
Beyond Traditional Repair: Comparing eTEP and Open Sublay for Ventral Hernia Repair

Abstract
1. Introduction
2. Materials and Methods
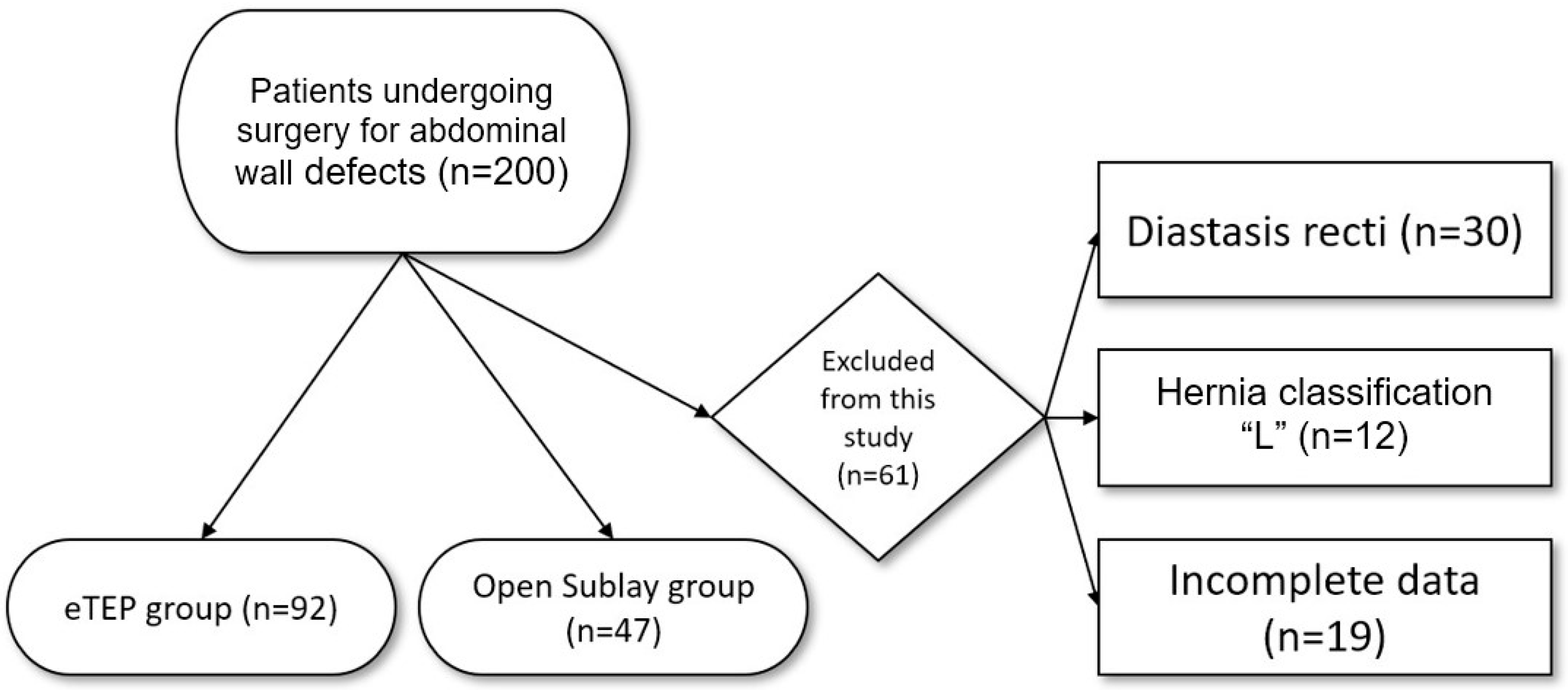
2.1. Study Design and Participants
2.2. Inclusion and Exclusion Criteria
2.3. Variables
2.4. Surgical Techniques
2.4.1. eTEP
2.4.2. Open Sublay (OS)
2.5. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Intraoperative Findings
3.3. Postoperative Findings
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| eTEP | Enhanced-View Totally Extraperitoneal |
| OS | Open Sublay |
| VAS | Visual Analog Scale |
| BMI | Body Mass Index |
| COPD | Chronic Obstructive Pulmonary Disease |
| ASA | American Society of Anesthesiologists |
| SSI | Surgical Site Infection |
| SSO | Surgical Site Occurrence |
| SSOPI | Surgical Site Occurrence Requiring Procedural Intervention |
References
- Henriksen, N.A.; Kaufmann, R.; Simons, M.P.; Berrevoet, F.; East, B.; Fischer, J.; Hope, W.; Klassen, D.; Lorenz, R.; Renard, Y.; et al. EHS and AHS guidelines for treatment of primary ventral hernias in rare locations or special circumstances. BJS Open 2020, 4, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Millikan, K.W. Incisional hernia repair. Surg. Clin. N. Am. 2003, 83, 1223–1234. [Google Scholar] [CrossRef]
- Muysoms, F.E.; Miserez, M.; Berrevoet, F.; Campanelli, G.; Champault, G.G.; Chelala, E.; Dietz, U.A.; Eker, H.H.; El Nakadi, I.; Hauters, P.; et al. Classification of primary and incisional abdominal wall hernias. Hernia 2009, 13, 407–414. [Google Scholar] [CrossRef]
- Bittner, R.; Bain, K.; Bansal, V.K.; Berrevoet, F.; Bingener-Casey, J.; Chen, D.; Chen, J.; Chowbey, P.; Dietz, U.A.; De Beaux, A.; et al. Update of Guidelines for laparoscopic treatment of ventral and incisional abdominal wall hernias (International Endohernia Society (IEHS))—Part A. Surg. Endosc. 2019, 33, 3069–3139. [Google Scholar] [CrossRef] [PubMed]
- Deerenberg, E.B.; Timmermans, L.; Hogerzeil, D.P.; Slieker, J.C.; Eilers, P.H.C.; Jeekel, J.; Lange, J.F. A systematic review of the surgical treatment of large incisional hernia. Hernia 2015, 19, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Köckerling, F.; Simon, T.; Hukauf, M.; Hellinger, A.; Fortelny, R.; Reinpold, W.; Bittner, R. The Importance of Registries in the Postmarketing Surveillance of Surgical Meshes. Ann. Surg. 2018, 268, 1097–1104. [Google Scholar] [CrossRef]
