
Pattern of Investigation Reflects Risk Profile in Emergency Medical Admissions


Abstract
:1. Introduction
2. Methods
2.1. Background
2.2. Data Collection
2.3. Study Inclusion Criteria
2.4. Categorisation of Risk
2.5. Statistical Methods
3. Results
3.1. Patient Demographics

{kind=link}
| Factor | Level | Survived | Died | p-Value |
|---|---|---|---|---|
| N | 26646 | 2288 | ||
| Gender | Male | 12873 (48.3%) | 1068 (46.7%) | 0.13 |
| Female | 13773 (51.7%) | 1220 (53.3%) | ||
| Age (years), mean (SD) | 55.2 (21.4) | 75.5 (14.6) | <0.001 | |
| LOS (days), mean (SD) | 6.4 (6.2) | 9.3 (8.0) | <0.001 | |
| Illness Severity Grade | I | 1309 (5.5%) | 1 (<1%) | <0.001 |
| II | 2801 (11.8%) | 4 (0.2%) | ||
| III | 3954 (16.7%) | 23 (1.0%) | ||
| IV | 4459 (18.8%) | 53 (2.4%) | ||
| V | 4305 (18.2%) | 194 (8.8%) | ||
| VI | 6866 (29.0%) | 1930 (87.5%) | ||
| Manchester Triage | 3 | 14742 (55.3%) | 658 (28.8%) | <0.001 |
| 2 | 11551 (43.3%) | 1368 (59.8%) | ||
| 1 | 353 (1.3%) | 262 (11.5%) | ||
| Disabling Disease Score | 0 | 3663 (18.1%) | 1659 (10.3%) | <0.001 |
| 1 | 7078 (35.0%) | 3075 (19.2%) | ||
| 2 | 5953 (29.4%) | 4100 (25.6%) | ||
| 3 | 2681 (13.3%) | 3994 (24.9%) | ||
| 4 | 858 (4.2%) | 3210 (20.0%) | ||
| Charlson Index | 0 | 15392 (57.8%) | 441 (19.3%) | <0.001 |
| 1 | 6569 (24.7%) | 644 (28.1%) | ||
| 2 | 4685 (17.6%) | 1203 (52.6%) |
3.2. Resource Utilization over Time (Table 2)
| Resource | 2008 | 2011 | 2013 | p < |
|---|---|---|---|---|
| CT Brain | 28.3% | 33.5% | 30.2% | 0.001 |
| MR Brain | 5.4% | 6.8% | 9.1% | 0.001 |
| CT Abdomen | 2.5% | 2.9% | 3.0% | 0.002 |
| CT CTAP * | 2.3% | 4.9% | 5.0% | 0.001 |
| Physiotherapy | 19.4% | 20.3% | 24.9% | 0.001 |
| Dietetics | 13.5% | 13.3% | 13.5% | 0.6 |
| Speech/Language | 2.9% | 4.8% | 4.4% | 0.001 |
| Occupation Therapy | 11.5% | 11.2% | 11.7% | 0.18 |
| Social Services | 16.9% | 15.6% | 16.3% | 0.004 |
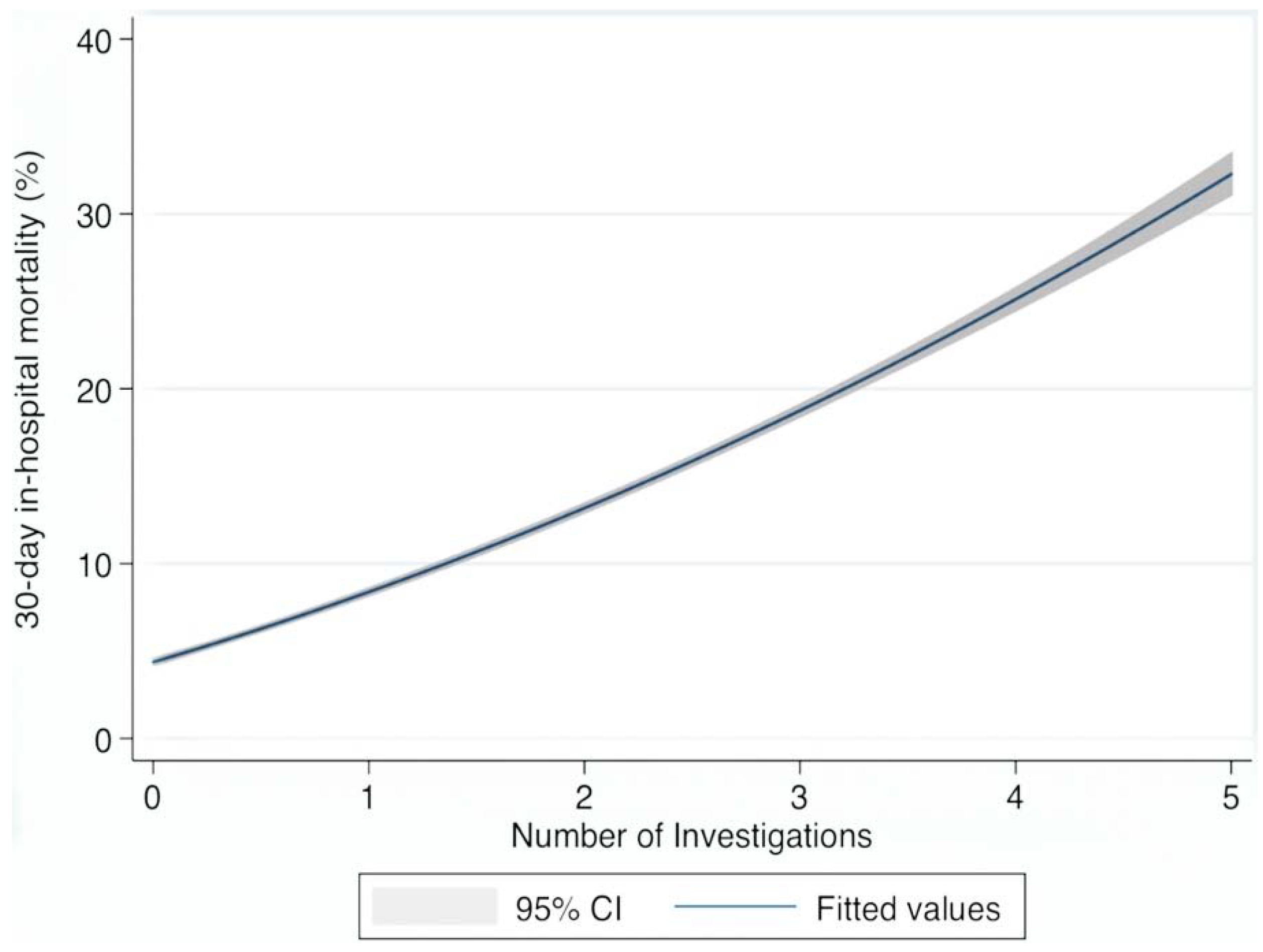
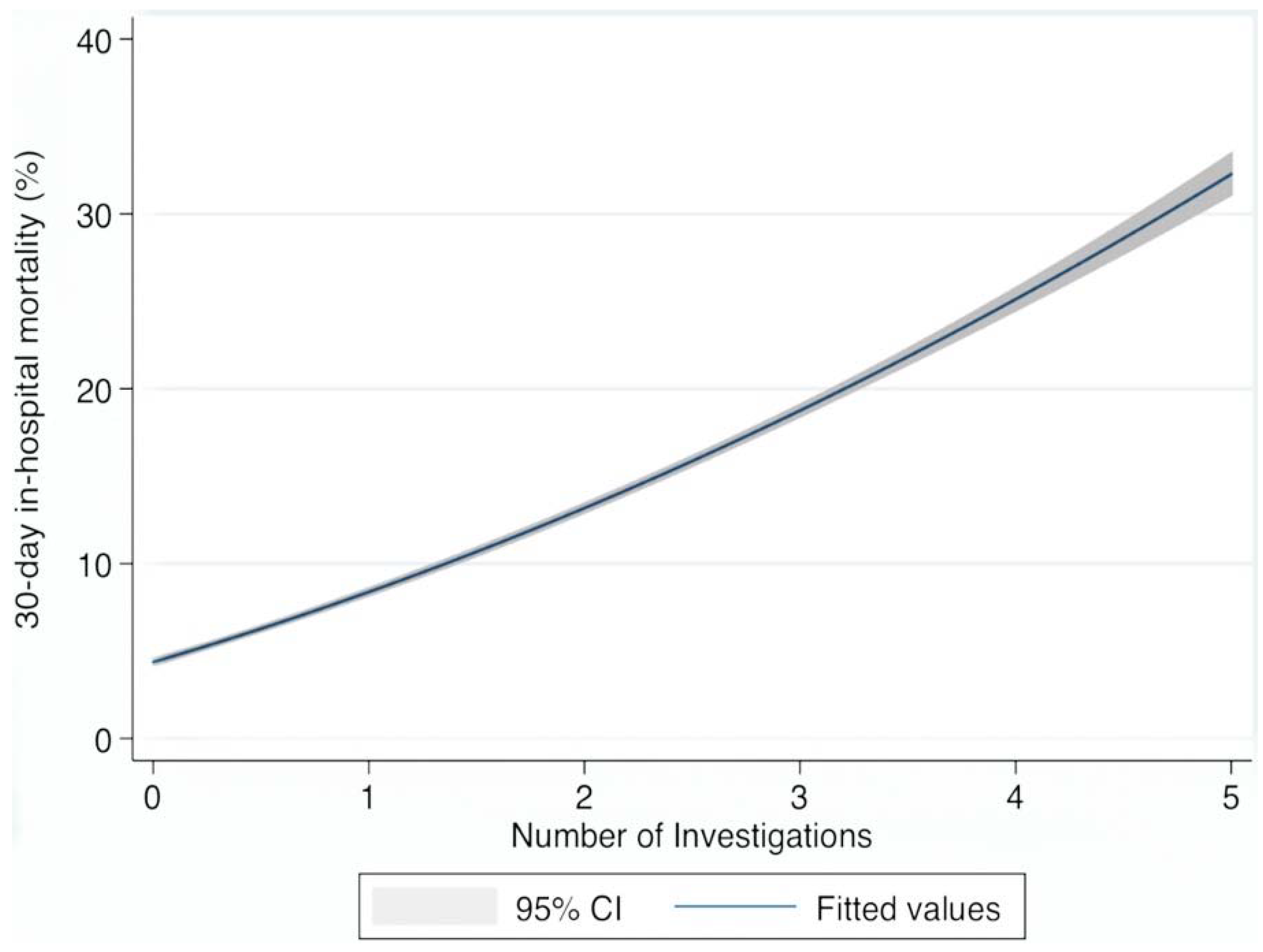
3.3. Resource Utilization as Outcome Predictors (Table 3/Table 4, Figure 1)
| Investigation | OR | 95% CI | p > |z| |
|---|---|---|---|
| CT Brain | 1.37 | 1.27, 1.50 | 0.001 |
