

Mapping Psychological Well-Being in Morbid Obesity: A Network Analysis Approach


 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Correlation Analysis
3.3. Psychometric Network Analysis
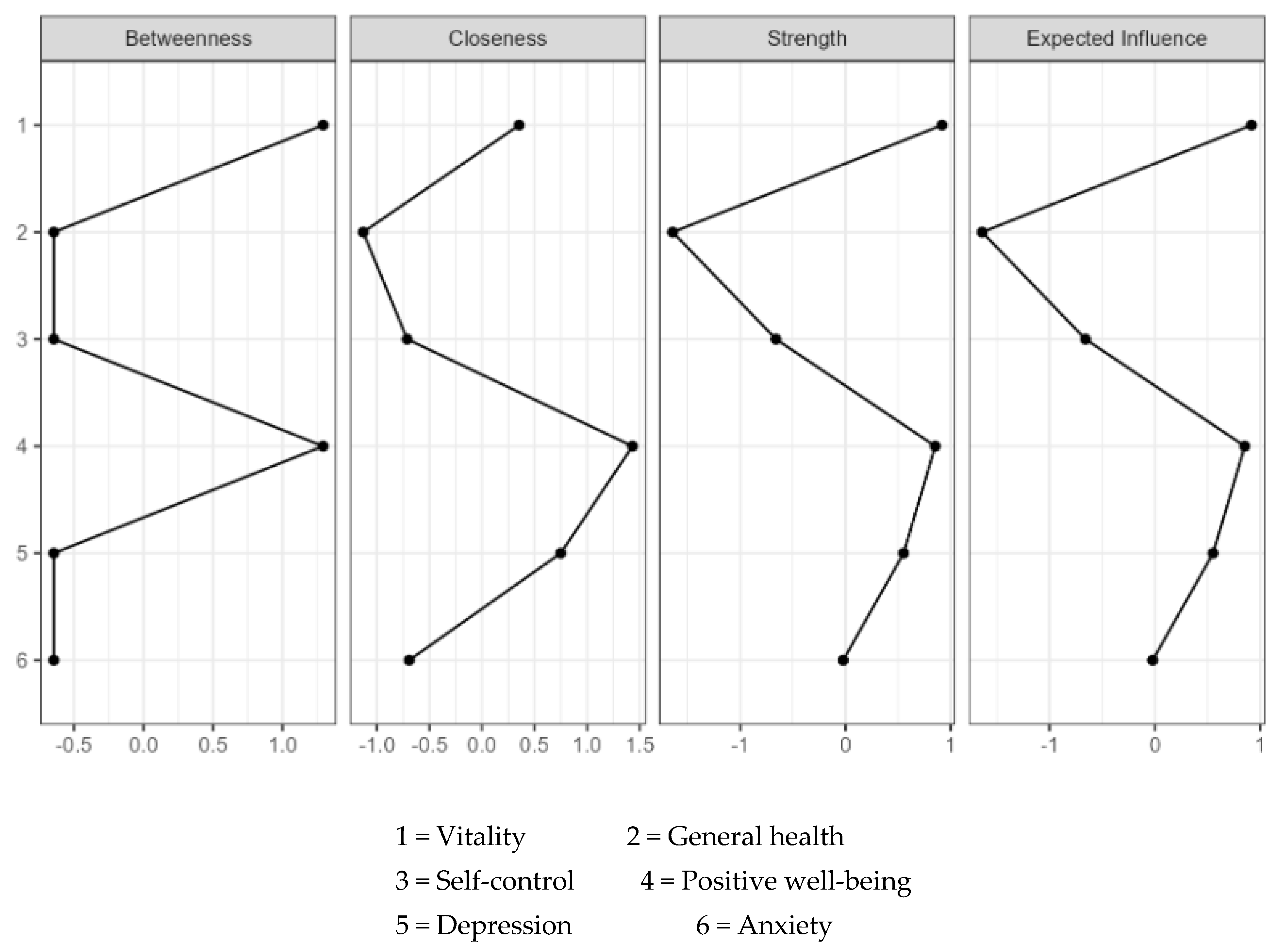
3.3.1. Network Structure and Edge Weights
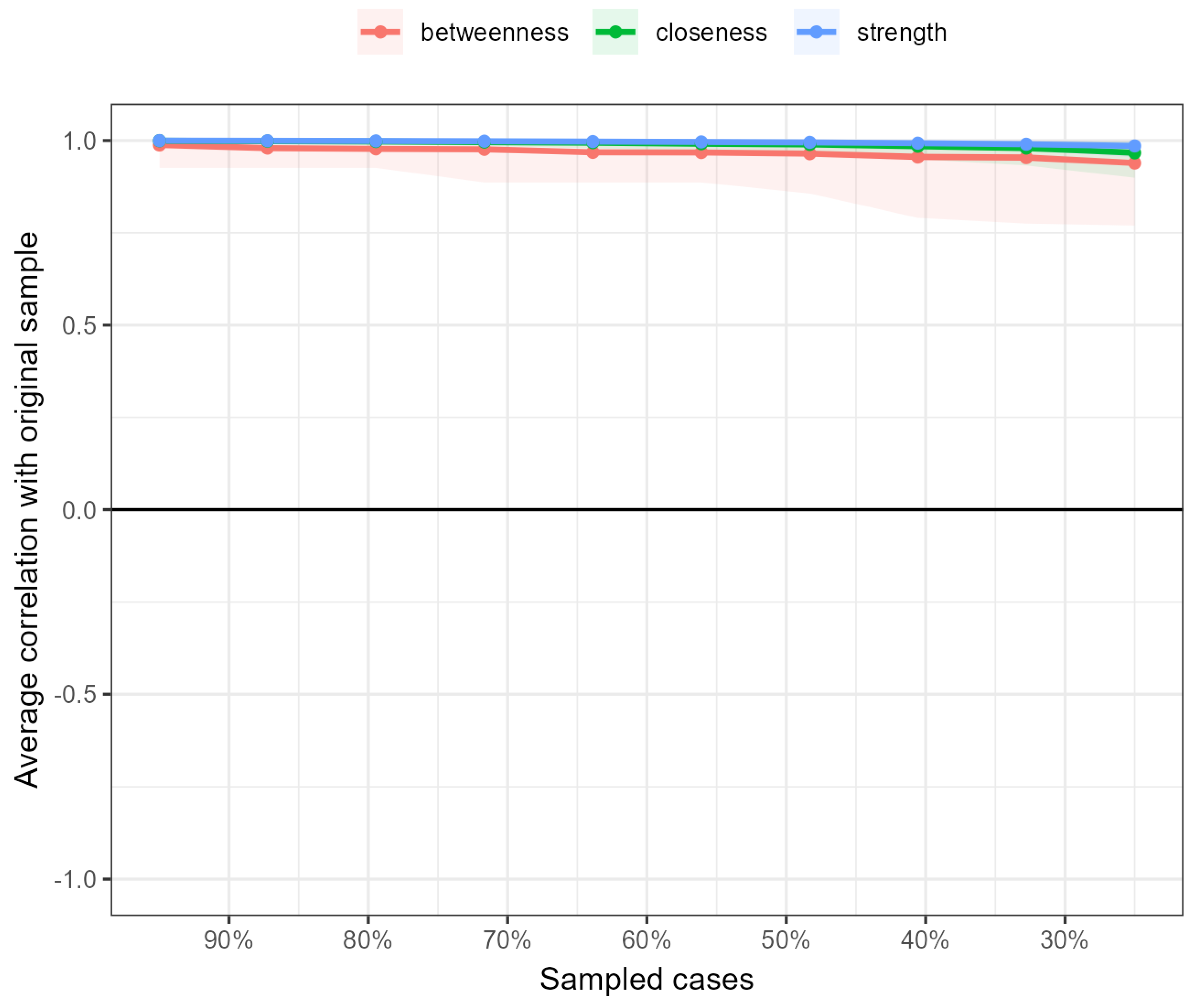
3.3.2. Network Stability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phelps, N.H.; Singleton, R.K.; Zhou, B.; Heap, R.A.; Mishra, A.; Bennett, J.E.; Paciorek, C.J.; Lhoste, V.P.F.; Carrillo-Larco, R.M.; Stevens, G.A.; et al. Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 2024, 403, 1027–1050. [Google Scholar] [CrossRef] [PubMed]
- Nagi, M.A.; Ahmed, H.; Rezq, M.A.A.; Sangroongruangsri, S.; Chaikledkaew, U.; Almalki, Z.; Thavorncharoensap, M. Economic costs of obesity: A systematic review. Int. J. Obes. 2024, 48, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Rubino, F.; Cummings, D.E.; Eckel, R.H.; Cohen, R.V.; Wilding, J.P.; Brown, W.A.; Stanford, F.C.; Batterham, R.L.; Farooqi, I.S.; Farpour-Lambert, N.J.; et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025, 13, 221–262. [Google Scholar] [CrossRef]
- Burki, T. European Commission classifies obesity as a chronic disease. Lancet Diabetes Endocrinol. 2021, 9, 418. [Google Scholar] [CrossRef]
- Castelnuovo, G.; Capodaglio, P.; De Amicis, R.; Gilardini, L.; Mambrini, S.P.; Pietrabissa, G.; Cavaggioni, L.; Piazzolla, G.; Galeone, C.; Garavaglia, G.; et al. Study protocol of a clinical randomized controlled trial on the efficacy of an innovative Digital thErapy to proMote wEighT loss in patients with obesity by incReasing their Adherence to treatment: The DEMETRA study. Front. Digit. Health 2023, 5, 1159744. [Google Scholar] [CrossRef]
- Cattivelli, R.; Castelnuovo, G.; Musetti, A.; Varallo, G.; Spatola, C.A.M.; Riboni, F.V.; Usubini, A.G.; Tosolin, F.; Manzoni, G.M.; Capodaglio, P.; et al. ACTonHEALTH study protocol: Promoting psychological flexibility with activity tracker and mHealth tools to foster healthful lifestyle for obesity and other chronic health conditions. Trials 2018, 19, 659. [Google Scholar] [CrossRef]
- Debski, J.; Przybylowski, J.; Skibiak, K.; Czerwinska, M.; Waledziak, M.; Rozanska-Waledziak, A. Depression and Obesity-Do We Know Everything about It? A Narrative Review. Nutrients 2024, 16, 3383. [Google Scholar] [CrossRef]
- Pietrabissa, G.; Bertuzzi, V.; Simpson, S.; Guerrini Usubini, A.; Cattivelli, R.; Bertoli, S.; Mozzi, E.; Roviaro, G.; Castelnuovo, G.; Molinari, E. Psychological Aspects of Treatment with Intragastric Balloon for Management of Obesity: A Systematic Review of the Literature. Obes. Facts 2022, 15, 1–18. [Google Scholar] [CrossRef]
- Amiri, S.; Behnezhad, S. Obesity and anxiety symptoms: A systematic review and meta-analysis. Neuropsychiatrie 2019, 33, 72–89. [Google Scholar] [CrossRef]
- Gomez-de-Regil, L.; Avila-Nava, A.; Gutierrez-Solis, A.L.; Lugo, R. Mobile Apps for the Management of Comorbid Overweight/Obesity and Depression/Anxiety: A Systematic Review. J. Healthc. Eng. 2020, 2020, 9317179. [Google Scholar] [CrossRef]