- Sanders, D.L.; Pawlak, M.M.; Simons, M.P.; Aufenacker, T.; Balla, A.; Berger, C.; Berrevoet, F.; de Beaux, A.C.; East, B.; Henriksen, N.A.; et al. Midline incisional hernia guidelines: The European Hernia Society. Br. J. Surg. 2023, 110, 1732–1768. [Google Scholar] [CrossRef]
- Belyansky, I.; Daes, J.; Radu, V.G.; Balasubramanian, R.; Reza Zahiri, H.; Weltz, A.S.; Sibia, U.S.; Park, A.; Novitsky, Y. A novel approach using the enhanced-view totally extraperitoneal (eTEP) technique for laparoscopic retromuscular hernia repair. Surg. Endosc. 2018, 32, 1525–1532. [Google Scholar] [CrossRef]
- Wieland, L.; Alfarawan, F.; Bockhorn, M.; El-Sourani, N. Comparison of eTEP and IPOM for ventral hernia surgery in the early postoperative period: A retrospective cohort study of a tertiary university centre. Hernia 2024, 28, 2195–2206. [Google Scholar] [CrossRef]
- DeBord, J.; Novitsky, Y.; Fitzgibbons, R.; Miserez, M.; Montgomery, A. SSI, SSO, SSE, SSOPI: The elusive language of complications in hernia surgery. Hernia 2018, 22, 737–738. [Google Scholar] [CrossRef]
- Nyhus, L.M. The posterior (preperitoneal) approach and iliopubic tract repair of inguinal and femoral hernias—An update. Hernia 2003, 7, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Burger, J.W.A.; Luijendijk, R.W.; Hop, W.C.J.; Halm, J.A.; Verdaasdonk, E.G.G.; Jeekel, J. Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann. Surg. 2004, 240, 578–583, discussion 583–585. [Google Scholar] [CrossRef]
- LeBlanc, K.A. Incisional hernia repair: Laparoscopic techniques. World J. Surg. 2005, 29, 1073–1079. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Arora, E.; Kukleta, J.; Ramana, B. A Detailed History of Retromuscular Repairs for Ventral Hernias: A Story of Surgical Innovation. World J. Surg. 2022, 46, 409–415. [Google Scholar] [CrossRef]
- Bauer, K.; Heinzelmann, F.; Büchler, P.; Mück, B. Robotisch assistierte extraperitoneale Ventralhernienversorgung—Erfahrung der ersten 61 konsekutiven Operationen in eTEP- und eTAR-Technik. Chirurgie 2023, 94, 147–154. [Google Scholar] [CrossRef]
- Köckerling, F.; Simon, T.; Adolf, D.; Köckerling, D.; Mayer, F.; Reinpold, W.; Weyhe, D.; Bittner, R. Laparoscopic IPOM versus open sublay technique for elective incisional hernia repair: A registry-based, propensity score-matched comparison of 9907 patients. Surg. Endosc. 2019, 33, 3361–3369. [Google Scholar] [CrossRef]
- Hoenig, H.M.; Rubenstein, L.Z. Hospital-Associated Deconditioning and Dysfunction. J. Am. Geriatr. Soc. 1991, 39, 220–222. [Google Scholar] [CrossRef]
