
Broad-Spectrum Adverse Events of Special Interests Based on Immune Response Following COVID-19 Vaccination: A Large-Scale Population-Based Cohort Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
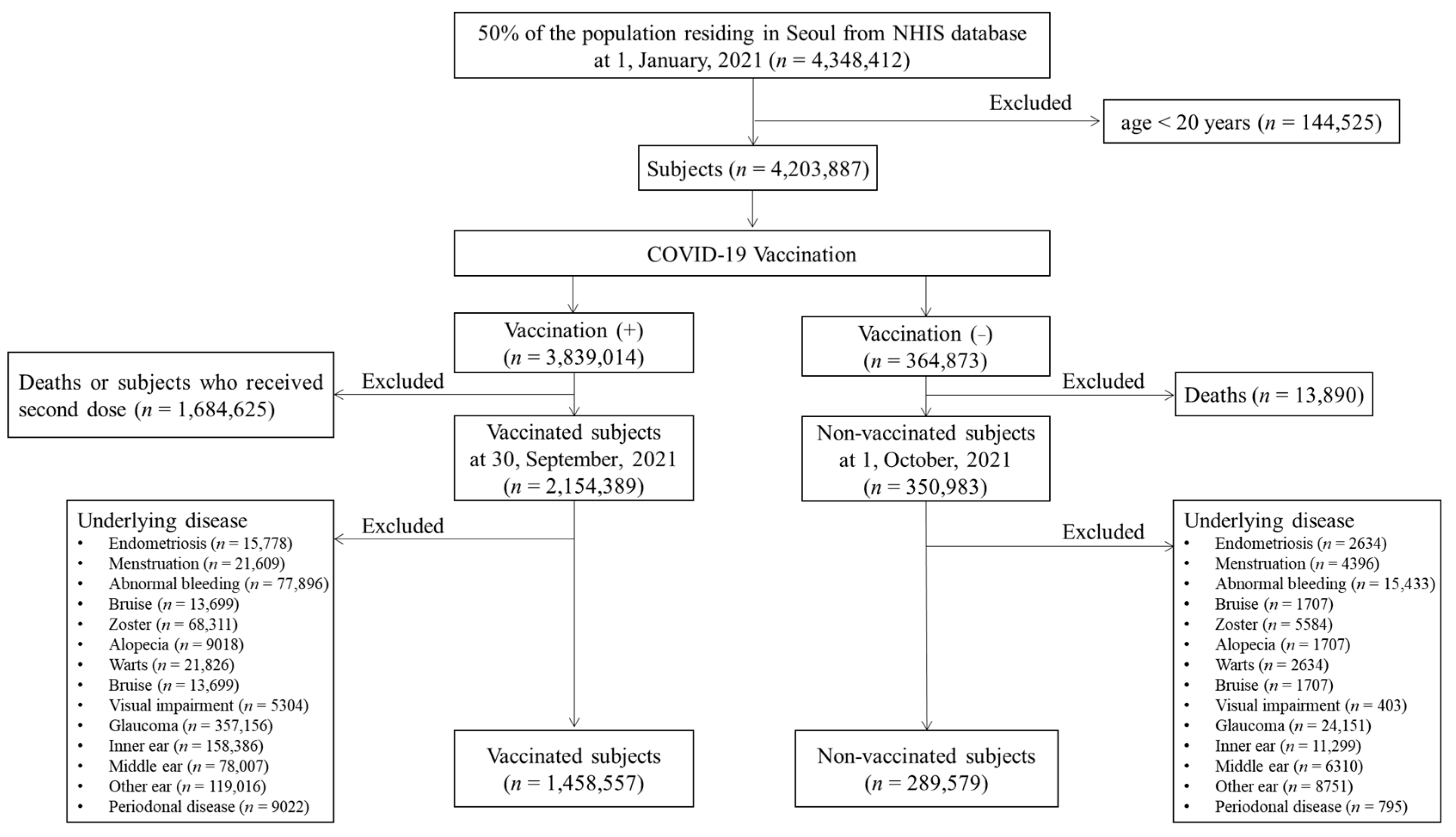
2.2. Study Population
2.3. Outcome Measurements
2.4. Statistical Analysis
3. Results
3.1. The Participants’ Characteristics
3.2. The cIRs per 10,000 of the Non-Serious AEs Following the COVID-19 Vaccination
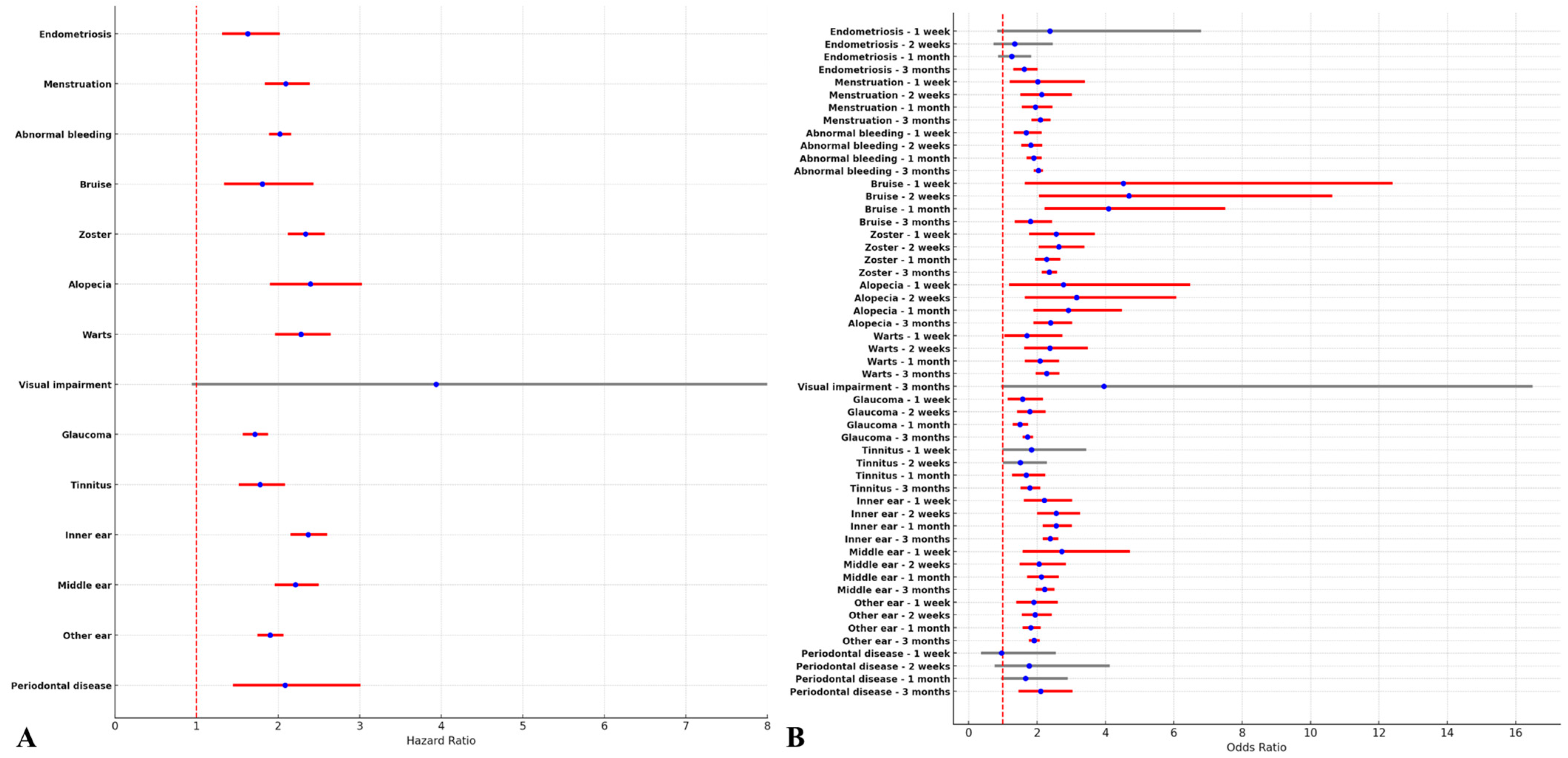
3.3. The Risks of Non-Serious AEs Following the COVID-19 Vaccination
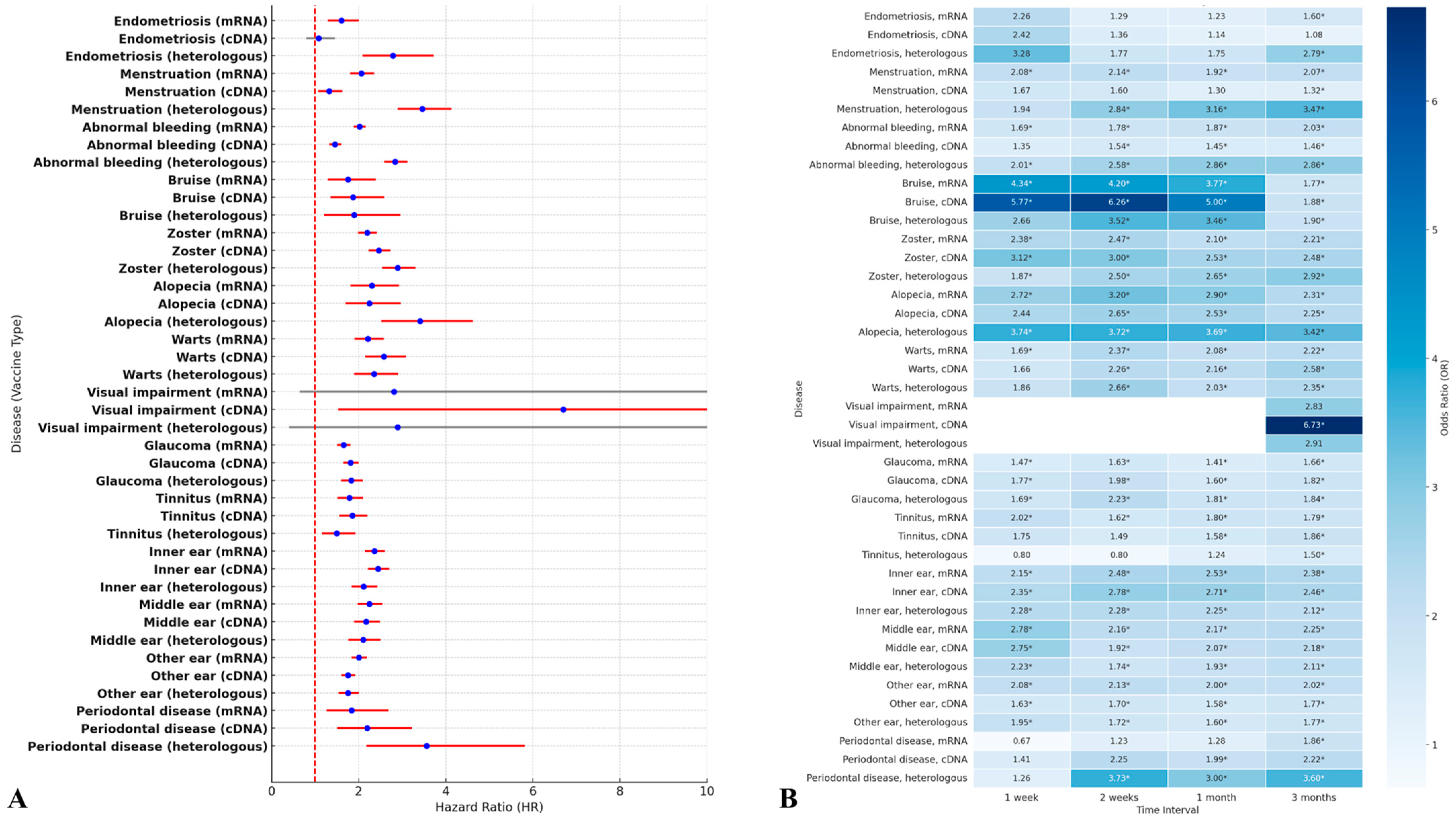
3.4. The Risks of the Broad-Spectrum AESIs According to the COVID-19 Vaccine Type
4. Discussion
4.1. Research Findings and Clinical Implications
4.2. The Type of Vaccination with the Association of Immune Response
4.3. The Role of Spike Protein in COVID-19 Vaccines
4.4. Gynecological AEs
4.5. Dermatological AEs
4.6. Strengths in This Study
4.7. Limitations in This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wang, C.Y.; Wang, S.I.; Wei, J.C. Long-term cardiovascular outcomes in COVID-19 survivors among non-vaccinated population: A retrospective cohort study from the TriNetX US collaborative networks. EClinicalMedicine 2022, 53, 101619. [Google Scholar] [CrossRef]
- Cho, J.Y.; Kim, K.H.; Lee, N.; Cho, S.H.; Kim, S.Y.; Kim, E.K.; Park, J.H.; Choi, E.Y.; Choi, J.O.; Park, H.; et al. COVID-19 vaccination-related myocarditis: A Korean nationwide study. Eur. Heart J. 2023, 44, 2234–2243. [Google Scholar] [CrossRef]