- Kokkinos, P.; Faselis, C.; Franklin, B.; Lavie, C.J.; Sidossis, L.; Moore, H.; Karasik, P.; Myers, J. Cardiorespiratory fitness, body mass index and heart failure incidence. Eur. J. Heart Fail. 2019, 21, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Pietrabissa, G.; Manzoni, G.M.; Rossi, A.; Castelnuovo, G. The MOTIV-HEART Study: A Prospective, Randomized, Single-Blind Pilot Study of Brief Strategic Therapy and Motivational Interviewing among Cardiac Rehabilitation Patients. Front. Psychol. 2017, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- Sarwer, D.B.; Polonsky, H.M. The Psychosocial Burden of Obesity. Endocrinol. Metab. Clin. North. Am. 2016, 45, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Ryan, L.; Quigley, F.; Birney, S.; Crotty, M.; Conlan, O.; Walsh, J.C. ’Beyond the Scale’: A Qualitative Exploration of the Impact of Weight Stigma Experienced by Patients With Obesity in General Practice. Health Expect. 2024, 27, e14098. [Google Scholar] [CrossRef]
- Rao, A.; Puhl, R.; Farrar, K. Weight Stigma in Online News Images: A Visual Content Analysis of Stigma Communication in the Depictions of Individuals with Obesity in U.S. and U.K. News. J. Health Commun. 2024, 29, 95–106. [Google Scholar] [CrossRef]
- Rossi, A.A.; Manzoni, G.M.; Pietrabissa, G.; Di Pauli, D.; Mannarini, S.; Castelnuovo, G. Weight stigma in patients with overweight and obesity: Validation of the Italian Weight Self-Stigma Questionnaire (WSSQ). Eat. Weight Disord. 2022, 27, 2459–2472. [Google Scholar] [CrossRef]
- Puhl, R.M.; Himmelstein, M.S.; Pearl, R.L. Weight stigma as a psychosocial contributor to obesity. Am. Psychol. 2020, 75, 274–289. [Google Scholar] [CrossRef]
- Albano, G.; Rowlands, K.; Baciadonna, L.; Coco, G.L.; Cardi, V. Interpersonal difficulties in obesity: A systematic review and meta-analysis to inform a rejection sensitivity-based model. Neurosci. Biobehav. Rev. 2019, 107, 846–861. [Google Scholar] [CrossRef]
- Côté, M.; Bégin, C. Review of the Experience of Weight-Based Stigmatization in Romantic Relationships. Curr. Obes. Rep. 2020, 9, 280–287. [Google Scholar] [CrossRef]
- Täuber, S.; Mulder, L.B.; Flint, S.W. The impact of workplace health promotion programs emphasizing individual responsibility on weight stigma and discrimination. Front. Psychol. 2018, 9, 2206. [Google Scholar] [CrossRef]
- Crompvoets, P.I.; Nieboer, A.P.; van Rossum, E.F.C.; Cramm, J.M. Perceived weight stigma in healthcare settings among adults living with obesity: A cross-sectional investigation of the relationship with patient characteristics and person-centred care. Health Expect. 2024, 27, e13954. [Google Scholar] [CrossRef] [PubMed]
- Ryan, L.; Coyne, R.; Heary, C.; Birney, S.; Crotty, M.; Dunne, R.; Conlan, O.; Walsh, J.C. Weight stigma experienced by patients with obesity in healthcare settings: A qualitative evidence synthesis. Obes. Rev. 2023, 24, e13606. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Wadden, T.A. Psychological aspects of severe obesity. Am. J. Clin. Nutr. 1992, 55, 524s–532s. [Google Scholar] [CrossRef] [PubMed]