| MR Brain | 0.54 | 0.43, 0.68 | 0.001 |
| CT Abdomen | 3.48 | 3.02, 4.02 | 0.001 |
| CT Chest/Abdo/Pelvis | 2.50 | 2.10, 2.97 | 0.001 |
| Physiotherapy | 2.57 | 2.35, 2.81 | 0.001 |
| Speech and Language | 5.29 | 4.57, 6.05 | 0.001 |
| Dietetics | 2.53 | 2.27, 2.82 | 0.001 |
| Occupational Therapy | 2.65 | 2.38, 2.94 | 0.001 |
| Social Services | 1.65 | 1.48, 1.83 | 0.001 |
| Investigation | OR | 95% CI | p > |z| |
|---|---|---|---|
| Acute Illness Severity | 3.41 | 3.11, 3.74 | 0.001 |
| Charlson Index | 1.56 | 1.45, 1.67 | 0.001 |
| Debilitating Disease | 1.29 | 1.22, 1.37 | 0.001 |
| Sepsis Status | 2.06 | 1.91, 2.23 | 0.001 |
| Manchester Triage Category | 2.71 | 2.47, 2.98 | 0.001 |
| CT Brain | 1.82 | 1.63, 2.04 | 0.001 |
| MR Brain | 0.63 | 0.48, 0.83 | 0.001 |
| CT Abdomen | 2.80 | 2.35, 3.35 | 0.001 |
| CT Chest/Abdo/Pelvis | 1.53 | 1.25, 1.87 | 0.001 |
| Physiotherapy | 0.99 | 0.88, 1.13 | 0.98 |
| Speech and Language | 1.93 | 1.62, 2.29 | 0.001 |
| Dietetics | 1.03 | 0.09, 1.18 | 0.66 |
| Occupational Therapy | 1.12 | 0.96, 1.31 | 0.15 |
| Social Services | 0.71 | 0.62, 0.82 | 0.001 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Litvak, E.; Bisognano, M. More patients, less payment: Increasing hospital efficiency in the aftermath of health reform. Health Aff. (Millwood) 2011, 30, 76–80. [Google Scholar] [CrossRef]
- Moses, H.I.; Matheson, D.; Dorsey, E.; George, B.; Sadoff, D.; Yoshimura, S. The anatomy of health care in the United States. JAMA 2013, 18, 1947–1963. [Google Scholar] [CrossRef]
- Curfman, G.; Morrissey, S.; Drazen, J. High-Value Health Care—A Sustainable Proposition. N. Engl. J. Med. 2013, 369, 1163–1164. [Google Scholar] [CrossRef]
- Iglehart, J.K. The new era of medical imaging—Progress and pitfalls. N. Engl. J. Med. 2006, 354, 2822–2828. [Google Scholar] [CrossRef] [PubMed]
- Upponi, S.; Shaw, A.S. Radiology provision in the United kingdom: An overview. J. Am. Coll. Radiol. JACR 2010, 7, 565–572. [Google Scholar] [CrossRef]
- Lee, D.W.; Foster, D.A. The association between hospital outcomes and diagnostic imaging: Early findings. J. Am. Coll. Radiol. JACR 2009, 6, 780–785. [Google Scholar] [CrossRef]
