Amygdala EFP Neurofeedback Effects on PTSD Symptom Clusters and Emotional Regulation Processes

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. Robustness and Long-Term Effects of Treatment
4.2. Cross-Cluster Symptom Improvement
4.3. Neural Circuit Mechanisms
4.4. Emotion Regulation Mechanisms
4.5. Clinical Implications and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Amyg-EFP-NF | Amygdala-derived-EEG-fMRI-Pattern |
| PTSD | Post-Traumatic Stress Disorder |
| ERQ | Emotional Regulation Questionnaire |
| fMRI-NF | Functional Magnetic Resonance Imaging-based NF |
| CR | Cognitive Reappraisal |
| ES | Expressive Suppression |
References
- Frans, O.; Rimmö, P.A.; Aberg, L.; Fredrikson, M. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatr. Scand. 2005, 111, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Galatzer-Levy, I.R.; Bryant, R.A. 636,120 Ways to Have Posttraumatic Stress Disorder. Perspect. Psychol. Sci. 2013, 8, 651–662. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association Publishing: Washington, DC, USA, 2022; ISBN 0-89042-575-2. [Google Scholar]
- Friedman, M.J.; Resick, P.A.; Bryant, R.A.; Brewin, C.R. Considering PTSD for DSM-5. Depress. Anxiety 2011, 28, 750–769. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.J. Finalizing PTSD in DSM-5: Getting here from there and where to go next. J. Trauma. Stress 2013, 26, 548–556. [Google Scholar] [CrossRef]
- Lee, D.J.; Bovin, M.J.; Weathers, F.W.; Palmieri, P.A.; Schnurr, P.P.; Sloan, D.M.; Keane, T.M.; Marx, B.P. Latent factor structure of DSM-5 posttraumatic stress disorder: Evaluation of method variance and construct validity of novel symptom clusters. Psychol. Assess. 2019, 31, 46–58. [Google Scholar] [CrossRef]
- Müller-Engelmann, M.; Schnyder, U.; Dittmann, C.; Priebe, K.; Bohus, M.; Thome, J.; Fydrich, T.; Pfaltz, M.C.; Steil, R. Psychometric Properties and Factor Structure of the German Version of the Clinician-Administered PTSD Scale for DSM-5. Assessment 2020, 27, 1128–1138. [Google Scholar] [CrossRef]
- Insel, T.; Cuthbert, B.; Garvey, M.; Heinssen, R.; Pine, D.S.; Quinn, K.; Sanislow, C.; Wang, P. Research domain criteria (RDoC): Toward a new classification framework for research on mental disorders. Am. J. Psychiatry 2010, 167, 748–751. [Google Scholar] [CrossRef]
