
Clinical Outcomes of Rotational Atherectomy in the Drug-Eluting Stent Era


Abstract
1. Introduction
2. Basic Principles of RA
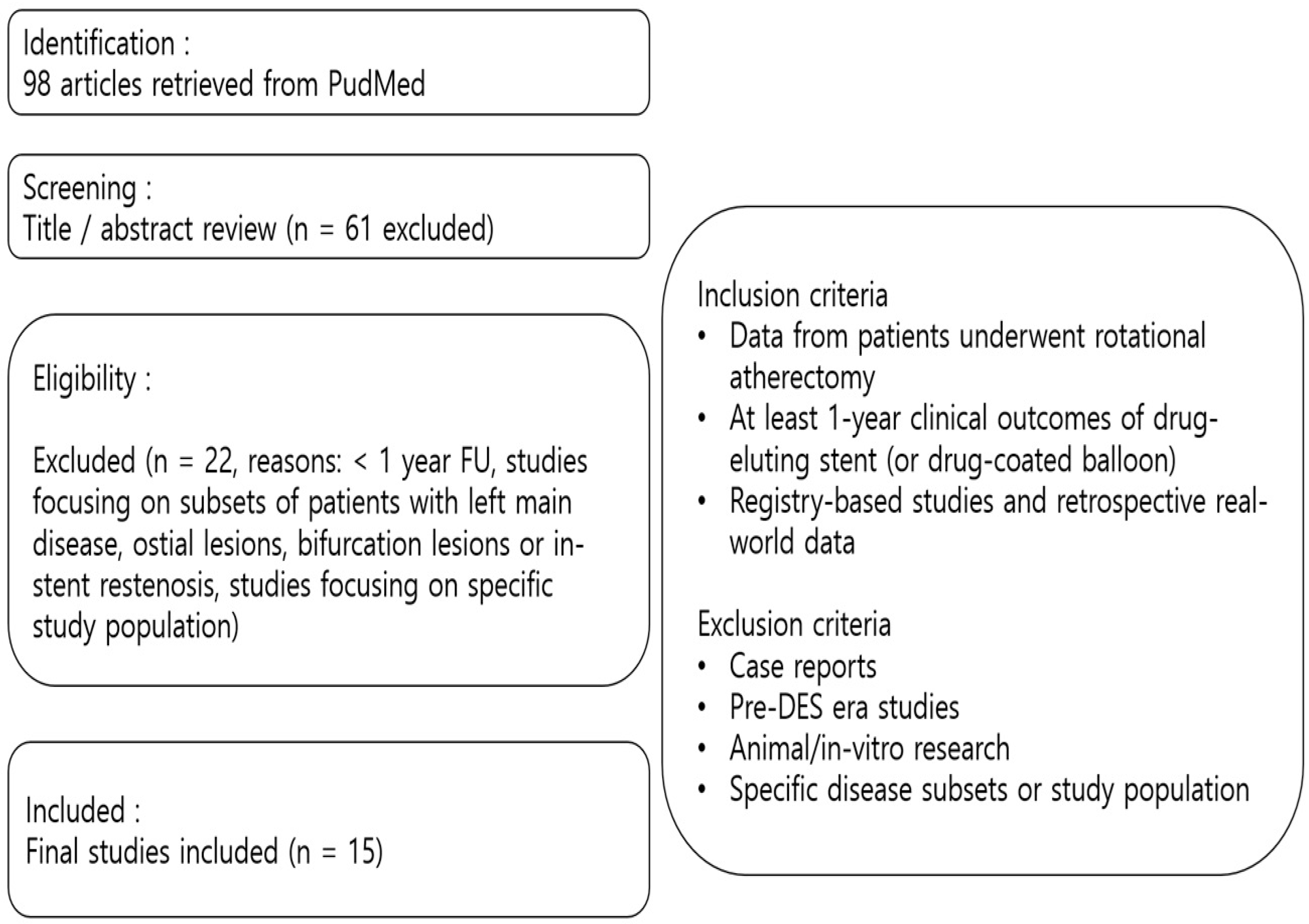
3. Methodology
4. Clinical Outcomes of RA Treated with DES (Early-Generation DES Versus New-Generation DES)
4.1. Clinical Impact of CAC During Procedure and on Long-Term Outcomes
4.2. Clinical Performance of EG-DES and NG-DES in CAC Lesions
4.3. Clinical Evidences of RA Treated with NG-DES
5. Studies Comparing Biodegradable Polymer Versus Durable Polymer DES After RA
5.1. Clinical Evidences of BP-DES and DP-DES in CAC Lesions
5.2. Clinical Evidences of BP-DES and DP-DES After RA
6. Clinical Impact of RA in CTO
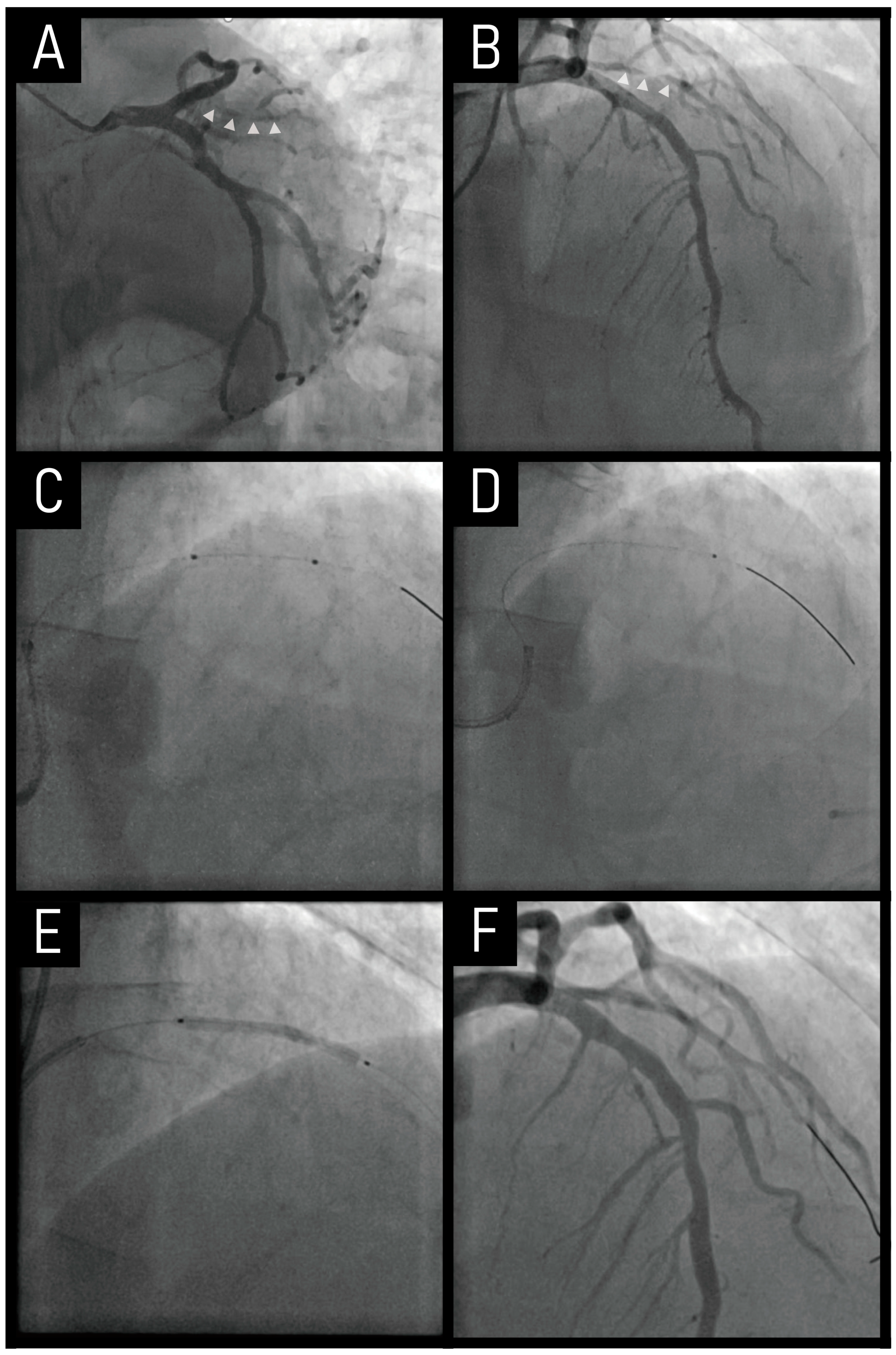
6.1. Case
6.2. Prevalence of Calcification in CTO Lesions
6.3. Clinical Usefullness of RA in CTO Lesions
6.4. Clinical Outcomes of RA in CTO Lesions
7. RA Co-Treated with Drug-Coated Balloon
7.1. Case
7.2. Clinical Evidences of Drug-Coated Balloon in De Novo Small Coronary Vessels
7.3. Clinical Outcomes of RA Co-Treated with Drug-Coated Balloon in De Novo Small Vessel Coronary Lesions
8. Discussion and Future Direction
Limitations
9. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAD | coronary artery disease |
| DES | drug-eluting stent(s) |
| MACE | major adverse cardiac event |
| MI | myocardial infarction |
| PCI | percutaneous coronary intervention |
| RA | rotational atherectomy |
| TVF | target-vessel failure |
| TVR | target-vessel revascularization |
References
- Grüntzig, A.R.; Senning, A.; Siegenthaler, W.E. Nonoperative dilatation of coronary-artery stenosis: Percutaneous transluminal coronary angioplasty. N. Engl. J. Med. 1979, 301, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Gertz, S.D.; Malekzadeh, S.; Dollar, A.L.; Kragel, A.H.; Roberts, W.C. Composition of atherosclerotic plaques in the four major epicardial coronary arteries in patients greater than or equal to 90 years of age. Am. J. Cardiol. 1991, 67, 1228–1233. [Google Scholar] [CrossRef] [PubMed]
- Waller, B.F.; Roberts, W.C. Cardiovascular disease in the very elderly. Analysis of 40 necropsy patients aged 90 years or over. Am. J. Cardiol. 1983, 51, 403–421. [Google Scholar] [CrossRef]
- Guedeney, P.; Claessen, B.E.; Mehran, R.; Mintz, G.S.; Liu, M.; Sorrentino, S.; Giustino, G.; Farhan, S.; Leon, M.B.; Serruys, P.W.; et al. Coronary Calcification and Long-Term Outcomes According to Drug-Eluting Stent Generation. JACC Cardiovasc. Interv. 2020, 13, 1417–1428. [Google Scholar] [CrossRef]
- Okai, I.; Dohi, T.; Okazaki, S.; Jujo, K.; Nakashima, M.; Otsuki, H.; Tanaka, K.; Arashi, H.; Okabe, R.; Nagura, F.; et al. Clinical Characteristics and Long-Term Outcomes of Rotational Atherectomy-J2T Multicenter Registry. Circ. J. 2018, 82, 369–375. [Google Scholar] [CrossRef]
- Allali, A.; Abdel-Wahab, M.; Elbasha, K.; Mankerious, N.; Traboulsi, H.; Kastrati, A.; El-Mawardy, M.; Hemetsberger, R.; Sulimov, D.S.; Neumann, F.J.; et al. Rotational atherectomy of calcified coronary lesions: Current practice and insights from two randomized trials. Clin. Res. Cardiol. 2023, 112, 1143–1163. [Google Scholar] [CrossRef]
- Pagnotta, P.; Briguori, C.; Mango, R.; Visconti, G.; Focaccio, A.; Belli, G.; Presbitero, P. Rotational atherectomy in resistant chronic total occlusions. Catheter. Cardiovasc. Interv. 2010, 76, 366–371. [Google Scholar] [CrossRef]
