
Muscle Activation and Mobility After Robotic Total Knee Arthroplasty: Insights from Early Postoperative Recovery


 , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Surgical Procedure
2.3. Postoperative Rehabilitation Protocol
2.4. Outcome Measures
2.5. Quadriceps Muscle Activity
- Vastus Lateralis: Positioned longitudinally over the muscle belly, approximately two-thirds of the distance between the anterior superior iliac spine and the lateral border of the patella.
2.6. Statistical Analysis
3. Results
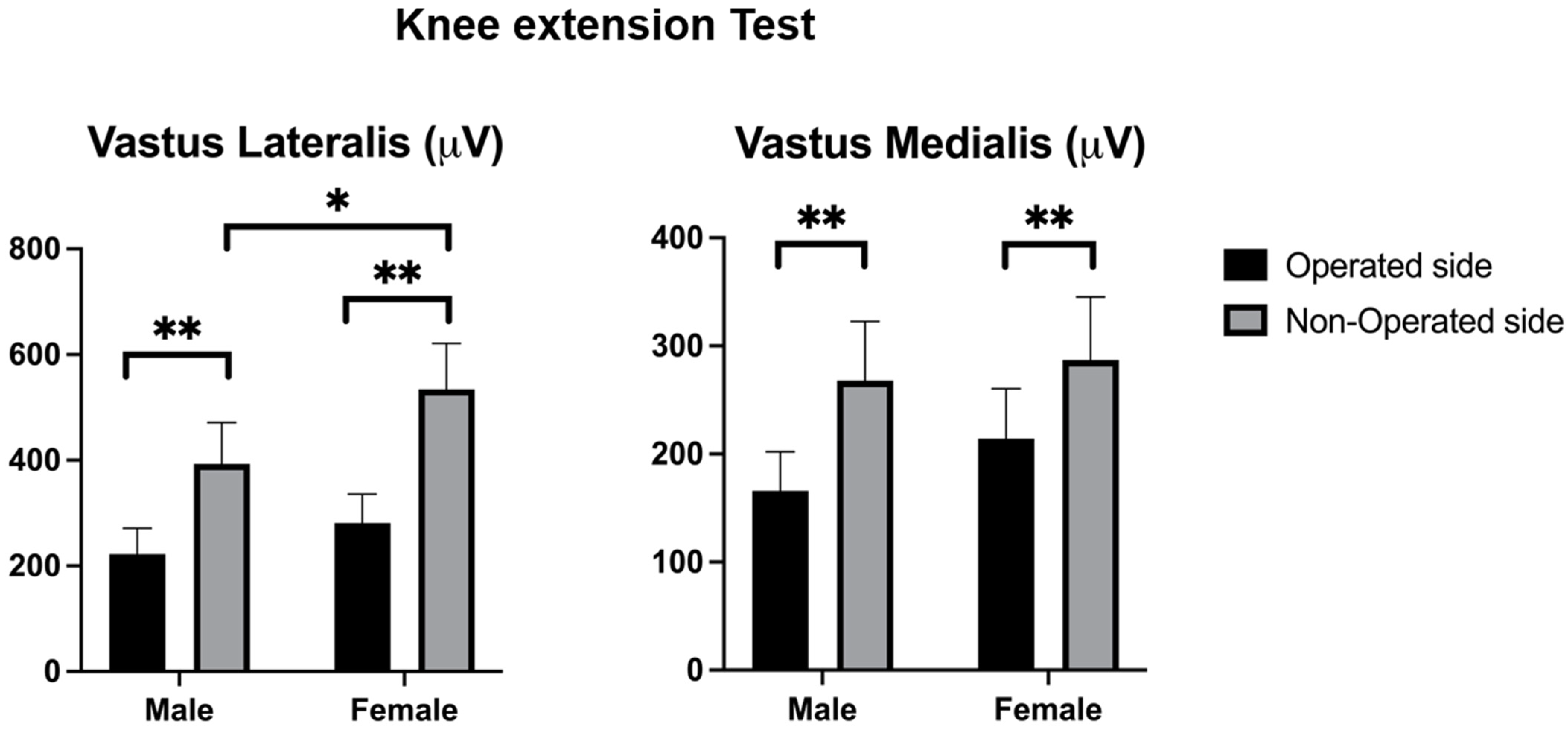
3.1. Knee Extension Test
3.2. 4-m Walking Test
3.3. Pairwise Comparisons
4. Discussion
4.1. Sex-Based Differences in Recovery
4.2. Clinical Implications
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. eClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef]
- Steinhaus, M.E.; Christ, A.B.; Cross, M.B. Total Knee Arthroplasty for Knee Osteoarthritis: Support for a Foregone Conclusion? HSS J. 2017, 13, 207–210. [Google Scholar] [CrossRef]
- St Mart, J.P.; Goh, E.L. The current state of robotics in total knee arthroplasty. EFORT Open Rev. 2021, 6, 270–279. [Google Scholar] [CrossRef]
- Xing, P.; Qu, J.; Feng, S.; Guo, J.; Huang, T. Comparison of the efficacy of robot-assisted total knee arthroplasty in patients with knee osteoarthritis with varying severity deformity. J. Orthop. Surg. 2024, 19, 872. [Google Scholar] [CrossRef]
- Pailhé, R. Total knee arthroplasty: Latest robotics implantation techniques. Orthop. Traumatol. Surg. Res. 2021, 107, 102780. [Google Scholar] [CrossRef]
- Klodmann, J.; Schlenk, C.; Hellings-Kuß, A.; Bahls, T.; Unterhinninghofen, R.; Albu-Schäffer, A.; Hirzinger, G. An Introduction to Robotically Assisted Surgical Systems: Current Developments and Focus Areas of Research. Curr. Robot. Rep. 2021, 2, 321–332. [Google Scholar] [CrossRef]
- Boonen, B.; Schotanus, M.G.M.; Kerens, B.; Hulsmans, F.J.; Tuinebreijer, W.E.; Kort, N.P. Patient-specific positioning guides for total knee arthroplasty: No significant difference between final component alignment and pre-operative digital plan except for tibial rotation. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2809–2817. [Google Scholar] [CrossRef]
- Song, E.K.; Seon, J.K.; Yim, J.H.; Netravali, N.A.; Bargar, W.L. Robotic-assisted TKA Reduces Postoperative Alignment Outliers and Improves Gap Balance Compared to Conventional TKA. Clin. Orthop. Relat. Res. 2013, 471, 118–126. [Google Scholar] [CrossRef]
- Masilamani, A.B.S.; Jayakumar, T.; Mulpur, P.; Gandhi, V.; Kikkuri, R.R.; Reddy, A.V.G. Functional alignment is associated with increased incidence of pre-balance, reduced soft-tissue release, and post-operative pain compared to mechanical alignment in patients undergoing simultaneous bilateral robotic-assisted TKA. J. Robot. Surg. 2023, 17, 2919–2927. [Google Scholar] [CrossRef]
