
Long-Term Clinical Remission on Benralizumab Treatment in Severe Eosinophilic Asthma: A Four-Year Real-Life Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Asthma Control Test (ACT)
2.2. Pulmonary Function Tests
2.3. Inflammatory Markers
2.4. Definition of Clinical Remission
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics at Baseline
3.2. Effect of Benralizumab on Individual Outcomes That Comprise the Definition of Clinical Remission
3.2.1. Effect of Benralizumab in Reducing Exacerbation
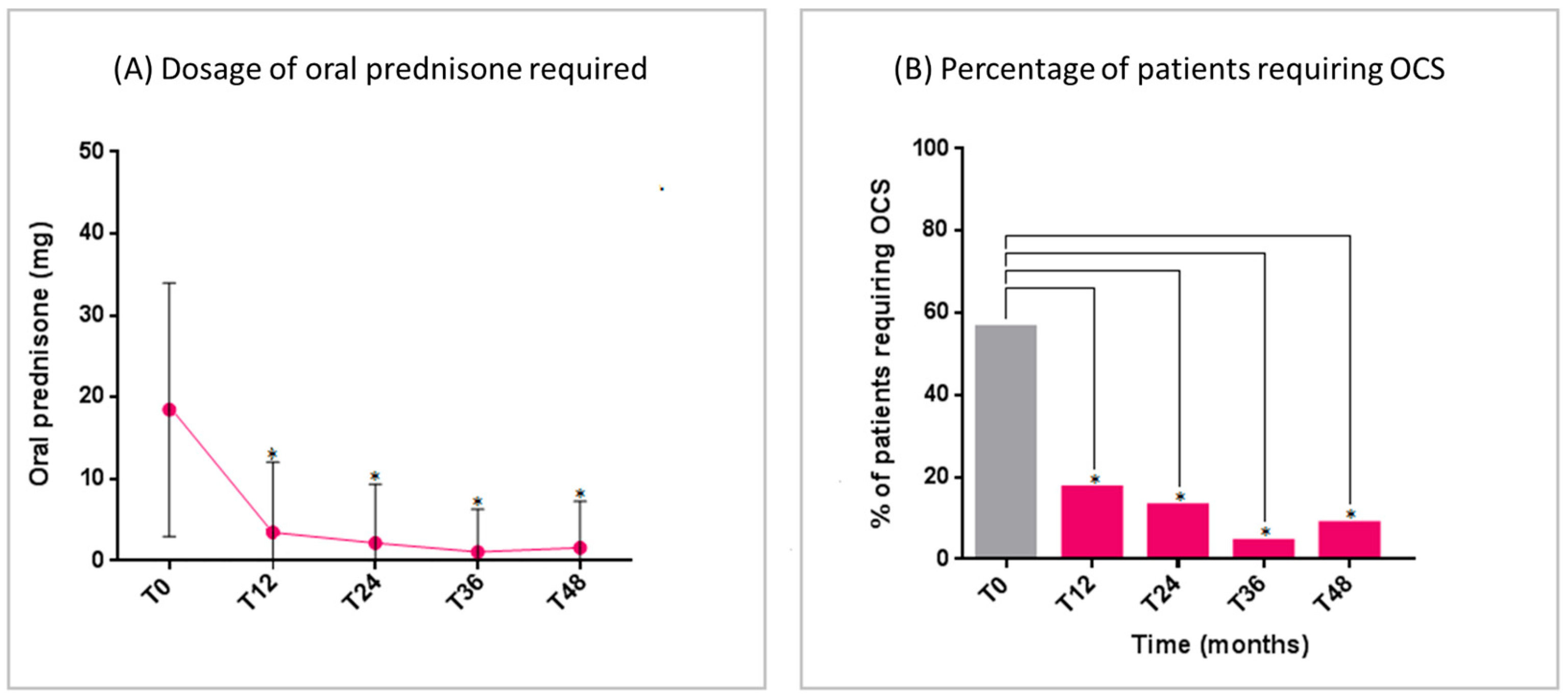
3.2.2. Effect of Benralizumab in Reducing OCS Dependence
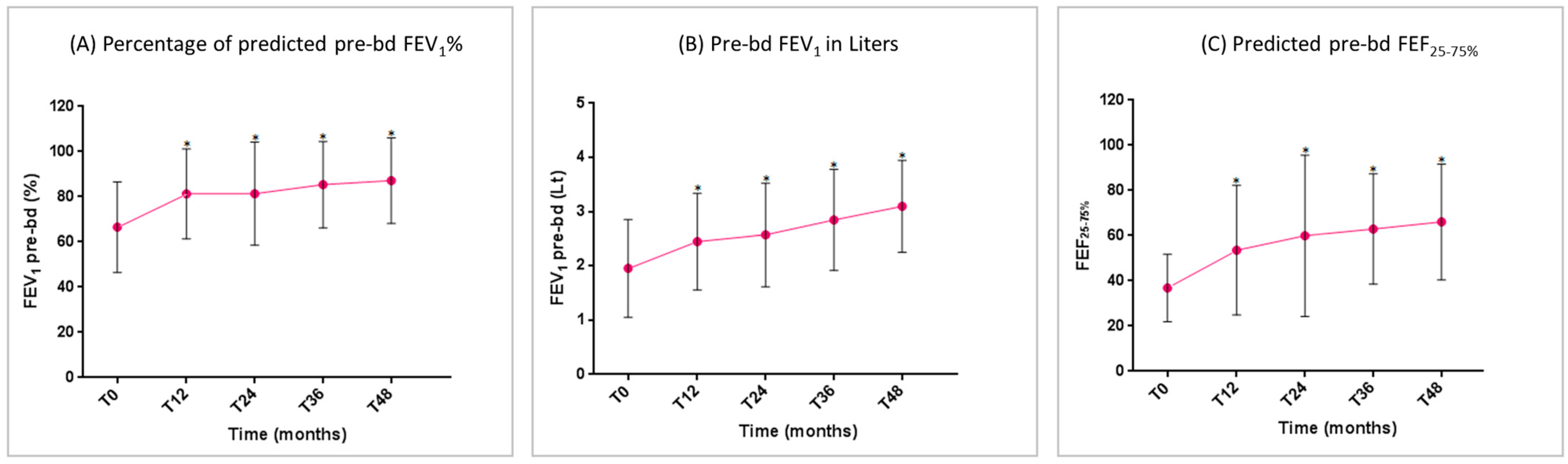
3.2.3. Effect of Benralizumab in Improving Respiratory Function
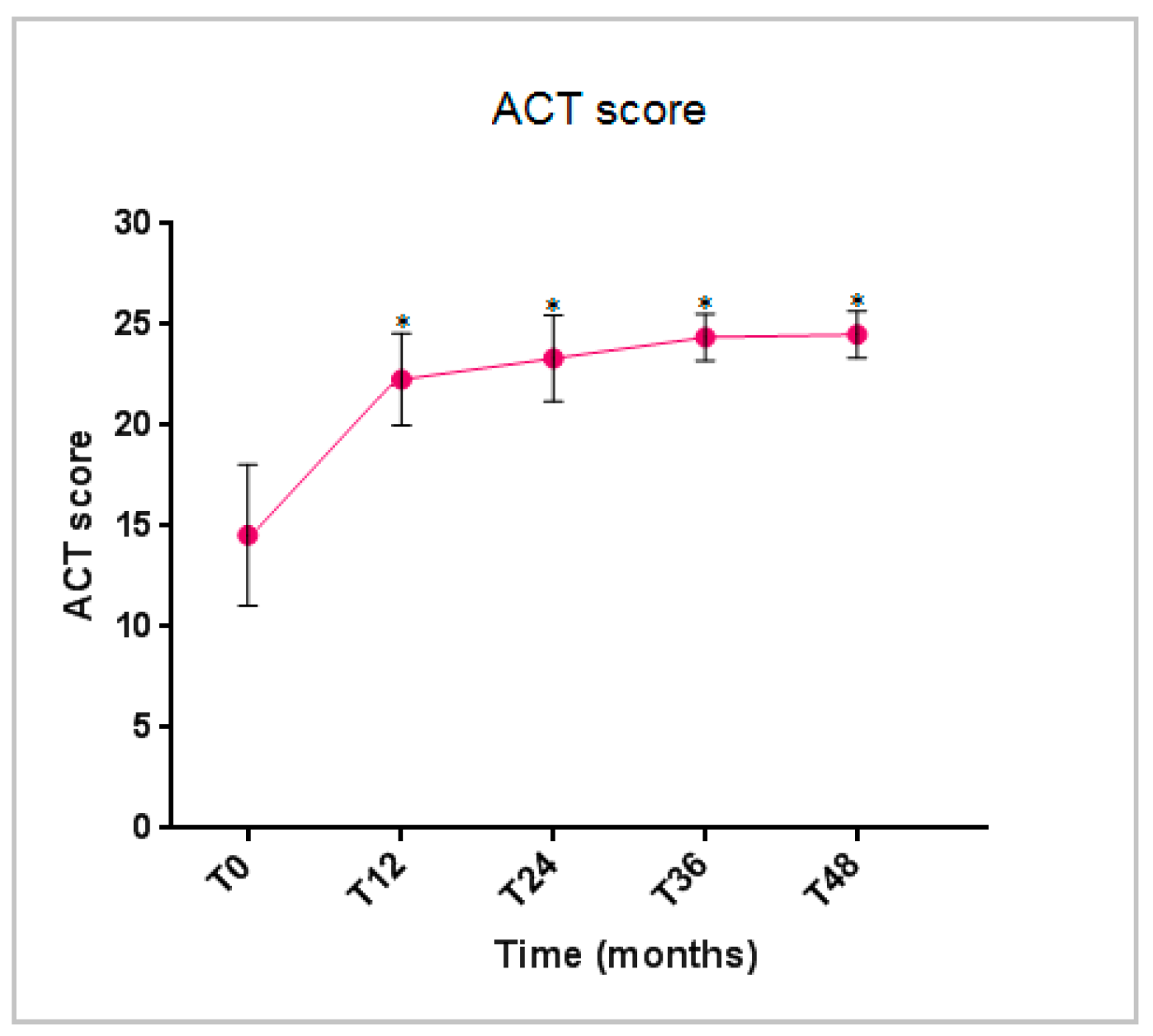
3.2.4. Effect of Benralizumab in the Asthma Control Test (ACT) Score
3.3. Effects of Benralizumab on Markers of Asthma-Related T2 Inflammation
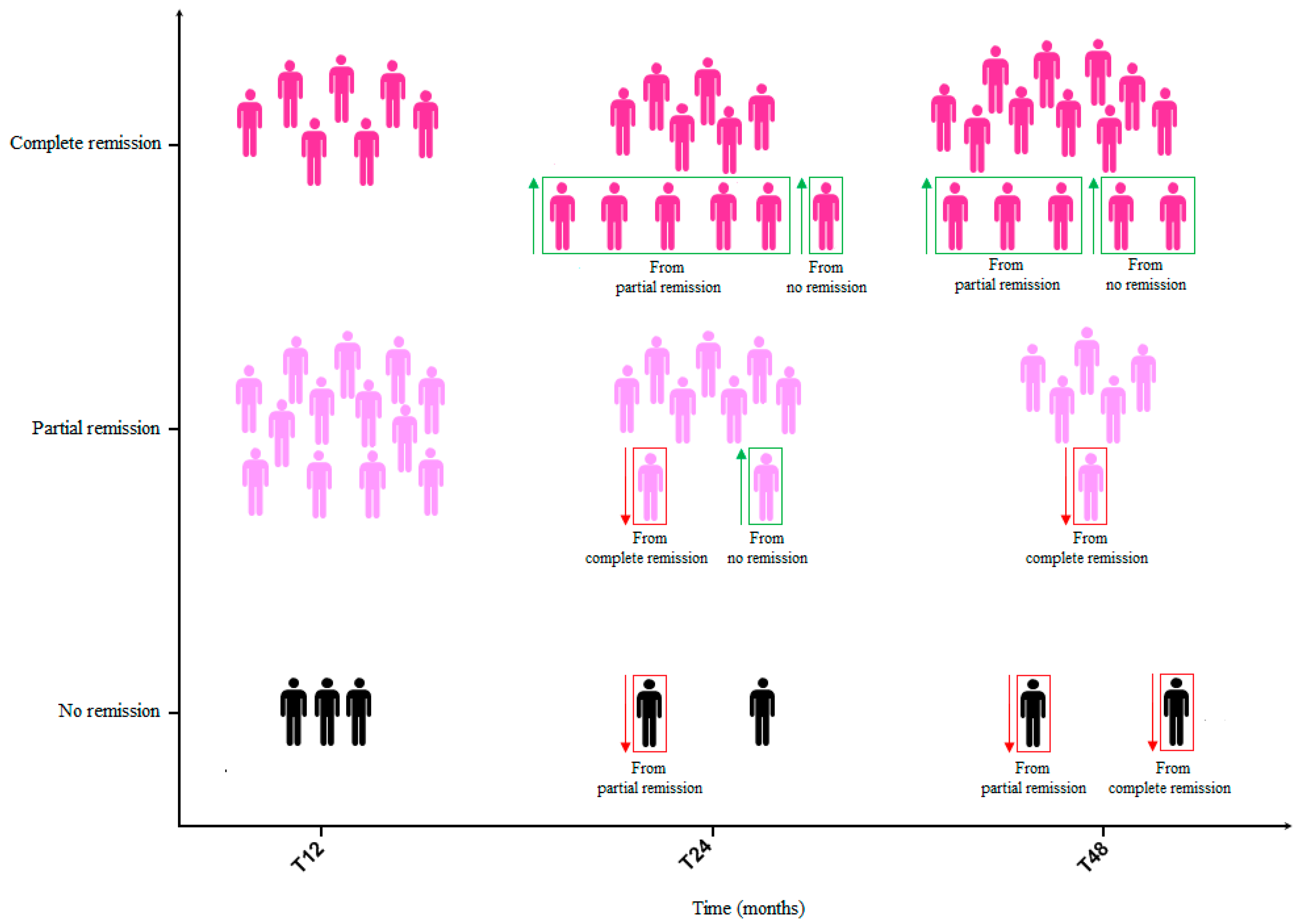
3.4. Clinical Remission Rates After Biological Therapy with Benralizumab
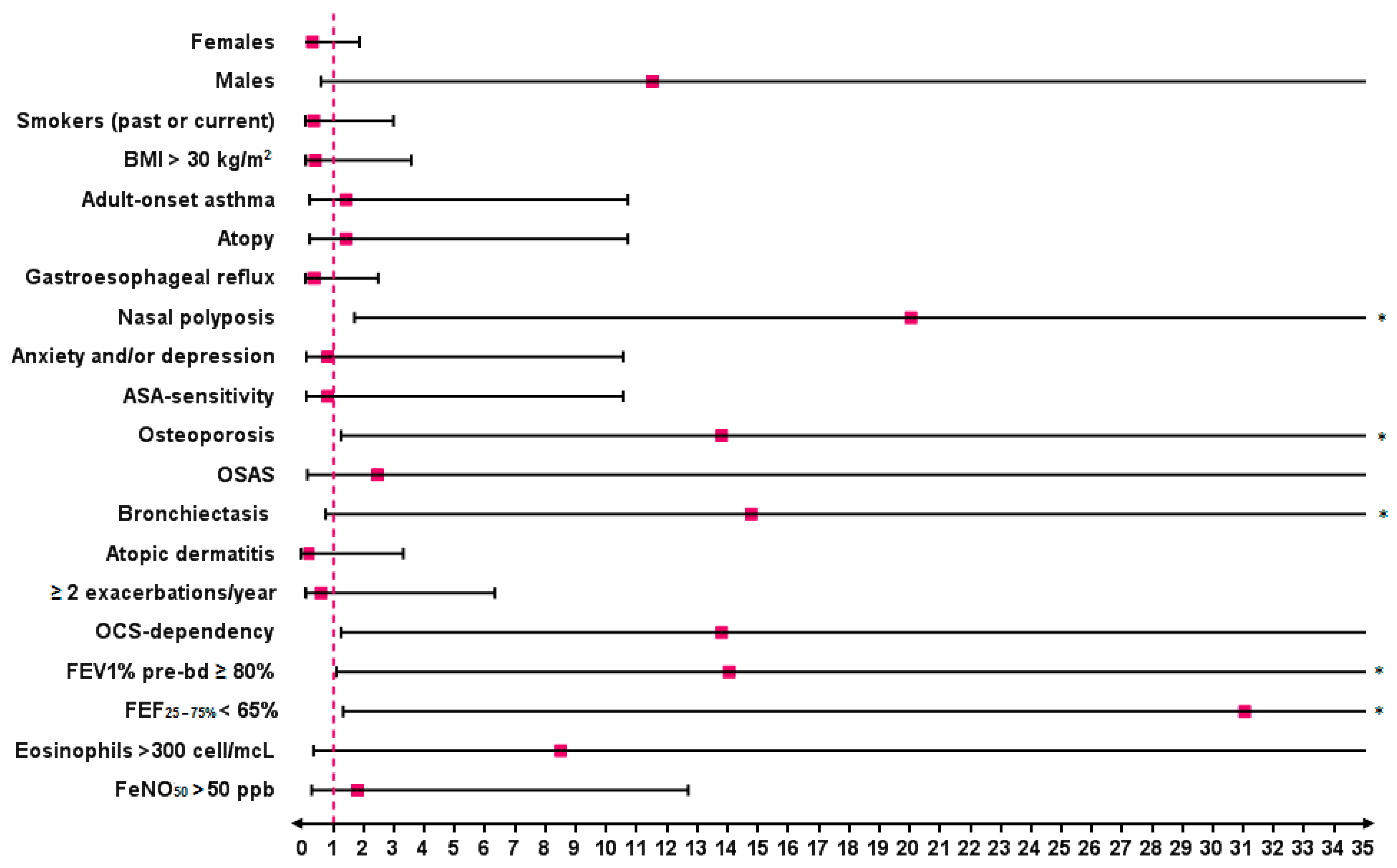
3.5. Baseline Predictors of SEA Complete Clinical Remission After 48 Months of Treatment with Benralizumab
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- 2023 GINA Main Report—Global Initiative for Asthma—GINA. Available online: https://ginasthma.org/2023-gina-main-report/ (accessed on 12 March 2024).
- Foster, J.M.; McDonald, V.M.; Guo, M.; Reddel, H.K. “I have lost in every facet of my life”: The hidden burden of severe asthma. Eur. Respir. J. 2017, 50, 1700765. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, P.; Duh, M.S.; Lafeuille, M.H.; Gozalo, L.; Desai, U.; Robitaille, M.N.; Albers, F.; Yancey, S.; Ortega, H.; Forshag, M.; et al. Acute and chronic systemic corticosteroid-related complications in patients with severe asthma. J. Allergy Clin. Immunol. 2015, 136, 1488–1495. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I.; Weiland, S.K. The International Study of Asthma and Allergies in Childhood (ISAAC). Clin. Exp. Allergy 1998, 28, 52–66. [Google Scholar] [CrossRef] [PubMed]
- The Global Asthma Report 2022. Available online: https://globalasthmareport.org/burden/burden.php (accessed on 12 March 2025).
- Hekking, P.P.W.; Wener, R.R.; Amelink, M.; Zwinderman, A.H.; Bouvy, M.L.; Bel, E.H. The prevalence of severe refractory asthma. J. Allergy Clin. Immunol. 2015, 135, 896–902. [Google Scholar] [CrossRef]
- Von Bülow, A.; Kriegbaum, M.; Backer, V.; Porsbjerg, C. The Prevalence of Severe Asthma and Low Asthma Control Among Danish Adults. J. Allergy Clin. Immunol. Pract. 2014, 2, 759–767.e2. [Google Scholar] [CrossRef]