- Williams, L.M.; Carpenter, W.T.; Carretta, C.; Papanastasiou, E.; Vaidyanathan, U. Precision psychiatry and Research Domain Criteria: Implications for clinical trials and future practice. CNS Spectr. 2024, 29, 26–39. [Google Scholar] [CrossRef]
- Lincoln, T.M.; Schulze, L.; Renneberg, B. The role of emotion regulation in the characterization, development and treatment of psychopathology. Nat. Rev. Psychol. 2022, 5, 272–286. [Google Scholar] [CrossRef]
- Braunstein, L.M.; Gross, J.J.; Ochsner, K.N. Explicit and implicit emotion regulation: A multi-level framework. Soc. Cogn. Affect. Neurosci. 2017, 12, 1545–1557. [Google Scholar] [CrossRef]
- Insel, T.R.; Cuthbert, B.N. Medicine. Brain disorders? Precisely. Science 2015, 348, 499–500. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T.; Quack, D. Emotion regulation difficulties in trauma survivors: The role of trauma type and PTSD symptom severity. Behav. Ther. 2010, 41, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Ciccarelli, G.; Federico, G.; Mele, G.; Di Cecca, A.; Migliaccio, M.; Ilardi, C.R.; Alfano, V.; Salvatore, M.; Cavaliere, C. Simultaneous real-time EEG-fMRI neurofeedback: A systematic review. Front. Hum. Neurosci. 2023, 17, 1123014. [Google Scholar] [CrossRef] [PubMed]
- Thibault, R.T.; MacPherson, A.; Lifshitz, M.; Roth, R.R.; Raz, A. Neurofeedback with fMRI: A critical systematic review. Neuroimage 2018, 172, 786–807. [Google Scholar] [CrossRef]
- Watanabe, T.; Sasaki, Y.; Shibata, K.; Kawato, M. Advances in fMRI Real-Time Neurofeedback. Trends Cogn. Sci. (Regul. Ed.) 2017, 21, 997–1010. [Google Scholar] [CrossRef]
- Linhartová, P.; Látalová, A.; Kóša, B.; Kašpárek, T.; Schmahl, C.; Paret, C. fMRI neurofeedback in emotion regulation: A literature review. Neuroimage 2019, 193, 75–92. [Google Scholar] [CrossRef]
- Etkin, A.; Büchel, C.; Gross, J.J. The neural bases of emotion regulation. Nat. Rev. Neurosci. 2015, 16, 693–700. [Google Scholar] [CrossRef]
- Sitaram, R.; Ros, T.; Stoeckel, L.; Haller, S.; Scharnowski, F.; Lewis-Peacock, J.; Weiskopf, N.; Blefari, M.L.; Rana, M.; Oblak, E.; et al. Closed-loop brain training: The science of neurofeedback. Nat. Rev. Neurosci. 2017, 18, 86–100. [Google Scholar] [CrossRef]
