


The Establishment of a Treatment Protocol for the Reconstruction of Mid-Sized Defects in Lip Cancer Using Combinations with the Abbe Flap


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
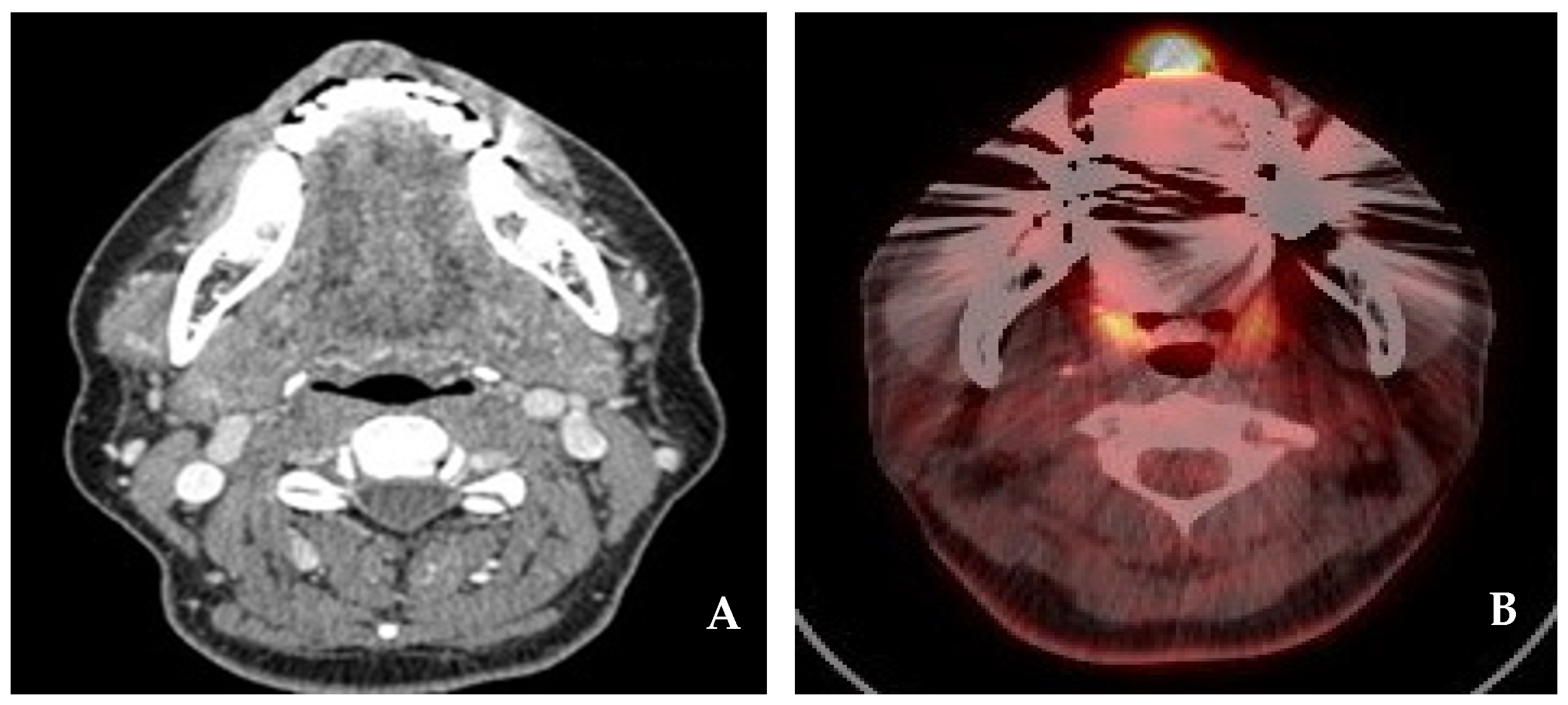
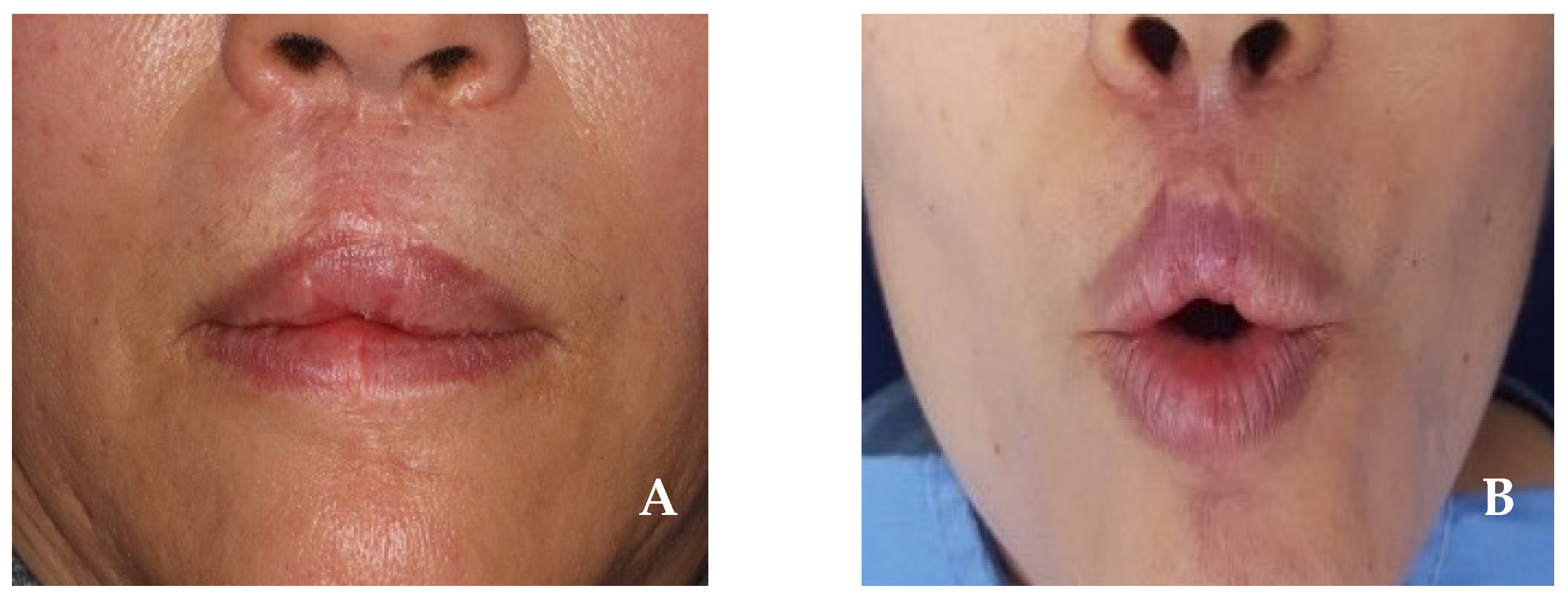