- Khalaf, K.; Paoletti, G.; Puggioni, F.; Racca, F.; De Luca, F.; Giorgis, V.; Canonica, G.W.; Heffler, E. Asthma from immune pathogenesis to precision medicine. Semin. Immunol. 2019, 46, 101294. [Google Scholar] [CrossRef]
- Lim, H.F.; Nair, P. Airway Inflammation and Inflammatory Biomarkers. Semin. Respir. Crit. Care Med. 2018, 39, 56–63. [Google Scholar] [CrossRef]
- Pelaia, C.; Pelaia, G.; Crimi, C.; Maglio, A.; Stanziola, A.A.; Calabrese, C.; Terracciano, R.; Longhini, F.; Vatrella, A. Novel Biological Therapies for Severe Asthma Endotypes. Biomedicines 2022, 10, 1064. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Bafadhel, M.; Busse, W.W.; Casale, T.B.; Kocks, J.W.H.; Pavord, I.D.; Szefler, S.J.; Woodruff, P.G.; de Giorgio-Miller, A.; Trudo, F.; et al. An expert consensus framework for asthma remission as a treatment goal. J. Allergy Clin. Immunol. 2020, 145, 757–765. [Google Scholar] [CrossRef]
- Canonica, G.W.; Blasi, F.; Carpagnano, G.E.; Guida, G.; Heffler, E.; Paggiaro, P.; Allegrini, C.; Antonelli, A.; Aruanno, A.; Bacci, E.; et al. Severe Asthma Network Italy Definition of Clinical Remission in Severe Asthma: A Delphi Consensus. J. Allergy Clin. Immunol. Pract. 2023, 11, 3629–3637. [Google Scholar] [CrossRef]
- Blaiss, M.; Oppenheimer, J.; Corbett, M.; Bacharier, L.; Bernstein, J.; Carr, T.; Chipps, B.; Couillard, S.; Forno, E.; Grant, T.; et al. Consensus of an American College of Allergy, Asthma, and Immunology, American Academy of Allergy, Asthma, and Immunology, and American Thoracic Society workgroup on definition of clinical remission in asthma on treatment. Ann. Allergy Asthma Immunol. 2023, 131, 782–785. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M.; Bagnasco, D.; Vaia, R.; Senna, G. New horizons for the treatment of severe, eosinophilic asthma: Benralizumab, a novel precision biologic. Biologics. 2019, 13, 89. [Google Scholar] [CrossRef] [PubMed]
- Dagher, R.; Kumar, V.; Copenhaver, A.M.; Gallagher, S.; Ghaedi, M.; Boyd, J.; Newbold, P.; Humbles, A.A.; Kolbeck, R. Novel mechanisms of action contributing to benralizumab’s potent anti-eosinophilic activity. Eur. Respir. J. 2022, 59, 2004306. [Google Scholar] [CrossRef] [PubMed]
- Bleecker, E.R.; FitzGerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkström, V.; et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef]