- Zotev, V.; Phillips, R.; Misaki, M.; Wong, C.K.; Wurfel, B.E.; Krueger, F.; Feldner, M.; Bodurka, J. Real-time fMRI neurofeedback training of the amygdala activity with simultaneous EEG in veterans with combat-related PTSD. Neuroimage Clin. 2018, 19, 106–121. [Google Scholar] [CrossRef]
- Lubianiker, N.; Paret, C.; Dayan, P.; Hendler, T. Neurofeedback through the lens of reinforcement learning. Trends Neurosci. 2022, 45, 579–593. [Google Scholar] [CrossRef]
- Cury, C.; Maurel, P.; Gribonval, R.; Barillot, C. A Sparse EEG-Informed fMRI Model for Hybrid EEG-fMRI Neurofeedback Prediction. Front. Neurosci. 2019, 13, 1451. [Google Scholar] [CrossRef]
- Keynan, J.N.; Meir-Hasson, Y.; Gilam, G.; Cohen, A.; Jackont, G.; Kinreich, S.; Ikar, L.; Or-Borichev, A.; Etkin, A.; Gyurak, A.; et al. Limbic Activity Modulation Guided by Functional Magnetic Resonance Imaging-Inspired Electroencephalography Improves Implicit Emotion Regulation. Biol. Psychiatry 2016, 80, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Keynan, J.N.; Cohen, A.; Jackont, G.; Green, N.; Goldway, N.; Davidov, A.; Meir-Hasson, Y.; Raz, G.; Intrator, N.; Fruchter, E.; et al. Electrical fingerprint of the amygdala guides neurofeedback training for stress resilience. Nat. Hum. Behav. 2019, 3, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Meir-Hasson, Y.; Kinreich, S.; Podlipsky, I.; Hendler, T.; Intrator, N. An EEG Finger-Print of fMRI deep regional activation. Neuroimage 2014, 102, 128–141. [Google Scholar] [CrossRef]
- Lubianiker, N.; Goldway, N.; Fruchtman-Steinbok, T.; Paret, C.; Keynan, J.N.; Singer, N.; Cohen, A.; Kadosh, K.C.; Linden, D.E.J.; Hendler, T. Process-based framework for precise neuromodulation. Nat. Hum. Behav. 2019, 3, 436–445. [Google Scholar] [CrossRef]
- Fruchtman-Steinbok, T.; Keynan, J.N.; Cohen, A.; Jaljuli, I.; Mermelstein, S.; Drori, G.; Routledge, E.; Krasnoshtein, M.; Playle, R.; Linden, D.E.J.; et al. Amygdala electrical-finger-print (AmygEFP) NeuroFeedback guided by individually-tailored Trauma script for post-traumatic stress disorder: Proof-of-concept. Neuroimage Clin. 2021, 32, 102859. [Google Scholar] [CrossRef]
