
Guided Frontal Sinus Osteotomy: A Pilot Study of a Digital Protocol for “In-House” Manufacturing Surgical Cutting Guides

 ,
,  , ,
, ,  and
and
Abstract

1. Introduction
2. Materials and Methods
- Inclusion Criteria
- Complex benign pathologies involving the frontal sinus (osteomas, mucoceles, recurrent sinusitis), needing a frontal sinus osteotomy + ESS (DRAF procedures) according to Chiu classification [4];
- Maxillofacial computer tomography (CT) performed within 7 days before surgery;
- Intraoperative employment of the “in-house” manufactured surgical cutting guide;
- A minimum follow-up of 18 months.
- Exclusion Criteria
- Contraindications to perform a frontal sinus osteotomy (pathologies resolved with the only endoscopic approach);
- Malignant tumors;
- Previous traumas/chemotherapy/radiotherapy in the frontal region;
- Patient refusal of surgery;
- Insufficient follow-up.
2.1. Data Collection
2.2. Step-By-Step Surgical Cutting Guides Manufacturing Protocol
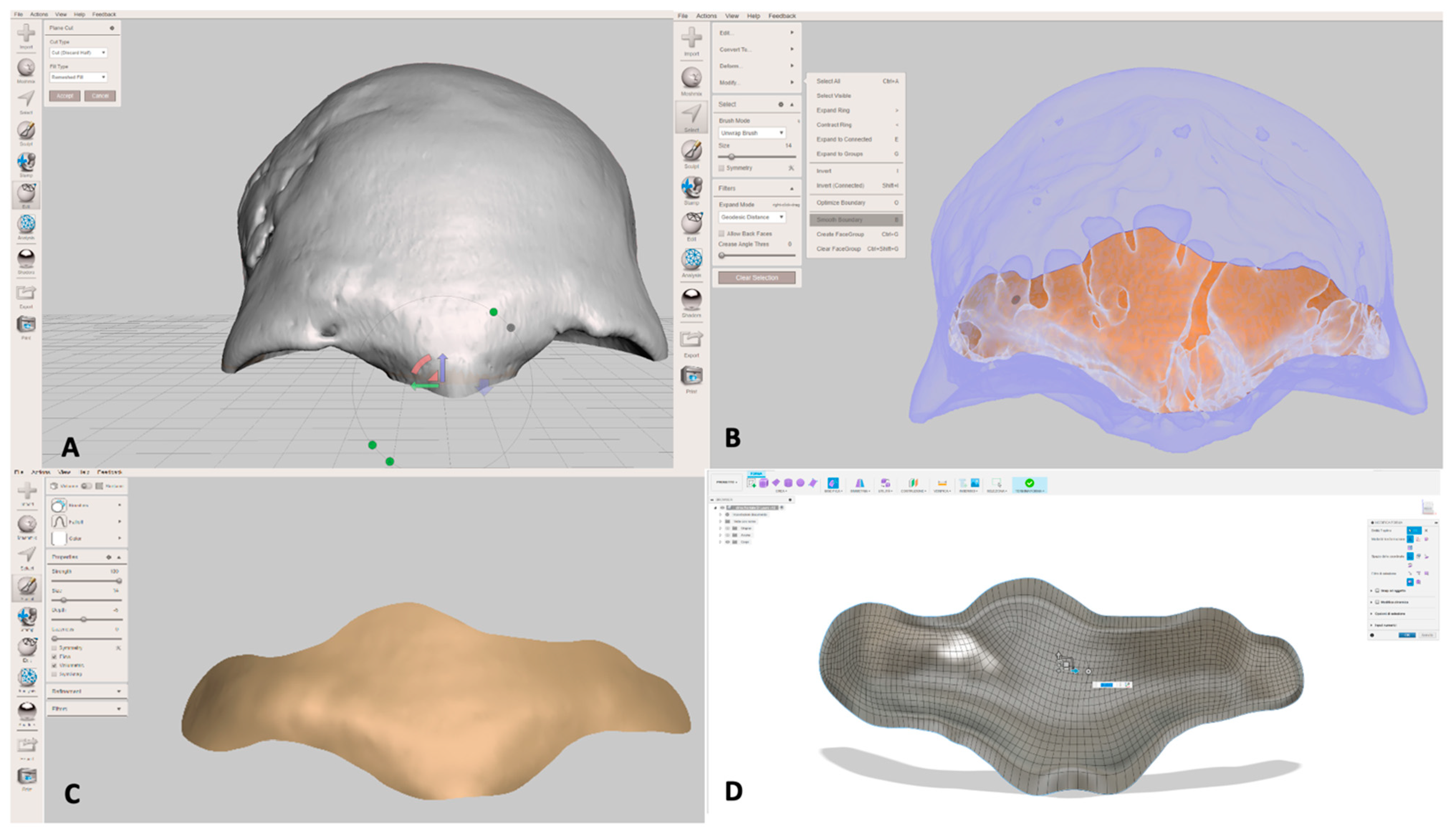
2.2.1. Conversion from DICOM (Digital Imaging and Communications in Medicine) Files to STL (Stereolithography) Files
2.2.2. Identification of the Frontal Sinus Margins and Selection of Osteotomy Lines
2.2.3. Cutting Guide Design
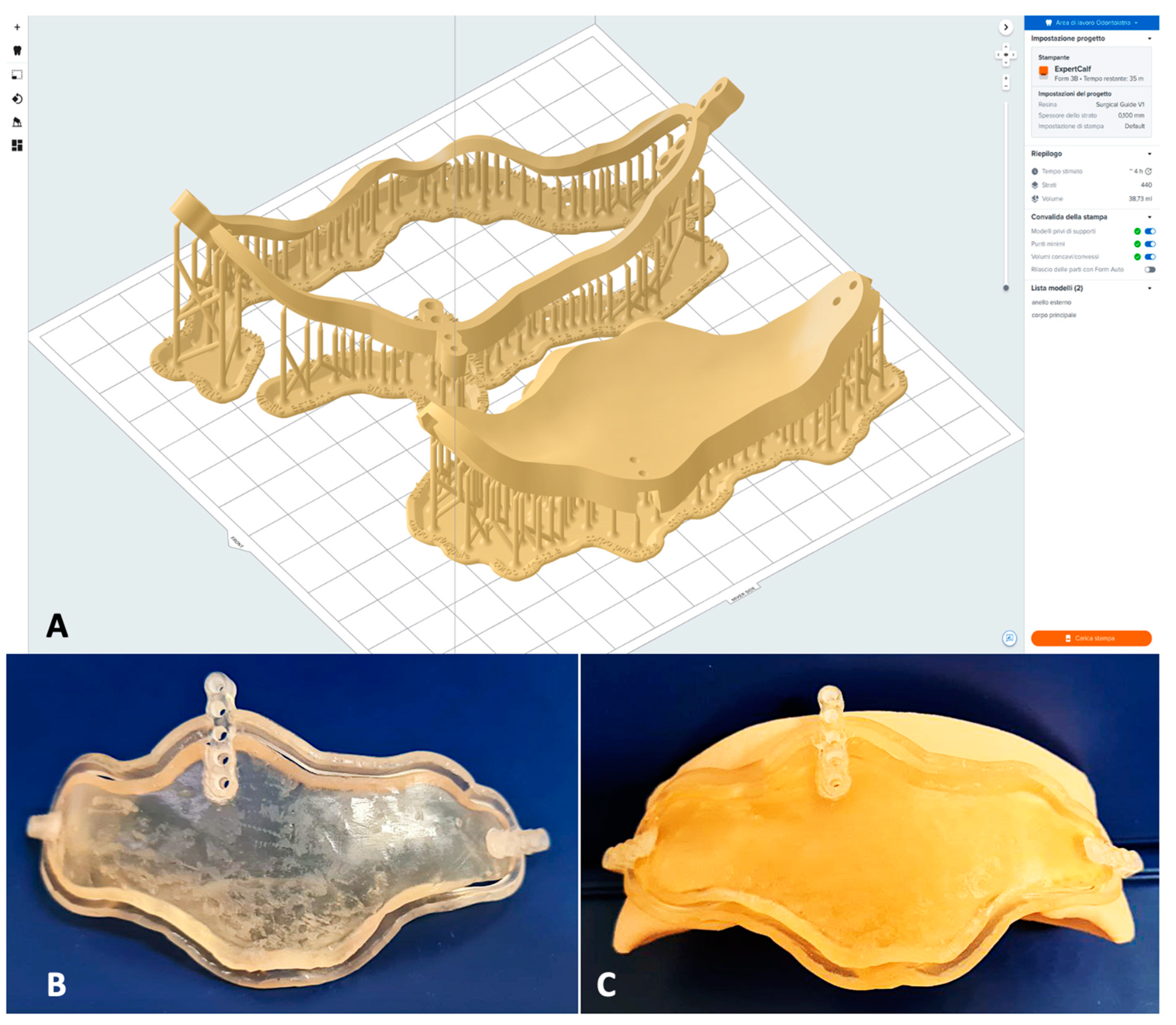
2.2.4. Rapid Prototyping 3D Printing
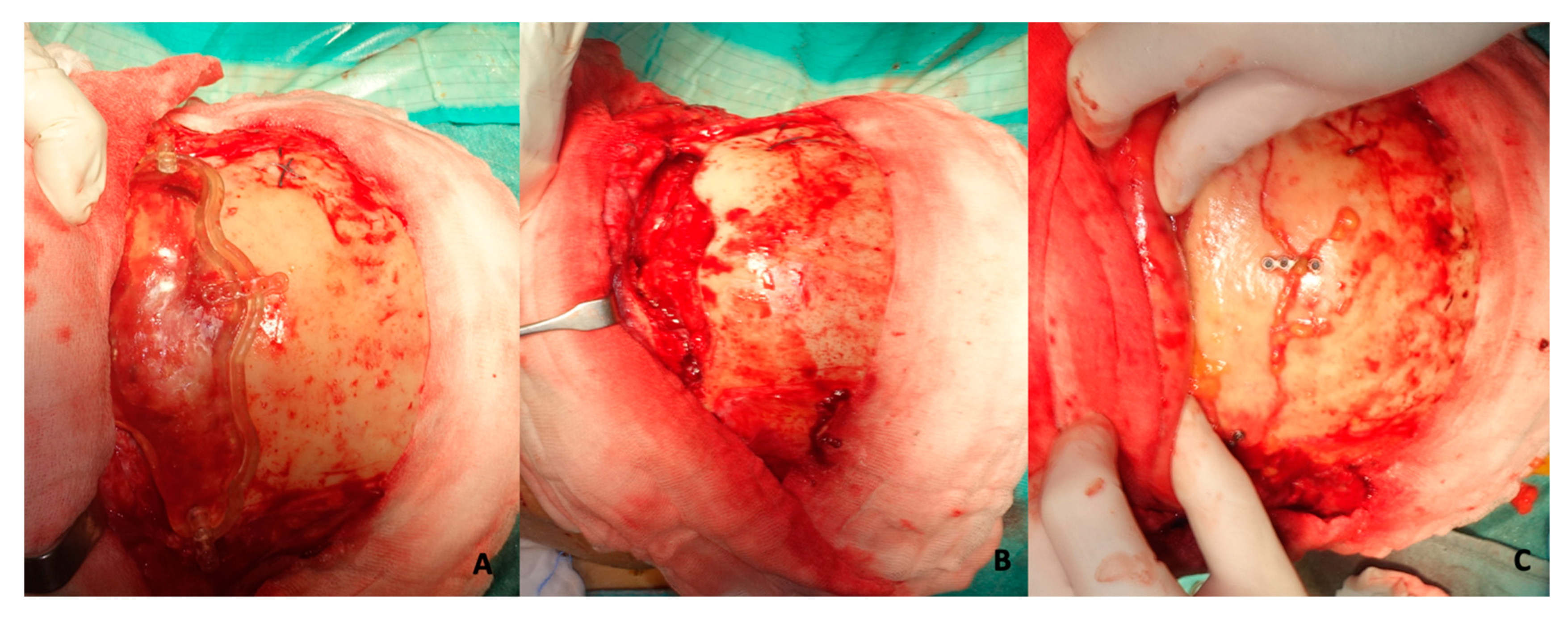
2.3. Surgical Procedure (Employment of Template)
2.4. Follow-Up and Outcomes
3. Results
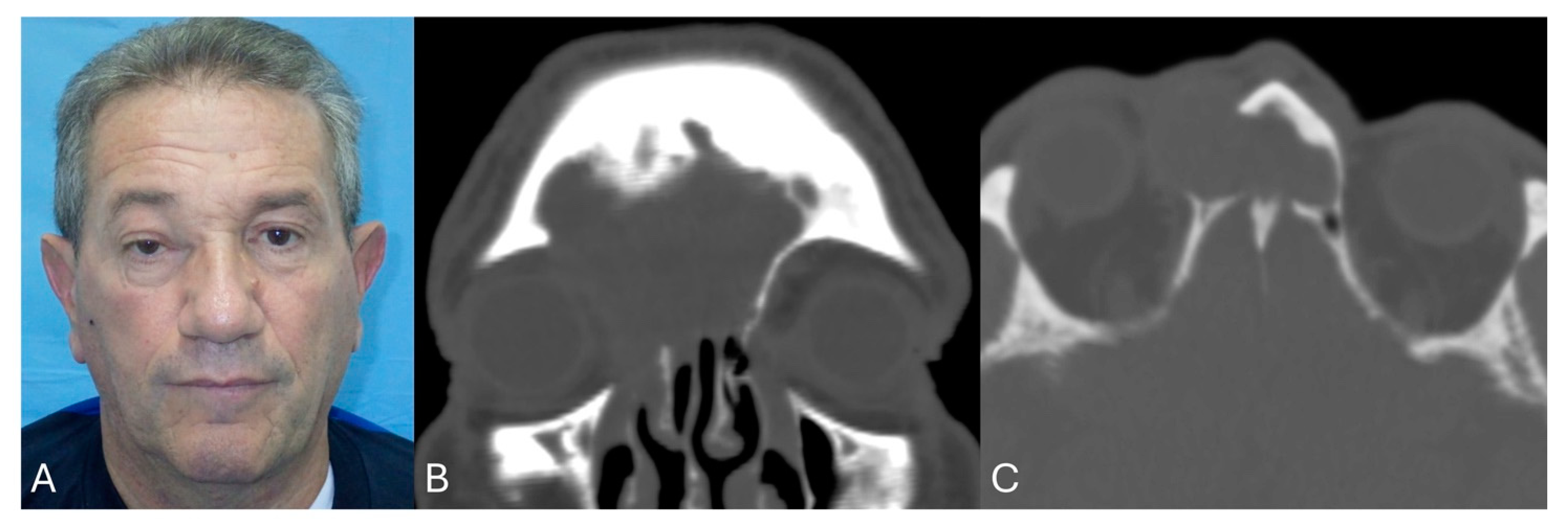
3.1. Population Features
3.2. Cutting Guides Manufacturing Results
3.3. Video
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAD/CAM | Computer-Aided Design/Computer-Aided Manufacturing |
| CT | Computer Tomography |
| 3D | Dimensional |
| VSP | Virtual Surgical Planning |
| USD | Dollars |
| ESS | Endoscopic sinus surgery |
| DICOM | Digital imaging and communication in medicine |
| STL | Standard triangulation language |
| SLA | Stereolithography Apparatus |
| EUR | Euros |
References