- FitzGerald, J.M.; Bleecker, E.R.; Nair, P.; Korn, S.; Ohta, K.; Lommatzsch, M.; Ferguson, G.T.; Busse, W.W.; Barker, P.; Sproule, S.; et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2016, 388, 2128–2141. [Google Scholar] [CrossRef]
- Nair, P.; Wenzel, S.; Rabe, K.F.; Bourdin, A.; Lugogo, N.L.; Kuna, P.; Barker, P.; Sproule, S.; Ponnarambil, S.; Goldman, M. Oral Glucocorticoid–Sparing Effect of Benralizumab in Severe Asthma. N. Engl. J. Med. 2017, 376, 2448–2458. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Gurnell, M.; Heaney, L.G.; Corren, J.; Bel, E.H.; Maspero, J.; Harrison, T.; Jackson, D.J.; Price, D.; Lugogo, N.; et al. Oral corticosteroid elimination via a personalised reduction algorithm in adults with severe, eosinophilic asthma treated with benralizumab (PONENTE): A multicentre, open-label, single-arm study. Lancet Respir. Med. 2022, 10, 47–58. [Google Scholar] [CrossRef]
- Vultaggio, A.; Aliani, M.; Altieri, E.; Bracciale, P.; Brussino, L.; Caiaffa, M.F.; Cameli, P.; Canonica, G.W.; Caruso, C.; Centanni, S.; et al. Long-term effectiveness of benralizumab in severe eosinophilic asthma patients treated for 96-weeks: Data from the ANANKE study. Respir. Res. 2023, 24, 135. [Google Scholar] [CrossRef]
- Qin, R.; An, J.; Xie, J.; Huang, R.; Xie, Y.; He, L.; Xv, H.; Qian, G.; Li, J. FEF25-75% Is a More Sensitive Measure Reflecting Airway Dysfunction in Patients with Asthma: A Comparison Study Using FEF25-75% and FEV1%. J. Allergy Clin. Immunol. Pract. 2021, 9, 3649–3659.e6. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.C.; Plummer, A.L.; Taylor, D.R. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Hoyte, F.L.; Price, D.B.; Cohen, D.; Barker, P.; Kreindler, J.; Jison, M.; Brooks, C.L.; Papeleu, P.; Katial, R. Clinical Remission in Severe Asthma: A Pooled Post Hoc Analysis of the Patient Journey with Benralizumab. Adv. Ther. 2022, 39, 2065. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, J.M.; Bleecker, E.R.; Bourdin, A.; Busse, W.W.; Ferguson, G.T.; Brooks, L.; Barker, P.; Martin, U.J. Two-Year Integrated Efficacy And Safety Analysis Of Benralizumab In Severe Asthma. J. Asthma Allergy. 2019, 12, 401. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.; Pelaia, G.; Padilla-Galo, A.; Watt, M.; Kayaniyil, S.; Boarino, S.; Tena, J.S.; Shih, V.; Tran, T.; Arbetter, D.; et al. Asthma Clinical Remission with Benralizumab in an Integrated Analysis of the Real-World XALOC-1 Study. J. Allergy Clin. Immunol. 2023, 151, AB13. [Google Scholar] [CrossRef]