2.1. Case 1
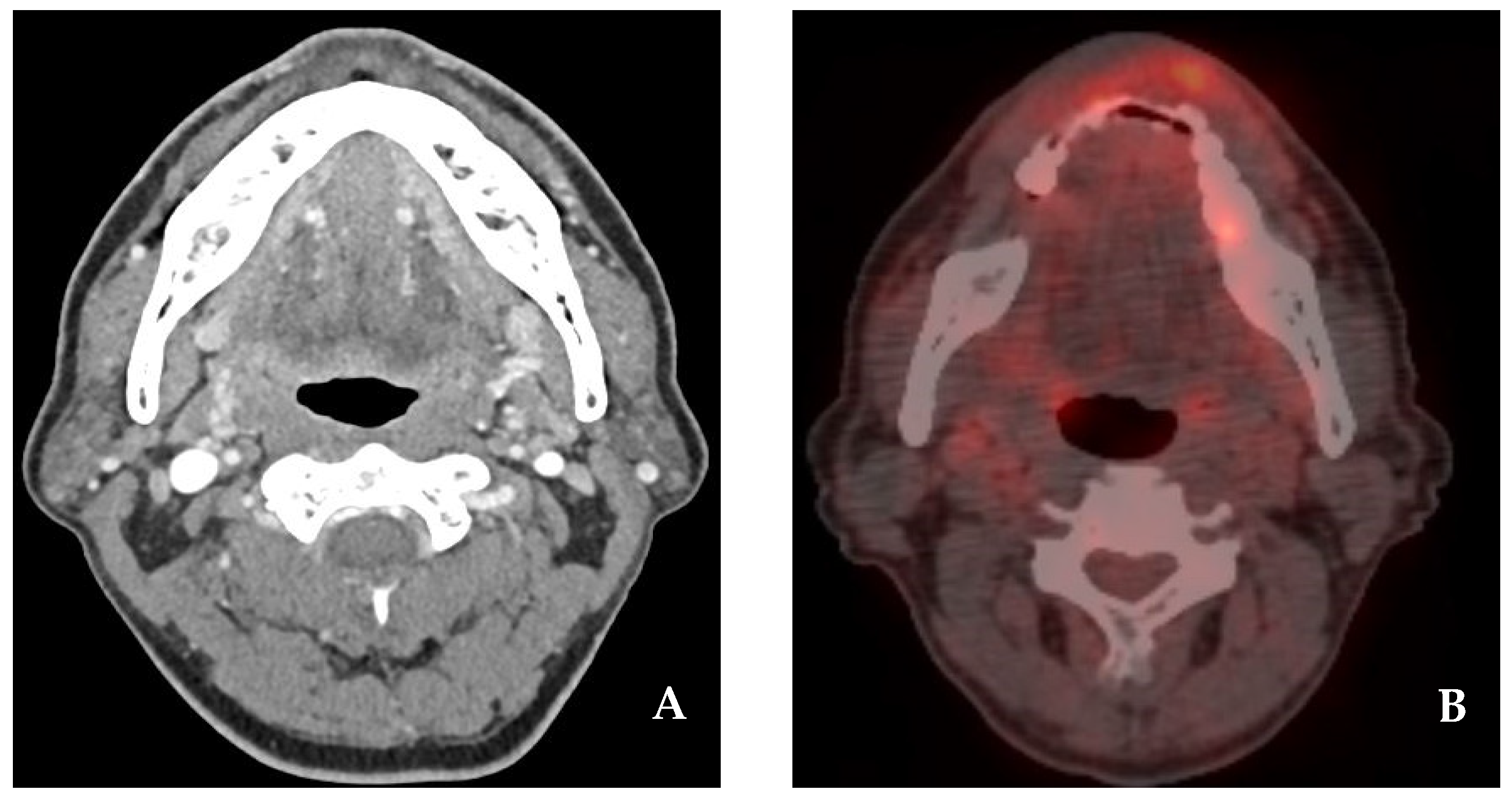
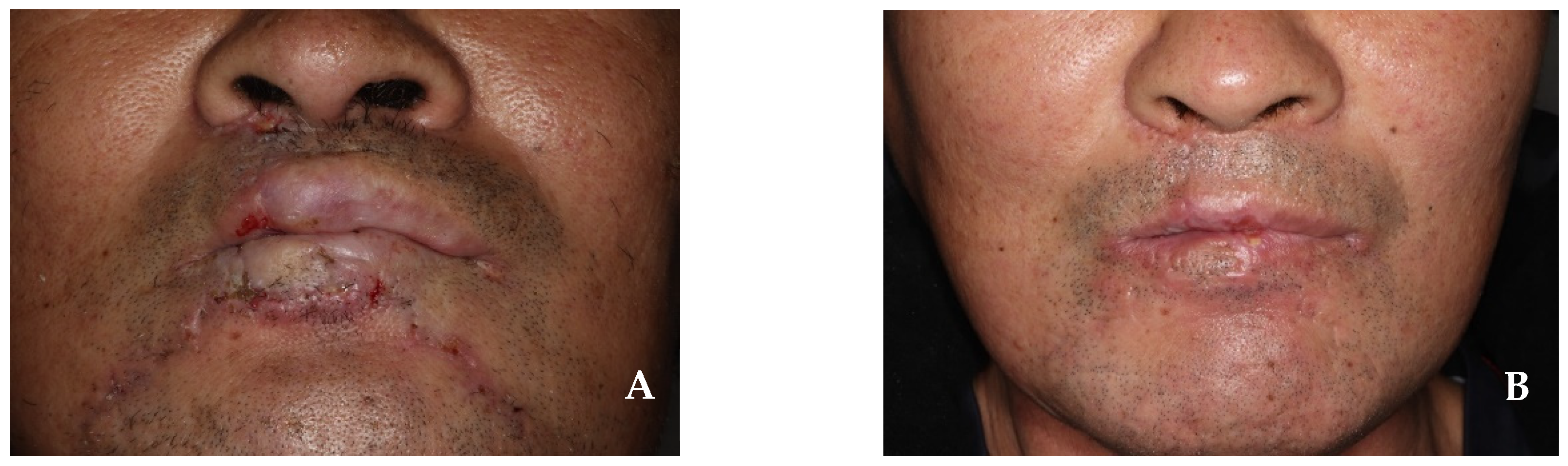
2.2. Case 2
3. Results and Discussion
