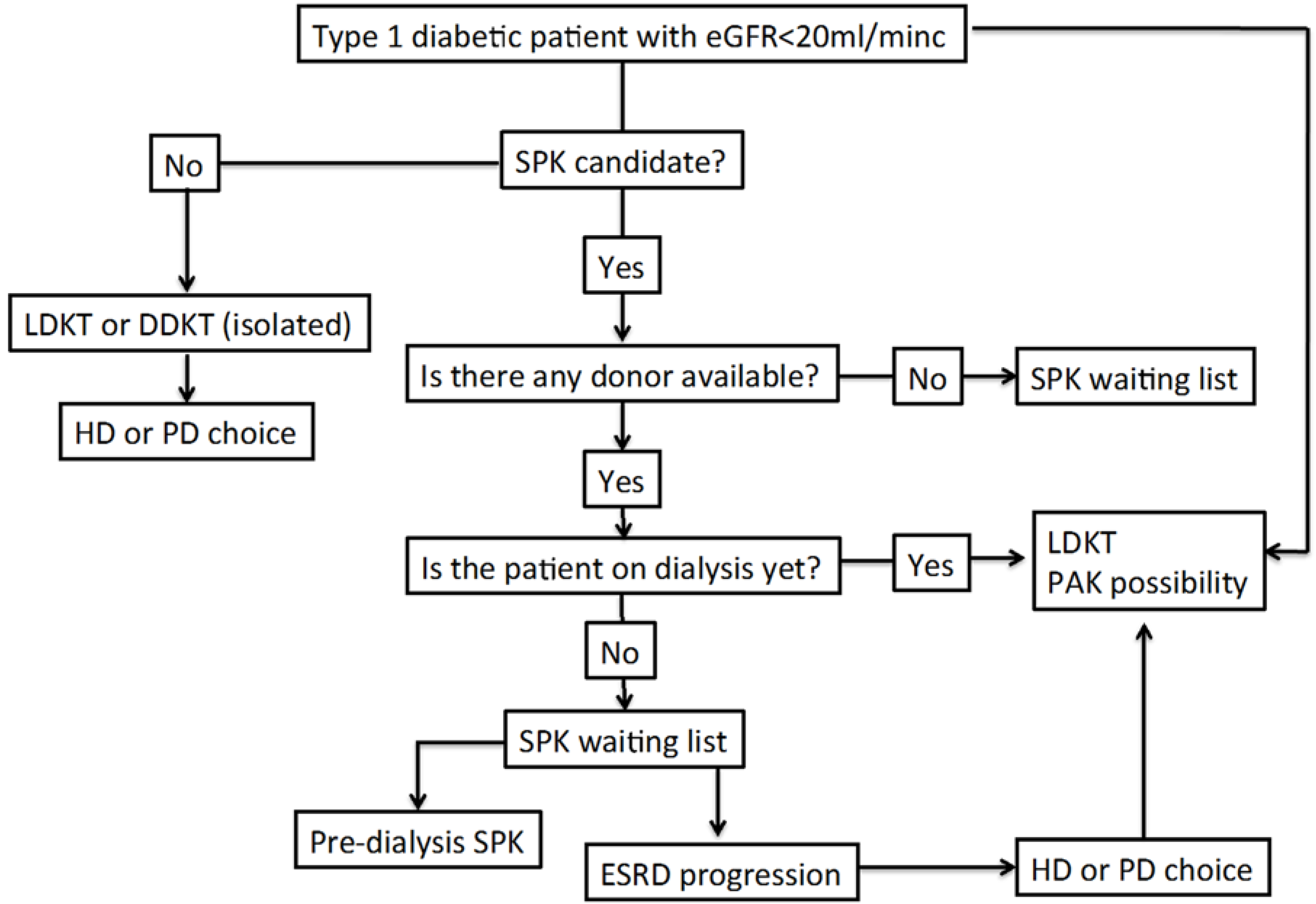
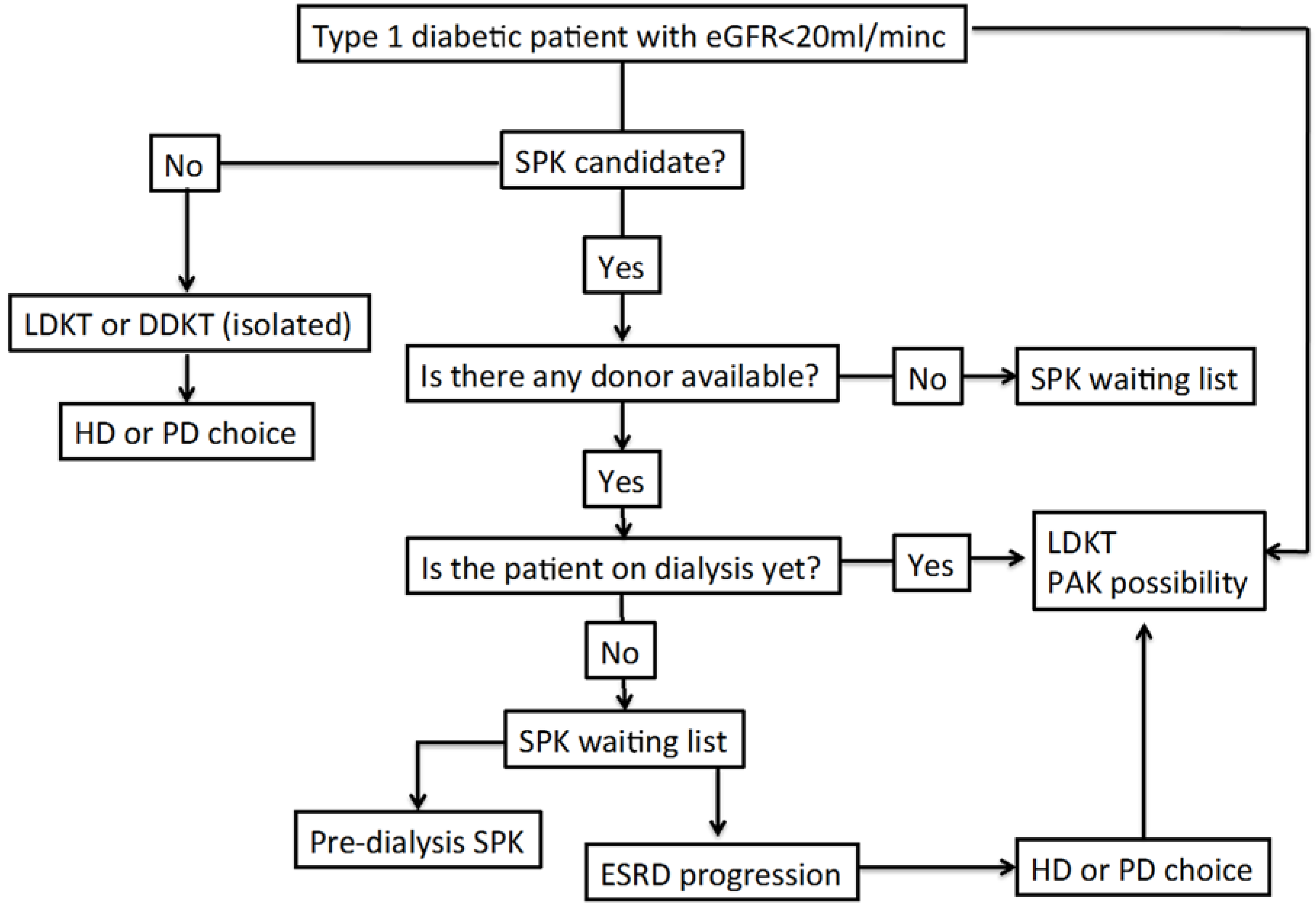
2. Transplantation Therapy Options
3. Results of Transplantation in Type 1 Diabetic Patients

{kind=link}
| Life-Years | Quality Life-Years | |
|---|---|---|
| Living donor KT | 18.3 | 10.3 |
| PAK transplantation | 17.2 | 10 |
| SPK transplantation | 15.7 | 9.1 |
| Deceased donor KT | 11.4 | 6.5 |
| Dialysis | 7.8 | 4.5 |
| Observation Period | Patient Survival | Kidney Graft Survival | Source/Database | Ref |
|---|---|---|---|---|
| Until 244th day | Dialysis > DDKT | Not applicable | USRDS | [5] |
| 3–6 years | SPK = DDKT | SPK = DDKT | UNOS | [20] |
| 0–7 years | LDKT > SPK = DDKT | LDKT > SPK = DDKT | OPTN/UNOS | [15] |
| Until 7 years | SPK (P+) > LDKT > DDKTLDKT > SPK | SPK (P+) > LDKT > DDKTLDKT > SPK | SRTR | [18] |
| (P-) = DDKT | (P-) = DDKT | |||
| 2–9 years | SPK = DDKT | SPK = DDKT | UNOS | [21] |
| 0–10 years | SPK > DDKT | SPK = DDKT | Irish Center | [22] |
| Until 10 years | LDKT = SPK > DDKT | LDKT = SPK > DDKT | US Center | [23] |
| Mean = 4.8 years | LDKT = SPK > DDKT | LDKT = SPK > DDKT | UNOS | [24] |
| 0–12 years | Not applicable | SPK > DDKT | OPTN/UNOS/SRTR | [25] |
| 18 years | SPK > LDKT > DDKT | SPK = LDKT > DDKT | CTS | [18] |
| 20 years | SPK > LDKT > DDKT | SPK > LDKT > DDKT | CTS | [20] |
4. Results of Transplantation in Type 2Diabetic Patients
5. Predialysis Kidney Transplant Results
6. Summary and Conclusion: The Way to the Best Quality in Diabetic Patient Care with CKD
Acknowledgments
Author Contributions
Conflicts of Interest
References
- United States Renal Data System. The 2014 Annual Date Report. Chapter 1: Incidence, prevalence, patient characteristics, and treatment modalities. Available online: http://www.usrds.org/2014/view/ (accessed on 6 June 2015).