- Morse, J.C.; Chandra, R.K. Is there still a role for cranialization in modern sinus surgery? Curr. Opin. Otolaryngol. Head Neck Surg. 2021, 29, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Solmell, O.; Sunnergren, O.; Qureshi, A.R.; Alinasab, B. Functional and Esthetic Outcomes of Either Surgically or Conservatively Treated Anterior Frontal Sinus Wall Fractures: A Long-Term Follow-Up. Craniomaxillofac. Trauma Reconstr. 2024, 17, NP68–NP76. [Google Scholar] [CrossRef]
- Hoshal, S.G.; Dedhia, R.D.; Strong, E.B. Frontal sinus fractures: A contemporary approach in the endoscopic era. Facial Plast. Surg. Clin. N. Am. 2022, 30, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Chiu, A.G.; Schipor, I.; Cohen, N.A.; Kennedy, D.W.; Palmer, J.N. Surgical Decisions in the Management of Frontal Sinus Osteomas. Am. J. Rhinol. 2005, 19, 191–197. [Google Scholar] [CrossRef]
- Lee, Y.H.; Lee, J.Y.; Lawson, W. Indications and Outcomes of the Osteoplastic Flap Procedure with or Without Obliteration. J. Craniofac. Surg. 2020, 31, 2243–2249. [Google Scholar] [CrossRef]
- Silverman, J.B.; Gray, S.T.; Busaba, N.Y. Role of osteoplastic frontal sinus obliteration in the era of endoscopic sinus surgery. Int. J. Otolaryngol. 2012, 2012, 501896. [Google Scholar] [CrossRef] [PubMed]
- Carraturo, E.; Germano, C.; Troise, S.; Spinelli, R.; Romano, A.; Giudice, G.L.; Vaira, L.A.; Piombino, P. In house 3-D printed surgical guide for frontal sinus osteotomy in traumatology: A technical note. J. Stomatol. Oral. Maxillofac. Surg. 2024, 126, 102023. [Google Scholar] [CrossRef]
- Romano, A.; Troise, S.; Committeri, U.; Arena, A.; Dell’Aversana Orabona, G.; Seidita, F.; Bonavolontà, P.; Iaconetta, G.; Califano, L. Surgical Approaches in Odontogenic Orbital Cellulitis (OOC): Our Experience and Review of Literature. Indian J. Otolaryngol. Head Neck Surg. 2022, 74 (Suppl. 3), 4552–4561. [Google Scholar]
