
Predicting New-Onset Atrial Fibrillation in Hypertrophic Cardiomyopathy: A Review

 ,
,  , ,
, ,  , ,
, ,  ,
, 
Abstract

1. Introduction
2. Electrocardiographic Markers
3. Clinical Markers
4. Genetic Implications
5. Structural and Mechanical Left Atrial Remodeling Detected by Imaging Techniques
6. Limitations
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| HCM | Hypertrophic cardiomyopathy |
| LV | Left ventricle |
| AF | Atrial fibrillation |
| ECG | Electrocardiogram |
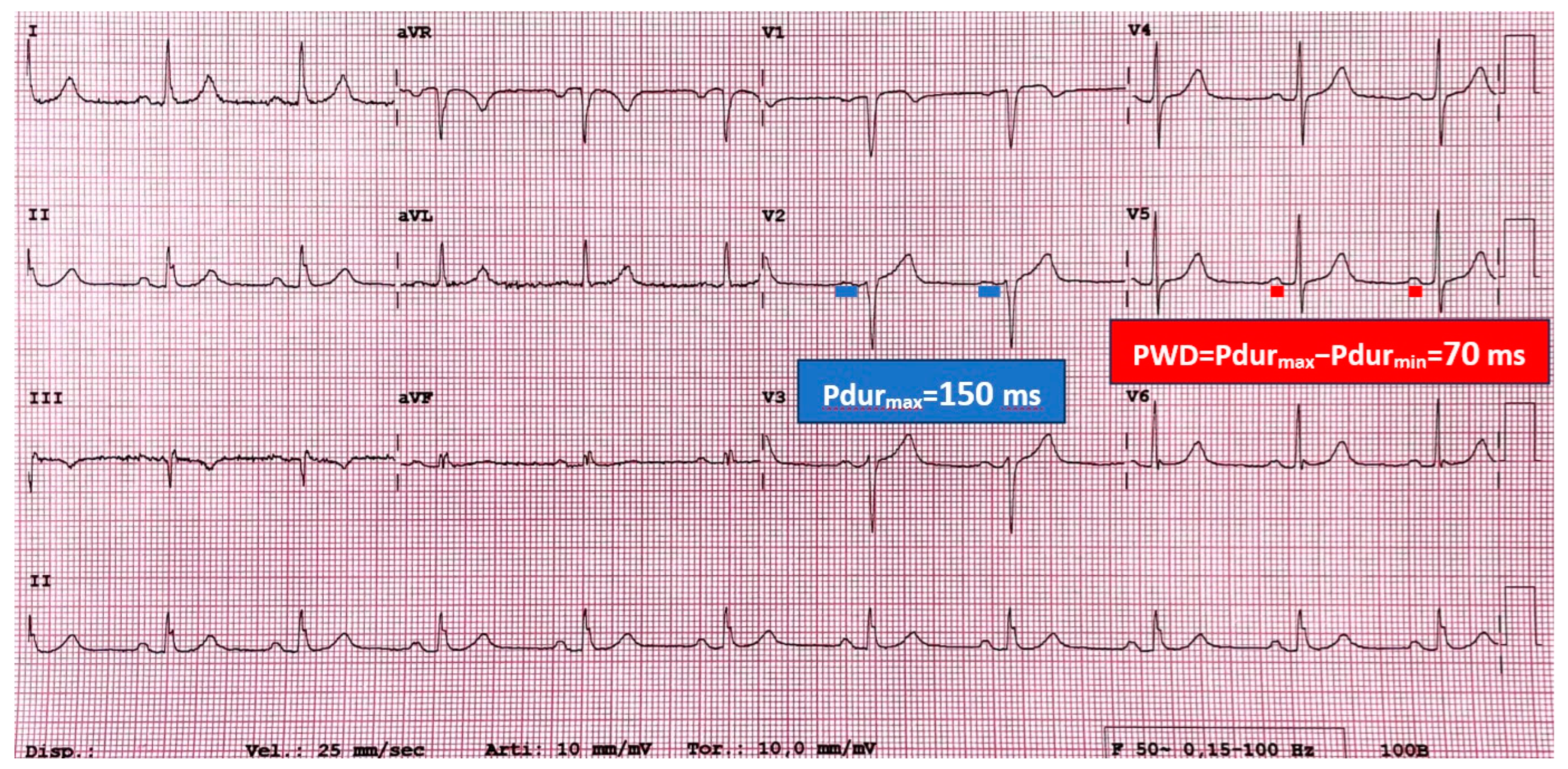
| Pdur | P-wave duration |
| PWD | P-wave dispersion |
| Pdurmax | Maximum P-wave duration |
| LA | Left atrium |
| BMI | Body mass index |
| NYHA | New York Heart Association |
| HF | Heart failure |
| CV | Cerebrovascular accidents |
| β-MHC | β-cardiac myosin heavy chain |
| RAAS | Renin–angiotensin–aldosterone system |
| LVOT | Left ventricular outflow tract |
| ACM | Atrial cardiomyopathy |
| LAVI | Left atrial volume index |
| CMR | Cardiovascular magnetic resonance |
| LAEF | Left atrial ejection fraction |
| LATEF | Left atrial total emptying fraction |
| LAAEF | Left atrial active emptying fraction |
| LGE | Late gadolinium enhancement |
| LACI | Left atrioventricular coupling index |
| EAT | Epicardial adipose tissue |
References
- Maron, B.J.; Desai, M.Y.; Nishimura, R.A.; Spirito, P.; Rakowski, H.; Towbin, J.A.; Dearani, J.A.; Rowin, E.J.; Maron, M.S.; Sherrid, M.V. Management of Hypertrophic Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 390–414. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; de Boer, R.A.; et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur. Heart J. 2023, 44, 3503–3626. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, G.; Sheikh, N.; Biagini, E.; Papadakis, M.; Maurizi, N.; Sinagra, G.; Pelliccia, A.; Rapezzi, C.; Sharma, S.; Olivotto, I. The electrocardiogram in the diagnosis and management of patients with hypertrophic cardiomyopathy. Heart Rhythm 2020, 17, 142–151. [Google Scholar] [CrossRef]
- Ommen, S.R.; Ho, C.Y.; Asif, I.M.; Balaji, S.; Burke, M.A.; Day, S.M.; Dearani, J.A.; Epps, K.C.; Evanovich, L.; Ferrari, V.A.; et al. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the Management of Hypertrophic Cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1239–e1311. [Google Scholar] [CrossRef]
- D’Onofrio, A.; Marini, M.; Rovaris, G.; Zanotto, G.; Calvi, V.; Iacopino, S.; Biffi, M.; Solimene, F.; Della Bella, P.; Caravati, F.; et al. Prognostic significance of remotely monitored nocturnal heart rate in heart failure patients with reduced ejection fraction. Heart Rhythm 2023, 20, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Gardin, J.M.; Flack, J.M.; Gidding, S.S.; Kurosaki, T.T.; Bild, D.E. Prevalence of hypertrophic cardiomyopathy in a general population of young adults. Echocardiographic analysis of 4111 subjects in the CARDIA Study. Coronary Artery Risk Development in (Young) Adults. Circulation 1995, 92, 785–789. [Google Scholar] [CrossRef]
- Robinson, K.; Frenneaux, M.P.; Stockins, B.; Karatasakis, G.; Poloniecki, J.D.; McKenna, W.J. Atrial fibrillation in hypertrophic cardiomyopathy: A longitudinal study. J. Am. Coll. Cardiol. 1990, 15, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.; Cecchi, F.; Casey, S.A.; Dolara, A.; Traverse, J.H.; Maron, B.J. Impact of atrial fibrillation on the clinical course of hypertrophic cardiomyopathy. Circulation 2001, 104, 2517–2524. [Google Scholar] [CrossRef]
- Tian, T.; Wang, Y.; Sun, K.; Wang, J.; Zou, Y.; Zhang, W.; Bao, J.; Zhu, L.; Shen, H.; Hui, R.; et al. Clinical profile and prognostic significance of atrial fibrillation in hypertrophic cardiomyopathy. Cardiology 2013, 126, 258–264. [Google Scholar] [CrossRef]
- Costabel, J.P.; Galve, E.; Terricabras, M.; Ametrano, C.; Ronderos, R.; Baranchuk, A.; Evangelista, A.; Avegliano, G. E/e’ ratio and left atrial area are predictors of atrial fibrillation in patients with hypertrophic cardiomyopathy. Echocardiography 2018, 35, 935–940. [Google Scholar] [CrossRef]
