

A Multicenter Study by the DENO Research Group on the Use of Denosumab in Giant-Cell Tumors of the Bone
 , , , add
Show full author list
, , , add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Neoadjuvant Treatment
3.2. Adjuvant Treatment
3.3. Recurrence in Curettage: Neoadjuvant vs. Adjuvant Treatment
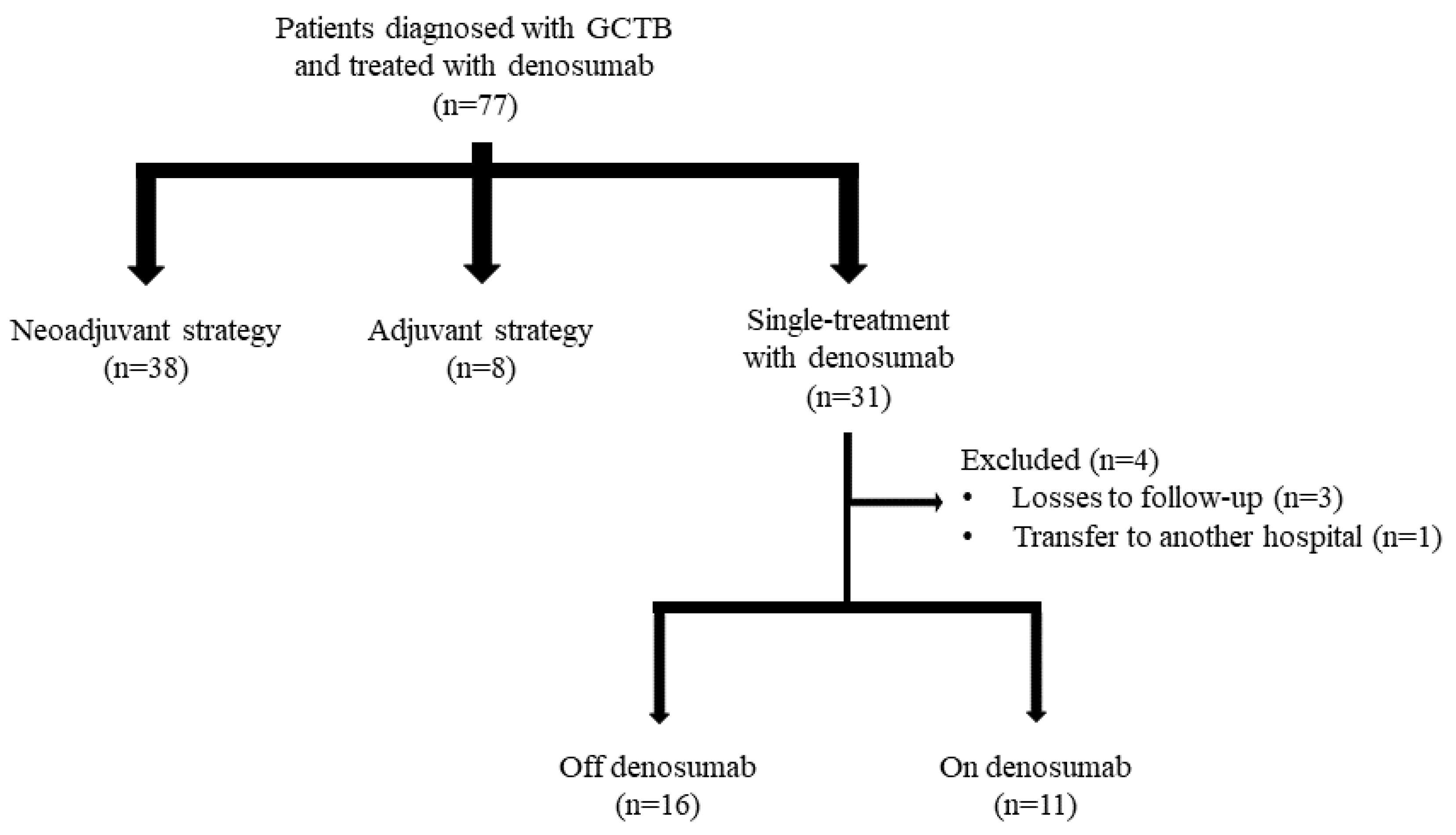
3.4. Single Treatment
3.5. Toxicity
4. Discussion
4.1. Treatment of GCTB with Denosumab
4.2. Neoadjuvant Treatment
4.3. Adjuvant Treatment
4.4. Single-Treatment
4.5. Toxicity
4.6. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AEMPS | Spanish Medicines Agency |
| CTCAE | Common Terminology Criteria for Adverse Events |
| GCTB | Giant-cell tumors of the bone |
| ICDS | Inverse Choi Density/Size |
| LIETAL | Spanish Musculoskeletal Tumors Research Consortium |
| RANKL | Receptor activator of nuclear factor kappa-B ligand |
| SECOT | Spanish Society of Orthopedics and Trauma Surgery |
References
- van der Heijden, L.; Dijkstra, P.D.S.; Blay, J.-Y.; Gelderblom, H. Giant Cell Tumour of Bone in the Denosumab Era. Eur. J. Cancer 2017, 77, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.A.; Puri, A. The Current Standing on the Use of Denosumab in Giant Cell Tumour of the Bone. J. Orthop. Surg. 2020, 28, 230949902097975. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Alonso, G.; Mellado-Romero, M.; Shemesh, S.; Ramos-Pascua, L.; Pretell-Mazzini, J. Denosumab Treatment for Giant-Cell Tumor of Bone: A Systematic Review of the Literature. Arch. Orthop. Trauma Surg. 2019, 139, 1339–1349. [Google Scholar] [CrossRef] [PubMed]
- Medellin, M.R.; Fujiwara, T.; Tillman, R.M.; Jeys, L.M.; Gregory, J.; Stevenson, J.D.; Parry, M.; Abudu, A. Prognostic Factors for Local Recurrence in Extremity-Located Giant Cell Tumours of Bone with Pathological Fracture. Bone Jt. J. 2018, 100-B, 1626–1632. [Google Scholar] [CrossRef]
- Chen, X.; Li, H.; Zhu, S.; Wang, Y.; Qian, W. Pre-Operative Denosumab Is Associated with Higher Risk of Local Recurrence in Giant Cell Tumor of Bone: A Systematic Review and Meta-Analysis. BMC Musculoskelet. Disord. 2020, 21, 256. [Google Scholar] [CrossRef]
- Palmerini, E.; Staals, E.L.; Jones, L.B.; Donati, D.M.; Longhi, A.; Randall, R.L. Role of (Neo)Adjuvant Denosumab for Giant Cell Tumor of Bone. Curr. Treat. Options Oncol. 2020, 21, 68. [Google Scholar] [CrossRef]
- Chakarun, C.J.; Forrester, D.M.; Gottsegen, C.J.; Patel, D.B.; White, E.A.; Matcuk, G.R. Giant Cell Tumor of Bone: Review, Mimics, and New Developments in Treatment. RadioGraphics 2013, 33, 197–211. [Google Scholar] [CrossRef]