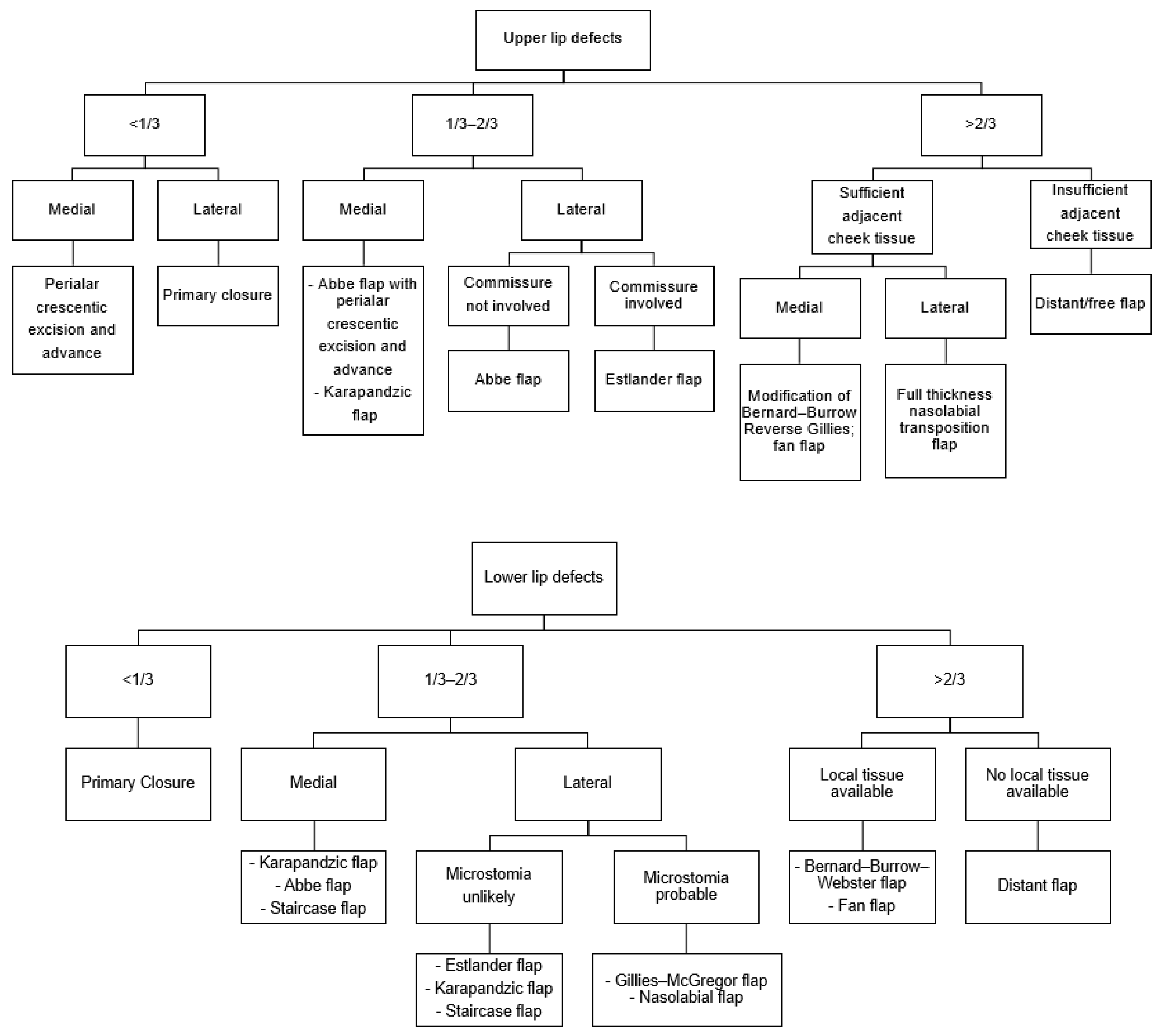
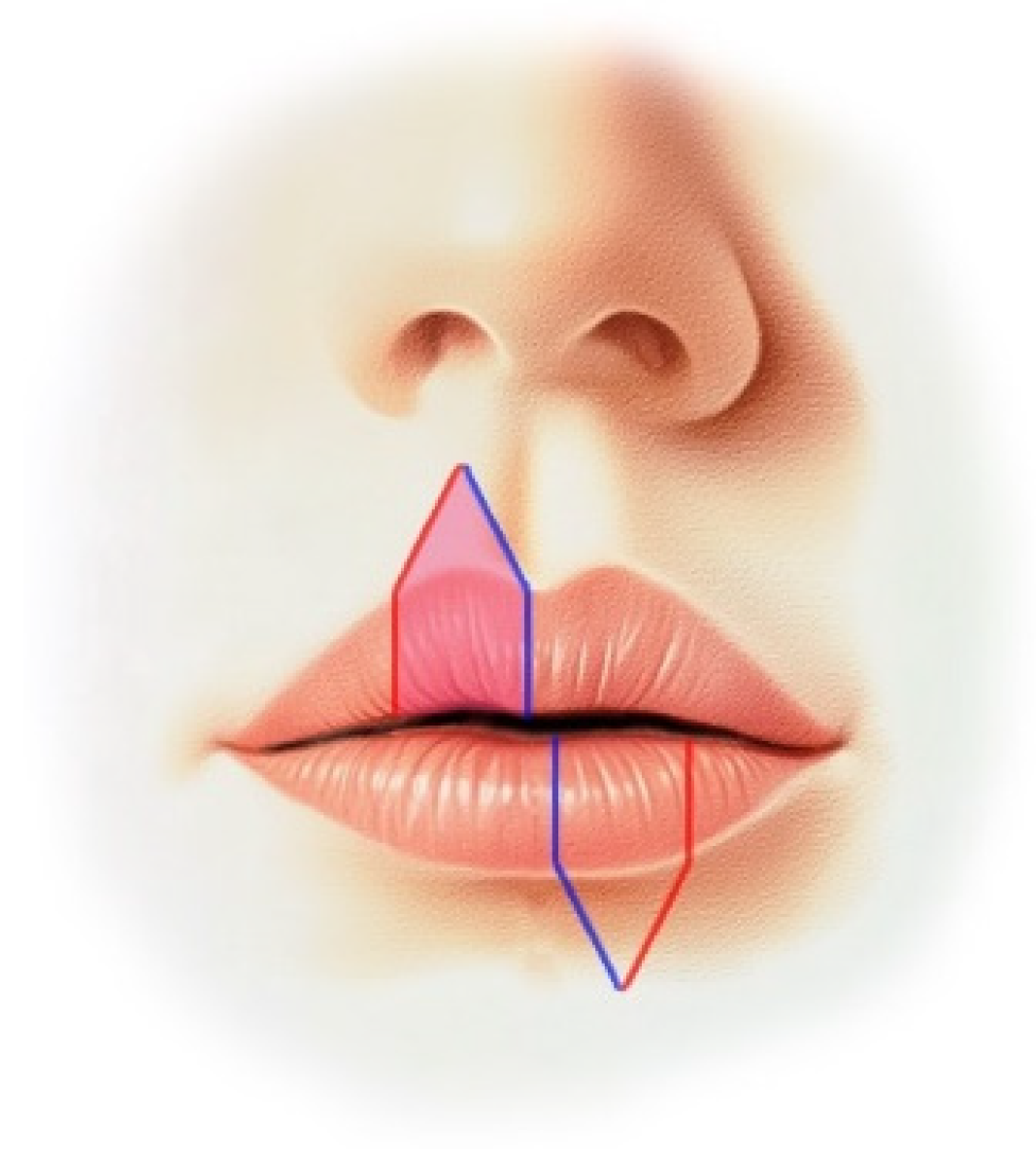
- Abbe flap design: the flap should be designed to minimize the length mismatch between the lips, with a width of half the defect’s width and a height equal to the defect’s height.