- Crompvoets, P.I.; Nieboer, A.P.; van Rossum, E.F.C.; Cramm, J.M. The relationship between person-centred care and well-being and satisfaction with care of patients living with obesity. Int. J. Qual. Health Care 2024, 36, mzae078. [Google Scholar] [CrossRef]
- Molina, K.; Baskin, M.L.; Long, D.; Carson, T.L. Psychological and behavioral pathways between perceived stress and weight change in a behavioral weight loss intervention. J. Behav. Med. 2021, 44, 822–832. [Google Scholar] [CrossRef]
- Guerrini Usubini, A.; Cattivelli, R.; Giusti, E.M.; Riboni, F.V.; Varallo, G.; Pietrabissa, G.; Manzoni, G.M.; Consoli, S.; Bastoni, I.; Granese, V.; et al. The ACTyourCHANGE study protocol: Promoting a healthy lifestyle in patients with obesity with Acceptance and Commitment Therapy-a randomized controlled trial. Trials 2021, 22, 290. [Google Scholar] [CrossRef]
- Rand, K.; Vallis, M.; Aston, M.; Price, S.; Piccinini-Vallis, H.; Rehman, L.; Kirk, S.F. “It is not the diet; it is the mental part we need help with.” A multilevel analysis of psychological, emotional, and social well-being in obesity. Int. J. Qual. Stud. Health Well-Being 2017, 12, 1306421. [Google Scholar] [CrossRef]
- Alberga, A.S.; Edache, I.Y.; Forhan, M.; Russell-Mayhew, S. Weight bias and health care utilization: A scoping review. Prim. Health Care Res. Dev. 2019, 20, e116. [Google Scholar] [CrossRef]
- Pietrabissa, G.; Castelnuovo, G.; Manzoni, G.M.; Cattivelli, R.; Molinari, E.; Gondoni, L.A. Psychological Well-Being as an Independent Predictor of Exercise Capacity in Cardiac Rehabilitation Patients With Obesity. Front. Psychol. 2019, 10, 2973. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being: The science of happiness and a proposal for a national index. Am. Psychol. 2000, 55, 34. [Google Scholar] [CrossRef]
- Boulon, L.; Prieur, F.; Gaget, O.; Martin, D.; Amichaud, R.; Al Naasan, I.; Hicter, M.-G.; Bossu Estour, C. Progression of quality of life in patients with grade 3 obesity after a 36 months care pathway with and without bariatric surgery. Nutr. Clin. Métab. 2022, 36, 203–209. [Google Scholar] [CrossRef]
- Phyo, A.Z.Z.; Freak-Poli, R.; Craig, H.; Gasevic, D.; Stocks, N.P.; Gonzalez-Chica, D.A.; Ryan, J. Quality of life and mortality in the general population: A systematic review and meta-analysis. BMC Public Health 2020, 20, 1596. [Google Scholar] [CrossRef] [PubMed]
- Rasyid, H.; Kasim, H.; Zatalia, S.R.; Sampebuntu, J. Quality of life in patients with renal failure undergoing hemodialysis. Acta Medica Indones. 2022, 54, 307–313. [Google Scholar]
- Greenspoon, P.J.; Saklofske, D.H. Toward an Integration of Subjective Well-Being and Psychopathology. Soc. Indic. Res. 2001, 54, 81–108. [Google Scholar] [CrossRef]
- Suldo, S.M.; Shaffer, E.J. Looking beyond psychopathology: The dual-factor model of mental health in youth. Sch. Psychol. Rev. 2008, 37, 52–68. [Google Scholar] [CrossRef]