- Nasca, V.; Frezza, A.M.; Morosi, C.; Buonomenna, C.; Parafioriti, A.; Zappalà, G.; Bini, F.; Casali, P.G.; Loppini, M.; Stacchiotti, S. Rechallenge of Denosumab in Advanced Giant Cell Tumor of the Bone after Atypical Femur Fracture: A Case Report and Review of Literature. Front. Oncol. 2022, 12, 953149. [Google Scholar] [CrossRef]
- Mattei, T.A.; Ramos, E.; Rehman, A.A.; Shaw, A.; Patel, S.R.; Mendel, E. Sustained Long-Term Complete Regression of a Giant Cell Tumor of the Spine after Treatment with Denosumab. Spine J. 2014, 14, e15–e21. [Google Scholar] [CrossRef]
- Xará-Leite, F.; Coutinho, L.; Fleming, C.; Magalhães, M.; Oliveira, V.; Rodrigues-Pinto, R.; Cardoso, P. Can Denosumab Cure Giant Cell Tumors of the Spine? A Case Report and Literature Review. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 19–23. [Google Scholar] [CrossRef]
- Bukata, S.V.; Blay, J.-Y.; Rutkowski, P.; Skubitz, K.; Henshaw, R.; Seeger, L.; Dai, T.; Jandial, D.; Chawla, S. Denosumab Treatment for Giant Cell Tumor of the Spine Including the Sacrum. Spine 2021, 46, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, E.; Chawla, N.S.; Ferrari, S.; Sudan, M.; Picci, P.; Marchesi, E.; Leopardi, M.P.; Syed, I.; Sankhala, K.K.; Parthasarathy, P.; et al. Denosumab in Advanced/Unresectable Giant-Cell Tumour of Bone (GCTB): For How Long? Eur. J. Cancer 2017, 76, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Campanacci, M.; Baldini, N.; Boriani, S.; Sudanese, A. Giant-Cell Tumor of Bone. J. Bone Jt. Surg. Am. 1987, 69, 106–114. [Google Scholar] [CrossRef]
- Choi, H.; Charnsangavej, C.; Faria, S.C.; Macapinlac, H.A.; Burgess, M.A.; Patel, S.R.; Chen, L.L.; Podoloff, D.A.; Benjamin, R.S. Correlation of Computed Tomography and Positron Emission Tomography in Patients With Metastatic Gastrointestinal Stromal Tumor Treated at a Single Institution with Imatinib Mesylate: Proposal of New Computed Tomography Response Criteria. J. Clin. Oncol. 2007, 25, 1753–1759. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE); Version 5; US Department of Health and Human Services: Washington, DC, USA, 2017. [Google Scholar]
- Sullivan, G.M.; Feinn, R. Using Effect Size—Or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- Puri, A.; Gulia, A.; Hegde, P.; Verma, V.; Rekhi, B. Neoadjuvant Denosumab: Its Role and Results in Operable Cases of Giant Cell Tumour of Bone. Bone Jt. J. 2019, 101-B, 170–177. [Google Scholar] [CrossRef]