- Gilbert, J.W.; Johnson, K.M.; Larkin, G.L.; Moore, C.L. Atraumatic headache in US emergency departments: Recent trends in CT/MRI utilisation and factors associated with severe intracranial pathology. Emerg. Med. J. EMJ 2012, 29, 576–581. [Google Scholar] [CrossRef]
- Korley, F.K.; Pham, J.C.; Kirsch, T.D. Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998–2007. JAMA 2010, 304, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Rosen, M.P.; Oake, N.; Forster, A.J.; Goelman, A.; Levy, F. The effect of imaging capacity on the imaging workup of patients with stroke: A preliminary case for a cross-country comparison. J. Am. Coll. Radiol. JACR 2011, 8. [Google Scholar] [CrossRef]
- Andersen, R.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. Milbank Mem. Fund Q. Health Soc. 1973, 51, 95–124. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, U.E. Does the Aging of the Population Really Drive the Demand for Health Care? Health Aff. 2003, 22, 27–39. [Google Scholar] [CrossRef]
- Strunk, B.C.; Ginsburg, P.B.; Banker, M.I. The Effect of Population Aging on Future Hospital Demand. Health Aff. (Millwood) 2006, 25. [Google Scholar] [CrossRef]
- Moloney, E.D.; Smith, D.; O’Riordan, D.; Silke, B. Impact of an acute medical admission units on length of hospital stay, and emergency department “wait times”. QJM 2005, 98, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Rooney, T.; Moloney, E.D.; Bennett, K.; O’Riordan, D.; Silke, B. Impact of an acute medical admission unit on hospital mortality: A 5-year prospective study. QJM 2008, 101, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; O’Riordan, D.; Silke, B. Long-term outcome of an AMAU—A decade’s experience. QJM 2014, 107, 43–49. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, R.; Allwright, S.; Barry, J.; Kelly, A.; Teljeur, C. Using HIPE data as a research and planning tool: Limitations and opportunities. Ir. J. Med. Sci. 2005, 174, 40–45. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, A.; Colgan, M.P.; McGuigan, C.; Smyth, F.; Haider, N.; O’Neill, S.; Moore, D.; Madhavan, P. A critical evaluation of HIPE data. Ir. Med. J. 2012, 105, 21–23. [Google Scholar] [PubMed]