- Merlo, M.; Porcari, A.; Pagura, L.; Cameli, M.; Vergaro, G.; Musumeci, B.; Biagini, E.; Canepa, M.; Crotti, L.; Imazio, M.; et al. A national survey on prevalence of possible echocardiographic red flags of amyloid cardiomyopathy in consecutive patients undergoing routine echocardiography: Study design and patients characterization-the first insight from the AC-TIVE Study. Eur. J. Prev. Cardiol. 2021, 29, e173–e177. [Google Scholar] [CrossRef] [PubMed]
- Pagura, L.; Porcari, A.; Cameli, M.; Biagini, E.; Canepa, M.; Crotti, L.; Imazio, M.; Forleo, C.; Pavasini, R.; Limongelli, G.; et al. ECG/echo indexes in the diagnostic approach to amyloid cardiomyopathy: A head-to-head comparison from the AC-TIVE study. Eur. J. Intern. Med. 2023, 122, 68–77. [Google Scholar] [CrossRef]
- Dilaveris, P.E.; Gialafos, E.J.; Sideris, S.K.; Theopistou, A.M.; Andrikopoulos, G.K.; Kyriakidis, M.; Gialafos, J.E.; Toutouzas, P.K. Simple electrocardiographic markers for the prediction of paroxysmal idiopathic atrial fibrillation. Am. Heart J. 1998, 135, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Mandes, L.; Rosca, M.; Ciuperca, D.; Calin, A.; Beladan, C.C.; Enache, R.; Cuculici, A.; Baicus, C.; Jurcut, R.; Ginghina, C.; et al. Electrocardiographic and Echocardiographic Predictors of Atrial Fibrillation in Patients With Hypertrophic Cardiomyopathy. Front. Cardiovasc. Med. 2022, 9, 905128. [Google Scholar] [CrossRef]
- Cecchi, F.; Montereggi, A.; Olivotto, I.; Marconi, P.; Dolara, A.; Maron, B.J. Risk for atrial fibrillation in patients with hypertrophic cardiomyopathy assessed by signal averaged P wave duration. Heart 1997, 78, 44–49. [Google Scholar] [CrossRef]
- Ozdemir, O.; Soylu, M.; Demir, A.D.; Topaloglu, S.; Alyan, O.; Turhan, H.; Bicer, A.; Kutuk, E. P-wave durations as a predictor for atrial fibrillation development in patients with hypertrophic cardiomyopathy. Int. J. Cardiol. 2004, 94, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Girasis, C.; Vassilikos, V.; Efthimiadis, G.K.; Papadopoulou, S.L.; Dakos, G.; Dalamaga, E.G.; Chouvarda, I.; Giannakoulas, G.; Kamperidis, V.; Paraskevaidis, S.; et al. Patients with hypertrophic cardiomyopathy at risk for paroxysmal atrial fibrillation: Advanced echocardiographic evaluation of the left atrium combined with non-invasive P-wave analysis. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 425–434. [Google Scholar] [CrossRef]
- Tuluce, K.; Yakar Tuluce, S.; Kahya Eren, N.; Kocabas, U.; Akyildiz Akcay, F.; Gunduz, R.; Akyildiz, Z.I.; Ergene, O. Predictors of Future Atrial Fibrillation Development in Patients with Hypertrophic Cardiomyopathy: A Prospective Follow-Up Study. Echocardiography 2016, 33, 379–385. [Google Scholar] [CrossRef]
- Kose, S.; Aytemir, K.; Sade, E.; Can, I.; Ozer, N.; Amasyali, B.; Aksoyek, S.; Ovunc, K.; Ozmen, F.; Atalar, E.; et al. Detection of patients with hypertrophic cardiomyopathy at risk for paroxysmal atrial fibrillation during sinus rhythm by P-wave dispersion. Clin. Cardiol. 2003, 26, 431–434. [Google Scholar] [CrossRef]
- Aytemir, K.; Ozer, N.; Atalar, E.; Sade, E.; Aksoyek, S.; Ovunc, K.; Oto, A.; Ozmen, F.; Kes, S. P wave dispersion on 12-lead electrocardiography in patients with paroxysmal atrial fibrillation. Pacing Clin. Electrophysiol. 2000, 23, 1109–1112. [Google Scholar] [CrossRef]
- Hopkins, C.B.; Barrett, O., Jr. Electrocardiographic diagnosis of left atrial enlargement. Role of the P terminal force in lead V1. J. Electrocardiol. 1989, 22, 359–363. [Google Scholar] [CrossRef]
- Tjahjadi, C.; Hiemstra, Y.L.; van der Bijl, P.; Pio, S.M.; Bootsma, M.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Assessment of left atrial electro-mechanical delay to predict atrial fibrillation in hypertrophic cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Siontis, K.C.; Geske, J.B.; Ong, K.; Nishimura, R.A.; Ommen, S.R.; Gersh, B.J. Atrial fibrillation in hypertrophic cardiomyopathy: Prevalence, clinical correlations, and mortality in a large high-risk population. J. Am. Heart Assoc. 2014, 3, e001002. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Olivotto, I.; Bellone, P.; Conte, M.R.; Cecchi, F.; Flygenring, B.P.; Casey, S.A.; Gohman, T.E.; Bongioanni, S.; Spirito, P. Clinical profile of stroke in 900 patients with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2002, 39, 301–307. [Google Scholar] [CrossRef]