- Sociedad Española de Nefrología (S.E.N.). Informe de 2013 (Congreso de Barcelona, 2014). Available online: http://www.senefro.org/modules.php?name=webstructure&idwebstructure=128 (accessed on 6 June 2015).
- Healthypeople.gov. 2020 Topics & Objectives. Chronic Kidney Disease. Available online: http://www.healthypeople.gov/2020/ (accessed on 6 June 2015).
- Williams, M.E.; Lacson, E.; Teng, M.; Ofsthum, N.; Lazarus, J.M. Hemodialyzed type I and type II diabetic patients in the US: Characteristics, glycemic control and survival. Kidney Int. 2006, 70, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation and recipients of first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Schnuelle, P.; Lorenz, D.; Trede, M.; van der Woude, F.J. Impact of renal cadaveric transplantation on survival in end-stage renal failure: Evidence for reduced mortality risk compared with hemodialysis during long-term follow-up. J. Am. Soc. Nephrol. 1998, 9, 2135–2141. [Google Scholar] [PubMed]
- McDonald, S.P.; Russ, G.R. Survival of recipients of cadaveric kidney transplants compared with those receiving dialysis treatment in Australia and New Zealand 1991–2001. Nephrol. Dial. Transplant. 2002, 17, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Lloveras, J.; Arcos, E.; Comas, J.; Crespo, M.; Pascual, J. A paired survival analysis comparing hemodialysis and kidney transplantation from deceased elderly donors older than 65 years. Transplantation 2015, 99, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Matas, A.J.; Smith, J.M.; Skeans, M.A.; Lamb, K.E.; Gustafson, S.K.; Samana, C.J.; Stewart, D.E.; Snyder, J.J.; Israni, A.K.; Kasiske, B.L. OPTN/SRTR 2011 Annual Data Report: Kidney. Am. J. Transplant. 2013, 13, 11–46. [Google Scholar] [CrossRef] [PubMed]
- Fridell, J.A.; Powelson, J.A.; Sanders, C.E.; Ciancio, G.; Burke, G.W.; Stratta, R.J. Preparation of the pancreas allograft for transplantation. Clin. Transplant. 2011, 25, E103–E112. [Google Scholar] [CrossRef] [PubMed]
- Heilman, R.L.; Mazur, M.J.; Reddy, K.S. Immunosuppression in simultaneous pancreas-kidney transplantation: Progress to date. Drugs 2010, 70, 793–804. [Google Scholar] [CrossRef] [PubMed]
- Kandaswamy, R.; Skeans, M.A.; Gustafson, S.K.; Carrico, R.J.; Tyler, K.H.; Israni1, A.K.; Snyder, J.J.; Kasiske, B.L. OPTN/SRTR 2013 Annual Data Report: Pancreas. Am. J. Transplant. 2015, 15, 1–20. [Google Scholar] [CrossRef] [PubMed]
- VanDellen, D.; Worthington, J.; Mitu-Pretorian, O.M.; Ghazanfar, A.; Forgacs, B.; Pararajasingam, R.; Campbell, B.; Parrott, N.R.; Augustine, T.; Tavakoli, A. Mortality in diabetes: Pancreas transplantation is associated with significant survival benefit. Nephrol. Dial. Transplant. 2013, 28, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Knoll, G.; Nichol, G. Dialysis, kidney transplantation or pancreas transplantation for patients with diabetes mellitus and renal failure: A decision analysis of treatment options. J. Am. Soc. Nephrol. 2003, 14, 500–515. [Google Scholar] [CrossRef] [PubMed]
- Poommipanit, N.; Sampaio, M.S.; Cho, Y.; Young, B.; Shah, T.; Pham, P.T.; Wilkinson, A.; Danovitch, G.; Bunnapradist, S. Pancreas after living donor kidney versus simultaneous pancreas-kidney transplant: An analysis of the organ procurement transplant network/United Network of Organ Sharing database. Transplantation 2010, 89, 1496–1503. [Google Scholar] [CrossRef] [PubMed]