- Fanchette, J.; Faucon, B.; Cartry, F.; Ratajczak, M. Reconstruction of the anterior wall of the frontal sinus by a custom-made titanium prosthesis after resection of a giant osteoma of the frontal sinus. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 33–36. [Google Scholar] [CrossRef]
- Ganry, L.; Cömert, M. Low-Cost and Simple Frontal Sinus Surgical Cutting Guide Modeling for Anterior Cranioplasty in Facial Feminization Surgery: How to Do It. J. Craniofac Surg. 2022, 33, e84–e87. [Google Scholar] [CrossRef]
- Tawa, P.; Brault, N.; Luca-Pozner, V.; Ganry, L.; Chebbi, G.; Atlan, M.; Qassemyar, Q. Three-Dimensional Custom-Made Surgical Guides in Facial Feminization Surgery: Prospective Study on Safety and Accuracy. Aesthet Surg. J. 2021, 41, NP1368–NP1378. [Google Scholar] [CrossRef]
- Wauters, L.D.; Miguel-Moragas, J.S.; Mommaerts, M.Y. Classification of Computer-Aided Design-Computer-Aided Manufacturing Applications for the Reconstruction of Cranio-Maxillo-Facial Defects. J. Craniofac. Surg. 2015, 26, 2329–2333. [Google Scholar] [CrossRef] [PubMed]
- Matsui, C.; Tokuyama, E.; Senoo, T.; Yamada, K.; Kameda, M.; Takeuchi, T.; Kimata, Y. Utilization of a Simple Surgical Guide for Multidirectional Cranial Distraction Osteogenesis in Craniosynostosis. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2797. [Google Scholar] [CrossRef] [PubMed]
- Certo, F.; Altieri, R.; Crimi, S.; Gurrera, G.; Cammarata, G.; Visocchi, M.; Bianchi, A.; Barbagallo, G.M.V. Image-Guided Surgery in Complex Skull Base and Facial Fractures: Initial Experience on the Role of Intra-Operative Computer Tomography. Acta Neurochir. Suppl. 2023, 135, 61–67. [Google Scholar]
- Borbon, C.; Novaresio, A.; Iocca, O.; Nonis, F.; Moos, S.; Vezzetti, E.; Ramieri, G.; Zavattero, E. Evaluating Osteotomy Accuracy in Mandibular Reconstruction: A Preliminary Study Using Custom Cutting Guides and Virtual Reality. Diseases 2025, 13, 81. [Google Scholar] [CrossRef] [PubMed]