- Gaston, C.L.; Grimer, R.J.; Parry, M.; Stacchiotti, S.; Dei Tos, A.P.; Gelderblom, H.; Ferrari, S.; Baldi, G.G.; Jones, R.L.; Chawla, S.; et al. Current Status and Unanswered Questions on the Use of Denosumab in Giant Cell Tumor of Bone. Clin. Sarcoma Res. 2016, 6, 15. [Google Scholar] [CrossRef]
- Agarwal, M.G.; Gundavda, M.K.; Gupta, R.; Reddy, R. Does Denosumab Change the Giant Cell Tumor Treatment Strategy? Lessons Learned From Early Experience. Clin. Orthop. Relat. Res. 2018, 476, 1773–1782. [Google Scholar] [CrossRef]
- Huang, Y.; Xu, M.; Wang, B.; Zhao, Z.; Lin, T.; Huang, G.; Yin, J.; Xie, X.; Shen, J.; Zou, C. Preoperative Denosumab Treatment in Patients with Giant Cell Bone Tumors in Limbs: A Retrospective Study Using Propensity Score Matching. Cancer Med. 2023, 12, 12041–12049. [Google Scholar] [CrossRef]
- Sun, Z.; Wu, Z.; Zhang, L.; Jia, Q.; Zhou, Z.; Xiao, J. Association between Preoperative Denosumab and the Risk of Local Recurrence in Patients with Giant Cell Tumor of Bone: A Meta-Analysis and Systematic Review. J. Cancer Res. Ther. 2023, 19, 25–33. [Google Scholar] [CrossRef]
- Chawla, S.; Blay, J.-Y.; Rutkowski, P.; Le Cesne, A.; Reichardt, P.; Gelderblom, H.; Grimer, R.J.; Choy, E.; Skubitz, K.; Seeger, L.; et al. Denosumab in Patients with Giant-Cell Tumour of Bone: A Multicentre, Open-Label, Phase 2 Study. Lancet Oncol. 2019, 20, 1719–1729. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Yang, Y.; Wong, K.C.; Huang, Z.; Ding, Y.; Zhang, W. Giant Cell Tumour of the Bone Treated with Denosumab: How Has the Blood Supply and Oncological Prognosis of the Tumour Changed? J. Orthop. Translat. 2019, 18, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, S.; Tanaka, Y.; Mavrogenis, A.F.; Kido, A.; Kawaguchi, M.; Errani, C. Is Treatment with Denosumab Associated with Local Recurrence in Patients with Giant Cell Tumor of Bone Treated with Curettage? A Systematic Review. Clin. Orthop. Relat. Res. 2020, 478, 1076–1085. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Gaston, L.; Borkowska, A.; Stacchiotti, S.; Gelderblom, H.; Baldi, G.G.; Palmerini, E.; Casali, P.; Gronchi, A.; Parry, M.; et al. Denosumab Treatment of Inoperable or Locally Advanced Giant Cell Tumor of Bone—Multicenter Analysis Outside Clinical Trial. Eur. J. Surg. Oncol. 2018, 44, 1384–1390. [Google Scholar] [CrossRef]
- Liang, H.; Liu, X.; Yang, Y.; Guo, W.; Yang, R.; Tang, X.; Yan, T.; Li, Y.; Tang, S.; Li, D.; et al. Ultra-Short Course of Neo-Adjuvant Denosumab for Nerve-Sparing Surgery for Giant Cell Tumor of Bone in Sacrum. Spine 2022, 47, 691–701. [Google Scholar] [CrossRef]