- Padilla-Galo, A.; Moya Carmona, I.; Ausín, P.; Carazo Fernández, L.; García-Moguel, I.; Velasco-Garrido, J.L.; Andújar-Espinosa, R.; Casas-Maldonado, F.; Martínez-Moragón, E.; Martínez Rivera, C.; et al. Achieving clinical outcomes with benralizumab in severe eosinophilic asthma patients in a real-world setting: Orbe II study. Respir. Res. 2023, 24, 235. [Google Scholar] [CrossRef]
- Pelaia, C.; Crimi, C.; Benfante, A.; Caiaffa, M.F.; Campisi, R.; Candia, C.; Carpagnano, G.E.; Carrieri, I.; D’Amato, M.; Detoraki, A.; et al. Sustained remission induced by 2 years of treatment with benralizumab in patients with severe eosinophilic asthma and nasal polyposis. Respirology 2024, 29, 869–879. [Google Scholar] [CrossRef]
- Pini, L.; Bagnasco, D.; Beghè, B.; Braido, F.; Cameli, P.; Caminati, M.; Caruso, C.; Crimi, C.; Guarnieri, G.; Latorre, M.; et al. Unlocking the Long-Term Effectiveness of Benralizumab in Severe Eosinophilic Asthma: A Three-Year Real-Life Study. J. Clin. Med. 2024, 13, 3013. [Google Scholar] [CrossRef]
- Lemanske, R.F. Inflammatory events in asthma: An expanding equation. J. Allergy Clin. Immunol. 2000, 105 Pt 2, S633–S636. [Google Scholar] [CrossRef]
- Agache, I.; Akdis, C.A.; Akdis, M.; Canonica, G.W.; Casale, T.; Chivato, T.; Corren, J.; Chu, D.K.; Del Giacco, S.; Eiwegger, T.; et al. EAACI Biologicals Guidelines—Recommendations for severe asthma. Allergy 2021, 76, 14–44. [Google Scholar] [CrossRef]
- Chan, R.; Lipworth, B.J. Impact of Biologic Therapy on the Small Airways Asthma Phenotype. Lung 2022, 200, 691. [Google Scholar] [CrossRef]
- Sposato, B.; Scalese, M.; Camiciottoli, G.; Carpagnano, G.E.; Pelaia, C.; Santus, P.; Pelaia, G.; Palmiero, G.; Tomassi, M.D.I.; Ronchi, M.C.; et al. Severe asthma and long-term Benralizumab effectiveness in real-life. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 7461–7473. [Google Scholar] [CrossRef]
- Contoli, M.; Santus, P.; Menzella, F.; Rocchi, C.; Radovanovic, D.; Baraldi, F.; Martelli, C.; Casanova, S.; Barbetta, C.; Micheletto, C.; et al. Effects of anti-IL5 biological treatments on blood IgE levels in severe asthmatic patients: A real-life multicentre study (BIONIGE). Clin. Transl. Allergy 2022, 12, e12143. [Google Scholar] [CrossRef] [PubMed]
- Nolasco, S.; Crimi, C.; Pelaia, C.; Benfante, A.; Caiaffa, M.F.; Calabrese, C.; Carpagnano, G.E.; Ciotta, D.; D’Amato, M.; Macchia, L.; et al. Benralizumab Effectiveness in Severe Eosinophilic Asthma with and without Chronic Rhinosinusitis with Nasal Polyps: A Real-World Multicenter Study. J. Allergy Clin. Immunol. Pract. 2021, 9, 4371–4380.e4. [Google Scholar] [CrossRef] [PubMed]