- Fine, N.B.; Helpman, L.; Armon, D.B.; Gurevitch, G.; Sheppes, G.; Seligman, Z.; Hendler, T.; Bloch, M. Amygdala-related electroencephalogram neurofeedback as add-on therapy for treatment-resistant childhood sexual abuse posttraumatic stress disorder: Feasibility study. Psychiatry Clin. Neurosci. 2023, 78, 19–28. [Google Scholar] [CrossRef]
- Fruchter, E.; Goldenthal, N.; Adler, L.A.; Gross, R.; Harel, E.V.; Deutsch, L.; Nacasch, N.; Grinapol, S.; Amital, D.; Voigt, J.D.; et al. Amygdala-derived-EEG-fMRI-pattern neurofeedback for the treatment of chronic post-traumatic stress disorder. A prospective, multicenter, multinational study evaluating clinical efficacy. Psychiatry Res. 2024, 333, 115711. [Google Scholar] [CrossRef]
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Pers. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Fenster, R.J.; Lebois, L.A.M.; Ressler, K.J.; Suh, J. Brain circuit dysfunction in post-traumatic stress disorder: From mouse to man. Nat. Rev. Neurosci. 2018, 19, 535–551. [Google Scholar] [CrossRef] [PubMed]
- LeDoux, J.E.; Pine, D.S. Using Neuroscience to Help Understand Fear and Anxiety: A Two-System Framework. Am. J. Psychiatry 2016, 173, 1083–1093. [Google Scholar] [CrossRef] [PubMed]
- Paret, C.; Hendler, T. Live from the “regulating brain”: Harnessing the brain to change emotion. Emotion 2020, 20, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Zilverstand, A.; Parvaz, M.A.; Goldstein, R.Z. Neuroimaging cognitive reappraisal in clinical populations to define neural targets for enhancing emotion regulation. A systematic review. Neuroimage 2017, 151, 105–116. [Google Scholar] [CrossRef]
- Melani, M.S.; Paiva, J.M.; Mendlowicz, M.V.; Vilete, L.; Luz, M.P.; Ventura, P.R.; Passos, R.B.F.; Berger, W. Are There Differences Among Evidence-Based Psychotherapies for Treating Different DSM-5 PTSD Symptom Clusters? A Systematic Review and Meta-analysis of Controlled Clinical Trials. J. Nerv. Ment. Dis. 2024, 212, 332–343. [Google Scholar] [CrossRef]
- Rance, M.; Walsh, C.; Sukhodolsky, D.G.; Pittman, B.; Qiu, M.; Kichuk, S.A.; Wasylink, S.; Koller, W.N.; Bloch, M.; Gruner, P.; et al. Time course of clinical change following neurofeedback. Neuroimage 2018, 181, 807–813. [Google Scholar] [CrossRef]