- Errani, C.; Tsukamoto, S.; Leone, G.; Righi, A.; Akahane, M.; Tanaka, Y.; Donati, D.M. Denosumab May Increase the Risk of Local Recurrence in Patients with Giant-Cell Tumor of Bone Treated with Curettage. J. Bone Jt. Surg. 2018, 100, 496–504. [Google Scholar] [CrossRef]
- Müller, D.A.; Beltrami, G.; Scoccianti, G.; Campanacci, D.A.; Franchi, A.; Capanna, R. Risks and Benefits of Combining Denosumab and Surgery in Giant Cell Tumor of Bone—A Case Series. World J. Surg. Oncol. 2016, 14, 281. [Google Scholar] [CrossRef]
- Jiang, C.Y.; Zhao, L.; Schuetze, S.M.; Chugh, R. Giant Cell Tumor of Bone: Effect of Longer Dosing Intervals of Denosumab on Tumor Control and Bone-Related Complications. Oncologist 2022, 27, 595–599. [Google Scholar] [CrossRef]
- Lim, C.Y.; Liu, X.; He, F.; Liang, H.; Yang, Y.; Ji, T.; Yang, R.; Guo, W. Retrospective Cohort Study of 68 Sacral Giant Cell Tumours Treated with Nerve-Sparing Surgery and Evaluation on Therapeutic Benefits of Denosumab Therapy. Bone Jt. J. 2020, 102-B, 177–185. [Google Scholar] [CrossRef]
- Akyıldız, A.; Ismayılov, R.; Güven, D.; Chalabiyev, E.; Abdurrahimli, N.; Aksoy, S. Adjuvant Denosumab Treatment in Patients with Resectable High-Risk Giant Cell Tumor of Bone. Anatol. Curr. Med. J. 2024, 6, 225–228. [Google Scholar] [CrossRef]
- Deveci, M.A.; Paydaş, S.; Gönlüşen, G.; Özkan, C.; Biçer, Ö.S.; Tekin, M. Clinical and Pathological Results of Denosumab Treatment for Giant Cell Tumors of Bone: Prospective Study of 14 Cases. Acta Orthop. Traumatol. Turc. 2017, 51, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ueda, T.; Morioka, H.; Nishida, Y.; Kakunaga, S.; Tsuchiya, H.; Matsumoto, Y.; Asami, Y.; Inoue, T.; Yoneda, T. Objective Tumor Response to Denosumab in Patients with Giant Cell Tumor of Bone: A Multicenter Phase II Trial. Ann. Oncol. 2015, 26, 2149–2154. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, A.; Simeone, N.; Guzzo, M.; Maniezzo, M.; Collini, P.; Morosi, C.; Greco, F.G.; Frezza, A.; Casali, P.G.; Stacchiotti, S. Rechallenge of Denosumab in Jaw Osteonecrosis of Patients with Unresectable Giant Cell Tumour of Bone: A Case Series Analysis and Literature Review. ESMO Open 2020, 5, e000663. [Google Scholar] [CrossRef]
- Rodríguez, M.A.; Casales, N.; Silveri, C.; Cardozo, J.; Filomeno, P.; Francescoli, L. Denosumab, Tratamiento Alternativo En Tumor Óseo de Células Gigantes. Rev. Méd. Urug. 2017, 33, 152–155. [Google Scholar]