- Bakakos, A.; Schleich, F.; Bakakos, P. Biological Therapy of Severe Asthma and Nasal Polyps. J. Pers. Med. 2022, 12, 976. [Google Scholar] [CrossRef]
- Choi, Y.; Sim, S.; Park, H.S. Distinct functions of eosinophils in severe asthma with type 2 phenotype: Clinical implications. Korean J. Intern. Med. 2020, 35, 823. [Google Scholar] [CrossRef]
- Santomasi, C.; Buonamico, E.; Dragonieri, S.; Iannuzzi, L.; Portacci, A.; Quaranta, N.; Carpagnano, G.E. Effects of benralizumab in a population of patients affected by severe eosinophilic asthma and chronic rhinosinusitis with nasal polyps: A real-life study. Acta Bio. Medica Atenei Parm. 2023, 94, e2023028. [Google Scholar] [CrossRef]
- Campisi, R.; Nolasco, S.; Pelaia, C.; Impellizzeri, P.; D’Amato, M.; Portacci, A.; Ricciardi, L.; Scioscia, G.; Crimi, N.; Scichilone, N.; et al. Benralizumab Effectiveness in Severe Eosinophilic Asthma with Co-Presence of Bronchiectasis: A Real-World Multicentre Observational Study. J. Clin. Med. 2023, 12, 3953. [Google Scholar] [CrossRef]
- Shteinberg, M.; Flume, P.A.; Chalmers, J.D. Is bronchiectasis really a disease? Eur. Respir. Rev. 2020, 29, 190051. [Google Scholar] [CrossRef]
- McIntosh, M.J.; Kooner, H.K.; Eddy, R.L.; Wilson, A.; Serajeddini, H.; Bhalla, A.; Licskai, C.; Mackenzie, C.A.; Yamashita, C.; Parraga, G. CT Mucus Score and 129Xe MRI Ventilation Defects After 2.5 Years’ Anti-IL-5Rα in Eosinophilic Asthma. Chest 2023, 164, 27–38. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Scioscia, G.; Lacedonia, D.; Curradi, G.; Barbaro, M.P.F. Severe uncontrolled asthma with bronchiectasis: A pilot study of an emerging phenotype that responds to mepolizumab. J. Asthma Allergy 2019, 12, 83. [Google Scholar] [CrossRef]
- Sposato, B.; Bianchi, F.; Ricci, A.; Scalese, M. Clinical Asthma Remission Obtained with Biologics in Real Life: Patients’ Prevalence and Characteristics. J. Pers. Med. 2023, 13, 1020. [Google Scholar] [CrossRef]
- Perez-de-Llano, L.; Scelo, G.; Tran, T.N.; Le, T.T.; Fagerås, M.; Cosio, B.G.; Peters, M.; Pfeffer, P.E.; Al-Ahmad, M.; Al-Lehebi, R.O.; et al. Exploring Definitions and Predictors of Severe Asthma Clinical Remission Post-Biologic in Adults. Am. J. Respir. Crit. Care Med. 2024, 41, 869–880. [Google Scholar] [CrossRef]
- Thomas, D.; McDonald, V.M.; Pavord, I.D.; Gibson, P.G. Asthma remission: What is it and how can it be achieved? Eur. Respir. J. 2022, 60, 2102583. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Results (n = 23) |