- Huang, W.C.; Teng, H.I.; Chan, W.L.; Lu, T.M. Short-term and long-term clinical outcomes of rotational atherectomy in resistant chronic total occlusion. J. Interv. Cardiol. 2018, 31, 458–464. [Google Scholar] [CrossRef]
- Généreux, P.; Madhavan, M.V.; Mintz, G.S.; Maehara, A.; Palmerini, T.; Lasalle, L.; Xu, K.; McAndrew, T.; Kirtane, A.; Lansky, A.J.; et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) TRIALS. J. Am. Coll. Cardiol. 2014, 63, 1845–1854. [Google Scholar] [CrossRef]
- Madhavan, M.V.; Tarigopula, M.; Mintz, G.S.; Maehara, A.; Stone, G.W.; Généreux, P. Coronary artery calcification: Pathogenesis and prognostic implications. J. Am. Coll. Cardiol. 2014, 63, 1703–1714. [Google Scholar] [CrossRef]
- Vliegenthart, R.; Oudkerk, M.; Hofman, A.; Oei, H.H.; van Dijck, W.; van Rooij, F.J.; Witteman, J.C. Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation 2005, 112, 572–577. [Google Scholar] [CrossRef]
- Hemetsberger, R.; Abdelghani, M.; Toelg, R.; Mankerious, N.; Allali, A.; Garcia-Garcia, H.M.; Windecker, S.; Lefèvre, T.; Saito, S.; Slagboom, T.; et al. Impact of Coronary Calcification on Clinical Outcomes After Implantation of Newer-Generation Drug-Eluting Stents. J. Am. Heart Assoc. 2021, 10, e019815. [Google Scholar] [CrossRef]
- Sangiorgi, G.; Rumberger, J.A.; Severson, A.; Edwards, W.D.; Gregoire, J.; Fitzpatrick, L.A.; Schwartz, R.S. Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: A histologic study of 723 coronary artery segments using nondecalcifying methodology. J. Am. Coll. Cardiol. 1998, 31, 126–133. [Google Scholar] [CrossRef]
- Kelly-Arnold, A.; Maldonado, N.; Laudier, D.; Aikawa, E.; Cardoso, L.; Weinbaum, S. Revised microcalcification hypothesis for fibrous cap rupture in human coronary arteries. Proc. Natl. Acad. Sci. USA 2013, 110, 10741–10746. [Google Scholar] [CrossRef]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Farb, A.; Schwartz, S.M. Lessons from sudden coronary death: A comprehensive morphological classification scheme for atherosclerotic lesions. Arter. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef]
- Wiemer, M.; Butz, T.; Schmidt, W.; Schmitz, K.P.; Horstkotte, D.; Langer, C. Scanning electron microscopic analysis of different drug eluting stents after failed implantation: From nearly undamaged to major damaged polymers. Catheter. Cardiovasc. Interv. 2010, 75, 905–911. [Google Scholar] [CrossRef]
- Barath, P.; Fishbein, M.C.; Vari, S.; Forrester, J.S. Cutting balloon: A novel approach to percutaneous angioplasty. Am. J. Cardiol. 1991, 68, 1249–1252. [Google Scholar] [CrossRef]
- Kawaguchi, R.; Tsurugaya, H.; Hoshizaki, H.; Toyama, T.; Oshima, S.; Taniguchi, K. Impact of lesion calcification on clinical and angiographic outcome after sirolimus-eluting stent implantation in real-world patients. Cardiovasc. Revasc. Med. 2008, 9, 2–8. [Google Scholar] [CrossRef]
- Bourantas, C.V.; Zhang, Y.J.; Garg, S.; Iqbal, J.; Valgimigli, M.; Windecker, S.; Mohr, F.W.; Silber, S.; Vries, T.; Onuma, Y.; et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: A patient-level pooled analysis of 7 contemporary stent trials. Heart 2014, 100, 1158–1164. [Google Scholar] [CrossRef]
- Choi, K.H.; Song, Y.B.; Lee, J.M.; Lee, S.Y.; Park, T.K.; Yang, J.H.; Choi, J.H.; Choi, S.H.; Gwon, H.C.; Hahn, J.Y. Impact of Intravascular Ultrasound-Guided Percutaneous Coronary Intervention on Long-Term Clinical Outcomes in Patients Undergoing Complex Procedures. JACC Cardiovasc. Interv. 2019, 12, 607–620. [Google Scholar] [CrossRef]