- Coppen, C.; Snoeijink, T.J.; Weijs, W.L.J.; Verhulst, A.; Verhoeven, T.; Rijssel, J.T.V.; Maal, T.J.J.; Dik, E.A. Augmented reality-guided osteotomies for simulated mandibular reconstruction with fibular bone using virtual cutting guides and 3D navigation. Br. J. Oral. Maxillofac. Surg. 2025, 63, 246–251. [Google Scholar] [CrossRef]
- Vu, C.; Hartsfield, J.K.; Mian, A.; Allan, B.; Gebauer, D.; Goonewardene, M. Accuracy of computer-simulated mandibular autorotation following single-jaw maxillary repositioning surgery using customized surgical cutting guides and fixation plates. Int. J. Oral. Maxillofac. Surg. 2025, in press. [Google Scholar] [CrossRef]
- Amarista, F.J.; Ellis, E., 3rd. Accuracy of Two Different Patient-Specific Drill/Cutting Guides for Maxillary Repositioning When Used for Minimally Invasive Bimaxillary Orthognathic Surgery. J. Oral. Maxillofac. Surg. 2025, 83, 421–428. [Google Scholar] [CrossRef]
- Yang, C.; Zhang, C.; Wu, J.; Xu, X.; Zhang, Y.; Zhang, S. Three-Dimensional Printed Customized Surgical Guides for the Precise Correction of Complex Midfacial Post-Traumatic Deformities. J. Craniofac Surg. 2022, 33, 1150–1153. [Google Scholar] [CrossRef]
- Schulze, M.; Juergensen, L.; Rischen, R.; Toennemann, M.; Reischle, G.; Puetzler, J.; Gosheger, G.; Hasselmann, J. Quality assurance of 3D-printed patient specific anatomical models: A systematic review. 3D Print Med. 2024, 10, 9. [Google Scholar] [CrossRef]
- Manfredini, M.; Poli, P.P.; Maiorana, C.; Salina, F.E.; Tandurella, M.; Beretta, M. Computer Aided Full Arch Restoration by Means of One-Piece Implants and Stackable Guide: A Technical Note. Dent. J. 2023, 11, 256. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, A.; Osypko, K. Complex Full-Arch Treatment with Zygomatic Implants, Fully Digital Protocol with Scan Flag Intraoral Scanning, and 3D-Printed Temporary Reconstructions in a Periodontal Patient—A Case Report. Biomedicines 2024, 12, 2617. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, A.; Osypko, K. Digital Workflow in Full Mouth Rehabilitation with Immediate Loading, Intraoral Welding and 3D-Printed Reconstructions in a Periodontal Patient: A Case Report. Reports 2023, 6, 52. [Google Scholar] [CrossRef]