- Maron, B.J.; Haas, T.S.; Maron, M.S.; Lesser, J.R.; Browning, J.A.; Chan, R.H.; Olivotto, I.; Garberich, R.F.; Schwartz, R.S. Left atrial remodeling in hypertrophic cardiomyopathy and susceptibility markers for atrial fibrillation identified by cardiovascular magnetic resonance. Am. J. Cardiol. 2014, 113, 1394–1400. [Google Scholar] [CrossRef]
- Klopotowski, M.; Kwapiszewska, A.; Kukula, K.; Jamiolkowski, J.; Dabrowski, M.; Derejko, P.; Oreziak, A.; Baranowski, R.; Spiewak, M.; Marczak, M.; et al. Clinical and echocardiographic parameters as risk factors for atrial fibrillation in patients with hypertrophic cardiomyopathy. Clin. Cardiol. 2018, 41, 1336–1340. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.M.; DiMarco, J.P.; Kolm, P.; Ho, C.Y.; Desai, M.Y.; Kwong, R.Y.; Dolman, S.F.; Desvigne-Nickens, P.; Geller, N.; Kim, D.Y.; et al. Predictors of Major Atrial Fibrillation Endpoints in the National Heart, Lung, and Blood Institute HCMR. JACC Clin. Electrophysiol. 2021, 7, 1376–1386. [Google Scholar] [CrossRef]
- Cochet, H.; Morlon, L.; Verge, M.P.; Salel, M.; Camaioni, C.; Reynaud, A.; Peyrou, J.; Ritter, P.; Jais, P.; Laurent, F.; et al. Predictors of future onset of atrial fibrillation in hypertrophic cardiomyopathy. Arch. Cardiovasc. Dis. 2018, 111, 591–600. [Google Scholar] [CrossRef]
- Santobuono, V.E.; Favale, S.; D’Onofrio, A.; Manzo, M.; Calò, L.; Bertini, M.; Savarese, G.; Santini, L.; Dello Russo, A.; Lavalle, C.; et al. Performance of a multisensor implantable defibrillator algorithm for heart failure monitoring related to co-morbidities. ESC Heart Fail. 2023, 10, 2469–2478. [Google Scholar] [CrossRef]
- Carrick, R.T.; Maron, M.S.; Adler, A.; Wessler, B.; Hoss, S.; Chan, R.H.; Sridharan, A.; Huang, D.; Cooper, C.; Drummond, J.; et al. Development and Validation of a Clinical Predictive Model for Identifying Hypertrophic Cardiomyopathy Patients at Risk for Atrial Fibrillation: The HCM-AF Score. Circ. Arrhythm. Electrophysiol. 2021, 14, e009796. [Google Scholar] [CrossRef]
- Lee, S.E.; Park, J.K.; Uhm, J.S.; Kim, J.Y.; Pak, H.N.; Lee, M.H.; Joung, B. Impact of atrial fibrillation on the clinical course of apical hypertrophic cardiomyopathy. Heart 2017, 103, 1496–1501. [Google Scholar] [CrossRef]
- Guttmann, O.P.; Pavlou, M.; O’Mahony, C.; Monserrat, L.; Anastasakis, A.; Rapezzi, C.; Biagini, E.; Gimeno, J.R.; Limongelli, G.; Garcia-Pavia, P.; et al. Prediction of thrombo-embolic risk in patients with hypertrophic cardiomyopathy (HCM Risk-CVA). Eur. J. Heart Fail. 2015, 17, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Fauchier, L.; Bisson, A.; Bodin, A.; Herbert, J.; Spiesser, P.; Pierre, B.; Clementy, N.; Bernard, A.; Babuty, D.; Lip, G.Y.H. Ischemic Stroke in Patients With Hypertrophic Cardiomyopathy According to Presence or Absence of Atrial Fibrillation. Stroke 2022, 53, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, M.; Lu, D.Y.; Ventoulis, I.; Greenland, G.V.; Yalcin, H.; Guan, Y.; Marine, J.E.; Olgin, J.E.; Zimmerman, S.L.; Abraham, T.P.; et al. Machine Learning Methods for Identifying Atrial Fibrillation Cases and Their Predictors in Patients With Hypertrophic Cardiomyopathy: The HCM-AF-Risk Model. CJC Open 2021, 3, 801–813. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.; Cecchi, F.; Poggesi, C.; Yacoub, M.H. Patterns of disease progression in hypertrophic cardiomyopathy: An individualized approach to clinical staging. Circ. Heart Fail. 2012, 5, 535–546. [Google Scholar] [CrossRef]
- Gruver, E.J.; Fatkin, D.; Dodds, G.A.; Kisslo, J.; Maron, B.J.; Seidman, J.G.; Seidman, C.E. Familial hypertrophic cardiomyopathy and atrial fibrillation caused by Arg663His beta-cardiac myosin heavy chain mutation. Am. J. Cardiol. 1999, 83, 13H–18H. [Google Scholar] [CrossRef]
- Eiras, S.; Narolska, N.A.; van Loon, R.B.; Boontje, N.M.; Zaremba, R.; Jimenez, C.R.; Visser, F.C.; Stooker, W.; van der Velden, J.; Stienen, G.J. Alterations in contractile protein composition and function in human atrial dilatation and atrial fibrillation. J. Mol. Cell. Cardiol. 2006, 41, 467–477. [Google Scholar] [CrossRef]