- Lee, K.; Jung, J.H.; Lee, M.; Kim, D.W.; Park, M.W.; Choi, I.J.; Lee, J.H.; Lee, J.H.; Lee, S.R.; Lee, P.H.; et al. Clinical Outcome of Rotational Atherectomy in Calcified Lesions in Korea-ROCK Registry. Medicina 2021, 57, 694. [Google Scholar] [CrossRef]
- Jinnouchi, H.; Kuramitsu, S.; Shinozaki, T.; Kobayashi, Y.; Hiromasa, T.; Morinaga, T.; Mazaki, T.; Sakakura, K.; Soga, Y.; Hyodo, M.; et al. Two-Year Clinical Outcomes of Newer-Generation Drug-Eluting Stent Implantation Following Rotational Atherectomy for Heavily Calcified Lesions. Circ. J. 2015, 79, 1938–1943. [Google Scholar] [CrossRef]
- Hachinohe, D.; Kashima, Y.; Kanno, D.; Kobayashi, K.; Sugie, T.; Kaneko, U.; Tadano, Y.; Watanabe, T.; Shitan, H.; Fujita, T. Rotational atherectomy and new-generation drug-eluting stent implantation. Catheter. Cardiovasc. Interv. 2018, 91, 1026–1034. [Google Scholar] [CrossRef]
- Kawamoto, H.; Latib, A.; Ruparelia, N.; Ielasi, A.; D’Ascenzo, F.; Pennacchi, M.; Sardella, G.; Garbo, R.; Meliga, E.; Moretti, C.; et al. In-hospital and midterm clinical outcomes of rotational atherectomy followed by stent implantation: The ROTATE multicentre registry. EuroIntervention 2016, 12, 1448–1456. [Google Scholar] [CrossRef]
- Allali, A.; Holy, E.W.; Sulimov, D.S.; Toelg, R.; Richardt, G.; Abdel-Wahab, M. Long-Term Clinical Outcome of Early Generation Versus New-Generation Drug-Eluting Stents in 481 Patients Undergoing Rotational Atherectomy: A Retrospective Analysis. Cardiol. Ther. 2018, 7, 89–99. [Google Scholar] [CrossRef]
- Buiten, R.A.; Ploumen, E.H.; Zocca, P.; Doggen, C.J.M.; van Houwelingen, K.G.; Danse, P.W.; Schotborgh, C.E.; Stoel, M.G.; Scholte, M.; Linssen, G.C.M.; et al. Three contemporary thin-strut drug-eluting stents implanted in severely calcified coronary lesions of participants in a randomized all-comers trial. Catheter. Cardiovasc. Interv. 2020, 96, E508–E515. [Google Scholar] [CrossRef]
- Mankerious, N.; Hemetsberger, R.; Traboulsi, H.; Toelg, R.; Abdel-Wahab, M.; Richardt, G.; Allali, A. Outcomes of patients treated with a biodegradable-polymer sirolimus-eluting stent versus durable-polymer everolimus-eluting stents after rotational atherectomy. Clin. Res. Cardiol. 2021, 110, 1574–1585. [Google Scholar] [CrossRef]
- Kim, K.A.; Her, S.H.; Lee, K.; Choi, I.J.; Lee, J.H.; Lee, J.H.; Lee, S.R.; Lee, P.H.; Lee, S.W.; Yoo, K.D.; et al. Clinical Outcomes of Biodegradable versus Durable Polymer Drug Eluting Stents in Rotational Atherectomy: Results from ROCK Registry. J. Clin. Med. 2022, 11, 6251. [Google Scholar] [CrossRef]
- Sakakura, K.; Nakano, M.; Otsuka, F.; Yahagi, K.; Kutys, R.; Ladich, E.; Finn, A.V.; Kolodgie, F.D.; Virmani, R. Comparison of pathology of chronic total occlusion with and without coronary artery bypass graft. Eur. Heart J. 2014, 35, 1683–1693. [Google Scholar] [CrossRef]
- Guo, J.; Maehara, A.; Mintz, G.S.; Ashida, K.; Pu, J.; Shang, Y.; Leon, M.B.; Stone, G.W.; Moses, J.W.; Ochiai, M. A virtual histology intravascular ultrasound analysis of coronary chronic total occlusions. Catheter. Cardiovasc. Interv. 2013, 81, 464–470. [Google Scholar] [CrossRef]