- Goldway, N.; Ablin, J.; Lubin, O.; Zamir, Y.; Keynan, J.N.; Or-Borichev, A.; Cavazza, M.; Charles, F.; Intrator, N.; Brill, S.; et al. Volitional limbic neuromodulation exerts a beneficial clinical effect on Fibromyalgia. Neuroimage 2019, 186, 758–770. [Google Scholar] [CrossRef]
- Bu, J.; Young, K.D.; Hong, W.; Ma, R.; Song, H.; Wang, Y.; Zhang, W.; Hampson, M.; Hendler, T.; Zhang, X. Effect of deactivation of activity patterns related to smoking cue reactivity on nicotine addiction. Brain 2019, 142, 1827–1841. [Google Scholar] [CrossRef]
- Herry, C.; Ferraguti, F.; Singewald, N.; Letzkus, J.J.; Ehrlich, I.; Lüthi, A. Neuronal circuits of fear extinction. Eur. J. Neurosci. 2010, 31, 599–612. [Google Scholar] [CrossRef]
- Alexander, W. Pharmacotherapy for Post-traumatic Stress Disorder In Combat Veterans: Focus on Antidepressants and Atypical Antipsychotic Agents. Pharm. Ther. 2012, 37, 32–38. [Google Scholar]
- Krystal, J.H.; Neumeister, A. Noradrenergic and serotonergic mechanisms in the neurobiology of posttraumatic stress disorder and resilience. Brain Res. 2009, 1293, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.T.; Holmes, S.E.; Pietrzak, R.H.; Esterlis, I. Neurobiology of Chronic Stress-Related Psychiatric Disorders: Evidence from Molecular Imaging Studies. Chronic Stress 2017, 1, 2470547017710916. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.A.; Chen, S.; Narine, K.; Contractor, A.A.; Oslin, D. DSM-5 PTSD symptom clusters and suicidal ideation in veterans. Psychiatry Res. 2020, 288, 112942. [Google Scholar] [CrossRef]
- Lee, S.Y.; Park, C.L.; Cilhoroz, B.T.; Pescatello, L.S. PTSD symptom clusters and cardiovascular responses to stress: Reactivity and recovery. J. Psychosom. Res. 2022, 161, 110996. [Google Scholar] [CrossRef]
- Hayes, J.P.; Vanelzakker, M.B.; Shin, L.M. Emotion and cognition interactions in PTSD: A review of neurocognitive and neuroimaging studies. Front. Integr. Neurosci. 2012, 6, 89. [Google Scholar] [CrossRef]
- Fitzgerald, J.M.; DiGangi, J.A.; Phan, K.L. Functional neuroanatomy of emotion and its regulation in PTSD. Harv. Rev. Psychiatry 2018, 26, 116–128. [Google Scholar] [CrossRef]
- Lanius, R.A. Trauma-related dissociation and altered states of consciousness: A call for clinical, treatment, and neuroscience research. Eur. J. Psychotraumatol. 2015, 6, 27905. [Google Scholar] [CrossRef]