|---|---|
| Age, years (mean ± SD) | 58.30 ± 10.26 |
| Females, n (%) | 16 (69.6%) |
| Males, n (%) | 7 (30.4%) |
| Smokers (ex or current), n (%) | 5 (21.7%) |
| BMI, kg/m2 (mean ± SD) | 27.25 ± 5.00 |
| Asthma onset, years (mean ± SD) | 34.26 ± 12.95 |
| Childhood onset, n (%) | 6 (26.1%) |
| Adult onset, n (%) | 17 (73.9%) |
| Atopy, n (%) | 17 (73.9%) |
| Nasal polyposis, n (%) | 14 (60.9%) |
| Gastroesophageal reflux, n (%) | 10 (43.5%) |
| ASA sensitivity, n (%) | 3 (13.0%) |
| Bronchiectasis, n (%) | 8 (34.8%) |
| Anxiety and/or depression, n (%) | 3 (13.0%) |
| Osteoporosis, n (%) | 12 (52.2%) |
| OSAS, n (%) | 2 (8.7%) |
| Atopic dermatitis, n (%) | 2 (8.7%) |
| Exacerbation patients, n (%) | 21 (91.3%) |
| Exacerbation/year, n (mean ± SD) | 2.61 ± 1.33 |
| OCS-dependent patients, n (%) | 13 (56.5%) |
| OCS dosage, mg (mean ± SD) | 18.48 ± 12.85 |
| ACT score (mean ± SD) | 14.57 ± 2.45 |
| FEV1%pre-bd, (mean ± SD) | 66.52 ± 15.94 |
| FEV1 Lpre-bd (mean ± SD) | 1.95 ± 0.62 |
| FEF25–75% (mean ± SD) | 36.83 ± 11.50 |
| Eosinophils, cell/mcL (mean ± SD) | 670.87 ± 237.26 |
| Eosinophils > 300 cell/mcL, n (%) | 22 (95.6%) |
| FeNO50, ppb (mean ± SD) | 48.43 ± 14.79 |
| FeNO50 > 50 ppb, n (%) | 9 (39.1%) |
| Total IgE, kU/L (mean ± SD) | 235.18 ± 219.65 |
| Clinical Outcomes | T0 | T12 | T24 | T36 | T48 |
|---|---|---|---|---|---|
| Exacerbations; mean ± SD (range) | 2.61 ± 1.33 (0–6) | 0.30 ± 0.45 (0–2) | 0.22 ± 0.34 (0–2) | 0.09 ± 0.16 (0–1) | 0.13 ± 0.23 (0–1) |
| p-value (T0 vs. T12) < 0.0001 * | |||||
| p-value (T0 vs. T24) < 0.0001 * | |||||
| p-value (T0 vs. T36) < 0.0001 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| Exacerbation patients (n, %) | 21 (91.3%) | 4 (17.4%) | 3 (23.1%) | 1 (4.3%) | 3 (23.1%) |
| p-value (T0 vs. T12) < 0.0001 * | |||||
| p-value (T0 vs. T24) < 0.0001 * | |||||
| p-value (T0 vs. T36) < 0.0001 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| Prednisone dose, mg; mean ± SD | 18.48 ± 12.85 | 3.48 ± 5.75 | 2.17 ± 3.97 | 1.09 ± 2.08 | 1.61 ± 2.94 |
| p-value (T0 vs. T12) 0.0002 * | |||||
| p-value (T0 vs. T24) < 0.0001 * | |||||
| p-value (T0 vs. T36) < 0.0001 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| Patients requiring OCS (n, %) | 13 (56.5%) | 4 (17.4%) | 3 (13.0%) | 1 (4.3%) | 2 (8.7%) |
| p-value (T0 vs. T12) 0.01 * | |||||
| p-value (T0 vs. T24) 0.0045 * | |||||
| p-value (T0 vs. T36) 0.0002 * | |||||
| p-value (T0 vs. T48) 0.001 * | |||||