- Uday, S.; Gaston, C.L.; Rogers, L.; Parry, M.; Joffe, J.; Pearson, J.; Sutton, D.; Grimer, R.; Högler, W. Osteonecrosis of the Jaw and Rebound Hypercalcemia in Young People Treated With Denosumab for Giant Cell Tumor of Bone. J. Clin. Endocrinol. Metab. 2018, 103, 596–603. [Google Scholar] [CrossRef]
- de la Calva, C.; Angulo, M.; González-Rojo, P.; Peiró, A.; Machado, P.; Cebrián, J.L.; García-Maroto, R.; Valcárcel, A.; Puertas, P.; Valero-Cifuentes, G.; et al. Do Unresectable Giant Cell Tumors of Bone Treated With Denosumab Progress After Discontinuation of Treatment? Cancer Rep. 2025, 8, e70117. [Google Scholar] [CrossRef]
- Boquete-Castro, A.; Gómez-Moreno, G.; Calvo-Guirado, J.L.; Aguilar-Salvatierra, A.; Delgado-Ruiz, R.A. Denosumab and Osteonecrosis of the Jaw. A Systematic Analysis of Events Reported in Clinical Trials. Clin. Oral Implant. Res. 2016, 27, 367–375. [Google Scholar] [CrossRef]

{kind=link}
| Neoadjuvant Treatment | Adjuvant Treatment | Single Treatment | |||
|---|---|---|---|---|---|
| Sex | |||||
| Male | 12 (31.6%) | 1 (12.5%) | 12 (44.4%) | ||
| Female | 26 (68.4%) | 7 (87.5%) | 19 (70.4%) | ||
| Age (years) | 38.0 ± 13.7 [16–64] | 26.0 ± 7.2 [15–39] | 39.5 ± 13.4 [18–63] | ||
| Origin | |||||
| Primary | 32 (84.2%) | 7 (87.5%) | 16 (59.3%) | ||
| Recurrence | 6 (15.8%) | 1 (12.5%) | 11 (40.7%) | ||
| Location of the tumor | |||||
| Axial skeleton | - | 1 (12.5%) | 5 (18.5%) | ||
| Proximal humerus | - | 1 (12.5%) | - | ||
| Distal humerus | 1 (2.6%) | - | - | ||
| Distal radius | 6 (15.8%) | - | 3 (11.1%) | ||
| Distal ulna | 1 (2.6%) | 2 (25.0%) | - | ||
| Pelvis | - | 1 (12.5%) | 11 (40.7%) | ||
| Distal femur | 14 (36.8%) | - | 2 (7.4%) | ||
| Proximal femur | 2 (5.3%) | - | - | ||
| Proximal tibia | 7 (18.4%) | 1 (12.5%) | 3 (11.1%) | ||
| Distal tibia | 1 (2.6%) | - | - | ||
| Hand | |||||
| Phalanges | 3 (7.9%) | - | - | ||
| Foot | |||||
| Talus | 1 (2.6%) | 2 (25.0%) | 2 (7.4%) | ||
| Cuneiforms | - | - | 1 (3.7%) | ||
| Scaphoids | 1 (2.6%) | - | - | ||
| Campanacci’s radiological classification | |||||
| I | - | - | 1 (3.7%) | ||
| II | 17 (44.7%) | 1 (12.5%) | 14 (51.9%) | ||
| II with fracture | 3 (7.9%) | 2 (25.0%) | 2 (7.4%) | ||
| III | 15 (39.5%) | 5 (62.5%) | 10 (37.0%) | ||
| Unknown | 3 (7.9%) | - | - | ||
| Treatment Strategy | Median | Range | |
|---|---|---|---|
| Neoadjuvant treatment | 6.1 | 0.5–19.8 | |
| Reintroduction after curettage | 4.8 | 0.9–7.5 | |
| Adjuvant treatment | |||
| Off-denosumab | 15.3 | 3.1–19.3 | |
| On-denosumab | 12.8 | 0.4–78.3 | |
| Single treatment | |||