- Calugi, S.; Dalle Grave, R. Psychological features in obesity: A network analysis. Int. J. Eat. Disord. 2020, 53, 248–255. [Google Scholar] [CrossRef]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Methods Prim. 2021, 1, 58. [Google Scholar] [CrossRef]
- Galderisi, S.; Rucci, P.; Kirkpatrick, B.; Mucci, A.; Gibertoni, D.; Rocca, P.; Rossi, A.; Bertolino, A.; Strauss, G.P.; Aguglia, E.; et al. Interplay Among Psychopathologic Variables, Personal Resources, Context-Related Factors, and Real-life Functioning in Individuals With Schizophrenia: A Network Analysis. JAMA Psychiatry 2018, 75, 396–404. [Google Scholar] [CrossRef]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef]
- Grossi, E.; Compare, A. Psychological General Well-Being Index (PGWB). In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 5152–5156. [Google Scholar]
- Dupuy, H.J. The psychological general well-being (PGWB) index. In Assessment of Quality of Life in clinical trials of cardiovascular therapies; Le Jacq Publishing: New York, NY, USA, 1984; pp. 170–183. [Google Scholar]
- Nilsson, G.; Ohrvik, J.; Lonnberg, I.; Hedberg, P. Low Psychological General Well-Being (PGWB) is associated with deteriorated 10-year survival in men but not in women among the elderly. Arch. Gerontol. Geriatr. 2011, 52, 167–171. [Google Scholar] [CrossRef]
- Talley, N.J.; Wiklund, I. Patient reported outcomes in gastroesophageal reflux disease: An overview of available measures. Qual. Life Res. 2005, 14, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Lundgren-Nilsson, Å.; Jonsdottir, I.H.; Ahlborg, G.; Tennant, A. Construct validity of the psychological general well being index (PGWBI) in a sample of patients undergoing treatment for stress-related exhaustion: A rasch analysis. Health Qual. Life Outcomes 2013, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows; Version 29.0.2.0; IBM Corp: Armonk, NY, USA, 2023. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- JASP Team. JASP, Version 0.19.0; JASP: Amsterdam, The Netherlands, 2024.
- Lauritzen, S.L. Oxford Statistical Science Series. In Graphical Models; Oxford University Press: Oxford, UK; New York, NY, USA, 1996. [Google Scholar]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics 2007, 9, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Golino, H.F.; Epskamp, S. Exploratory graph analysis: A new approach for estimating the number of dimensions in psychological research. PLoS ONE 2017, 12, e0174035. [Google Scholar] [CrossRef]
- Costantini, G.; Epskamp, S.; Borsboom, D.; Perugini, M.; Mõttus, R.; Waldorp, L.J.; Cramer, A.O.J. State of the aRt personality research: A tutorial on network analysis of personality data in R. J. Res. Personal. 2015, 54, 13–29. [Google Scholar] [CrossRef]
- Epskamp, S.; Maris, G.; Waldorp, L.J.; Borsboom, D. Network Psychometrics. In The Wiley Handbook of Psychometric Testing: AnMultidisciplinary Reference on Survey, Scale and Test Development; University of Amsterdam: Amsterdam, The Netherlands, 2017; Volume 2, pp. 953–986. [Google Scholar]
- Chen, J.; Chen, Z. Extended Bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef]