- Jung, J. Preparing for the Coronavirus Disease (COVID-19) Vaccination: Evidence, Plans, and Implications. J. Korean Med. Sci. 2021, 36, e59. [Google Scholar] [CrossRef]
- Lee, D.S.; Kim, J.W.; Lee, K.L.; Jung, Y.J.; Kang, H.W. Adverse events following COVID-19 vaccination in South Korea between February 28 and August 21, 2021: A nationwide observational study. Int. J. Infect. Dis. 2022, 118, 173–182. [Google Scholar] [CrossRef]
- Sharifian-Dorche, M.; Bahmanyar, M.; Sharifian-Dorche, A.; Mohammadi, P.; Nomovi, M.; Mowla, A. Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis post COVID-19 vaccination; a systematic review. J. Neurol. Sci. 2021, 428, 117607. [Google Scholar] [CrossRef] [PubMed]
- Ewer, K.J.; Barrett, J.R.; Belij-Rammerstorfer, S.; Sharpe, H.; Makinson, R.; Morter, R.; Flaxman, A.; Wright, D.; Bellamy, D.; Bittaye, M.; et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 2021, 27, 270–278. [Google Scholar] [CrossRef]
- Li, C.; Lee, A.; Grigoryan, L.; Arunachalam, P.S.; Scott, M.K.D.; Trisal, M.; Wimmers, F.; Sanyal, M.; Weidenbacher, P.A.; Feng, Y.; et al. Mechanisms of innate and adaptive immunity to the Pfizer-BioNTech BNT162b2 vaccine. Nat. Immunol. 2022, 23, 543–555. [Google Scholar] [CrossRef]