- Harvesting technique: harvesting a flap from the other lip on the opposite side of the defect is recommended to effectively reduce lip asymmetry.
- Flap preservation: the Abbe flap must be harvested with the full thickness of the lip tissue, ensuring the preservation of the labial artery, which branches from the facial artery.
- The combination of flaps: combining the Abbe flap with a staircase flap may be particularly advantageous for patients with defects comprising more than two-thirds of the lower lip, excluding the commissure.
- Revision surgery: revision surgery may be necessary for minor corrections to achieve maximum aesthetic results, typically performed 3–6 months after initial surgery.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ryu, D.M. Textbook of Maxillofacial Plastic & Reconstructive Surgery, 3rd ed.; Koonja: Paju, Republic of Korea, 2016. [Google Scholar]
- Agostini, T.; Spinelli, G.; Arcuri, F.; Perello, R. Metastatic Squamous Cell Carcinoma of the Lower Lip: Analysis of the 5-Year Survival Rate. Arch. Craniofac. Surg. 2017, 18, 105–111. [Google Scholar] [CrossRef]
- Brodland, D.G.; Zitelli, J.A. Surgical margins for excision of primary cutaneous squamous cell carcinoma. J. Am. Acad. Dermatol. 1992, 27 Pt 1, 241–248. [Google Scholar] [CrossRef]
- Salgarelli, A.C.; Sartorelli, F.; Cangiano, A.; Collini, M. Treatment of lower lip cancer: An experience of 48 cases. Int. J. Oral Maxillofac. Surg. 2005, 34, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Roldan, J.C.; Schulte-Mattler, W. Stein’s Double Cross-Lip Flaps Combined with Johanson’s Step Technique for Subtotal Lower Lip Reconstruction. Plast. Reconstr. Surg. Glob. Open 2016, 4, e615. [Google Scholar] [CrossRef]
- Karapandzic, M. Reconstruction of lip defects by local arterial flaps. Br. J. Plast. Surg. 1974, 27, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Abbe, R. A new plastic operation for the relief of deformity due to double harelip. Plast. Reconstr. Surg. 1968, 42, 481–483. [Google Scholar]
- Johanson, B.; Aspelund, E.; Breine, U.; Holmstrom, H. Surgical treatment of non-traumatic lower lip lesions with special reference to the step technique. A follow-up on 149 patients. Scand. J. Plast. Reconstr. Surg. 1974, 8, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Estlander, J.A. Eine Methode aus der einen Lippe Substanzverluste der anderen zu ersetzen. Arch. Klin. Chir. 1872, 14, 622. [Google Scholar]
- Gillies, H.D.; Millard, D.R. The Principles and Art of Plastic Surgery, 1st ed.; Little: Boston, MA, USA, 1957. [Google Scholar]
- McGregor, I.A. Reconstruction of the lower lip. Br. J. Plast. Surg. 1983, 36, 40–47. [Google Scholar] [CrossRef]
- Bernard, C. Cancer of the lower lip: Restoration with the help of quadrilateral-lateral flaps. Scalpel 1852, 5, 162–164. [Google Scholar]
- Webster, R.C.; Coffey, R.J.; Kelleher, R.E. Total and partial reconstruction of the lower lip with innervated musclebearing flaps. Plast. Reconstr. Surg. Transpl. Bull. 1960, 25, 360–371. [Google Scholar] [CrossRef]
- Jackson, L.T. Local Flaps in Head and Neck Reconstruction; Mosby Company: St. Louis, MO, USA, 1985. [Google Scholar]
- Anvar, B.A.; Evans, B.C.D.; Evans, G.R.D. Lip reconstruction. Plast. Reconstr. Surg. 2007, 120, 57e–64e. [Google Scholar] [CrossRef] [PubMed]
