
Sex-Related Analgesic Effects of Opioid-Based Anesthesia and Low-Opioid Anesthesia with Non-Opioid Postoperative Analgesia—A Clinical Observational Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blum, K.; Liew, L.; Dutia, A.; Aljohani, D.; Bugada, D.; Forget, P.; Nesvadba, D.S. Opioid-free anesthesia: A practical guide for teaching and implementation. Minerva Anesthesiol. 2024, 90, 300–310. [Google Scholar]
- Mulier, J.P.; Hunter, J.M.; de Boer, H.D. Seventy-five years since the birth of the Liverpool anaesthetic technique. Br. J. Anaesth. 2021, 126, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Lersch, F.; Correia, P.; Hight, D.; Kaiser, H.; Berger-Estilita, J. The nuts and bolts of multimodal anaesthesia in the 21 st century: A primer for clinicians. Curr. Opin. Anesthesiol. 2023, 36, 666–675. [Google Scholar]
- Lamperti, M.; Romero, C.; Guarracino, F.; Cammarota, G.; Vetrugno, L.; Tufegdzic, B.; Lozsan, F.; Frias, J.J.M.; Duma, A.; Bock, M.; et al. Preoperative assessment of adults undergoing elective noncardiac surgery: Updated guidelines from the European Society of Anaesthesiology and Intensive Care. Eur. J. Anaesthesiol. 2025, 42, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.N.; Pavone, K.J.; Naranjo, M. Multimodal General Anesthesia: Theory and Practice. Anesth. Analg. 2018, 127, 1246–1258. [Google Scholar] [CrossRef]
- Shanthanna, H.; Joshi, G. Opioid-free general anesthesia: Considerations, techniques, and limitations. Curr. Opin. Anesthesiol. 2024, 37, 384–390. [Google Scholar]
- Boysen, P.; Patel, J.; King, A. Brief history of opioids in perioperative and periprocedural medicine to inform the future. Ochsner J. 2023, 23, 43–49. [Google Scholar] [PubMed]
- Savoia, G.; Scibelli, G. From opioid free anesthesia to opioid free postoperative analgesia: A difficult target to reach. Minerva Anesthesiol. 2022, 88, 421–424. [Google Scholar]
- Bugada, D.; Lorini, L.; Lavand’homme, P. Opioid-free anesthesia: Evidence for short and long–term outcome. Minerva Anesthesiol. 2021, 87, 230–237. [Google Scholar]
- Feenstra, M.L.; Jansen, S.; Eshuis, W.J.; van Berge Henegouwen, M.I.; Hollmann, M.W.; Hermanides, J. Opioid-free anesthesia: A systematic review and meta-analysis. J. Clin. Anesth. 2023, 90, 111215. [Google Scholar] [CrossRef]
- Kharasch, E.; Clark, D. Opioid-free anesthesia: Time to regain our balance. Anesthesiology 2021, 134, 509–514. [Google Scholar] [PubMed]
- Chia, P.A.; Cannesson, M.; Bui, C.C.M. Opioid free anesthesia: Feasible? Curr. Opin. Anaesthesiol. 2020, 33, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Oya, R.; Ogawa, S.; Oya, K.; Hirakawa, Y.; Maeda, C.; Amaya, F. Prevalence of preoperative opioid usage and its impact on postoperative outcomes: A retrospective cohort study. J. Anesth. 2023, 37, 532–538. [Google Scholar] [CrossRef]