- Koch, C.; Massimini, M.; Boly, M.; Tononi, G. Neural correlates of consciousness: Progress and problems. Nat. Rev. Neurosci. 2016, 17, 307–321. [Google Scholar] [CrossRef]
- Fine, N.B.; Schwartz, N.; Hendler, T.; Gonen, T.; Sheppes, G. Neural Indices of Emotion Regulatory Implementation Correlate with Behavioral Regulatory Selection: Proof-of-Concept Investigation. Front. Behav. Neurosci. 2022, 16, 835253. [Google Scholar] [CrossRef]
- Gurevitch, G.; Lubianiker, N.; Markovits, T.; Or-Borichev, A.; Sharon, H.; Fine, N.B.; Fruchtman-Steinbok, T.; Keynan, J.N.; Shahar, M.; Friedman, A.; et al. Amygdala self-neuromodulation capacity as a window for process-related network recruitment. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2024, 379, 20240186. [Google Scholar] [CrossRef]
- Kim, J.; Pignatelli, M.; Xu, S.; Itohara, S.; Tonegawa, S. Antagonistic negative and positive neurons of the basolateral amygdala. Nat. Neurosci. 2016, 19, 1636–1646. [Google Scholar] [CrossRef] [PubMed]
- Pare, D.; Duvarci, S. Amygdala microcircuits mediating fear expression and extinction. Curr. Opin. Neurobiol. 2012, 22, 717–723. [Google Scholar] [CrossRef]
- Ressler, R.L.; Maren, S. Synaptic encoding of fear memories in the amygdala. Curr. Opin. Neurobiol. 2019, 54, 54–59. [Google Scholar] [CrossRef]
- Tng, G.Y.Q.; Koh, J.; Soh, X.C.; Majeed, N.M.; Hartanto, A. Efficacy of digital mental health interventions for PTSD symptoms: A systematic review of meta-analyses. J. Affect. Disord. 2024, 357, 23–36. [Google Scholar] [CrossRef]
- Kothgassner, O.D.; Goreis, A.; Kafka, J.X.; Van Eickels, R.L.; Plener, P.L.; Felnhofer, A. Virtual reality exposure therapy for posttraumatic stress disorder (PTSD): A meta-analysis. Eur. J. Psychotraumatol. 2019, 10, 1654782. [Google Scholar] [CrossRef]
- Sheppes, G.; Brady, W.J.; Samson, A.C. In (visual) search for a new distraction: The efficiency of a novel attentional deployment versus semantic meaning regulation strategies. Front. Psychol. 2014, 5, 346. [Google Scholar] [CrossRef]