| Off-denosumab | 34.2 | 5.0–83.2 | |
| On-denosumab | 51.8 | 14.6–130.7 | |
| Neoadjuvant Treatment | Adjuvant Treatment | Single Treatment | |
|---|---|---|---|
| Jaw osteonecrosis | - | - | 5 (18.5%) |
| Pain in the limbs | 8 (21.1%) | 1 (12.5%) | 5 (18.5%) |
| Backache | 3 (7.9%) | - | 1 (3.7%) |
| Muscle weakness | 7 (18.4%) | 1 (12.5%) | 3 (11.1%) |
| Diarrhea | - | - | 1 (3.7%) |
| Nausea | 3 (7.9%) | - | - |
| Fatigue | 6 (15.8%) | 3 (37.5%) | 4 (14.8%) |
| Headache | 2 (5.3%) | 1 (12.5%) | 1 (3.7%) |
| Hypocalcemia | 1 (2.6%) | - | - |
| Respiratory failure | 1 (2.6%) | - | - |
| Atypical fracture | 1 (2.6%) | - | - |
| Leg cramps | - | - | 1 (3.7%) |
| Myalgia | - | - | 1 (3.7%) |
| Anemia | - | - | 1 (3.7%) |
| Hypertransaminasemia | - | - | 1 (3.7%) |
| Dizziness | 1 (2.6%) | - | - |
| Asthenia | 1 (2.6%) | - | 1 (3.7%) |
| Neutropenia | - | - | 1 (3.7%) |
| Insomnia | - | - | 1 (3.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DENO Research Group; Calva, C.d.l.; Angulo, M.; González-Rojo, P.; Peiró, A.; Machado, P.; Cebrián, J.L.; García-Maroto, R.; Valcárcel, A.; Puertas, P.; et al. A Multicenter Study by the DENO Research Group on the Use of Denosumab in Giant-Cell Tumors of the Bone. J. Clin. Med. 2025, 14, 3242. https://doi.org/10.3390/jcm14093242
DENO Research Group, Calva Cdl, Angulo M, González-Rojo P, Peiró A, Machado P, Cebrián JL, García-Maroto R, Valcárcel A, Puertas P, et al. A Multicenter Study by the DENO Research Group on the Use of Denosumab in Giant-Cell Tumors of the Bone. Journal of Clinical Medicine. 2025; 14(9):3242. https://doi.org/10.3390/jcm14093242
Chicago/Turabian StyleDENO Research Group, Carolina de la Calva, Manuel Angulo, Paula González-Rojo, Ana Peiró, Pau Machado, Juan Luis Cebrián, Roberto García-Maroto, Antonio Valcárcel, Pablo Puertas, and et al. 2025. "A Multicenter Study by the DENO Research Group on the Use of Denosumab in Giant-Cell Tumors of the Bone" Journal of Clinical Medicine 14, no. 9: 3242. https://doi.org/10.3390/jcm14093242
APA StyleDENO Research Group, Calva, C. d. l., Angulo, M., González-Rojo, P., Peiró, A., Machado, P., Cebrián, J. L., García-Maroto, R., Valcárcel, A., Puertas, P., Valero-Cifuentes, G., Pablos, Ó., Maireles, M., Fontalva, M. L., Chaves, I., Orce, A., Coll-Mesa, L., Pérez, I., González, F., ... Gracia, I. (2025). A Multicenter Study by the DENO Research Group on the Use of Denosumab in Giant-Cell Tumors of the Bone. Journal of Clinical Medicine, 14(9), 3242. https://doi.org/10.3390/jcm14093242