- Kasradze, D.; Kubilius, R. The Influence of Guiding Concept on the Accuracy of Static Computer-Assisted Implant Surgery in Partially Edentulous Cases: An In Vitro Study. Medicina 2025, 61, 617. [Google Scholar] [CrossRef]
- Fatima, A.; Hackman, T.G.; Wood, J.S. Cost-Effectiveness Analysis of Virtual Surgical Planning in Mandibular Reconstruction. Plast. Reconstr. Surg. 2019, 143, 1185–1194. [Google Scholar] [CrossRef]
- Ritschl, L.M.; Kilbertus, P.; Grill, F.D.; Schwarz, M.; Weitz, J.; Nieberler, M.; Wolff, K.D.; Fichter, A.M. In-House, Open-Source 3D-Software-Based, CAD/CAM-Planned Mandibular Reconstructions in 20 Consecutive Free Fibula Flap Cases: An Explorative Cross-Sectional Study with Three-Dimensional Performance Analysis. Front. Oncol. 2021, 11, 731336. [Google Scholar] [CrossRef]
- McAllister, P.; Watson, M.; Burke, E. A Cost-Effective, In-House, Positioning and Cutting Guide System for Orthognathic Surgery. J. Maxillofac. Oral. Surg. 2018, 17, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Abbate, V.; Committeri, U.; Troise, S.; Bonavolontà, P.; Vaira, L.A.; Gabriele, G.; Biglioli, F.; Tarabbia, F.; Califano, L.; Dell’Aversana Orabona, G. Virtual Surgical Reduction in Atrophic Edentulous Mandible Fractures: A Novel Approach Based on “in House” Digital Work-Flow. Appl. Sci. 2023, 13, 1474. [Google Scholar] [CrossRef]
- Troise, S.; De Fazio, G.R.; Committeri, U.; Spinelli, R.; Nocera, M.; Carraturo, E.; Salzano, G.; Arena, A.; Abbate, V.; Bonavolontà, P.; et al. Mandibular reconstruction after post-traumatic complex fracture: Comparison analysis between traditional and virtually planned surgery. J. Stomatol. Oral. Maxillofac. Surg. 2024, 126, 102029. [Google Scholar] [CrossRef]