- Fine, N.B.; Ben-Aharon, N.; Armon, D.B.; Seligman, Z.; Helpman, L.; Bloch, M.; Hendler, T.; Sheppes, G. Reduced emotion regulatory selection flexibility in post-traumatic stress disorder: Converging performance-based evidence from two PTSD populations. Psychol. Med. 2023, 53, 2758–2767. [Google Scholar] [CrossRef]
- Shepherd, L.; Wild, J. Emotion regulation, physiological arousal and PTSD symptoms in trauma-exposed individuals. J. Behav. Ther. Exp. Psychiatry 2014, 45, 360–367. [Google Scholar] [CrossRef]
- Powers, A.; Cross, D.; Fani, N.; Bradley, B. PTSD, emotion dysregulation, and dissociative symptoms in a highly traumatized sample. J. Psychiatr. Res. 2015, 61, 174–179. [Google Scholar] [CrossRef]
- Chesney, S.A.; Gordon, N.S. Profiles of emotion regulation: Understanding regulatory patterns and the implications for posttraumatic stress. Cogn. Emot. 2017, 31, 598–606. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | Study 1 (N = 25) | Study 2 (N = 37) | Study 3 (N = 66) |
|---|---|---|---|
| Demographics | |||
| Age, mean ± SD, years | 39.2 ± 12.3 | 36.8 ± 9.4 | 39.0 ± 10.6 |
| Female, n (%) | 12 (48.0%) | 37 (100%) | 35 (53.0%) |
| Education years, mean ± SD | 14.1 ± 2.5 | 14.5 ± 4.4 | 14.3 ± 2.8 |
| Marital Status | |||
| Married, n (%) | 12 (48.0%) | 9 (24.3%) | 32 (48.5%) |
| Single/Divorced/Separated, n (%) | 13 (52.0%) | 28 (75.7%) | 34 (51.5%) |
| Trauma Type | |||
| Combat/Military, n (%) | 9 (36.0%) | 0 (0%) | 31 (47.0%) |
| Childhood sexual abuse, n (%) | 4 (16.0%) | 37 (100%) | 12 (18.2%) |
| Interpersonal violence, n (%) | 6 (24.0%) | 0 (0%) | 10 (15.1%) |
| Accidents/Other, n (%) | 6 (24.0%) | 0 (0%) | 13 (19.7%) |
| Clinical Characteristics | |||
| CAPS-5 total score, mean ± SD | 35.4 ± 7.8 | 40.2 ± 8.1 | 42.5 ± 11.4 |
| Time from trauma, mean ± SD, years | 7.3 ± 5.2 | 13.5 ± 8.7 | 10.0 ± 5.7 |
| Medication use, n (%) | 17 (68.0%) | 30 (81.1%) | 48 (72.7%) |
| Concurrent psychotherapy, n (%) | 9 (36.0%) | 37 (100%) | 30 (45.5%) |
| Prior trauma-focused therapy completed, n (%) | 8 (32.0%) | 13 (35.1%) | 23 (34.8%) |
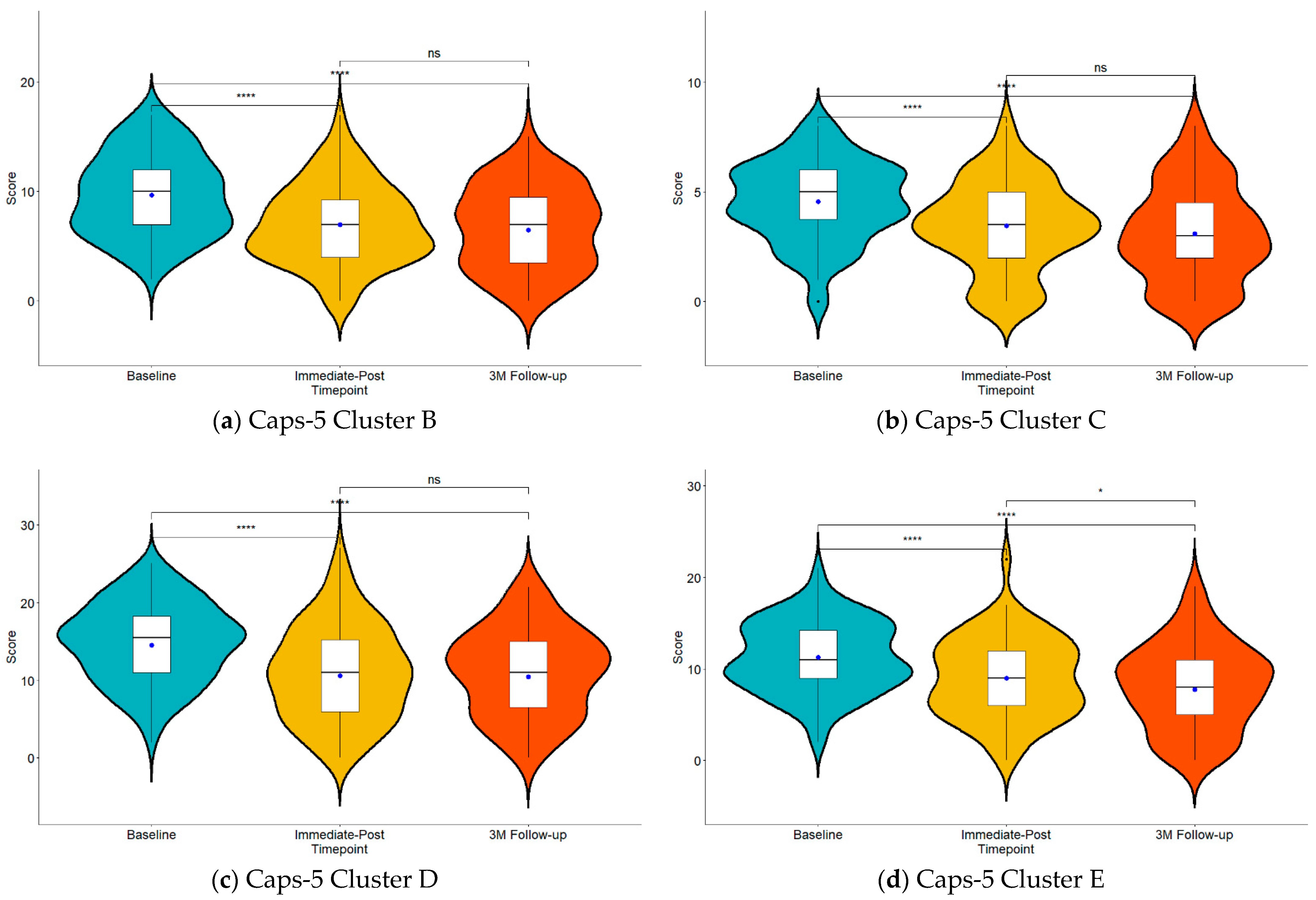
| Cluster | Timepoint | Mean [SD] | ||
|---|---|---|---|---|
| Study 1 (N = 25) | Study 2 (N = 37) | Study 3 (N = 66/63) | ||
| Intrusion (B) | Baseline | 8.60 [3.61] | 9.43 [3.90] | 10.24 [3.54] |
| Immediate-Post | 6.48 [3.92] | 7.05 [3.76] | 7.21 [3.49] | |
| 3 M Follow-up | 6.71 [3.79] | |||