| FEV1pre-bd %; mean ± SD | 66.52 ± 15.94 | 81.30 ± 15.44 | 81.35 ± 17.81 | 85.39 ± 14.93 | 87.14 ± 15.32 |
| p-value (T0 vs. T12) 0.02 * | |||||
| p-value (T0 vs. T24) 0.02 * | |||||
| p-value (T0 vs. T36) 0.002 * | |||||
| p-value (T0 vs. T48) 0.0008 * | |||||
| FEV1 gain, mL; mean ± SD | - | 296 ± 257 | 617 ± 273 | 891 ± 270 | 1145 ± 258 |
| p-value (T0 vs. T12) 0.07 * | |||||
| p-value (T0 vs. T24) 0.03 * | |||||
| p-value (T0 vs. T36) 0.002 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| FEF25–75%; mean ± SD | 36.83 ± 11.50 | 53.55 ± 24.28 | 59.95 ± 26.04 | 63.05 ± 19.78 | 66.21 ± 20.79 |
| p-value (T0 vs. T12) 0.02 * | |||||
| p-value (T0 vs. T24) 0.006 * | |||||
| p-value (T0 vs. T36) < 0.0001 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| ACT score; mean ± SD | 14.57 ± 2.45 | 22.30 ± 2.00 | 23.35 ± 1.58 | 24.39 ± 0.79 | 24.52 ± 0.75 |
| p-value (T0 vs. T12) < 0.0001 * | |||||
| p-value (T0 vs. T24) < 0.0001 * | |||||
| p-value (T0 vs. T36) < 0.0001 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| Markers | T0 | T12 | T24 | T36 | T48 |
|---|---|---|---|---|---|
| Eosinophils, cell/mcL; mean ± SD | 670.87 ± 237.26 | 52.57 ± 89.12 | 3.91 ± 6.81 | 0.87 ± 1.66 | 0.87 ± 1.66 |
| p-value (T0 vs. T12) < 0.0001 * | |||||
| p-value (T0 vs. T24) < 0.0001 * | |||||
| p-value (T0 vs. T36) < 0.0001 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| FeNO50, ppb; mean ± SD | 48.43 ± 14.79 | 28.83 ± 11.93 | 21.38 ± 7.83 | 16.75 ± 4.76 | 14.61 ± 4.76 |
| p-value (T0 vs. T12) 0.002 * | |||||
| p-value (T0 vs. T24) < 0.0001 * | |||||
| p-value (T0 vs. T36) < 0.0001 * | |||||
| p-value (T0 vs. T48) < 0.0001 * | |||||
| Total IgE, kU/L; mean ± SD | 235.18 ± 219.65 | 114.19 ± 109.20 | 65.17 ± 43.84 | 52.88 ± 36.97 | 37.78 ± 22.87 |
| p-value (T0 vs. T12) 0.21 | |||||
| p-value (T0 vs. T24) 0.06 | |||||
| p-value (T0 vs. T36) 0.04 * | |||||
| p-value (T0 vs. T48) 0.02 * | |||||
| Characteristics at T0 | Complete Remission at T48 | OR | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|
| Yes (n = 15) | No (n = 6) | |||||
| Females | 8 (53.3%) | 6 (100.0%) | 0.09 | 0.01 | 1.82 | 0.06 |
| Males | 7 (46.7%) | 0 (0.0%) | 11.47 | 0.55 | 239.80 | 0.06 |
| Smokers (past or current) | 2 (13.3%) | 2 (33.3%) | 0.31 | 0.03 | 2.94 | 0.54 |
| BMI > 30 kg/m2 | 4 (26.7%) | 2 (33.3%) | 0.36 | 0.04 | 3.52 | 0.56 |
| Adult-onset asthma | 11 (73.3%) | 4 (66.7%) | 1.37 | 0.18 | 10.66 | 1.00 |
| Atopy | 11 (73.3%) | 4 (66.7%) | 1.37 | 0.18 | 10.66 | 1.00 |