- Committeri, U.; Magliulo, R.; Carraturo, E.; Arena, A.; Abbate, V.; Salzano, G.; Troise, S.; Barone, S.; Germano, C.; Vaira, L.A.; et al. Virtual surgical planning in tripod zygomatico-maxillary complex fractures: A prospective comparison between two different strategies. J. Craniomaxillofac. Surg. 2024, 52, 1497–1504. [Google Scholar] [CrossRef]
- Velusamy, A.; Anand, A.; Hameed, N. Navigation Assisted Frontal Sinus Osteoplastic Flap Surgeries—A Case Series. Indian J. Otolaryngol. Head Neck Surg. 2022, 74 (Suppl. 2), 1232–1236. [Google Scholar] [CrossRef]
- Yu, P.; Mao, X.; Li, X.; Hu, X.; Li, J.; Sun, G. Endoscopic frontal trephination verse the osteoplastic flap in patients with frontal sinus disease after bifrontal craniotomy. Br. J. Neurosurg. 2021, 35, 65–67. [Google Scholar] [CrossRef]
- Kim, I.; Kim, J.M.; Kim, J.; Lee, S.J.; Nam, E.C. Management of frontal sinus trauma: A retrospective study of surgical interventions and complications. Maxillofac. Plast. Reconstr. Surg. 2024, 46, 4. [Google Scholar] [CrossRef] [PubMed]
- Crocetta, F.M.; Farneti, P.; Sollini, G.; Castellucci, A.; Ghidini, A.; Spinosi, M.C.; Fernandez, I.J.; Zoli, M.; Mazzatenta, D.; Pasquini, E. Endoscopic management of frontal sinus diseases after frontal craniotomy: A case series and review of the literature. Eur. Arch. Otorhinolaryngol. 2021, 278, 1035–1045. [Google Scholar] [CrossRef]
- Horowitz, G.; Amit, M.; Ben-Ari, O.; Gil, Z.; Abergel, A.; Margalit, N.; Cavel, O.; Wasserzug, O.; Fliss, D.M. Cranialization of the frontal sinus for secondary mucocele prevention following open surgery for benign frontal lesions. PLoS ONE 2013, 8, e83820. [Google Scholar] [CrossRef]
- Weber, R.; Draf, W.; Keerl, R.; Kahle, G.; Schinzel, S.; Thomann, S.; Lawson, W. Osteoplastic frontal sinus surgery with fat obliteration: Technique and long-term results using magnetic resonance imaging in 82 operations. Laryngoscope 2000, 110, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Rampinelli, V.; Ferrari, M.; Dohin, I.; Vinciguerra, A.; Mattavelli, D.; Saccardo, T.; Testa, G.; Conti, C.; Frigerio, C.; Verillaud, B.; et al. Advanced paranasal sinuses osteomas: A