- Smith, A.F.; Eccles, C.J.; Bhimani, S.J.; Denehy, K.M.; Bhimani, R.B.; Smith, L.S.; Malkani, A.L. Improved Patient Satisfaction following Robotic-Assisted Total Knee Arthroplasty. J. Knee Surg. 2021, 34, 730–738. [Google Scholar] [CrossRef]
- Capin, J.J.; Bade, M.J.; Jennings, J.M.; Snyder-Mackler, L.; Stevens-Lapsley, J.E. Total Knee Arthroplasty Assessments Should Include Strength and Performance-Based Functional Tests to Complement Range-of-Motion and Patient-Reported Outcome Measures. Phys. Ther. Rehabil. J. 2022, 102, pzac033. [Google Scholar] [CrossRef]
- Chan, A.C.M.; Jehu, D.A.; Pang, M.Y.C. Falls After Total Knee Arthroplasty: Frequency, Circumstances, and Associated Factors—A Prospective Cohort Study. Phys. Ther. Rehabil. J. 2018, 98, 767–778. [Google Scholar] [CrossRef]
- Kim, Y.H.; Yoon, S.H.; Park, J.W. Does Robotic-assisted TKA Result in Better Outcome Scores or Long-Term Survivorship Than Conventional TKA? A Randomized, Controlled Trial. Clin. Orthop. Relat. Res. 2020, 478, 266–275. [Google Scholar] [CrossRef]
- Meier, W.; Mizner, R.; Marcus, R.; Dibble, L.; Peters, C.; Lastayo, P.C. Total Knee Arthroplasty: Muscle Impairments, Functional Limitations, and Recommended Rehabilitation Approaches. J. Orthop. Sports Phys. Ther. 2008, 38, 246–256. [Google Scholar] [CrossRef]
- Mizner, R.L.; Petterson, S.C.; Stevens, J.E.; Vandenborne, K.; Snyder-Mackler, L. Early Quadriceps Strength Loss After Total Knee Arthroplasty. J. Bone Jt. Surg. 2005, 87, 1047–1053. [Google Scholar] [CrossRef]
- Mizner, R.L.; Petterson, S.C.; Snyder-Mackler, L. Quadriceps Strength and the Time Course of Functional Recovery After Total Knee Arthroplasty. J. Orthop. Sports Phys. Ther. 2005, 35, 424–436. [Google Scholar] [CrossRef]
- Yoshida, Y.; Mizner, R.L.; Ramsey, D.K.; Snyder-Mackler, L. Examining outcomes from total knee arthroplasty and the relationship between quadriceps strength and knee function over time. Clin. Biomech. 2008, 23, 320–328. [Google Scholar] [CrossRef]
- Pozzi, F.; White, D.K.; Snyder-Mackler, L.; Zeni, J.A. Restoring physical function after knee replacement: A cross sectional comparison of progressive strengthening vs. standard physical therapy. Physiother. Theory Pract. 2020, 36, 122–133. [Google Scholar] [CrossRef]
- Ma, N.; Sun, P.; Xin, P.; Zhong, S.; Xie, J.; Xiao, L. Comparison of the efficacy and safety of MAKO robot-assisted total knee arthroplasty versus conventional manual total knee arthroplasty in uncomplicated unilateral total knee arthroplasty a single-centre retrospective analysis. Int. Orthop. 2024, 48, 2351–2358. [Google Scholar] [CrossRef]
- Jakobsen, T.L.; Jakobsen, M.D.; Andersen, L.L.; Husted, H.; Kehlet, H.; Bandholm, T. Quadriceps muscle activity during commonly used strength training exercises shortly after total knee arthroplasty: Implications for home-based exercise-selection. J. Exp. Orthop. 2019, 6, 29. [Google Scholar] [CrossRef]
- Von, E.E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, 1623–1627. [Google Scholar]