- van Borkulo, C.D.; Borsboom, D.; Epskamp, S.; Blanken, T.F.; Boschloo, L.; Schoevers, R.A.; Waldorp, L.J. A new method for constructing networks from binary data. Sci. Rep. 2014, 4, 5918. [Google Scholar] [CrossRef]
- Barber, R.F.; Drton, M. High-dimensional Ising model selection with Bayesian information criteria. Electron. J. Stat. 2015, 9, 567–607. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef]
- Marchetti, I. Hopelessness: A network analysis. Cogn. Ther. Res. 2019, 43, 611–619. [Google Scholar] [CrossRef]
- Haslbeck, J.M.B.; Waldorp, L.J. How well do network models predict observations? On the importance of predictability in network models. Behav. Res. Methods 2018, 50, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Haslbeck, J.M.B.; Waldorp, L.J. mgm: Estimating Time-Varying Mixed Graphical Models in High-Dimensional Data. J. Stat. Softw. 2020, 93, 1–46. [Google Scholar] [CrossRef]
- Dalege, J.; Borsboom, D.; van Harreveld, F.; van der Maas, H.L.J. Network Analysis on Attitudes:A Brief Tutorial. Soc. Psychol. Personal. Sci. 2017, 8, 528–537. [Google Scholar] [CrossRef]
- McNally, R.J.; Mair, P.; Mugno, B.L.; Riemann, B.C. Co-morbid obsessive–compulsive disorder and depression: A Bayesian network approach. Psychol. Med. 2017, 47, 1204–1214. [Google Scholar] [CrossRef]
- Borsboom, D.; Cramer, A.O. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef]
- Luo, X.; Ruan, Z.; Liu, L. The association between overweight and varying degrees of obesity with subjective well-being and depressive symptoms: A two sample Mendelian randomization study. J. Psychosom. Res. 2024, 187, 111940. [Google Scholar] [CrossRef]
- Putra, I.; Daly, M.; Sutin, A.; Steptoe, A.; Scholes, S.; Robinson, E. Obesity, psychological well-being related measures, and risk of seven non-communicable diseases: Evidence from longitudinal studies of UK and US older adults. Int. J. Obes. 2024, 48, 1283–1291. [Google Scholar] [CrossRef]
- Conradson, H.E.; Hayden, K.A.; Russell-Mayhew, S.; Raffin Bouchal, S.; King-Shier, K. Positive psychological well-being in women with obesity: A scoping review of qualitative and quantitative primary research. Obes. Sci. Pr. 2022, 8, 691–714. [Google Scholar] [CrossRef]
- Dockray, S.; Steptoe, A. Positive affect and psychobiological processes. Neurosci. Biobehav. Rev. 2010, 35, 69–75. [Google Scholar] [CrossRef]
- Guerrini Usubini, A.; Varallo, G.; Granese, V.; Cattivelli, R.; Consoli, S.; Bastoni, I.; Volpi, C.; Castelnuovo, G.; Molinari, E. The Impact of Psychological Flexibility on Psychological Well-Being in Adults With Obesity. Front. Psychol. 2021, 12, 636933. [Google Scholar] [CrossRef]
- Pietrabissa, G.; Volpi, C.; Bottacchi, M.; Bertuzzi, V.; Guerrini Usubini, A.; Löffler-Stastka, H.; Prevendar, T.; Rapelli, G.; Cattivelli, R.; Castelnuovo, G.; et al. The Impact of Social Isolation during the COVID-19 Pandemic on Physical and Mental Health: The Lived Experience of Adolescents with Obesity and Their Caregivers. Int. J. Env. Res. Public Health 2021, 18, 3026. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, J.F. Determinants of well-being and their implications for health care. Ann. Nutr. Metab. 2019, 74, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Beekman, A.; Deeg, D.; Braam, A.; Smit, J.; Van Tilburg, W. Consequences of major and minor depression in later life: A study of disability, well-being and service utilization. Psychol. Med. 1997, 27, 1397–1409. [Google Scholar] [CrossRef]