- Maron, B.J.; Maron, M.S. Hypertrophic cardiomyopathy. Lancet 2013, 381, 242–255. [Google Scholar] [CrossRef]
- Olivotto, I.; Maron, B.J.; Cecchi, F. Clinical significance of atrial fibrillation in hypertrophic cardiomyopathy. Curr. Cardiol. Rep. 2001, 3, 141–146. [Google Scholar] [CrossRef]
- Bassiouny, M.; Lindsay, B.D.; Lever, H.; Saliba, W.; Klein, A.; Banna, M.; Abraham, J.; Shao, M.; Rickard, J.; Kanj, M.; et al. Outcomes of nonpharmacologic treatment of atrial fibrillation in patients with hypertrophic cardiomyopathy. Heart Rhythm 2015, 12, 1438–1447. [Google Scholar] [CrossRef]
- Olivotto, I.; Girolami, F.; Ackerman, M.J.; Nistri, S.; Bos, J.M.; Zachara, E.; Ommen, S.R.; Theis, J.L.; Vaubel, R.A.; Re, F.; et al. Myofilament protein gene mutation screening and outcome of patients with hypertrophic cardiomyopathy. Mayo Clin. Proc. 2008, 83, 630–638. [Google Scholar] [CrossRef]
- Bongini, C.; Ferrantini, C.; Girolami, F.; Coppini, R.; Arretini, A.; Targetti, M.; Bardi, S.; Castelli, G.; Torricelli, F.; Cecchi, F.; et al. Impact of Genotype on the Occurrence of Atrial Fibrillation in Patients With Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2016, 117, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Perkins, M.J.; Van Driest, S.L.; Ellsworth, E.G.; Will, M.L.; Gersh, B.J.; Ommen, S.R.; Ackerman, M.J. Gene-specific modifying effects of pro-LVH polymorphisms involving the renin-angiotensin-aldosterone system among 389 unrelated patients with hypertrophic cardiomyopathy. Eur. Heart J. 2005, 26, 2457–2462. [Google Scholar] [CrossRef] [PubMed]
- White, P.C. Disorders of aldosterone biosynthesis and action. N. Engl. J. Med. 1994, 331, 250–258. [Google Scholar] [CrossRef]
- Curnow, K.M.; Tusie-Luna, M.T.; Pascoe, L.; Natarajan, R.; Gu, J.L.; Nadler, J.L.; White, P.C. The product of the CYP11B2 gene is required for aldosterone biosynthesis in the human adrenal cortex. Mol. Endocrinol. 1991, 5, 1513–1522. [Google Scholar] [CrossRef]
- Challa, A.A.; Vukmirovic, M.; Blackmon, J.; Stefanovic, B. Withaferin-A reduces type I collagen expression in vitro and inhibits development of myocardial fibrosis in vivo. PLoS ONE 2012, 7, e42989. [Google Scholar] [CrossRef]
- Orenes-Pinero, E.; Hernandez-Romero, D.; Romero-Aniorte, A.I.; Martinez, M.; Garcia-Honrubia, A.; Caballero, L.; Garrigos-Gomez, N.; Andreu-Cayuelas, J.M.; Gonzalez, J.; Feliu, E.; et al. Prognostic value of two polymorphisms in non-sarcomeric genes for the development of atrial fibrillation in patients with hypertrophic cardiomyopathy. QJM 2014, 107, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Belenkov, Y.N.; Privalova, E.V.; Kaplunova, V.Y.; Stambol’skii, D.V.; Fomin, A.A. Analysis of morpho-functional parameters of the heart and polymorphisms of Renin-Angiotensin-aldosterone system genes in patients with different variants of the course of hypertrophic cardiomyopathy. Kardiologiia 2010, 50, 27–34. [Google Scholar]
- Christophersen, I.E.; Ellinor, P.T. Genetics of atrial fibrillation: From families to genomes. J. Hum. Genet. 2016, 61, 61–70. [Google Scholar] [CrossRef]
- Nielsen, J.B.; Fritsche, L.G.; Zhou, W.; Teslovich, T.M.; Holmen, O.L.; Gustafsson, S.; Gabrielsen, M.E.; Schmidt, E.M.; Beaumont, R.; Wolford, B.N.; et al. Genome-wide Study of Atrial Fibrillation Identifies Seven Risk Loci and Highlights Biological Pathways and Regulatory Elements Involved in Cardiac Development. Am. J. Hum. Genet. 2018, 102, 103–115. [Google Scholar] [CrossRef]
- Ye, J.; Tucker, N.R.; Weng, L.C.; Clauss, S.; Lubitz, S.A.; Ellinor, P.T. A Functional Variant Associated with Atrial Fibrillation Regulates PITX2c Expression through TFAP2a. Am. J. Hum. Genet. 2016, 99, 1281–1291. [Google Scholar] [CrossRef]
- Cheng, C.; Liu, H.; Tan, C.; Tong, D.; Zhao, Y.; Liu, X.; Si, W.; Wang, L.; Liang, L.; Li, J.; et al. Mutation in NPPA causes atrial fibrillation by activating inflammation and cardiac fibrosis in a knock-in rat model. FASEB J. 2019, 33, 8878–8891. [Google Scholar] [CrossRef] [PubMed]