- Maggio, M.; Ceda, G.P.; Ticinesi, A.; De Vita, F.; Gelmini, G.; Costantino, C.; Meschi, T.; Kressig, R.W.; Cesari, M.; Fabi, M.; et al. Instrumental and Non-Instrumental Evaluation of 4-Meter Walking Speed in Older Individuals. PLoS ONE 2016, 11, e0153583. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.S.; Vieira, T.M.; Pullinen, T.; Finni, T. Interpreting Signal Amplitudes in Surface Electromyography Studies in Sport and Rehabilitation Sciences. Front. Physiol. 2018, 8, 985. [Google Scholar] [CrossRef]
- Tikkanen, O.; Haakana, P.; Pesola, A.J.; Häkkinen, K.; Rantalainen, T.; Havu, M.; Pullinen, T.; Finni, T. Muscle Activity and Inactivity Periods during Normal Daily Life. PLoS ONE 2013, 8, e52228. [Google Scholar] [CrossRef]
- Marshall, R.N.; Morgan, P.T.; Martinez-Valdes, E.; Breen, L. Quadriceps muscle electromyography activity during physical activities and resistance exercise modes in younger and older adults. Exp. Gerontol. 2020, 136, 110965. [Google Scholar] [CrossRef]
- Alshatwi, R.; Alfadhel, S.; Alrasheed, M.; Alhakbani, A.; AlShaya, O. Comparison of Postoperative Pain and Function in Robotic Total Knee Arthroplasty and Conventional Total Knee Arthroplasty Amongst Patients at King Fahad Medical City in Riyadh, Saudi Arabia. Cureus 2023, 15, e36285. [Google Scholar] [CrossRef]
- Arhos, E.K.; Di Stasi, S.; Hartigan, E.H.; Snyder-Mackler, L. Males and females have different muscle activity patterns during gait after ACL injury and reconstruction. J. Electromyogr. Kinesiol. 2022, 66, 102694. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Intervention | Description |
|---|---|
| Range of Motion (ROM) Exercises | Passive and active-assisted exercises to improve knee flexion and extension, aiming to achieve at least 0° to 90° of motion within the first two weeks. |
| Strength Training | Strengthening the quadriceps, hamstrings, and hip muscles through isometric and isotonic exercises, progressing from closed-chain to open-chain activities as tolerated. |
| Neuromuscular Electrical Stimulation (NMES) | NMES was applied to the quadricep muscle to enhance muscle activation and strength. |
| Gait Training | Patients practiced weight-bearing and ambulation exercises, progressing from the use of assistive devices to independent walking. |
| Variables | Sample | Females (n = 50) | Males (n = 51) | Difference |
|---|---|---|---|---|
| Age, years | 69.8 ± 8.3 | 71.2 ± 6.9 | 68.2 ± 9.4 | 3.0 (0.8;5.2) p = 0.008 |
| Height, meters | 1.67 ± 0.08 | 1.62 ± 0.06 | 1.73 ± 0.07 | 0.1 (0.09;0.12) p < 0.001 |
| Weight, kilograms | 80.0 ± 15.4 | 75.1 ± 15.3 | 85.6 ± 13.6 | 10.5 (6.6;14.4) p < 0.001 |
| BMI, kg/m2 | 28.5 ± 4.8 | 28.5 ± 5.6 | 28.5 ± 3.7 | 0.0 (−1.3;1.3) p = 0.963 |
| Right side affected, n (%) | 60 (56.8) | 63 (55.8) | 58 (58.0) | p = 0.783 |
| Variables | Operated Side (n = 101) | Non-Operated Side (n = 101) | Inter-Subjects Effects (F; p-Value (η2p)) | ||||
|---|---|---|---|---|---|---|---|