- Olausson, A.; Svensson, C.; Andrell, P.; Jildenstal, P.; Thorn, S.; Wolf, A. Total opioid-free general anaesthesia can improve postoperative outcomes after surgery, without evidence of adverse effects on patient safety and pain management: A systematic review and meta-analysis. Acta Anaesth. Scan. 2021, 66, 170–185. [Google Scholar]
- Baboli, K.M.; Liu, H.; Poggio, J.L. Opioid-free postoperative analgesia: Is it feasible? Curr. Probl. Surg. 2020, 57, 100794. [Google Scholar]
- Lavandhomme, P.; Estebe, J. Opioid-free anesthesia: A different regard to anesthesia practice. Curr. Opin. Anesthesiol. 2018, 31, 556–561. [Google Scholar]
- Kosciuczuk, U.; Jakubow, P.; Tarnowska, K.; Rynkiewicz-Szczepanska, E. Opioid Therapy and Implications for Oxidative Balance: A Clinical Study of Total Oxidative Capacity (TOC) and Total Antioxidative Capacity (TAC). J. Clin. Med. 2024, 13, 82. [Google Scholar] [CrossRef]
- Carcamo-Cavazos, V.; Cannesson, M. Opioid-Free Anesthesia: The Pros and Cons. Adv. Anesth. 2022, 40, 149–166. [Google Scholar] [CrossRef]
- Frauenknecht, J.; Kirkham, K.; Jacot-Guillarmod, A.; Albrecht, E. Analgesic impast of intra-operative opioids vs. Opioid-free anaesthesia: A systematic review and meta-analysis. Anaesthesia 2019, 74, 651–662. [Google Scholar]
- de Boer, H.D.; Detriche, O.; Forget, P. Opioid-related side effects: Postoperative ileus, urinary retention, nausea and vomiting, and shivering. A review of the literature. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 499–504. [Google Scholar] [CrossRef]
- Salomé, A.; Harkouk, H.; Fletcher, D.; Martinez, V. Opioid-Free Anesthesia Benefit-Risk Balance: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 2069. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, A.; Lirk, P. Multimodal Analgesia. Anesthesiol. Clin. 2022, 40, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, D.; Hill, S.; Carty, S.; Rockett, M.; Bastable, R.; Knaggs, R.; Lambert, D.; Levy, N.; Hughes, J.; Wilkinson, P. Surgery and opioids: Evidence-based expert consensus guidelines on the perioperative use of opioids in the United Kingdom. Br. J. Anaesth. 2021, 126, 1208–1216. [Google Scholar] [CrossRef]
- Rogobete, A.; Sandesc, D. General Anesthesia as multimodal individualized clinical concept. Medicina 2022, 58, 956. [Google Scholar] [CrossRef]
- Elkassabany, N.; Mariano, E. Opioid-free anaesthesia-what Gould Inigo Montoya say? Anaesthesia 2019, 74, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Hartley, R.; Leung, A.; Ronksley, P.; Jette, N.; Casha, S.; Cambrin, J. Preoperative predictors f poor acute postoperative pain control: A systematic review and meta-analysis. BMJ Open 2019, 9, e 025091. [Google Scholar] [CrossRef]