- Menon, A.; Hong, L.; Savio-Galimberti, E.; Sridhar, A.; Youn, S.W.; Zhang, M.; Kor, K.; Blair, M.; Kupershmidt, S.; Darbar, D. Electrophysiologic and molecular mechanisms of a frameshift NPPA mutation linked with familial atrial fibrillation. J. Mol. Cell. Cardiol. 2019, 132, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Goette, A.; Corradi, D.; Dobrev, D.; Aguinaga, L.; Cabrera, J.A.; Chugh, S.S.; de Groot, J.R.; Soulat-Dufour, L.; Fenelon, G.; Hatem, S.N.; et al. Atrial cardiomyopathy revisited-evolution of a concept: A clinical consensus statement of the European Heart Rhythm Association (EHRA) of the ESC, the Heart Rhythm Society (HRS), the Asian Pacific Heart Rhythm Society (APHRS), and the Latin American Heart Rhythm Society (LAHRS). Europace 2024, 26, euae204. [Google Scholar] [CrossRef]
- Forleo, C.; Carella, M.C.; Basile, P.; Carulli, E.; Dadamo, M.L.; Amati, F.; Loizzi, F.; Sorrentino, S.; Dentamaro, I.; Dicorato, M.M.; et al. Missense and Non-Missense Lamin A/C Gene Mutations Are Similarly Associated with Major Arrhythmic Cardiac Events: A 20-Year Single-Centre Experience. Biomedicines 2024, 12, 1293. [Google Scholar] [CrossRef] [PubMed]
- Tuluce, K.; Yakar Tuluce, S.; Yavuzgil, O.; Isayev, E.; Bilgin, M.; Akyildiz Akcay, F.; Nalbantgil, S.; Ozerkan, F. The left atrial phasic functions and the relationship with plasma N-terminal pro-B-type natriuretic peptide levels and symptomatic states in patients with hypertrophic cardiomyopathy. Anadolu Kardiyol. Derg. 2014, 14, 719–727. [Google Scholar] [CrossRef]
- Varnava, A.M.; Elliott, P.M.; Sharma, S.; McKenna, W.J.; Davies, M.J. Hypertrophic cardiomyopathy: The interrelation of disarray, fibrosis, and small vessel disease. Heart 2000, 84, 476–482. [Google Scholar] [CrossRef]
- Cameli, M.; Sciaccaluga, C.; Loiacono, F.; Simova, I.; Miglioranza, M.H.; Nistor, D.; Bandera, F.; Emdin, M.; Giannoni, A.; Ciccone, M.M.; et al. The analysis of left atrial function predicts the severity of functional impairment in chronic heart failure: The FLASH multicenter study. Int. J. Cardiol. 2019, 286, 87–91. [Google Scholar] [CrossRef]
- Yamaji, K.; Fujimoto, S.; Yutani, C.; Ikeda, Y.; Mizuno, R.; Hashimoto, T.; Nakamura, S. Does the progression of myocardial fibrosis lead to atrial fibrillation in patients with hypertrophic cardiomyopathy? Cardiovasc. Pathol. 2001, 10, 297–303. [Google Scholar] [CrossRef]
- Guglielmo, M.; Baggiano, A.; Muscogiuri, G.; Fusini, L.; Andreini, D.; Mushtaq, S.; Conte, E.; Annoni, A.; Formenti, A.; Mancini, E.M.; et al. Multimodality imaging of left atrium in patients with atrial fibrillation. J. Cardiovasc. Comput. Tomogr. 2019, 13, 340–346. [Google Scholar] [CrossRef]
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; D’Avila, A.; Dobrev, D.; et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: Definition, characterization, and clinical implication. Heart Rhythm 2017, 14, e3–e40. [Google Scholar] [CrossRef]
- Blume, G.G.; McLeod, C.J.; Barnes, M.E.; Seward, J.B.; Pellikka, P.A.; Bastiansen, P.M.; Tsang, T.S. Left atrial function: Physiology, assessment, and clinical implications. Eur. J. Echocardiogr. 2011, 12, 421–430. [Google Scholar] [CrossRef]
- Merlo, M.; Gagno, G.; Baritussio, A.; Bauce, B.; Biagini, E.; Canepa, M.; Cipriani, A.; Castelletti, S.; Dellegrottaglie, S.; Guaricci, A.I.; et al. Clinical application of CMR in cardiomyopathies: Evolving concepts and techniques: A position paper of myocardial and pericardial diseases and cardiac magnetic resonance working groups of Italian society of cardiology. Heart Fail. Rev. 2023, 28, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Authors/Task Force members; Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- Tsang, T.S.; Abhayaratna, W.P.; Barnes, M.E.; Miyasaka, Y.; Gersh, B.J.; Bailey, K.R.; Cha, S.S.; Seward, J.B. Prediction of cardiovascular outcomes with left atrial size: Is volume superior to area or diameter? J. Am. Coll. Cardiol. 2006, 47, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Tani, T.; Tanabe, K.; Ono, M.; Yamaguchi, K.; Okada, M.; Sumida, T.; Konda, T.; Fujii, Y.; Kawai, J.; Yagi, T.; et al. Left atrial volume and the risk of paroxysmal atrial fibrillation in patients with hypertrophic cardiomyopathy. J. Am. Soc. Echocardiogr. 2004, 17, 644–648. [Google Scholar] [CrossRef]