- Burget, G.C.; Menick, F.J. Aesthetic restoration of one-half the upper lip. Plast. Reconstr. Surg. 1986, 78, 583–593. [Google Scholar] [CrossRef]
- Smith, J.W. The anatomical and physiologic acclimatization of tissue transplanted by the lip switch technique. Plast. Reconstr. Surg. Transpl. Bull. 1960, 26, 40–56. [Google Scholar] [CrossRef]
- McCarn, K.E.; Park, S.S. Lip reconstruction. Otolaryngol. Clin. N. Am. 2007, 40, 361–380. [Google Scholar] [CrossRef]
- Earley, M.J. Peri-alar skin excision and lip advancement in the closure of lip defects. Br. J. Plast. Surg. 1984, 37, 50–51. [Google Scholar] [CrossRef]
- Ethunandan, M.; Macpherson, D.W.; Santhanam, V. Karapandzic flap for reconstruction of lip defects. J. Oral Maxillofac. Surg. 2007, 65, 2512–2517. [Google Scholar] [CrossRef]
- Gonzalez, A.; Etchichury, D. Reconstruction of Large Defects of the Lower Lip After Mohs Surgery: The Use of Combined Karapandzic and Abbe Flaps. Ann. Plast. Surg. 2018, 81, 433–437. [Google Scholar] [CrossRef]
- Salgarelli, A.C.; Sartorelli, F.; Cangiano, A.; Pagani, R.; Collini, M. Surgical treatment of lip cancer: Our experience with 106 cases. J. Oral Maxillofac. Surg. 2009, 67, 840–845. [Google Scholar] [CrossRef]
- Campos, M.A.; Varela, P.; Marques, C. Near-total lower lip reconstruction: Combined Karapandzic and Bernard-Burrow-Webster flap. Acta Dermatovenerol. Alp. Pannonica Adriat. 2017, 26, 19–20. [Google Scholar]
- Grinsell, D.; Herle, P. Composite pronator quadratus: Radial forearm free flap in functional lip reconstruction. ANZ J. Surg. 2019, 89, 940–944. [Google Scholar] [CrossRef] [PubMed]
- Daya, M.; Nair, V. Free radial forearm flap lip reconstruction: A clinical series and case reports of technical refinements. Ann. Plast. Surg. 2009, 62, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Keskin, M.; Sutcu, M.; Tosun, Z.; Savaci, N. Reconstruction of total lower lip defects using radial forearm free flap with subsequent tongue flap. J. Craniofac. Surg. 2010, 21, 349–351. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kweon, H.; Kim, H.; Park, S.; Choi, E.; Fang, Y.; Lee, C. The Establishment of a Treatment Protocol for the Reconstruction of Mid-Sized Defects in Lip Cancer Using Combinations with the Abbe Flap. J. Clin. Med. 2025, 14, 2343. https://doi.org/10.3390/jcm14072343
Kweon H, Kim H, Park S, Choi E, Fang Y, Lee C. The Establishment of a Treatment Protocol for the Reconstruction of Mid-Sized Defects in Lip Cancer Using Combinations with the Abbe Flap. Journal of Clinical Medicine. 2025; 14(7):2343. https://doi.org/10.3390/jcm14072343
Chicago/Turabian StyleKweon, Hyungjin, Hyunjoong Kim, Seoyeon Park, Euitae Choi, Yiqin Fang, and Chunui Lee. 2025. "The Establishment of a Treatment Protocol for the Reconstruction of Mid-Sized Defects in Lip Cancer Using Combinations with the Abbe Flap" Journal of Clinical Medicine 14, no. 7: 2343. https://doi.org/10.3390/jcm14072343
APA StyleKweon, H., Kim, H., Park, S., Choi, E., Fang, Y., & Lee, C. (2025). The Establishment of a Treatment Protocol for the Reconstruction of Mid-Sized Defects in Lip Cancer Using Combinations with the Abbe Flap. Journal of Clinical Medicine, 14(7), 2343. https://doi.org/10.3390/jcm14072343