- Tighe, P.; Le-Wendling, L.; Patel, A.; Zou, B.; Fillingim, R. Clinically derived early postopeative pain trajectories differ by age, sex, and type of surgery. Pain 2015, 4, 609–617. [Google Scholar] [CrossRef]
- Forget, P. Opioid-free anaesthesia. Why and how? A contextual analysis. Anaesth. Crit. Care Pain. Med. 2019, 38, 169–172. [Google Scholar]
- Forget, P.; de Velde, M.; Pogatzki-Zahn, E. Opioid-free anaesthesia: Should we all adept it? An overview of current evidence. Eur. J. Anaesthesiol. 2023, 40, 539–541. [Google Scholar] [CrossRef]
- Veyckemans, F. Opioid-free anaesthesia: Still a debate? Eur. J. Anaesthesiol. 2019, 36, 245–246. [Google Scholar] [CrossRef]
- Ramwani, R.; Wernberg, J. The use of opioi analgesia after surgery: Assessing postoperative prescription from patient and surgeon perspective. Clin. Med. Res. 2021, 20, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Lirk, P.; Rathmell, J. Opioid-free anaesthesia. Con: It is too Elary to adept opioid-free anaesthesia today. Eur. J. Anaesthesiol. 2019, 36, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Pius, A.; Jones, E.; Bonnel, L.; Fujii, M.; MacLean, C.D. Patients experience with opioid pain medication after discharge from surgery: A mixed-methods study. J. Surg. Res. 2020, 256, 328–337. [Google Scholar]
- Egan, T. Are opioids indispensable for general anaesthesia? Br. J. Anaesth. 2019, 122, e127–e135. [Google Scholar] [CrossRef]
- Levand’homme, P. Opioid-free anaesthesia. Pro: Damned if you do not use opioids Turing burgery. Eur. J. Anaesthesiol. 2019, 36, 247–249. [Google Scholar]
- Camu, F. Why sould I change my practice of anesthesia? Opioids. Minerva Anesthesiol. 2000, 66, 268–272. [Google Scholar]
- El-Kefraoui, C.; Olleik, G.; Chay, M.A.; Kouyoumdjian, A.; Nguyen-Powanda, P.; Rajabiyazdi, F.; Fiore, J.F., Jr. Opioid versus opioid-free analgesia after surgical discharge: Protocol for a systemie review and meta-analysis. BMJ Open 2020, 10, e035443. [Google Scholar] [PubMed]
- Cuba, T.; Fassarella, C.; Camerini, F.; Henrique, D. Incidence of respiratory depression in a Postanesthesia Care Unit in patients undergoing anesthesia using opioids. J. PeriAnesthesia Nurs. 2021, 36, 36–40. [Google Scholar]
- Thota, R.S.; Ramkiran, S.; Garg, R.; Goswami, J.; Baxi, V.; Thomas, M. Opioid free onco-anesthesia: Is it time to convict opioids? A systematic review of literature. J. Anaesthesiol. Clin. Pharmacol. 2019, 35, 441–452. [Google Scholar] [CrossRef]
- Khanna, A.; Bergese, S.; Jugquist, C.; Morimatsu, H.; Uezono, S.; Lee, S.; Kah, L.; Urman, R.; Mcintyre, R.; Tornero, C.; et al. Prediction of opioid-induced respiratoy depression on inpatient wards Rusingcontinous capnography and oximetry: An international prospective, observatinaltrial. Anasth. Analg. 2020, 131, 4. [Google Scholar]