- Singh, R.B.; Parmar, U.P.S.; Kahale, F.; Agarwal, A.; Tsui, E. Vaccine-Associated Uveitis after COVID-19 Vaccination: Vaccine Adverse Event Reporting System Database Analysis. Ophthalmology 2023, 130, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Wichova, H.; Miller, M.E.; Derebery, M.J. Otologic Manifestations After COVID-19 Vaccination: The House Ear Clinic Experience. Otol. Neurotol. 2021, 42, e1213–e1218. [Google Scholar] [CrossRef]
- Fazlollahi, A.; Zahmatyar, M.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Shekarriz-Foumani, R.; Kolahi, A.A.; Singh, K.; Safiri, S. Cardiac complications following mRNA COVID-19 vaccines: A systematic review of case reports and case series. Rev. Med. Virol. 2022, 32, e2318. [Google Scholar] [CrossRef]
- Genco, L.; Cantelli, M.; Noto, M.; Battista, T.; Patrì, A.; Fabbrocini, G.; Vastarella, M. Alopecia Areata after COVID-19 Vaccines. Ski. Appendage Disord. 2023, 9, 141–143. [Google Scholar] [CrossRef]
- Cazzato, G.; Romita, P.; Foti, C.; Lobreglio, D.; Trilli, I.; Colagrande, A.; Ingravallo, G.; Resta, L. Development of Flat Warts on the Cheeks after BioNTech-Pfizer BNT162b2 Vaccine: Is There a Correlation? Vaccines 2022, 10, 532. [Google Scholar] [CrossRef] [PubMed]
- Toljan, K.; Amin, M.; Kunchok, A.; Ontaneda, D. New diagnosis of multiple sclerosis in the setting of mRNA COVID-19 vaccine exposure. J. Neuroimmunol. 2022, 362, 577785. [Google Scholar] [CrossRef]