- Karacsonyi, J.; Karmpaliotis, D.; Alaswad, K.; Jaffer, F.A.; Yeh, R.W.; Patel, M.; Mahmud, E.; Lombardi, W.; Wyman, M.R.; Doing, A.; et al. Impact of Calcium on Chronic Total Occlusion Percutaneous Coronary Interventions. Am. J. Cardiol. 2017, 120, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Danek, B.A.; Karatasakis, A.; Karmpaliotis, D.; Alaswad, K.; Yeh, R.W.; Jaffer, F.A.; Patel, M.P.; Mahmud, E.; Lombardi, W.L.; Wyman, M.R.; et al. Development and Validation of a Scoring System for Predicting Periprocedural Complications During Percutaneous Coronary Interventions of Chronic Total Occlusions: The Prospective Global Registry for the Study of Chronic Total Occlusion Intervention (PROGRESS CTO) Complications Score. J. Am. Heart Assoc. 2016, 5, e004272. [Google Scholar] [CrossRef] [PubMed]
- Okamura, A.; Yamane, M.; Muto, M.; Matsubara, T.; Igarashi, Y.; Nakamura, S.; Muramatsu, T.; Fujita, T.; Oida, A.; Tsuchikane, E. Complications during retrograde approach for chronic coronary total occlusion: Sub-analysis of Japanese multicenter registry. Catheter. Cardiovasc. Interv. 2016, 88, 7–14. [Google Scholar] [CrossRef]
- Morino, Y.; Abe, M.; Morimoto, T.; Kimura, T.; Hayashi, Y.; Muramatsu, T.; Ochiai, M.; Noguchi, Y.; Kato, K.; Shibata, Y.; et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: The J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc. Interv. 2011, 4, 213–221. [Google Scholar] [CrossRef]
- Szijgyarto, Z.; Rampat, R.; Werner, G.S.; Ho, C.; Reifart, N.; Lefevre, T.; Louvard, Y.; Avran, A.; Kambis, M.; Buettner, H.J.; et al. Derivation and Validation of a Chronic Total Coronary Occlusion Intervention Procedural Success Score From the 20,000-Patient EuroCTO Registry: The EuroCTO (CASTLE) Score. JACC Cardiovasc. Interv. 2019, 12, 335–342. [Google Scholar] [CrossRef]
- Cosgrove, C.; Mahadevan, K.; Spratt, J.C.; McEntegart, M. The Impact of Calcium on Chronic Total Occlusion Management. Interv. Cardiol. 2021, 16, e30. [Google Scholar] [CrossRef]
- Fujii, K.; Carlier, S.G.; Mintz, G.S.; Yang, Y.M.; Moussa, I.; Weisz, G.; Dangas, G.; Mehran, R.; Lansky, A.J.; Kreps, E.M.; et al. Stent underexpansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation: An intravascular ultrasound study. J. Am. Coll. Cardiol. 2005, 45, 995–998. [Google Scholar] [CrossRef]
- Doi, H.; Maehara, A.; Mintz, G.S.; Yu, A.; Wang, H.; Mandinov, L.; Popma, J.J.; Ellis, S.G.; Grube, E.; Dawkins, K.D.; et al. Impact of post-intervention minimal stent area on 9-month follow-up patency of paclitaxel-eluting stents: An integrated intravascular ultrasound analysis from the TAXUS IV, V, and VI and TAXUS ATLAS Workhorse, Long Lesion, and Direct Stent Trials. JACC Cardiovasc. Interv. 2009, 2, 1269–1275. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011, 124, e574–e651. [Google Scholar] [CrossRef]
- Moussa, I.; Di Mario, C.; Moses, J.; Reimers, B.; Di Francesco, L.; Martini, G.; Tobis, J.; Colombo, A. Coronary stenting after rotational atherectomy in calcified and complex lesions. Angiogr. Clin. Follow-Up Results. Circ. 1997, 96, 128–136. [Google Scholar] [CrossRef]
- Abdel-Wahab, M.; Richardt, G.; Joachim Büttner, H.; Toelg, R.; Geist, V.; Meinertz, T.; Schofer, J.; King, L.; Neumann, F.J.; Khattab, A.A. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: The randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc. Interv. 2013, 6, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.; Toelg, R.; Byrne, R.A.; Geist, V.; El-Mawardy, M.; Allali, A.; Rheude, T.; Robinson, D.R.; Abdelghani, M.; Sulimov, D.S.; et al. High-Speed Rotational Atherectomy Versus Modified Balloons Prior to Drug-Eluting Stent Implantation in Severely Calcified Coronary Lesions. Circ. Cardiovasc. Interv. 2018, 11, e007415. [Google Scholar] [CrossRef] [PubMed]