- Chida, Y.; Steptoe, A. Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef]
- Lundqvist, C.; Kenttä, G. Positive Emotions Are Not Simply the Absence of the Negative Ones: Development and Validation of the Emotional Recovery Questionnaire (EmRecQ). Sport Psychol. 2010, 24, 468–488. [Google Scholar] [CrossRef]
- Ruggeri, K.; Garcia-Garzon, E.; Maguire, Á.; Matz, S.; Huppert, F.A. Well-being is more than happiness and life satisfaction: A multidimensional analysis of 21 countries. Health Qual. Life Outcomes 2020, 18, 192. [Google Scholar] [CrossRef]
- Park, C.L.; Kubzansky, L.D.; Chafouleas, S.M.; Davidson, R.J.; Keltner, D.; Parsafar, P.; Conwell, Y.; Martin, M.Y.; Hanmer, J.; Wang, K.H. Emotional Well-Being: What It Is and Why It Matters. Affect. Sci. 2023, 4, 10–20. [Google Scholar] [CrossRef]
- Diener, E.; Pressman, S.D.; Hunter, J.; Delgadillo-Chase, D. If, Why, and When Subjective Well-Being Influences Health, and Future Needed Research. Appl. Psychol. Health Well-Being 2017, 9, 133–167. [Google Scholar] [CrossRef]
- Lapin, B.; Mate, K.; Li, Y.; Thakore, N. Subjective health perception prioritizes psychological well-being over physical function in advanced ALS: A multigroup structural equation modeling analysis. J. Neurol. Sci. 2022, 442, 120442. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- Chew, H.S.J.; Gao, Y.; Shabbir, A.; Lim, S.L.; Geetha, K.; Kim, G.; Chong, C.S.; Lomanto, D.; So, B.Y.J. Personal motivation, self-regulation barriers and strategies for weight loss in people with overweight and obesity: A thematic framework analysis. Public Health Nutr. 2022, 25, 2426–2435. [Google Scholar] [CrossRef] [PubMed]
- Lumeng, J.C.; Miller, A.L.; Horodynski, M.A.; Brophy-Herb, H.E.; Contreras, D.; Lee, H.; Sturza, J.; Kaciroti, N.; Peterson, K.E. Improving self-regulation for obesity prevention in head start: A randomized controlled trial. Pediatrics 2017, 139, e20162047. [Google Scholar] [CrossRef]
- Tomiyama, A.J.; Carr, D.; Granberg, E.M.; Major, B.; Robinson, E.; Sutin, A.R.; Brewis, A. How and why weight stigma drives the obesity ’epidemic’ and harms health. BMC Med. 2018, 16, 123. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Gillebaart, M. Lessons learned from trait self-control in well-being: Making the case for routines and initiation as important components of trait self-control. Health Psychol. Rev. 2017, 11, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Gariepy, G.; Nitka, D.; Schmitz, N. The association between obesity and anxiety disorders in the population: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 407–419. [Google Scholar] [CrossRef]