- O’Sullivan, E.; Callely, E.; O’Riordan, D.; Bennett, K.; Silke, B. Predicting outcomes in emergency medical admissions—Role of laboratory data and co-morbidity. Acute Med. 2012, 2, 59–65. [Google Scholar]
- Silke, B.; Kellett, J.; Rooney, T.; Bennett, K.; O’Riordan, D. An improved medical admissions risk system using multivariable fractional polynomial logistic regression modelling. QJM 2010, 103, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Mikulich, O.; Callaly, E.; Bennett, K.; Silke, B.; O’Riordan, D. The increased mortality associated with a weekend emergency admission is due to increased illness severity and altered case-mix. Acute Med. 2011, 10, 181–186. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Chotirmall, S.H.; Picardo, S.; Lyons, J.; D’Alton, M.; O’Riordan, D.; Silke, B. Disabling disease codes predict worse outcomes for acute medical admissions. Intern. Med. J. 2014, 44, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Mackway-Jones, K.; Marsden, J.; Windle, J. Emergency Triage, 2nd ed.; Group, M.T., Ed.; Blackwell Publishing Ltd.: London, UK, 2006. [Google Scholar]
- Chotirmall, S.H.; Callaly, E.; Lyons, J.; O’Connell, B.; Kelleher, M.; Byrne, D.; O’Riordan, D.; Silke, B. Blood cultures in emergency medical admissions: A key patient cohort. Eur. J. Emerg. Med. 2014. [Google Scholar] [CrossRef]
- Jayadevappa, R.; Chhatre, S.; Weiner, M.; Raziano, D.B. Health resource utilization and medical care cost of acute care elderly unit patients. Value Health 2006, 9, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Dodel, R.C.; Haacke, C.; Zamzow, K.; Paweilik, S.; Spottke, A.; Rethfeldt, M.; Siebert, U.; Oertel, W.H.; Schöffski, O.; Back, T. Resource utilization and costs of stroke unit care in Germany. Value Health 2004, 7, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Ni Mhurchu, C.; Brown, P.M.; Carter, K. Stroke rehabilitation services to accelerate hospital discharge and provide home-based care: An overview and cost analysis. Pharmacoeconomics 2002, 20, 537–552. [Google Scholar] [CrossRef] [PubMed]