- Gallo, G.; Mastorino, L.; Tonella, L.; Ribero, S.; Quaglino, P. Alopecia areata after COVID-19 vaccination. Clin. Exp. Vaccine Res. 2022, 11, 129–132. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Seyed Hosseini, E.; Riahi Kashani, N.; Nikzad, H.; Azadbakht, J.; Hassani Bafrani, H.; Haddad Kashani, H. The novel coronavirus Disease-2019 (COVID-19): Mechanism of action, detection and recent therapeutic strategies. Virology 2020, 551, 1–9. [Google Scholar] [CrossRef]
- Lee, H.K.; Go, J.; Sung, H.; Kim, S.W.; Walter, M.; Knabl, L.; Furth, P.A.; Hennighausen, L.; Huh, J.W. Heterologous ChAdOx1-BNT162b2 vaccination in Korean cohort induces robust immune and antibody responses that includes Omicron. iScience 2022, 25, 104473. [Google Scholar] [CrossRef] [PubMed]
- Yonker, L.M.; Swank, Z.; Bartsch, Y.C.; Burns, M.D.; Kane, A.; Boribong, B.P.; Davis, J.P.; Loiselle, M.; Novak, T.; Senussi, Y.; et al. Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis. Circulation 2023, 147, 867–876. [Google Scholar] [CrossRef]
- Ndeupen, S.; Qin, Z.; Jacobsen, S.; Bouteau, A.; Estanbouli, H.; Igyártó, B.Z. The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience 2021, 24, 103479. [Google Scholar] [CrossRef] [PubMed]
- Blix, K.; Laake, I.; Juvet, L.; Robertson, A.H.; Caspersen, I.H.; Mjaaland, S.; Skodvin, S.N.; Magnus, P.; Feiring, B.; Trogstad, L. Unexpected vaginal bleeding and COVID-19 vaccination in nonmenstruating women. Sci. Adv. 2023, 9, eadg1391. [Google Scholar] [CrossRef]