- Gruberg, L.; Mehran, R.; Dangas, G.; Hong, M.K.; Mintz, G.S.; Kornowski, R.; Lansky, A.J.; Kent, K.M.; Pichard, A.D.; Satler, L.F.; et al. Effect of plaque debulking and stenting on short- and long-term outcomes after revascularization of chronic total occlusions. J. Am. Coll. Cardiol. 2000, 35, 151–156. [Google Scholar] [CrossRef]
- Moliterno, D.J. Rotational atherectomy for resistant chronic total occlusions: Another spin for tough old problems. Catheter. Cardiovasc. Interv. 2010, 76, 372–373. [Google Scholar] [CrossRef]
- Barbato, E.; Carrié, D.; Dardas, P.; Fajadet, J.; Gaul, G.; Haude, M.; Khashaba, A.; Koch, K.; Meyer-Gessner, M.; Palazuelos, J.; et al. European expert consensus on rotational atherectomy. EuroIntervention 2015, 11, 30–36. [Google Scholar] [CrossRef]
- Lee, S.N.; Her, S.H.; Jang, W.Y.; Moon, D.; Moon, K.W.; Yoo, K.D.; Lee, K.; Choi, I.J.; Lee, J.H.; Lee, J.H.; et al. Impact of chronic total occlusion lesions on clinical outcomes in patients receiving rotational atherectomy: Results from the ROCK registry. Heart Vessel. 2021, 36, 1617–1625. [Google Scholar] [CrossRef]
- Ayoub, M.; Corpataux, N.; Behnes, M.; Schupp, T.; Forner, J.; Akin, I.; Neumann, F.J.; Westermann, D.; Rudolph, V.; Mashayekhi, K. Safety and Efficiency of Rotational Atherectomy in Chronic Total Coronary Occlusion-One-Year Clinical Outcomes of an Observational Registry. J. Clin. Med. 2023, 12, 3510. [Google Scholar] [CrossRef]
- Azzalini, L.; Dautov, R.; Ojeda, S.; Serra, A.; Benincasa, S.; Bellini, B.; Giannini, F.; Chavarría, J.; Gheorghe, L.L.; Pan, M.; et al. Long-term outcomes of rotational atherectomy for the percutaneous treatment of chronic total occlusions. Catheter. Cardiovasc. Interv. 2017, 89, 820–828. [Google Scholar] [CrossRef]
- Sandoval, Y.; Brilakis, E.S. The role of rotational atherectomy in contemporary chronic total occlusion percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2017, 89, 829–831. [Google Scholar] [CrossRef]
- Abdelaziz, A.; Elsayed, H.; Hamdaalah, A.; Atta, K.; Mechi, A.; Kadhim, H.; Aboutaleb, A.M.; Elaraby, A.; Ellabban, M.H.; Rzk, F.M.; et al. Safety and feasibility of rotational atherectomy (RA) versus conventional stenting in patients with chronic total occlusion (CTO) lesions: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2024, 24, 4. [Google Scholar] [CrossRef]
- Jeger, R.V.; Farah, A.; Ohlow, M.A.; Mangner, N.; Möbius-Winkler, S.; Weilenmann, D.; Wöhrle, J.; Stachel, G.; Markovic, S.; Leibundgut, G.; et al. Long-term efficacy and safety of drug-coated balloons versus drug-eluting stents for small coronary artery disease (BASKET-SMALL 2): 3-year follow-up of a randomised, non-inferiority trial. Lancet 2020, 396, 1504–1510. [Google Scholar] [CrossRef]
- Latib, A.; Colombo, A.; Castriota, F.; Micari, A.; Cremonesi, A.; De Felice, F.; Marchese, A.; Tespili, M.; Presbitero, P.; Sgueglia, G.A.; et al. A randomized multicenter study comparing a paclitaxel drug-eluting balloon with a paclitaxel-eluting stent in small coronary vessels: The BELLO (Balloon Elution and Late Loss Optimization) study. J. Am. Coll. Cardiol. 2012, 60, 2473–2480. [Google Scholar] [CrossRef] [PubMed]