- Young, B.Y.; Gill, J.; Huang, E.; Takemoto, S.K.; Anastasi, B.; Shah, T.; Bunnapradist, S. Living donor kidney versus simultaneous pancreas-kidney transplant in type I diabetics: An analysis of the OPTN/UNOS database. Clin. J. Am. Soc. Nephrol. 2009, 4, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Kamgar, M.; Huang, E.; Kamgar, M.; Nata, N.; Leeaphorn, N.; Kalantar-Zadeh, K.; Bunnapradist, S. Zero-mismatch deceased-donor kidney versus simultaneous pancreas-kidney transplantation. Transplantation 2012, 94, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Morath, C.; Zeier, M.; Dohler, B.; Schmidt, J.; Nawroth, P.P.; Opelz, G. Metabolic control improves long-term renal allograft and patient survival in type I diabetes. J. Am. Soc. Nephrol. 2008, 19, 1557–1563. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.S.; Smits, G.; Wiseman, A.C. Twelve-month pancreas graft function significantly influences survival following simultaneous pancreas-kidney transplantation. Clin. J. Am. Soc. Nephrol. 2009, 4, 988–955. [Google Scholar] [CrossRef] [PubMed]
- Morath, C.; Zeier, M.; Dohler, B.; Schmidt, J.; Nawroth, P.P.; Schwenger, V.; Opelz, G. Transplantation of the type I diabetic patient: The long-term benefit of a functioning pancreas allograft. Clin. J. Am. Soc. Nephrol. 2010, 5, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Bunnapradist, S.; Cho, Y.W.; Cecka, J.M.; Wilkinson, A.; Danovitch, G.M. Kidney allograft and patient survival in type I diabetic recipients of cadaveric kidney alone versus simultaneous pancreas kidney transplants: A multivariate analysis of the UNOS database. J. Am. Soc. Nephrol. 2003, 14, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Waki, K.; Terasaki, P.I. Kidney graft and patient survival with and without a simultaneous pancreas utilizing contralateral kidneys from the same donor. Diabetes Care 2006, 29, 1670–1672. [Google Scholar] [CrossRef] [PubMed]
- Mohan, P.; Safi, K.; Little, D.M.; Donohoe, J.; Conlon, P.; Walshe, J.J.; O’Kelly, P.; Thompson, C.J.; Hickey, D.P. Improved patient survival in recipients of simultaneous pancreas-kidney transplant compared with kidney transplant alone in patients with type 1 diabetes mellitus and end-stage renal disease. Br. J. Surg. 2003, 90, 1137–1141. [Google Scholar] [CrossRef] [PubMed]
- Rayhil, S.C.; D’Alessandro, A.M.; Odorico, J.S.; Knechtle, S.J.; Pirsch, J.D.; Heisey, D.M.; Kirk, A.D.; van der Werf, W.; Sollinger, H.W. Simultaneous pancreas-kidney transplantation and living related donor renal transplantation in patients with diabetes: Is there a difference in survival? Ann. Surg. 2000, 231, 417–423. [Google Scholar] [CrossRef]
- Reddy, K.S.; Stablein, D.; Taranto, S.; Stratta, R.J.; Johnston, T.D.; Waid, T.H.; McKeown, J.W.; Lucas, B.A.; Ranjan, D. Long-term survival following simultaneous kidney-pancreas transplantation versus kidney transplantation alone in patients with type 1 diabetes mellitus and renal failure. Am. J. Kidney Dis. 2003, 41, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Israni, A.K.; Feldman, H.I.; Propert, K.J.; Leonard, M.; Mange, K.C. Impact of simultaneous kidney-pancreas transplant and timing of transplant on kidney allograft survival. Am. J. Transplant. 2005, 5, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Norman, S.P.; Kommareddi, M.; Ojo, A.O.; Luan, F.L. Early pancreas graft failure is associated with inferior late clinical outcomes after simultaneous kidney-pancreas transplantation. Transplantation 2011, 92, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Pascual, J.; Abramowicz, D.; Cochat, P.; Claas, F.; Dudley, C.; Harden, P.; Heeman, U.; Hourmant, M.; Maggiore, U.; Salvadori, M.; et al. European renal best practice guideline on the management and evaluation of the kidney donor and recipient. Nefrologia 2014, 34, 293–301. [Google Scholar] [PubMed]