retrospective multicentric analysis on surgical management outcomes and intra- and postsurgical complications. Rhinology 2025, 63, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Merola, R.; Vargas, M. Economic Indicators, Quantity and Quality of Health Care Resources Affecting Post-surgical Mortality. J. Epidemiol. Glob. Health 2024, 14, 613–620. [Google Scholar] [CrossRef]
- Meng, M.; Wang, J.; Sun, T.; Zhang, W.; Zhang, J.; Shu, L.; Li, Z. Clinical applications and prospects of 3D printing guide templates in orthopaedics. J. Orthop. Translat. 2022, 34, 22–41. [Google Scholar] [CrossRef]
- Abo Sharkh, H.; Makhoul, N. In-House Surgeon-Led Virtual Surgical Planning for Maxillofacial Reconstruction. J. Oral. Maxillofac. Surg. 2020, 78, 651–660. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Sex | Age | Type of Disease | Signs and Symptoms | Time of Procedure * | Follow-Up | Complications | Outcomes |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 47 | Frontal-ethmoidal mucocele | Frontal wall erosion with skin fistulization | 28 min (about 5 h) | 50 months | No | Resolution of the symptom |
| 2 | M | 68 | Recurrent frontal sinusitis | Headache, Rhinorrhea | 26 min (about 5.5 h) | 46 months | No | Resolution of the symptom |
| 3 | M | 53 | Frontal-ethmoidal mucocele | Headache, pain | 25 min (about 4 h) | 43 months | No | Resolution of the symptom |
| 4 | M | 31 | Frontal-orbital-ethmoidal osteoma | Lateral globe dislocation | 23 min (about 5.5 h) | 38 months | No | Partial resolution of the symptom |
| 5 | F | 72 | Recurrent frontal sinusitis | Pain, rhinorrhea, and hyposmia | 22 min (about 5 h) | 36 months | No | Partial resolution of the symptom (hyposmia) |
| 6 | M | 43 | Frontal-ethmoidal mucocele | Headache, pain | 25 min (about 4.5 h) | 30 months | No | Resolution of the symptom |
| 7 | F | 57 | Frontal-orbital-ethmoidal osteoma | Exophthalmos, dystopia, and lateral globe dislocation | 20 min (about 5 h) | 28 months | No | Partial resolution of the symptom |