- Losi, M.A.; Betocchi, S.; Aversa, M.; Lombardi, R.; Miranda, M.; D’Alessandro, G.; Cacace, A.; Tocchetti, C.G.; Barbati, G.; Chiariello, M. Determinants of atrial fibrillation development in patients with hypertrophic cardiomyopathy. Am. J. Cardiol. 2004, 94, 895–900. [Google Scholar] [CrossRef]
- Suga, H. Importance of atrial compliance in cardiac performance. Circ. Res. 1974, 35, 39–43. [Google Scholar] [CrossRef]
- Abhayaratna, W.P.; Fatema, K.; Barnes, M.E.; Seward, J.B.; Gersh, B.J.; Bailey, K.R.; Casaclang-Verzosa, G.; Tsang, T.S. Left atrial reservoir function as a potent marker for first atrial fibrillation or flutter in persons > or = 65 years of age. Am. J. Cardiol. 2008, 101, 1626–1629. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Martini, C.; Gatti, M.; Dell’Aversana, S.; Ricci, F.; Guglielmo, M.; Baggiano, A.; Fusini, L.; Bracciani, A.; Scafuri, S.; et al. Feasibility of late gadolinium enhancement (LGE) in ischemic cardiomyopathy using 2D-multisegment LGE combined with artificial intelligence reconstruction deep learning noise reduction algorithm. Int. J. Cardiol. 2021, 343, 164–170. [Google Scholar] [CrossRef]
- Peretto, G.; Barison, A.; Forleo, C.; Di Resta, C.; Esposito, A.; Aquaro, G.D.; Scardapane, A.; Palmisano, A.; Emdin, M.; Resta, N.; et al. Late gadolinium enhancement role in arrhythmic risk stratification of patients with LMNA cardiomyopathy: Results from a long-term follow-up multicentre study. Europace 2020, 22, 1864–1872. [Google Scholar] [CrossRef] [PubMed]
- Ghanbari, F.; Joyce, T.; Lorenzoni, V.; Guaricci, A.I.; Pavon, A.G.; Fusini, L.; Andreini, D.; Rabbat, M.G.; Aquaro, G.D.; Abete, R.; et al. AI Cardiac MRI Scar Analysis Aids Prediction of Major Arrhythmic Events in the Multicenter DERIVATE Registry. Radiology 2023, 307, e222239. [Google Scholar] [CrossRef] [PubMed]
- Pontone, G.; Guaricci, A.I.; Fusini, L.; Baggiano, A.; Guglielmo, M.; Muscogiuri, G.; Volpe, A.; Abete, R.; Aquaro, G.; Barison, A.; et al. Cardiac Magnetic Resonance for Prophylactic Implantable-Cardioverter Defibrillator Therapy in Ischemic Cardiomyopathy: The DERIVATE-ICM International Registry. JACC Cardiovasc. Imaging 2023, 16, 1387–1400. [Google Scholar] [CrossRef]
- Mushtaq, S.; Chiesa, M.; Novelli, V.; Sommariva, E.; Biondi, M.L.; Manzoni, M.; Florio, A.; Lampus, M.L.; Avallone, C.; Zocchi, C.; et al. Role of advanced CMR features in identifying a positive genotype of hypertrophic cardiomyopathy. Int. J. Cardiol. 2024, 417, 132554. [Google Scholar] [CrossRef] [PubMed]
- Basile, P.; Soldato, N.; Pedio, E.; Siena, P.; Carella, M.C.; Dentamaro, I.; Khan, Y.; Baggiano, A.; Mushtaq, S.; Forleo, C.; et al. Cardiac magnetic resonance reveals concealed structural heart disease in patients with frequent premature ventricular contractions and normal echocardiography: A systematic review. Int. J. Cardiol. 2024, 412, 132306. [Google Scholar] [CrossRef]
- Hohneck, A.; Overhoff, D.; Doesch, C.; Sandberg, R.; Rudic, B.; Tueluemen, E.; Budjan, J.; Szabo, K.; Borggrefe, M.; Papavassiliu, T. Extent of Late Gadolinium Enhancement Predicts Thromboembolic Events in Patients With Hypertrophic Cardiomyopathy. Circ. J. 2020, 84, 754–762. [Google Scholar] [CrossRef]
- Hollowell, M.; Banno, J.; Marsy, D.; Shrestha, N.; Tan, J.; McNamara, R.; Decker, J.; Albano, A.; Franey, L.; Abdallah, W.; et al. Ventricular late gadolinium enhancement by cardiac MRI as a predictor of atrial fibrillation in hypertrophic cardiomyopathy. Int. J. Cardiol. 2024, 411, 132263. [Google Scholar] [CrossRef]
- Raman, B.; Smillie, R.W.; Mahmod, M.; Chan, K.; Ariga, R.; Nikolaidou, C.; Ormondroyd, E.; Thomson, K.; Harper, A.R.; Tan, G.; et al. Incremental value of left atrial booster and reservoir strain in predicting atrial fibrillation in patients with hypertrophic cardiomyopathy: A cardiovascular magnetic resonance study. J. Cardiovasc. Magn. Reson. 2021, 23, 109. [Google Scholar] [CrossRef]
- Parisi, F.; La Franca, E.; Giovanni, G.; Bellavia, D.; Pistelli, L.; Zito, C.; Carerj, S.; Cipriani, M. Novel Integrated Imaging Parameters for Risk Stratification of Atrial Fibrillation in Patients with Hypertrophic Cardiomyopathy. Eur. Heart J. Suppl. 2024, 26, ii12–ii13. [Google Scholar] [CrossRef]