| Avoidance (C) | Baseline | 4.28 [1.46] | 4.73 [1.88] | 4.59 [1.93] |
| Immediate-Post | 3.00 [1.61] | 3.65 [2.24] | 3.52 [2.03] | |
| 3 M Follow-up | 3.13 [2.21] | |||
| Cognition and Mood (D) | Baseline | 11.88 [4.37] | 15.38 [4.88] | 15.71 [4.90] |
| Immediate-Post | 8.16 [4.84] | 13.38 [5.88] | 10.67 [6.15] | |
| 3 M Follow-up | 11.06 [5.55] | |||
| Arousal and reactivity (E) | Baseline | 10.68 [3.48] | 10.70 [3.88] | 11.92 [3.92] |
| Immediate-Post | 8.32 [4.07] | 9.00 [4.25] | 9.26 [4.57] | |
| 3 M Follow-up | 8.10 [4.65] | |||
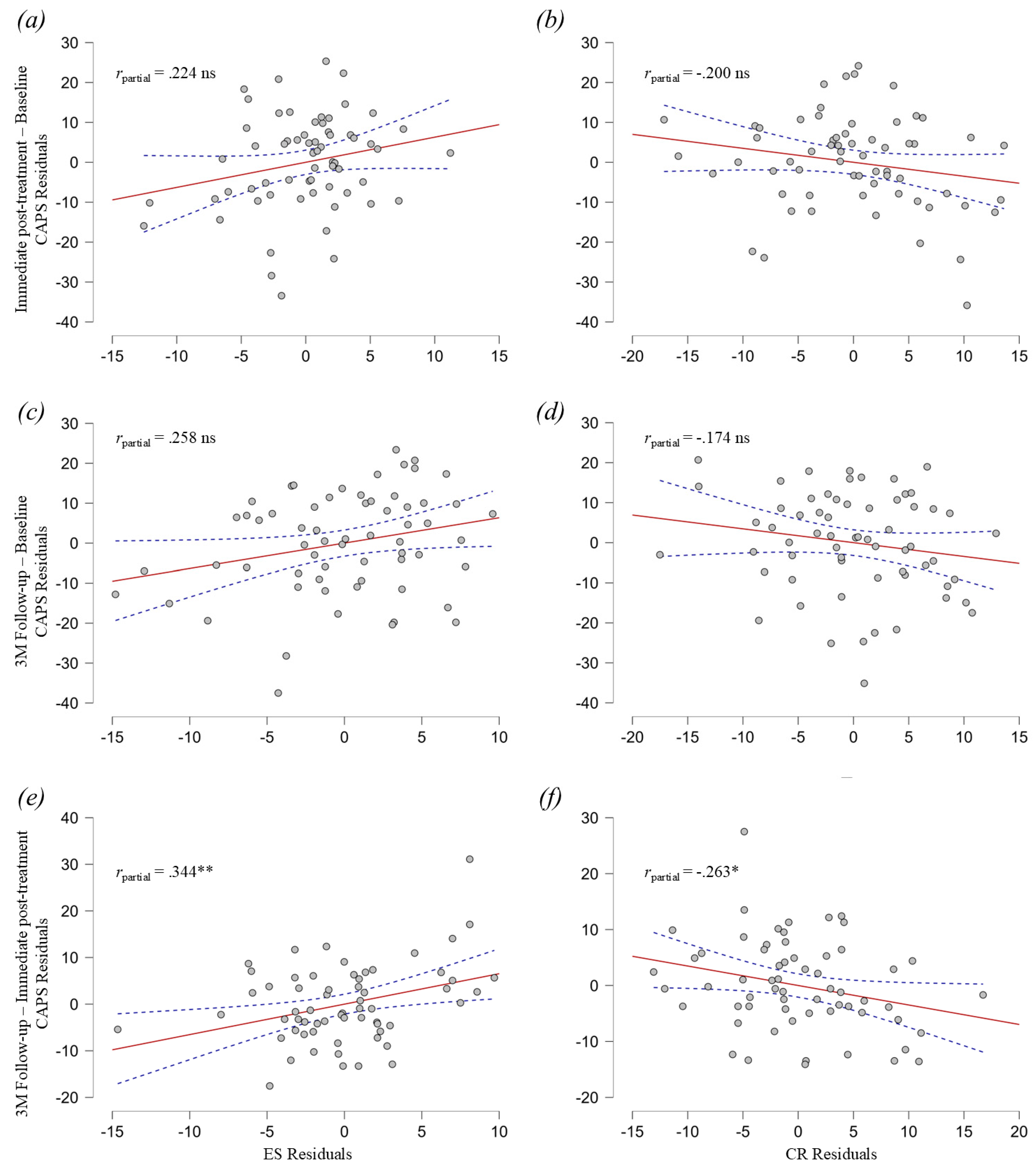
| Timepoint | Mean [SD] | ||
|---|---|---|---|
| CAPS-5 Total | ERQ Cognitive Reappraisal | ERQ Expressive Suppression | |
| Baseline | 42.52 [11.46] | 24.89 [8.34] | 15.38 [6.03] |
| Immediate Post | 30.49 [13.47] | 25.71 [6.79] | 14.62 [6.31] |
| 3 M Follow-up | 29.00 [13.61] | 27.02 [6.78] | 14.68 [5.98] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goldental, N.; Gross, R.; Amital, D.; Harel, E.V.; Hendler, T.; Tendler, A.; Levi, L.; Lavro, D.; Harmelech, T.; Grinapol, S.; et al. Amygdala EFP Neurofeedback Effects on PTSD Symptom Clusters and Emotional Regulation Processes. J. Clin. Med. 2025, 14, 2421. https://doi.org/10.3390/jcm14072421
Goldental N, Gross R, Amital D, Harel EV, Hendler T, Tendler A, Levi L, Lavro D, Harmelech T, Grinapol S, et al. Amygdala EFP Neurofeedback Effects on PTSD Symptom Clusters and Emotional Regulation Processes. Journal of Clinical Medicine. 2025; 14(7):2421. https://doi.org/10.3390/jcm14072421
Chicago/Turabian StyleGoldental, Nadav, Raz Gross, Daniela Amital, Eiran V. Harel, Talma Hendler, Aron Tendler, Liora Levi, Dmitri Lavro, Tal Harmelech, Shulamit Grinapol, and et al. 2025. "Amygdala EFP Neurofeedback Effects on PTSD Symptom Clusters and Emotional Regulation Processes" Journal of Clinical Medicine 14, no. 7: 2421. https://doi.org/10.3390/jcm14072421
APA StyleGoldental, N., Gross, R., Amital, D., Harel, E. V., Hendler, T., Tendler, A., Levi, L., Lavro, D., Harmelech, T., Grinapol, S., Nacasch, N., & Fruchter, E. (2025). Amygdala EFP Neurofeedback Effects on PTSD Symptom Clusters and Emotional Regulation Processes. Journal of Clinical Medicine, 14(7), 2421. https://doi.org/10.3390/jcm14072421