- Latib, A.; Ruparelia, N.; Menozzi, A.; Castriota, F.; Micari, A.; Cremonesi, A.; De Felice, F.; Marchese, A.; Tespili, M.; Presbitero, P.; et al. 3-Year Follow-Up of the Balloon Elution and Late Loss Optimization Study (BELLO). JACC Cardiovasc. Interv. 2015, 8, 1132–1134. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Qiao, S.; Su, X.; Chen, Y.; Jin, Z.; Chen, H.; Xu, B.; Kong, X.; Pang, W.; Liu, Y.; et al. Drug-Coated Balloon Versus Drug-Eluting Stent for Small-Vessel Disease: The RESTORE SVD China Randomized Trial. JACC Cardiovasc. Interv. 2018, 11, 2381–2392. [Google Scholar] [CrossRef] [PubMed]
- Jeger, R.V.; Farah, A.; Ohlow, M.A.; Mangner, N.; Möbius-Winkler, S.; Leibundgut, G.; Weilenmann, D.; Wöhrle, J.; Richter, S.; Schreiber, M.; et al. Drug-coated balloons for small coronary artery disease (BASKET-SMALL 2): An open-label randomised non-inferiority trial. Lancet 2018, 392, 849–856. [Google Scholar] [CrossRef]
- Cortese, B.; Di Palma, G.; Guimaraes, M.G.; Piraino, D.; Orrego, P.S.; Buccheri, D.; Rivero, F.; Perotto, A.; Zambelli, G.; Alfonso, F. Drug-Coated Balloon Versus Drug-Eluting Stent for Small Coronary Vessel Disease: PICCOLETO II Randomized Clinical Trial. JACC Cardiovasc. Interv. 2020, 13, 2840–2849. [Google Scholar] [CrossRef]
- Mitsui, K.; Lee, T.; Miyazaki, R.; Hara, N.; Nagamine, S.; Nakamura, T.; Terui, M.; Okata, S.; Nagase, M.; Nitta, G.; et al. Drug-coated balloon strategy following orbital atherectomy for calcified coronary artery compared with drug-eluting stent: One-year outcomes and optical coherence tomography assessment. Catheter. Cardiovasc. Interv. 2023, 102, 11–17. [Google Scholar] [CrossRef]
- Ito, R.; Ueno, K.; Yoshida, T.; Takahashi, H.; Tatsumi, T.; Hashimoto, Y.; Kojima, Y.; Kitamura, T.; Morita, N. Outcomes after drug-coated balloon treatment for patients with calcified coronary lesions. J. Interv. Cardiol. 2018, 31, 436–441. [Google Scholar] [CrossRef]
- Nagai, T.; Mizobuchi, M.; Funatsu, A.; Kobayashi, T.; Nakamura, S. Acute and mid-term outcomes of drug-coated balloon following rotational atherectomy. Cardiovasc. Interv. Ther. 2020, 35, 242–249. [Google Scholar] [CrossRef]
- Dong, H.; Shan, Y.; Gong, S.; Li, R.; Li, Y.; Lu, X.; Sun, G. Clinical research of drug-coated balloon after rotational atherectomy for severe coronary artery calcification. BMC Cardiovasc. Disord. 2023, 23, 40. [Google Scholar] [CrossRef]
- Kawashima, H.; Kyono, H.; Nakashima, M.; Okai, I.; Jujo, K.; Dohi, T.; Otsuki, H.; Tanaka, K.; Nagura, F.; Okazaki, S.; et al. Prognostic Impact of Scoring Balloon Angioplasty After Rotational Atherectomy in Heavily Calcified Lesions Using Second-Generation Drug-Eluting Stents: A Multicenter Registry-Based Study. Cardiovasc. Revasc Med. 2020, 21, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Torii, S.; Jinnouchi, H.; Sakamoto, A.; Mori, H.; Park, J.; Amoa, F.C.; Sawan, M.; Sato, Y.; Cornelissen, A.; Kuntz, S.H.; et al. Vascular responses to coronary calcification following implantation of newer-generation drug-eluting stents in humans: Impact on healing. Eur. Heart J. 2020, 41, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, F.; Vorpahl, M.; Nakano, M.; Foerst, J.; Newell, J.B.; Sakakura, K.; Kutys, R.; Ladich, E.; Finn, A.V.; Kolodgie, F.D.; et al. Pathology of second-generation everolimus-eluting stents versus first-generation sirolimus- and paclitaxel-eluting stents in humans. Circulation 2014, 129, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Milzi, A.; Simonetto, F.; Landi, A. Percutaneous Revascularization of Thrombotic and Calcified Coronary Lesions. J. Clin. Med. 2025, 14, 692. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur. Heart J. 2024, 45, 3415–3537. [Google Scholar] [CrossRef]