- Aguerreche, C.; Cadier, G.; Beurton, A.; Imbault, J.; Leuliet, S.; Remy, A.; Zaouter, C.; Ouattara, A. Fasibility and postoperative opioid sparing effect of an opioid-free anaesthesia in adult cardiac surgery: A retrospective study. BMC Anesthesiol. 2021, 21, 166. [Google Scholar] [CrossRef]
- Kosciuczuk, U.; Jakubow, P.; Czyzewska, J.; Knapp, P.; Rynkiewicz-Szczepanska, E. Plasma Brain-Derived Neurotrophic Factor and Opioid Therapy: Results of Pilot Cross-Sectional Study. Clin. Med. Res. 2022, 20, 195–203. [Google Scholar] [CrossRef]
- Toleska, M.; Dimitrovski, A.; Dimitrovska, N. Comparison among opioid-based, low opioid and opioid free anesthesia in colorectal oncologic surgery. Pril. (Makedon. Akad. Na Nauk. I Umet. Oddelenie Za Med. Nauk.) 2023, 44, 117–126. [Google Scholar] [CrossRef]
- Rahmani, L.; Abdelaatti, A.; Wall, T.P.; Buggy, D. Anaesthesia and cancer recurrence: The influence of perioperative anaesthetic technique on cancer recurrence after surgery. Curr. Opin. Anesthesiol. 2023, 36, 361–368. [Google Scholar] [CrossRef]
- Smith, L.; Cata, J.; Forget, P. Immunological Insights into Opioid-Free anaesthesia in oncological surgery: A scoping review. Curr. Oncol. Rep. 2022, 24, 1327–1336. [Google Scholar] [CrossRef]
- Kosciuczuk, U.; Knapp, P.; Lotowska-Cwiklewska, A.M. Opioid-induced immunosuppression and carcinogenesis promotion theories create the newest trend in acute and chronic pain pharmacotherapy. Clinics 2020, 75, e1554. [Google Scholar] [CrossRef]
- Buchanan, F.; Myles, P.; Cicuttini, F. Patient sex and its influence on general anaesthesia. Anaesth. Intensive Care 2009, 37, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, J.; Craft, R.; Leresche, L.; Nielsen, L.; Berkley, K.; Fillingim, R.; Gold, M.; Holdcroft, A.; Lautenbacher, S.; Mayer, E.A.; et al. Studying sex and gender differences in pain and analgesia: A consensus report. Pain 2007, 132, S26–S45. [Google Scholar] [CrossRef] [PubMed]
- Araujo Palmeira, C.; Ashmawi, H.; Posso, I. Sex and pain perception and analgesia. Rev. Bras. Anesthesiol. 2011, 61, 814–828. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Ho, I. Sex differences in opioid analgesia and addiction: Interactions among opioid receptors and estrogen receptors. Mol. Pain 2013, 9, 45. [Google Scholar] [CrossRef]
- Blanton, H.; Barnes, R.; McHann, M.; Bilbrey, J.; Wilkerson, J.; Guindon, J. Sex differences and endocannabinoid system in pain. Pharmacol. Biochem. Behav. 2021, 202, 173107. [Google Scholar]
- Kwon, A.; Flood, P. Genetics and gender in acute pain and perioperative opioid analgesia. Anesthesiol. Clin. 2020, 38, 341–355. [Google Scholar] [CrossRef]
- Paller, C.J.; Campbell, C.; Edwards, R.; Dobs, A. Sex-based differences in pain perception and treatment. Pain Med. 2009, 10, 289–299. [Google Scholar] [PubMed]