| 8 | M | 67 | Frontal-ethmoidal mucocele | Headache, pain, rhinorrhea, and frontal wall erosion with skin fistulization | 25 min (about 4.5 h) | 26 months | Recurrence after one year | Headache, pain, and rhinorrea |
| 9 | M | 71 | Recurrent frontal sinusitis | Headache, pain, and rhinorrhea | 23 min (about 4 h) | 24 months | No | Resolution of the symptom |
| 10 | M | 48 | Frontal-ethmoidal osteoma | Asymptomatic | 20 min (about 5 h) | 21 months | No | / |
| 11 | F | 58 | Recurrent frontal sinusitis | Headache, pain, and rhinorrhea, | 21 min (about 4 h) | 20 months | No | Resolution of the symptom |
| 12 | M | 63 | Frontal-ethmoidal mucocele | Frontal wall erosion with skin fistulization | 22 min (about 4 h) | 18 months | No | Resolution of the symptom |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, A.; Troise, S.; Spinelli, R.; Abbate, V.; Dell’Aversana Orabona, G. Guided Frontal Sinus Osteotomy: A Pilot Study of a Digital Protocol for “In-House” Manufacturing Surgical Cutting Guides. J. Clin. Med. 2025, 14, 3141. https://doi.org/10.3390/jcm14093141
Romano A, Troise S, Spinelli R, Abbate V, Dell’Aversana Orabona G. Guided Frontal Sinus Osteotomy: A Pilot Study of a Digital Protocol for “In-House” Manufacturing Surgical Cutting Guides. Journal of Clinical Medicine. 2025; 14(9):3141. https://doi.org/10.3390/jcm14093141
Chicago/Turabian StyleRomano, Antonio, Stefania Troise, Raffaele Spinelli, Vincenzo Abbate, and Giovanni Dell’Aversana Orabona. 2025. "Guided Frontal Sinus Osteotomy: A Pilot Study of a Digital Protocol for “In-House” Manufacturing Surgical Cutting Guides" Journal of Clinical Medicine 14, no. 9: 3141. https://doi.org/10.3390/jcm14093141
APA StyleRomano, A., Troise, S., Spinelli, R., Abbate, V., & Dell’Aversana Orabona, G. (2025). Guided Frontal Sinus Osteotomy: A Pilot Study of a Digital Protocol for “In-House” Manufacturing Surgical Cutting Guides. Journal of Clinical Medicine, 14(9), 3141. https://doi.org/10.3390/jcm14093141