- Barbato, E.; Gallinoro, E.; Abdel-Wahab, M.; Andreini, D.; Carrié, D.; Di Mario, C.; Dudek, D.; Escaned, J.; Fajadet, J.; Guagliumi, G.; et al. Management strategies for heavily calcified coronary stenoses: An EAPCI clinical consensus statement in collaboration with the EURO4C-PCR group. Eur. Heart J. 2023, 44, 4340–4356. [Google Scholar] [CrossRef]
- Bangalore, S.; Toklu, B.; Patel, N.; Feit, F.; Stone, G.W. Newer-Generation Ultrathin Strut Drug-Eluting Stents Versus Older Second-Generation Thicker Strut Drug-Eluting Stents for Coronary Artery Disease. Circulation 2018, 138, 2216–2226. [Google Scholar] [CrossRef]
- Iglesias, J.F.; Degrauwe, S.; Cimci, M.; Chatelain, Q.; Roffi, M.; Windecker, S.; Pilgrim, T. Differential Effects of Newer-Generation Ultrathin-Strut Versus Thicker-Strut Drug-Eluting Stents in Chronic and Acute Coronary Syndromes. JACC Cardiovasc. Interv. 2021, 14, 2461–2473. [Google Scholar] [CrossRef]
- Pilgrim, T.; Heg, D.; Roffi, M.; Tüller, D.; Muller, O.; Vuilliomenet, A.; Cook, S.; Weilenmann, D.; Kaiser, C.; Jamshidi, P.; et al. Ultrathin strut biodegradable polymer sirolimus-eluting stent versus durable polymer everolimus-eluting stent for percutaneous coronary revascularisation (BIOSCIENCE): A randomised, single-blind, non-inferiority trial. Lancet 2014, 384, 2111–2122. [Google Scholar] [CrossRef]
- von Birgelen, C.; Zocca, P.; Buiten, R.A.; Jessurun, G.A.J.; Schotborgh, C.E.; Roguin, A.; Danse, P.W.; Benit, E.; Aminian, A.; van Houwelingen, K.G.; et al. Thin composite wire strut, durable polymer-coated (Resolute Onyx) versus ultrathin cobalt-chromium strut, bioresorbable polymer-coated (Orsiro) drug-eluting stents in allcomers with coronary artery disease (BIONYX): An international, single-blind, randomised non-inferiority trial. Lancet 2018, 392, 1235–1245. [Google Scholar] [CrossRef] [PubMed]
- Kandzari, D.E.; Mauri, L.; Koolen, J.J.; Massaro, J.M.; Doros, G.; Garcia-Garcia, H.M.; Bennett, J.; Roguin, A.; Gharib, E.G.; Cutlip, D.E.; et al. Ultrathin, bioresorbable polymer sirolimus-eluting stents versus thin, durable polymer everolimus-eluting stents in patients undergoing coronary revascularisation (BIOFLOW V): A randomised trial. Lancet 2017, 390, 1843–1852. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.O.; Thayssen, P.; Maeng, M.; Ravkilde, J.; Krusell, L.R.; Raungaard, B.; Junker, A.; Terkelsen, C.J.; Veien, K.T.; Villadsen, A.B.; et al. Randomized Comparison of a Biodegradable Polymer Ultrathin Strut Sirolimus-Eluting Stent With a Biodegradable Polymer Biolimus-Eluting Stent in Patients Treated With Percutaneous Coronary Intervention: The SORT OUT VII Trial. Circ. Cardiovasc. Interv. 2016, 9, e003610. [Google Scholar] [CrossRef]
- Morofuji, T.; Kuramitsu, S.; Shinozaki, T.; Jinnouchi, H.; Sonoda, S.; Domei, T.; Hyodo, M.; Shirai, S.; Ando, K. Clinical impact of calcified nodule in patients with heavily calcified lesions requiring rotational atherectomy. Catheter. Cardiovasc. Interv. 2021, 97, 10–19. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Study Population | Era | Duration | Study Period | IVUS or OCT, % | MACE, % | All-Cause Death, % | MI, % | TVR, % | TLR, % | ST, % | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lee et al. [21] | 540 | NG-DES | 1.5 years | 2010–2019 | 46.0 | 16.0 * | 8.4 | 2.1 | 9.8 | 8.2 | 1.2 |