- Fillingim, R.; Ness, T. Sex-related hormonal influences on pain and analgesic responses. Neuriscience Behav. Rev. 2000, 24, 485–501. [Google Scholar]
- Gerbershagen, H.; Aduckathil, S.; van Wijck, A.; Peelen, L.; Kalkman, C.; Meissner, W. Pain intensity on the first day after surgery. Anesthesiology 2013, 118, 934–944. [Google Scholar] [PubMed]
- Karamesinis, A.; Neto, A.; Shi, J.; Fletcher, C.; Hinton, J.; Xing, Z.; Penny-Dimri, J.C.; Ramson, D.; Liu, Z.; Plummer, M.; et al. Sex differences in opioid administration after cardiac surgery. J. Cardiothorasic. Vasc. Anesth. 2024, 38, 701–708. [Google Scholar]
- Yeh, C.; Chang, W.; Wu, H.; Chau, G.; Tai, Y.; Chang, K. Associations of multimodal analgesia with postoperative pain trajectories and morphine consumption after hepatic cancer surgery. Front. Med. 2022, 8, 777369. [Google Scholar]
- Vishnuraj, K.R.; Singh, K.; Sahay, N.; Sinha, C.; Kumar, A.; Kumar, N. Opioid-free anesthesia using a combination of ketamine and dexmedetomidine in patients undergoing laparoscopic cholecystectomy: A randomized controlled trial. Anesth. Pain Med. 2024, 19, 109–116. [Google Scholar]
- Kosciuczuk, U.; Tarnowska, K.; Rynkiewicz-Szczepanska, E. Are There Any Advantages of the Low Opioid Anaesthesia and Non-Opioid Postoperative Analgesia Protocol: A Clinical Observational Study. J. Pain Res. 2024, 17, 941–951. [Google Scholar] [CrossRef]
- Bakan, M.; Umutoglu, T.; Topuz, U.; Uysal, H.; Bayram, M.; Kadioglu, H.; Salihoglu, Z. Opioid-free Total intravenous anesthesia with propofol, dexmedetomidine and lidocaine infusions for laparoscopic cholecystectomy: A prospective, randomized, double-blinded study. Rev. Bras. Anestesiol. 2015, 65, 191–199. [Google Scholar] [CrossRef]
- Barazanchi, A.; MacFater, W.; Rahiri, J.; Tutone, S.; Hill, A.; Joshi, G.; on behalf on the PROSPECT Collaboration. Evidence-based management of pain after laparoscopic cholecystectomy: A PROSPECT review update. Br. J. Anaesth. 2018, 121, 787–803. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
| Premedication | Preoperatively | Induction Phase | Maintenance and Recovery Phase of Anesthesia | Postoperatively | |
|---|---|---|---|---|---|
| LOA | midazolam 7.5 mg p.o | 1 g of paracetamol 2 g of magnesium sulfate 100 mg of lidocaine 50 mg of ketamine | 0.1 mg of fentanyl 2 mg/kg of propofol 0.15 mg of cisatracurium | infusion of lignocaine (2 mg mL−1 solution), at a dose of 1.5–3.0 mg kg−1 h−1 ketamine (1 mg mL−1 solution), at a dose of 0.125–0.25 mg kg−1 h−1 ketamine infusion was stopped 10 min before the end of surgery lignocaine infusion was terminated at the end of anesthesia 2 g of metamizole 30 min before awakening | 1 g of paracetamol 1 g of metamizole intravenously every 6 h |