| Gastroesophageal reflux | 6 (40.0%) | 4 (66.7%) | 0.33 | 0.04 | 2.43 | 0.36 |
| Nasal polyposis | 12 (80.0%) | 1 (16.7%) | 20.00 | 1.65 | 241.90 | 0.01 * |
| Anxiety and/or depression | 2 (13.3%) | 1 (16.7%) | 0.77 | 0.06 | 10.50 | 1.00 |
| ASA sensitivity | 2 (12.3%) | 1 (16.7%) | 0.77 | 0.06 | 10.50 | 1.00 |
| Osteoporosis | 11 (73.3%) | 1 (16.7%) | 13.75 | 1.21 | 156.70 | 0.04 * |
| OSAS | 2 (13.3%) | 0 (0.0%) | 2.41 | 0.10 | 57.78 | 1.00 |
| Bronchiectasis | 8 (53.3%) | 0 (0.0%) | 14.73 | 0.70 | 308.10 | 0.04 * |
| Atopic dermatitis | 0 (0.0%) | 1 (16.7%) | 0.12 | 0.01 | 3.26 | 0.28 |
| ≥2 exacerbations/year | 11 (73.3%) | 5 (83.3%) | 0.55 | 0.05 | 6.27 | 1.00 |
| OCS dependency | 11 (73.3%) | 1 (16.7%) | 13.75 | 1.21 | 156.70 | 0.04 * |
| FEV1%pre-bd ≥ 80% | 14 (93.3%) | 3 (50.0%) | 14.00 | 1.06 | 185.60 | 0.05 * |
| FEF25–75% < 65% | 15 (100.0%) | 3 (50.0%) | 31.00 | 1.28 | 747.60 | 0.01 * |
| Eosinophils > 300 cell/mcL | 15 (100.0%) | 5 (83.3%) | 8.45 | 0.30 | 240.00 | 0.28 |
| FeNO50 > 50 ppb | 7 (46.7%) | 2 (33.3%) | 1.75 | 0.24 | 12.65 | 0.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quarato, C.M.I.; Tondo, P.; Lacedonia, D.; Soccio, P.; Pescatore, D.; Baccellieri, M.L.; Lepore, G.; Foschino Barbaro, M.P.; Scioscia, G. Long-Term Clinical Remission on Benralizumab Treatment in Severe Eosinophilic Asthma: A Four-Year Real-Life Study. J. Clin. Med. 2025, 14, 2075. https://doi.org/10.3390/jcm14062075
Quarato CMI, Tondo P, Lacedonia D, Soccio P, Pescatore D, Baccellieri ML, Lepore G, Foschino Barbaro MP, Scioscia G. Long-Term Clinical Remission on Benralizumab Treatment in Severe Eosinophilic Asthma: A Four-Year Real-Life Study. Journal of Clinical Medicine. 2025; 14(6):2075. https://doi.org/10.3390/jcm14062075
Chicago/Turabian StyleQuarato, Carla Maria Irene, Pasquale Tondo, Donato Lacedonia, Piera Soccio, Dalila Pescatore, Maria Lisa Baccellieri, Giorgia Lepore, Maria Pia Foschino Barbaro, and Giulia Scioscia. 2025. "Long-Term Clinical Remission on Benralizumab Treatment in Severe Eosinophilic Asthma: A Four-Year Real-Life Study" Journal of Clinical Medicine 14, no. 6: 2075. https://doi.org/10.3390/jcm14062075
APA StyleQuarato, C. M. I., Tondo, P., Lacedonia, D., Soccio, P., Pescatore, D., Baccellieri, M. L., Lepore, G., Foschino Barbaro, M. P., & Scioscia, G. (2025). Long-Term Clinical Remission on Benralizumab Treatment in Severe Eosinophilic Asthma: A Four-Year Real-Life Study. Journal of Clinical Medicine, 14(6), 2075. https://doi.org/10.3390/jcm14062075