- Waki, K.; Sugawara, Y.; Kokudo, N.; Kadowaki, T. Long-term pancreas allograft survival in simultaneous pancreas-kidney transplantation by era. Clin. Transpl. 2012, 13–22. [Google Scholar]
- Becker, B.N.; Brazy, P.C.; Becker, Y.T.; Odorico, J.S.; Pintar, T.J.; Collins, B.H.; Pirsch, J.D.; Leverson, G.E.; Heisey, D.M.; Sollinger, H.W. Simultaneous pancreas-kidney transplantation reduces excess mortality in type 1 diabetic patients with end-stage renal disease. Kidney Int. 2000, 57, 2129–2135. [Google Scholar] [CrossRef] [PubMed]
- Reese, P.P.; Israni, A.K. Best option for transplant candidates with type 1 diabetes and a live kidney donor: A bird in the hand is worth two in the bush. Clin. J. Am. Nephrol. 2009, 4, 700–702. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, W.R.; Navarro, X.; Goetz, F.C.; Sutherland, D.E.R.; Najarian, J.S. Effects of pancreas transplantation on diabetic neuropathy. N. Engl. J. Med. 1990, 322, 1031–1037. [Google Scholar] [CrossRef] [PubMed]
- Fioretto, P.; Mauer, S.M.; Bilous, R.W.; Sutherland, D.E.R.; Steffes, M.W. Effects of pancreas transplantation on glomerular structure in insulin-dependent diabetic patients with their own kidneys. N. Engl. J. Med. 1993, 342, 1193–1196. [Google Scholar] [CrossRef]
- Robertson, R.P. Islet transplantation a decade later and strategies for filling a half-full glass. Diabetes 2010, 59, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Gaston, R.S.; Alveranga, D.Y.; Becker, B.N.; Distant, D.A.; Held, P.J.; Bragg-Gresham, J.L.; Humar, A.; Ting, A.; Wynn, J.J.; Leichtman, A.B. Kidney and pancreas transplantation. Am. J. Transplant. 2003, 3 (Suppl. s4), 64–77. [Google Scholar] [CrossRef] [PubMed]
- Boucek, P.; Saudek, F.; Pokorna, E.; Vitko, S.; Adamec, M.; Koznarova, R.; Lanska, V. Kidney transplantation in type 2 diabetic patients: A comparison with matched non-diabetic subjects. Nephrol. Dial. Transplant. 2002, 17, 1678–1683. [Google Scholar] [CrossRef] [PubMed]
- Cosio, F.G.; Hickson, L.J.; Griffin, M.D.; Stegall, M.D.; Kudva, Y. Patient survival and cardiovascular risk after kidney transplantation: The challenge of diabetes. Am. J. Transplant. 2008, 8, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, M.S.; Kuo, H.T.; Bunnapradist, S. Outcomes of simultaneous pancreas-kidney transplantation in type 2 diabetic recipients. Clin. J. Am. Soc. Nephrol. 2011, 6, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Light, J.; Tucker, M. Simultaneous pancreas kidney transplants in diabetic patients with end-stage renal disease: The 20-yr experience. Clin. Transplant. 2013, 27, E256–E263. [Google Scholar] [CrossRef] [PubMed]
- Margreiter, C.; Resch, T.; Oberhuber, R.; Aigner, F.; Maier, H.; Sucher, R.; Schneeberger, S.; Ulmer, H.; Bösmüller, C.; Margreiter, R.; et al. Combined pancreas-kidney transplantation for patients with end-stage nephropathy caused by type-2 diabetes mellitus. Transplantation 2013, 95, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, A.C.; Gralla, J. Simultaneous pancreas kidney transplant versus other kidney transplant options in patients with type 2 diabetes. Clin. J. Am. Soc. Nephrol. 2012, 7, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Mange, K.C.; Joffe, M.M.; Feldman, H.I. Effect of the use or non-use of long-term dialysis on subsequent survival of renal transplants from living donors. N. Engl. J. Med. 2001, 344, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Matas, A.J.; Ellison, M.D.; Gill, J.S.; Kausz, A.T. Preemptive kidney transplantation: The advantage and advantaged. J. Am. Soc. Nephrol. 