- Wong, C.X.; Ganesan, A.N.; Selvanayagam, J.B. Epicardial fat and atrial fibrillation: Current evidence, potential mechanisms, clinical implications, and future directions. Eur. Heart J. 2017, 38, 1294–1302. [Google Scholar] [CrossRef]
- Zhou, Y.; Yu, M.; Cui, J.; Hu, F.; Yang, Z.; Yuan, J.; Qiao, S. The predictive value of epicardial adipose tissue volume assessed by cardiac magnetic resonance for atrial fibrillation in patients with hypertrophic obstructive cardiomyopathy. Int. J. Cardiovasc. Imaging 2021, 37, 1383–1393. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Yu, H.; Li, Y.; Deng, W.; Jia, Z.; Xue, Y.; Wang, Z.; Xu, H.; Yu, Y.; Zhao, R.; et al. The Association of Epicardial Adipose Tissue Volume and Atrial Fibrillation in Patients With Hypertrophic Cardiomyopathy: As Assessed by Cardiac MR. J. Magn. Reson. Imaging 2024, 61, 1299–1310. [Google Scholar] [CrossRef] [PubMed]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef]
- Francisco, A.; Pascoal, C.; Lamborne, P.; Morais, H.; Goncalves, M. Wearables and Atrial Fibrillation: Advances in Detection, Clinical Impact, Ethical Concerns, and Future Perspectives. Cureus 2025, 17, e77404. [Google Scholar] [CrossRef]
- Poh, M.Z.; Poh, Y.C.; Chan, P.H.; Wong, C.K.; Pun, L.; Leung, W.W.; Wong, Y.F.; Wong, M.M.; Chu, D.W.; Siu, C.W. Diagnostic assessment of a deep learning system for detecting atrial fibrillation in pulse waveforms. Heart 2018, 104, 1921–1928. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, J.; Jaakkola, S.; Lahdenoja, O.; Hurnanen, T.; Koivisto, T.; Pankaala, M.; Knuutila, T.; Kiviniemi, T.O.; Vasankari, T.; Airaksinen, K.E.J. Mobile Phone Detection of Atrial Fibrillation With Mechanocardiography: The MODE-AF Study (Mobile Phone Detection of Atrial Fibrillation). Circulation 2018, 137, 1524–1527. [Google Scholar] [CrossRef]
- Lown, M.; Yue, A.M.; Shah, B.N.; Corbett, S.J.; Lewith, G.; Stuart, B.; Garrard, J.; Brown, M.; Little, P.; Moore, M. Screening for Atrial Fibrillation Using Economical and Accurate Technology (From the SAFETY Study). Am. J. Cardiol. 2018, 122, 1339–1344. [Google Scholar] [CrossRef]
- Kao, Y.T.; Huang, C.Y.; Fang, Y.A.; Liu, J.C.; Chang, T.H. Machine Learning-Based Prediction of Atrial Fibrillation Risk Using Electronic Medical Records in Older Aged Patients. Am. J. Cardiol. 2023, 198, 56–63. [Google Scholar] [CrossRef]
- Lu, R.; Lumish, H.S.; Hasegawa, K.; Maurer, M.S.; Reilly, M.P.; Weiner, S.D.; Tower-Rader, A.; Fifer, M.A.; Shimada, Y.J. Prediction of new-onset atrial fibrillation in patients with hypertrophic cardiomyopathy using machine learning. Eur. J. Heart Fail. 2024, 83, 506. [Google Scholar] [CrossRef]
- Molnar, A.A.; Merkely, B. The Added Value of Atrial Strain Assessment in Clinical Practice. Diagnostics 2022, 12, 982. [Google Scholar] [CrossRef]
- O’Neill, L.; Harrison, J.; O’Neill, M.; Williams, S.E. Clinical, electrophysiological and imaging predictors of atrial fibrillation ablation outcome. Expert Rev. Cardiovasc. Ther. 2017, 15, 289–305. [Google Scholar] [CrossRef] [PubMed]
- Mariani, M.V.; Pierucci, N.; Piro, A.; Trivigno, S.; Chimenti, C.; Galardo, G.; Miraldi, F.; Vizza, C.D. Incidence and Determinants of Spontaneous Cardioversion of Early Onset Symptomatic Atrial Fibrillation. Medicina 2022, 58, 1513. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, J.J.; Arora, R.; Green, D.; Greenland, P.; Lee, D.C.; Lloyd-Jones, D.M.; Markl, M.; Ng, J.; Shah, S.J. Evaluating the Atrial Myopathy Underlying Atrial Fibrillation: Identifying the Arrhythmogenic and Thrombogenic Substrate. Circulation 2015, 132, 278–291. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Gene(s) Studied | Protein Encoded | Authors | Main Findings |
|---|---|---|---|
| MYH7 (Arg663His) | β- myosin heavy chain | Gruver et al. [36] | Significantly higher rate of AF onset compared to that of ungenotyped familial HCM population. |
| MYBPC3, MYH7, other genotypes | myosin binding protein C3, β- myosin heavy chain | Bongini et al. [42] | Three subgroups (MYBPC3, MYH7, and “other genotypes”), with similar LA size: genotype was not correlated to AF onset or severity. |