- Hauck, K.; Zhao, X. How Dangerous is a Day in Hospital?: A Model of Adverse Events and Length of Stay for Medical Inpatients. Med. Care 2011, 49, 1068–1075. [Google Scholar] [CrossRef]
- Habeeb, T.A.A.M.; Mokhtar, M.M.; Sieda, B.; Osman, G.; Ibrahim, A.; Metwalli, A.-E.M.; Riad, M.; Khalil, O.M.H.; Mansour, M.I.; Elshahidy, T.M.; et al. Changing the innate consensus about mesh fixation in trans-abdominal preperitoneal laparoscopic inguinal hernioplasty in adults: Short and long term outcome. Randomized controlled clinical trial. Int. J. Surg. 2020, 83, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Gossetti, F.; D’Amore, L.; Annesi, E.; Bruzzone, P.; Bambi, L.; Grimaldi, M.R.; Ceci, F.; Negro, P. Mesh-related visceral complications following inguinal hernia repair: An emerging topic. Hernia 2019, 23, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Bellido Luque, J.; Gomez Rosado, J.C.; Bellido Luque, A.; Gomez Menchero, J.; Suarez Grau, J.M.; Sanchez Matamoros, I.; Nogales Muñoz, A.; Oliva Mompeán, F.; Morales Conde, S. Endoscopic retromuscular technique (eTEP) vs conventional laparoscopic ventral or incisional hernia repair with defect closure (IPOM+) for midline hernias. A case–control study. Hernia 2021, 25, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Palanisamy, N.V.; Parthasarathi, R.; Sabnis, S.C.; Nayak, S.K.; Palanivelu, C. A comparative prospective study of short-term outcomes of extended view totally extraperitoneal (e-TEP) repair versus laparoscopic intraperitoneal on lay mesh (IPOM) plus repair for ventral hernia. Surg. Endosc. 2021, 35, 5072–5077. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | eTEP (n = 92) | OS (n = 47) | p-Value |
|---|---|---|---|
| Age (years) | 51.82 ± (13.15) * | 54.96 ± (15.11) * | 0.28 |
| BMI (kg/cm2) | 32.51 ± (7.45) * | 31.02 ± (7.92) * | 0.41 |
| Obesity level | |||
| Normal weight | 10 | 8 | 0.45 |
| Overweight | 25 | 13 | 1.0 |
| Obesity level I | 26 | 12 | 0.888 |
| Obesity level II | 17 | 10 | 0.867 |
| Obesity level III | 14 | 4 | 0.397 |
| Sex | 0.927 | ||
| Male | 58; 63.04% | 30; 63.83% | |
| Female | 34; 36.96% | 17; 36.17% | |
| ASA Score | |||
| I | 6; 6.52% | 5; 10.64% | 0.604 |
| II | 62; 67.39% | 25; 53.19% | 0.147 |
| III | 24; 26.09% | 14; 29.79% | 0.793 |
| IV | 0 | 3; 6.38 | 0.067 |
| V | 0 | 0 | / |
| Risk factors | |||
| Cardiovascular disease | 48; 52.17% | 21; 44.68% | 0.403 |
| COPD (%) | 2; 2.17% | 1; 2.13% | 0.986 |
| Diabetes (%) | 11; 11.96% | 6; 12.77% | 0.890 |
| Smoking (%) | 19; 20.0% | 15; 31.91% | 0.144 |