2002, 13, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Becker, B.N.; Rush, S.H.; Dykstra, D.M.; Becker, Y.T.; Port, F.K. Preemptive transplantation for patients with diabetes-related kidney disease. Arch. Intern. Med. 2006, 166, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Pruijm, M.T.; De Fijter, H.J.W.; Doxiadis, I.J.; Vandenbroucke, J.P. Preemptive versus non-preemptive simultaneous pancreas-kidney transplantation: A single-center, long-term follow-up study. Transplantation 2006, 81, 1119–1124. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.; Wiseman, A.; Okumura, S.; Kuo, H.T.; Bunnapradist, S. Outcomes of preemptive kidney with or without subsequent pancreas transplant compared with preemptive simultaneous pancreas/kidney transplantation. Transplantation 2011, 92, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Browne, S.; Gill, J.; Dong, J.; Rose, C.; Johnston, O.; Zhang, P.; Landsberg, D.; Gill, J.S. The impact of pancreas transplantation on kidney allograft survival. Am. J. Transplant. 2011, 11, 1951–1958. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, A.C.; Huang, E.; Kamgar, M.; Bunnapradist, S. The impact of pre-transplant dialysis on simultaneous pancreas-kidney versus living donor kidney transplant outcomes. Nephrol. Dial. Transplant. 2013, 28, 1047–1058. [Google Scholar] [CrossRef] [PubMed]
- Ishani, A.; Ibrahim, H.N.; Gilbertson, D.; Collins, A.J. The impact of residual renal function on graft and patient survival rates in recipients of preemptive renal transplants. Am. J. Kidney Dis. 2003, 42, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Levin, N.W.; Kotanko, P.; Eckardt, K.U.; Kasiske, B.L.; Chazot, C.; Cheung, A.K.; Redon, J.; Wheeler, D.C.; Zoccali, C.; London, G.M. Blood pressure in chronic kidney disease stage 5D-report from a kidney disease: Improving global outcomes controversies conference. Kidney Int. 2010, 77, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Duong, U.; Mehrotra, R.; Molnar, M.Z.; Noori, N.; Kovesdy, C.P.; Nissenson, A.R.; Kalantar-Zadeh, K. Glycemic control and survival in peritoneal dialysis patients with diabetes mellitus. Clin. J. Am. Soc. Nephrol. 2011, 6, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Holdaas, H.; Holme, I.; Schmieder, R.E.; Jardine, A.G.; Zannad, F.; Norby, G.E.; Fellström, B.C.; AURORA Study Group. Rosuvastatin in diabetic hemodialysis patients. J. Am. Soc. Nephrol. 2011, 22, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Marz, W.; Genser, B.; Drechsler, C.; Krane, V.; Grammer, T.B.; Ritz, E.; Stojakovic, T.; Scharnagl, H.; Winkler, K.; Holme, I.; et al. Atorvastatin and low-density lipoprotein cholesterol in type 2 diabetes mellitus patients on hemodialysis. Clin. J. Soc. Nephrol. 2011, 6, 1316–1325. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Cano, N.J.; Budde, K.; Chazot, C.; Kovesdy, C.P.; Mak, R.H.; Mehrotra, R.; Raj, D.S.; Sehgal, A.R.; Stenvinkel, P.; et al. Diets and enteral supplements for improving outcomes in chronic renal disease. Nat. Rev. Nephrol. 2011, 7, 369–384. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Sáez, M.J.; Pascual, J. Kidney Transplantation in the Diabetic Patient. J. Clin. Med. 2015, 4, 1269-1280. https://doi.org/10.3390/jcm4061269
Pérez-Sáez MJ, Pascual J. Kidney Transplantation in the Diabetic Patient. Journal of Clinical Medicine. 2015; 4(6):1269-1280. https://doi.org/10.3390/jcm4061269
Chicago/Turabian StylePérez-Sáez, María José, and Julio Pascual. 2015. "Kidney Transplantation in the Diabetic Patient" Journal of Clinical Medicine 4, no. 6: 1269-1280. https://doi.org/10.3390/jcm4061269
APA StylePérez-Sáez, M. J., & Pascual, J. (2015). Kidney Transplantation in the Diabetic Patient. Journal of Clinical Medicine, 4(6), 1269-1280. https://doi.org/10.3390/jcm4061269