| OBA | midazolam 7.5 mg p.o | - | 0.1 mg of fentanyl 2 mg/kg of propofol 0.15 mg of cisatracurium | repeated doses of fentanyl of 0.1 mg 2 g of metamizole 30 min before awakening | 1 g of paracetamol 1 g of metamizole intravenously every 6 h |
| Low-Opioid Anesthesia (LOA) | Opioid-Based Anesthesia (OBA) | p-Value | |||
|---|---|---|---|---|---|
| Women n = 26 | Men n = 13 | Women n = 26 | Men n = 11 | ||
| age | 63 (26–79) | 50 (40–85) | 53.5 (27–81) | 65 (31–73) | NS |
| BMI | 28.5 (18–38) | 26 (22–34) | 27.5 (19–41) | 29 (23–38) | NS |
| BSA | 1.84 (1.56–2.21) | 1.82 (1.7–2.07) | 1.81 (1.54–2.05) | 2.04 (1.85–2.35) | NS |
| Duration of anesthesia (min) | 53.5 (30–210) | 50 (30–90) | 57.5 (30–110) | 55 (40–105) | NS |
| Duration of operation (min) | 40 (20–192) | 35 (20–75) | 40 (25–95) | 48 (30–90) | NS |
| Mean NRS | 1.62 * (0–7) | 2.25 (0–4) | 4.0 (1–8) | 2.0 (1–8) | p < 0.05 |
| Total dose of fentanyl (mg) | 0.1 | 0.1 | 0.25 (0.15–0.4) | 0.2 (0.2–0.4) | NS |
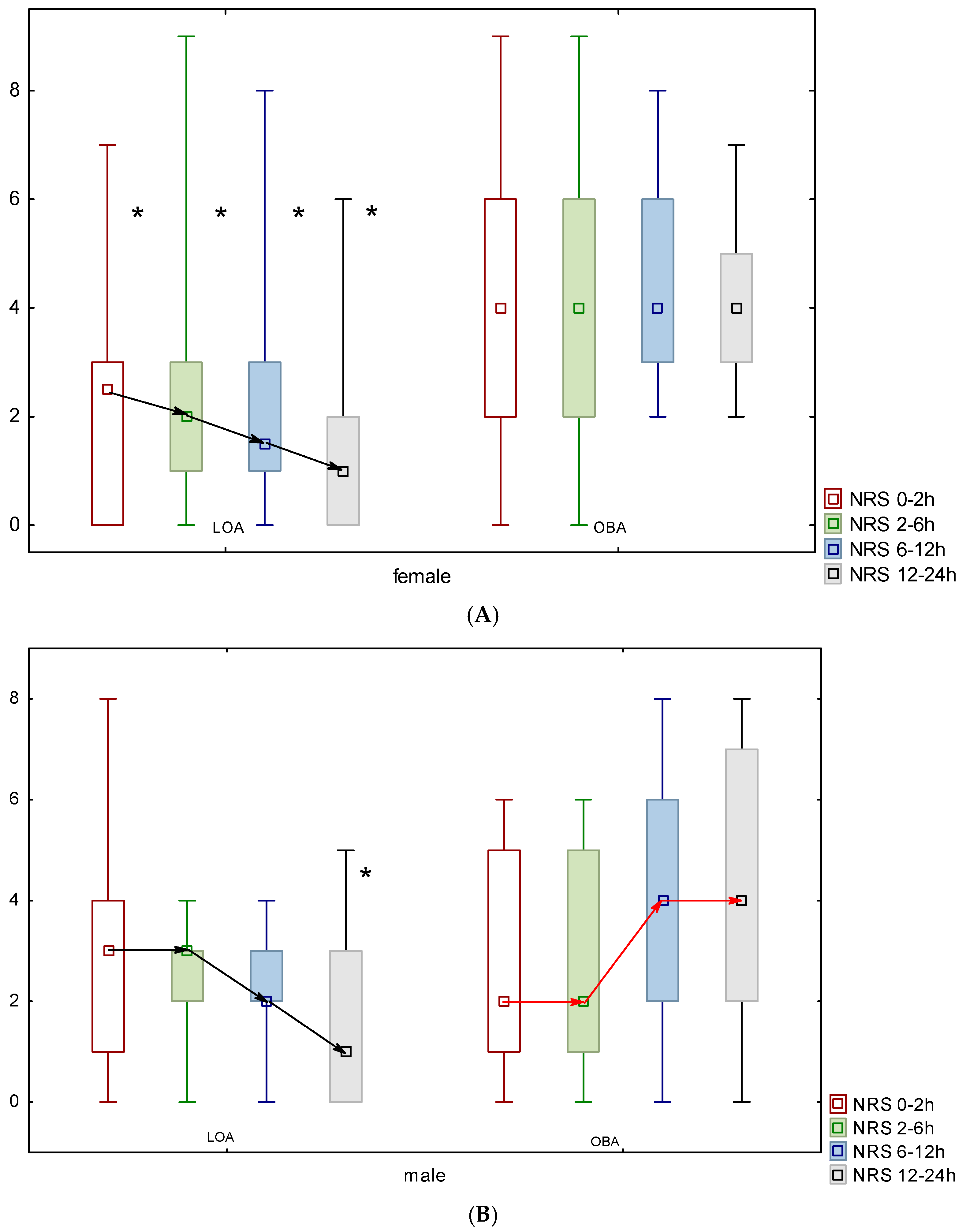
| Low-Opioid Anesthesia | Opioid-Based Anesthesia | |||
|---|---|---|---|---|
| Women n = 26 | Men n = 13 | Women n = 26 | Men n = 13 | |
| 0–2 h | 2.5 * (0–7) | 3 (0–8) | 4.0 (0–9) | 2.0 (0–6) |
| 2–6 h | 2.0 * (0–9) | 3.0 (0–4) | 4.0 (0–9) | 2.0 (0–6) |
| 6–12 h | 1.5 * (0–8) | 2.0 (0–4) | 4.0 (2–8) | 4.0 (0–8) |
| 12–24h | 1.0 * (0–6) | 1 ** (0–5) | 4.0 (2–7) | 4.0 (0–8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosciuczuk, U.; Kossakowska, A.; Talalaj, M.; Grabowska, K.; Pryzmont, M. Sex-Related Analgesic Effects of Opioid-Based Anesthesia and Low-Opioid Anesthesia with Non-Opioid Postoperative Analgesia—A Clinical Observational Study. J. Clin. Med. 2025, 14, 2163. https://doi.org/10.3390/jcm14072163
Kosciuczuk U, Kossakowska A, Talalaj M, Grabowska K, Pryzmont M. Sex-Related Analgesic Effects of Opioid-Based Anesthesia and Low-Opioid Anesthesia with Non-Opioid Postoperative Analgesia—A Clinical Observational Study. Journal of Clinical Medicine. 2025; 14(7):2163. https://doi.org/10.3390/jcm14072163
Chicago/Turabian StyleKosciuczuk, Urszula, Agnieszka Kossakowska, Marcin Talalaj, Katarzyna Grabowska, and Marta Pryzmont. 2025. "Sex-Related Analgesic Effects of Opioid-Based Anesthesia and Low-Opioid Anesthesia with Non-Opioid Postoperative Analgesia—A Clinical Observational Study" Journal of Clinical Medicine 14, no. 7: 2163. https://doi.org/10.3390/jcm14072163
APA StyleKosciuczuk, U., Kossakowska, A., Talalaj, M., Grabowska, K., & Pryzmont, M. (2025). Sex-Related Analgesic Effects of Opioid-Based Anesthesia and Low-Opioid Anesthesia with Non-Opioid Postoperative Analgesia—A Clinical Observational Study. Journal of Clinical Medicine, 14(7), 2163. https://doi.org/10.3390/jcm14072163