- Dakanalis, A.; Mentzelou, M.; Papadopoulou, S.K.; Papandreou, D.; Spanoudaki, M.; Vasios, G.K.; Pavlidou, E.; Mantzorou, M.; Giaginis, C. The association of emotional eating with overweight/obesity, depression, anxiety/stress, and dietary patterns: A review of the current clinical evidence. Nutrients 2023, 15, 1173. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Burton, C.L. Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspect. Psychol. Sci. 2013, 8, 591–612. [Google Scholar] [CrossRef]
- Rademacher, L.; Kraft, D.; Eckart, C.; Fiebach, C.J. Individual differences in resilience to stress are associated with affective flexibility. Psychol. Res. 2023, 87, 1862–1879. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Steen, T.A.; Park, N.; Peterson, C. Positive Psychology Progress: Empirical Validation of Interventions. Am. Psychol. 2005, 60, 410–421. [Google Scholar] [CrossRef]
- Peters, M.L.; Smeets, E.; Feijge, M.; Van Breukelen, G.; Andersson, G.; Buhrman, M.; Linton, S.J. Happy despite pain: A randomized controlled trial of an 8-week internet-delivered positive psychology intervention for enhancing well-being in patients with chronic pain. Clin. J. Pain 2017, 33, 962–975. [Google Scholar] [CrossRef]
- Schotanus-Dijkstra, M.; Pieterse, M.E.; Drossaert, C.H.; Walburg, J.A.; Bohlmeijer, E.T. Possible mechanisms in a multicomponent email guided positive psychology intervention to improve mental well-being, anxiety and depression: A multiple mediation model. J. Posit. Psychol. 2019, 14, 141–155. [Google Scholar] [CrossRef]
- Reed, J.; Buck, S. The effect of regular aerobic exercise on positive-activated affect: A meta-analysis. Psychol. Sport Exerc. 2009, 10, 581–594. [Google Scholar] [CrossRef]
- Miller, K.J.; Mesagno, C.; McLaren, S.; Grace, F.; Yates, M.; Gomez, R. Exercise, mood, self-efficacy, and social support as predictors of depressive symptoms in older adults: Direct and interaction effects. Front. Psychol. 2019, 10, 2145. [Google Scholar] [CrossRef] [PubMed]
- Paluska, S.A.; Schwenk, T.L. Physical activity and mental health: Current concepts. Sports Med. 2000, 29, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef]
- Ruffault, A.; Czernichow, S.; Hagger, M.S.; Ferrand, M.; Erichot, N.; Carette, C.; Boujut, E.; Flahault, C. The effects of mindfulness training on weight-loss and health-related behaviours in adults with overweight and obesity: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2017, 11, 90–111. [Google Scholar] [CrossRef]
- Cotter, E.W.; Kelly, N.R. Stress-related eating, mindfulness, and obesity. Health Psychol. 2018, 37, 516. [Google Scholar] [CrossRef]
- Rapelli, G.; Pietrabissa, G.; Angeli, L.; Manzoni, G.M.; Tovaglieri, I.; Perger, E.; Garbarino, S.; Fanari, P.; Lombardi, C.; Castelnuovo, G. Study protocol of a randomized controlled trial of motivational interviewing-based intervention to improve adherence to continuous positive airway pressure in patients with obstructive sleep apnea syndrome: The MotivAir study. Front. Psychol. 2022, 13, 947296. [Google Scholar] [CrossRef]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Annesi, J. Effects of exercise self-regulation on subsequent eating self-regulation: Implications for depletion vs. improvement based on behavioral treatment foci. Eur. Rev. Appl. Psychol. 2019, 69, 100472. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Mean (SD) | Min–Max | |