| Female (n = 50) | Male (n = 51) | Female (n = 50) | Male (n = 51) | Sex | Side | Sex*Side | |
| Peak Muscle Activity (µV) | |||||||
| Vastus lateralis | 281.2 ± 192.6 | 221.2 ± 175.6 | 534.1 ± 307.4 | 393.1 ± 278.8 | F = 4.814; p = 0.031 (0.05) | F = 46.104; p < 0.001 (0.32) | F = 1.118; p = 0.293 (0.01) |
| Vastus medialis | 214.3 ± 162.2 | 166.0 ± 128.7 | 286.7 ± 204.9 | 267.5 ± 194.9 | F = 1.462; p = 0.229 (0.05) | F = 13.348; p < 0.001 (0.12) | F = 0.270; p = 0.604 (0.00) |
| Variables | Operated Side (n = 101) | Non-Operated Side (n = 101) | Inter-Subjects Effects (F; p-Value (η2p)) | ||||
|---|---|---|---|---|---|---|---|
| Female (n = 50) | Male (n = 51) | Female (n = 50) | Male (n = 51) | Sex | Side | Sex*Side | |
| Range of movement (degrees) | |||||||
| Flexion–extension | 74.6 ± 26.0 | 74.5 ± 28.1 | 79.4 ± 29.5 | 80.3 ± 26.8 | F = 0.015; p = 0.903 (0.00) | F = 6.503; p = 0.012 (0.063) | F = 0.175; p = 0.677 (0.00) |
| Peak Muscle activity (µV) | |||||||
| Vastus lateralis | 385.5 ± 252.6 | 252.5 ± 181.7 | 492.4 ± 298.5 | 435.2 ± 258.2 | F = 8.943; p = 0.004 (0.084) | F = 19.547; p < 0.001 (0.17) | F = 0.075; p = 0.784 (0.00) |
| Vastus medialis | 333.5 ± 243.9 | 300.5 ± 232.3 | 446.5 ± 262.5 | 400.1 ± 254.5 | F = 1.011; p = 0.317 (0.01) | F = 14.100; p < 0.001 (0.13) | F = 0.366; p = 0.547 (0.00) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Sanz, F.; Romero-Morales, C.; Espejo-Carrizo, R.; Caballero-López, J.; Sánchez-Clemente, D.; Bravo-Aguilar, M.; López-López, D.; Villafañe, J.H.; Jiménez-Saiz, S.L.; González-de-la-Flor, Á. Muscle Activation and Mobility After Robotic Total Knee Arthroplasty: Insights from Early Postoperative Recovery. J. Clin. Med. 2025, 14, 3150. https://doi.org/10.3390/jcm14093150
García-Sanz F, Romero-Morales C, Espejo-Carrizo R, Caballero-López J, Sánchez-Clemente D, Bravo-Aguilar M, López-López D, Villafañe JH, Jiménez-Saiz SL, González-de-la-Flor Á. Muscle Activation and Mobility After Robotic Total Knee Arthroplasty: Insights from Early Postoperative Recovery. Journal of Clinical Medicine. 2025; 14(9):3150. https://doi.org/10.3390/jcm14093150
Chicago/Turabian StyleGarcía-Sanz, Fernando, Carlos Romero-Morales, Rocío Espejo-Carrizo, Julio Caballero-López, Daniel Sánchez-Clemente, María Bravo-Aguilar, Daniel López-López, Jorge Hugo Villafañe, Sergio L. Jiménez-Saiz, and Ángel González-de-la-Flor. 2025. "Muscle Activation and Mobility After Robotic Total Knee Arthroplasty: Insights from Early Postoperative Recovery" Journal of Clinical Medicine 14, no. 9: 3150. https://doi.org/10.3390/jcm14093150
APA StyleGarcía-Sanz, F., Romero-Morales, C., Espejo-Carrizo, R., Caballero-López, J., Sánchez-Clemente, D., Bravo-Aguilar, M., López-López, D., Villafañe, J. H., Jiménez-Saiz, S. L., & González-de-la-Flor, Á. (2025). Muscle Activation and Mobility After Robotic Total Knee Arthroplasty: Insights from Early Postoperative Recovery. Journal of Clinical Medicine, 14(9), 3150. https://doi.org/10.3390/jcm14093150