- Kalant, N.; Berlinguet, M.; Diodati, J.G.; Dragatakis, L.; Marcotte, F. How valid are utilization review tools in assessing appropriate use of acute care beds? CMAJ 2000, 162, 1809–1813. [Google Scholar] [PubMed]
- (NZHTA) NZHTACH. Acute medical admissions—A critical appraisal of the literature Christchurch, New Zealand 1998. Available online: http://www.otago.ac.nz/christchurch/otago014024.pdf (accessed on 1 November 2014).
- Barry, M.; Bennett, K.; Brick, A.; Morgenroth, E.; Normand, C.; O’Reilly, J.; Thomas, S.; Tilson, L.; Wiley, M.; Wren, M.-A. Projecting the Impact of Demographic Change on the Demand for and Delivery of Health Care in Ireland Dublin: The Economic and Social Reseach Institute 2009. Available online: http://www.hrb.ie/uploads/tx_hrbpublications/Final_Report.ESRI.pdf (accessed on 1 November 2014).
- HSE and Department of Health to Appear before PAC 2014. Available online: http://www.oireachtas.ie/parliament/mediazone/pressreleases/name-22660-en.html (accessed on 1 November 2014).
- Cournane, S.; Creagh, D.; O’Hare, N.; Sheehy, N.; Silke, B. MRI in Acutely Ill Medical Patients in an Irish Hospital: Influence on Outcomes and Length of Hospital Stay. J. Am. Coll. Radiol. 2014, 11, 698–702. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cournane, S.; Byrne, D.; O'Riordan, D.; Sheehy, N.; Silke, B. Pattern of Investigation Reflects Risk Profile in Emergency Medical Admissions. J. Clin. Med. 2015, 4, 1113-1125. https://doi.org/10.3390/jcm4051113
Cournane S, Byrne D, O'Riordan D, Sheehy N, Silke B. Pattern of Investigation Reflects Risk Profile in Emergency Medical Admissions. Journal of Clinical Medicine. 2015; 4(5):1113-1125. https://doi.org/10.3390/jcm4051113
Chicago/Turabian StyleCournane, Seán, Declan Byrne, Deirdre O'Riordan, Niall Sheehy, and Bernard Silke. 2015. "Pattern of Investigation Reflects Risk Profile in Emergency Medical Admissions" Journal of Clinical Medicine 4, no. 5: 1113-1125. https://doi.org/10.3390/jcm4051113
APA StyleCournane, S., Byrne, D., O'Riordan, D., Sheehy, N., & Silke, B. (2015). Pattern of Investigation Reflects Risk Profile in Emergency Medical Admissions. Journal of Clinical Medicine, 4(5), 1113-1125. https://doi.org/10.3390/jcm4051113