| Kawamoto et al. [24] | 985 | 8.8% BMS | 2 years | 2002–2013 | 31.2 | 32.2 ** | 9.5 | 3.3 | 19.8 | 16.6 | 1.8 |
| 21.9% EG-DES | 19.2 ** | ||||||||||
| 69.3% NG-DES | 12.9 ** | ||||||||||
| Allali et al. [25] | 268 | 55.7% EG-DES | 2.5 years | 2002–2015 | NA | 31.1 | 13.5 | 4.9 | 17.6 | 12.7 | 0.9 |
| 44.3% NG-DES | 1.5 years | 21.1 | 8.2 | 4.1 | 12.9 | 7.9 | 2.4 | ||||
| Jinnouchi et al. [22] | 252 | NG-DES | 2 years | 2010–2012 | NA | 20.3 | 13.5 | 2.1 | 24.8 | 21.9 | 2.1 |
| Hachinohe et al. [23] | 744 | NG-DES | 1 year | 2013–2015 | 99.6 | 6.6 * | 5.5 | 0.1 | - | 2.9 | 0.1 |
| Okai et al. [5] | 1090 | 11.2% BMS | 3.8 years | 2004–2015 | 73.0 | 45.5 | 24.2 | 6.8 $ | 21.4 | 16.2 | 1.3 |
| 52.5% EG-DES | |||||||||||
| 36.3% NG-DES |
| Study Population | Stent Type | Duration | Study Period | Primary Endpoint, % | All-Cause Death, % | Cardiac Death, % | MI, % | TVR, % | TLR, % | ST, % | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mankerious et al. [27] | 285 | 42.5% BP-DES | 2 years | 2007–2018 | 10.0 * | - | 5.0 | 1.0 | - | 4.0 | 0 |
| 57.5% DP-DES | 18.0 * | - | 9.0 | 2.0 | - | 10.0 | 2.0 | ||||
| Subgroup analysis with small-stent group [27] | 168 | 40.5% BP-DES | 2 years | 2007–2018 | 3.0 | - | 2.0 | 0 | - | 2.0 | - |
| 59.5% DP-DES | 19.0 | - | 8.0 | 2.0 | - | 12.0 | - | ||||
| Kim et al. [28] | 510 | 46.7% BP-DES | 3 years | 2010–2019 | 12.2 ** | 4.7 | 3.4 | 1.3 | 10.2 | 8.5 | 1.3 |
| 53.3% DP-DES | 13.6 ** | 10.7 | 8.1 | 1.9 | 6.7 | 5.9 | 0.7 |
| Patients | Primary Endpoint, % | All-Cause Death, % | Cardiac Death, % | MI, % | TVR, % | TLR, % | ST, % | |
|---|---|---|---|---|---|---|---|---|
| Lee et al. [46] | CTO, N = 42 | 14.3 * | 4.8 | 4.8 | 0 | 9.5 | - | 0 |
| Non-CTO, N = 541 | 12.9 * | 7.8 | 5.7 | 3.3 | 7.0 | - | 1.3 | |
| Ayoub et al. [47] | RA, N = 193 | 18.7 ** | 5.7 | - | 1.0 | 18.7 | 18.1 | - |
| Without RA, N = 2596 | 16.7 ** | 3.7 | - | 1.2 | 16.3 | 14.3 | - | |
| Huang et al. [8] | RA, N = 25 | 12.0 * | - | 4.0 | 8.0 | - | 4.0 | - |
| Without RA, N = 205 | 19.5 * | - | 11.7 | 9.8 | - | 8.3 | - | |
| Azzalini et al. [48] | RA, N = 35 | 15.0 * | - | 6 | 9 | 6 | - | - |
| Without RA, N = 968 | 13.0 * | - | 3 | 3 | 9 | - | - |
| Patients | Primary Endpoint, % | All-Cause Death, % | Cardiac Death, % | MI, % | TVR, % | TLR, % | ST, % | |
| Nagai et al. [59] | 167 | - | 2 | 0 | - | 20.7 | 16.4 | - |
| Dong et al. [60] | DCB-RA, N = 57 | 12.3 * | 1.8 | - | 0 | - | 7.0 | - |
| DES-RA, N = 261 | 18.8 * | 1.5 | - | 1.2 | - | 13.8 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Lee, K.; Her, S.-H. Clinical Outcomes of Rotational Atherectomy in the Drug-Eluting Stent Era. J. Clin. Med. 2025, 14, 2199. https://doi.org/10.3390/jcm14072199
Kim Y, Lee K, Her S-H. Clinical Outcomes of Rotational Atherectomy in the Drug-Eluting Stent Era. Journal of Clinical Medicine. 2025; 14(7):2199. https://doi.org/10.3390/jcm14072199
Chicago/Turabian StyleKim, Yonghee, Kyusup Lee, and Sung-Ho Her. 2025. "Clinical Outcomes of Rotational Atherectomy in the Drug-Eluting Stent Era" Journal of Clinical Medicine 14, no. 7: 2199. https://doi.org/10.3390/jcm14072199
APA StyleKim, Y., Lee, K., & Her, S.-H. (2025). Clinical Outcomes of Rotational Atherectomy in the Drug-Eluting Stent Era. Journal of Clinical Medicine, 14(7), 2199. https://doi.org/10.3390/jcm14072199