| CYP11B2 (344 T > C) | cytochrome P450 11B2 | Orenes-Piñero et al. [47] | Independently predicted the onset of AF and was associated with higher aldosterone serum levels. |
| COL1A1 (2046 G > T) | collagen type I alpha 1 chain | Orenes-Piñero et al. [47] | Not statistically significant trend towards a lower risk of AF onset (potential protective role). |
| AGTR1 (1166 A > G) | angiotensin II type 1 receptor | Belenkov et al. [48] | Associated with development of HCM with atrial fibrillation. |
| Study | Year | Sample Size | Type of Study | Technique | Significant Variable(s) | Cut-Off Value |
|---|---|---|---|---|---|---|
| Cecchi et al. [15] | 1997 | 110 | Retrospective and prospective | ECG | Filtered Pdur | >140 ms |
| Ozdemir et al. [16] | 2004 | 80 | Retrospective | ECG-Echo | P-wave dispersion Filtered Pdur LA diameter | >52.5 ms >134.5 ms >42 mm |
| Girasis et al. [17] | 2013 | 62 | Retrospective, case–control | ECG | LAD-AP LAT peak SR-S Pdur | >42 mm >2.32 s−1 >98.8 ms |
| Mandeş et al. [14] | 2022 | 126 | Prospective | ECG-Echo | P-wave dispersion LA booster pump strain | ≥47.5 ms ≥−0.88 s−1 |
| Tjahiadi et al. [22] | 2021 | 208 | Retrospective | ECG-Echo | PA-TDI LA diameter LAVI LA reservoir strain | >115 ms ≥45 mm ≥34 mL/m2 <21.3% |
| Maron et al. [25] | 2014 | 427 | Prospective | CMR | Age LAEF LAEDV | >40 years <38% ≥118 ml |
| Klopotowski et al. [26] | 2018 | 546 | Retrospective | Echo | Age Presyncope/syncope/nsVT LA diameter (initially) LA diameter at last follow-up LVEF | >44.5 years Yes >41.5 mm >45.5 mm <65.5% |
| Olivotto et al. [8] | 2001 | 480 | Prospective | Echo | LA diameter | > 45 mm |
| Tani et al. [66] | 2004 | 141 | Retrospective | Echo | LAVI | ≥34 mL/m2 |
| Losi et al. [67] | 2004 | 150 | Prospective | Echo | LA fractional shortening LA diameter LAVI | ≤16% ≥45 mm >27 mL/m2 |
| Tuluce et al. [56] | 2014 | 70 | Prospective | ECG-Echo-biomarkers | P-wave dispersion LATEF LAAEF NT-proBNP | >47.5 ms <49% <36% >720 pg/ml |
| Costabel et al. [10] | 2018 | 321 | Retrospective | Echo | E/e’ LA area | ≥17 ≥28 cm2 |
| Cochet et al. [28] | 2018 | 209 | Prospective | CMR | Fibrosis on RV-LV insertions NYHA class LA volume | |
| Hohneck et al. [76] | 2020 | 115 | Prospective | CMR | LV LGE | >14.4% |
| Hollowell et al. [77] | 2024 | 351 | Retrospective | CMR | LV LGE | >15% |
| Raman et al. [78] | 2021 | 258 | Retrospective | CMR | LA booster strain LA reservoir strain Age LAEF | ≤8% ≤18% ≥55 years ≤45% |
| Parisi et al. [79] | 2024 | 141 | Prospective | Echo-CMR | LACI LAEF | >44% <43% |
| Zhou et al. [81] | 2021 | 93 | Retrospective | CMR | EATVI LAVI LVEF | ≥143.8 mL/m2 ≥69.6 mL/m2 ≤64.2% |
| Li et al. [82] | 2024 | 304 | Retrospective | CMR | EATVI LV wall thickness LA diameter LAVI | ≥53.9 mL/m2 ≥21.7 mm ≥44 mm ≥53.0 mL/m2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dicorato, M.M.; Basile, P.; Naccarati, M.L.; Carella, M.C.; Dentamaro, I.; Falagario, A.; Cicco, S.; Forleo, C.; Guaricci, A.I.; Ciccone, M.M.; et al. Predicting New-Onset Atrial Fibrillation in Hypertrophic Cardiomyopathy: A Review. J. Clin. Med. 2025, 14, 2018. https://doi.org/10.3390/jcm14062018
Dicorato MM, Basile P, Naccarati ML, Carella MC, Dentamaro I, Falagario A, Cicco S, Forleo C, Guaricci AI, Ciccone MM, et al. Predicting New-Onset Atrial Fibrillation in Hypertrophic Cardiomyopathy: A Review. Journal of Clinical Medicine. 2025; 14(6):2018. https://doi.org/10.3390/jcm14062018
Chicago/Turabian StyleDicorato, Marco Maria, Paolo Basile, Maria Ludovica Naccarati, Maria Cristina Carella, Ilaria Dentamaro, Alessio Falagario, Sebastiano Cicco, Cinzia Forleo, Andrea Igoren Guaricci, Marco Matteo Ciccone, and et al. 2025. "Predicting New-Onset Atrial Fibrillation in Hypertrophic Cardiomyopathy: A Review" Journal of Clinical Medicine 14, no. 6: 2018. https://doi.org/10.3390/jcm14062018
APA StyleDicorato, M. M., Basile, P., Naccarati, M. L., Carella, M. C., Dentamaro, I., Falagario, A., Cicco, S., Forleo, C., Guaricci, A. I., Ciccone, M. M., & Santobuono, V. E. (2025). Predicting New-Onset Atrial Fibrillation in Hypertrophic Cardiomyopathy: A Review. Journal of Clinical Medicine, 14(6), 2018. https://doi.org/10.3390/jcm14062018