|---|---|---|
| Age (years) | 57.18 (14.11) | 19–90 |
| BMI (kg/m2) | 43.40 (5.66) | 3500–7392 |
| PGWBI_Depression | 11.34 (3.12) | 0–24 |
| PGWBI_ Positive well-being | 10.23 (4.25) | 0–20 |
| PGWBI_Self-control | 10.43 (3.34) | 0–19 |
| PGWBI_ General health | 8.46 (3.04) | 0–21 |
| PGWBI_Vitality | 10.41 (4.24) | 0–20 |
| PGWBI_Anxiety | 15.71 (5.54) | 0–43 |
| PGWBI_Total | 66.57 (20.00) | 2–110 |
| Sex | Frequency | % |
| Male | 1.349 | 42.0 |
| Female | 1.863 | 58.0 |
| DEP | ANX | PWB | SC | GH | VIT | |
|---|---|---|---|---|---|---|
| Depression | - | |||||
| Anxiety | 0.746 * | - | ||||
| Positive well-being | 0.757 * | 0.720 * | - | |||
| Self-control | 0.699 * | 0.663 * | 0.694 * | - | ||
| General health | 0.522 * | 0.519 * | 0.541 * | 0.483 * | - | |
| Vitality | 0.669 * | 0.668 * | 0.768 * | 0.646 ** | 0.654 * | - |
| Anxiety | Depression | Positive Well-Being | Self-Control | General Health | Vitality | |
|---|---|---|---|---|---|---|
| Anxiety | - | |||||
| Depression | 0.342 | - | ||||
| Positive well-being | 0.182 | 0.298 | - | |||
| Self-control | 0.165 | 0.246 | 0.181 | - | ||
| General health | 0.071 | 0.071 | 0.000 | 0.023 | - | |
| Vitality | 0.119 | 0.037 | 0.394 | 0.133 | 0.385 | - |
| Network | ||||
|---|---|---|---|---|
| Betweenness | Closeness | Strength | Expected Influence | |
| Anxiety | −0.645 | −0.693 | −0.022 | −0.022 |
| Depression | −0.645 | 0.749 | 0.552 | 0.552 |
| Positive well-being | 1.291 | 1.432 | 0.853 | 0.853 |
| Self-control | −0.645 | −0.712 | −0.660 | −0.660 |
| General health | −0.645 | −1.130 | −1.641 | −1.641 |
| Vitality | 1.291 | 0.353 | 0.917 | 0.917 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietrabissa, G.; Guerrini-Usubini, A.; Villa, V.; Sartorio, A.; Castelnuovo, G.; Brunani, A. Mapping Psychological Well-Being in Morbid Obesity: A Network Analysis Approach. J. Clin. Med. 2025, 14, 2076. https://doi.org/10.3390/jcm14062076
Pietrabissa G, Guerrini-Usubini A, Villa V, Sartorio A, Castelnuovo G, Brunani A. Mapping Psychological Well-Being in Morbid Obesity: A Network Analysis Approach. Journal of Clinical Medicine. 2025; 14(6):2076. https://doi.org/10.3390/jcm14062076
Chicago/Turabian StylePietrabissa, Giada, Anna Guerrini-Usubini, Valentina Villa, Alessandro Sartorio, Gianluca Castelnuovo, and Amelia Brunani. 2025. "Mapping Psychological Well-Being in Morbid Obesity: A Network Analysis Approach" Journal of Clinical Medicine 14, no. 6: 2076. https://doi.org/10.3390/jcm14062076
APA StylePietrabissa, G., Guerrini-Usubini, A., Villa, V., Sartorio, A., Castelnuovo, G., & Brunani, A. (2025). Mapping Psychological Well-Being in Morbid Obesity: A Network Analysis Approach. Journal of Clinical Medicine, 14(6), 2076. https://doi.org/10.3390/jcm14062076