| Defect size (cm2) | 6 (IQR 9.25) † | 16 (IQR 40) † | 0.028 |
| Classification | eTEP (n = 127) | OS (n = 50) | p-Value |
|---|---|---|---|
| M1 | 2, 2.11% | 2, 4.26% | 0.548 |
| M2 | 41, 44.57% | 21, 44.68% | 0.990 |
| M3 | 73, 79.35% | 18, 38.3% | <0.001 |
| M4 | 8, 8.70% | 7, 14.89% | 0.265 |
| M5 | 3, 3.26% | 2, 4.26% | 0.842 |
| Variables | eTEP (n = 92) | OS (n = 47) | p-Value |
|---|---|---|---|
| Mesh size (cm2) | 450 (IQR 125) † | 150 (IQR 270) † | <0.001 |
| Operation time (minutes) | 110 (IQR 60) † | 100 (IQR 47) † | 0.064 |
| Intraoperative complications | 2 (2.17%) | 3 (6.38%) | 0.207 |
| Admission period (days) | 3 (IQR 1) † | 5 (IQR 2) † | <0.001 |
| Variables | eTEP (n = 92) | OS (n = 47) | p-Value |
|---|---|---|---|
| Postoperative complications | 6 (6.52%) | 10 (21.28%) | 0.009 |
| Clavien–Dindo | 0.082 | ||
| I | 2 | 5 | |
| II | 1 | 0 | |
| IIIa | 1 | 0 | |
| IIIb | 2 | 4 | |
| IV | 0 | 0 | |
| V | 0 | 1 | |
| Admission period (days) | 3 (IQR 1) † | 5 (IQR 2) † | <0.001 |
| VAS | |||
| Postoperative day 1 | 1.4 (IQR 1,92) † | 2 (IQR 2.75) † | 0.884 |
| Postoperative day 2 | 1 (IQR 2) † | 1.3 (IQR 1.9) † | 0.208 |
| Postoperative day 3 | 0.5 (IQR 2) † | 0 (IQR 2) † | 0.636 |
| Technique | n | Description of Complication |
|---|---|---|
| eTEP | 2 | Hemoglobin-relevant bleeding |
| 1 | Abscess | |
| 1 | Early recurrence | |
| 2 | Hematoma | |
| OS | 1 | Wound dehiscence |
| 1 | Rupture of a drainage tube | |
| 4 | Infection of the wound | |
| 2 | Hematoma | |
| 1 | Pneumonia | |
| 1 | Subcutaneous seroma |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Looft, P.; Alfarawan, F.; Bockhorn, M.; El-Sourani, N. Beyond Traditional Repair: Comparing eTEP and Open Sublay for Ventral Hernia Repair. J. Clin. Med. 2025, 14, 2586. https://doi.org/10.3390/jcm14082586
Looft P, Alfarawan F, Bockhorn M, El-Sourani N. Beyond Traditional Repair: Comparing eTEP and Open Sublay for Ventral Hernia Repair. Journal of Clinical Medicine. 2025; 14(8):2586. https://doi.org/10.3390/jcm14082586
Chicago/Turabian StyleLooft, Phillip, Fadl Alfarawan, Maximilian Bockhorn, and Nader El-Sourani. 2025. "Beyond Traditional Repair: Comparing eTEP and Open Sublay for Ventral Hernia Repair" Journal of Clinical Medicine 14, no. 8: 2586. https://doi.org/10.3390/jcm14082586
APA StyleLooft, P., Alfarawan, F., Bockhorn, M., & El-Sourani, N. (2025). Beyond Traditional Repair: Comparing eTEP and Open Sublay for Ventral Hernia Repair. Journal of Clinical Medicine, 14(8), 2586. https://doi.org/10.3390/jcm14082586