- Lee, K.M.N.; Junkins, E.J.; Luo, C.; Fatima, U.A.; Cox, M.L.; Clancy, K.B.H. Investigating trends in those who experience menstrual bleeding changes after SARS-CoV-2 vaccination. Sci. Adv. 2022, 8, eabm7201. [Google Scholar] [CrossRef]
- Ciorba, A.; Corazzi, V.; Bianchini, C.; Aimoni, C.; Pelucchi, S.; Skarżyński, P.H.; Hatzopoulos, S. Autoimmune inner ear disease (AIED): A diagnostic challenge. Int. J. Immunopathol. Pharmacol. 2018, 32, 2058738418808680. [Google Scholar] [CrossRef]
- Farland, L.V.; Khan, S.M.; Shilen, A.; Heslin, K.M.; Ishimwe, P.; Allen, A.M.; Herbst-Kralovetz, M.M.; Mahnert, N.D.; Pogreba-Brown, K.; Ernst, K.C.; et al. COVID-19 vaccination and changes in the menstrual cycle among vaccinated persons. Fertil. Steril. 2023, 119, 392–400. [Google Scholar] [CrossRef]
- Su, Y.W.; Yeh, S.J.; Chen, M.J. New-onset Glaucoma Following Moderna COVID-19 Vaccination. J. Curr. Glaucoma Pract. 2023, 17, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Mulroney, T.E.; Pöyry, T.; Yam-Puc, J.C.; Rust, M.; Harvey, R.F.; Kalmar, L.; Horner, E.; Booth, L.; Ferreira, A.P.; Stoneley, M.; et al. N(1)-methylpseudouridylation of mRNA causes +1 ribosomal frameshifting. Nature 2024, 625, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Rahimi Mansour, F.; Keyvanfar, A.; Najafiarab, H.; Rajaei Firouzabadi, S.; Sefidgar, S.; Hooshmand Chayijan, S.; Tarom, M.; Fadaei, M.; Farzaneh, F.; Karimzadeh Bardeei, L.; et al. Menstrual disturbances following COVID-19 vaccination: A probable puzzle about the role of endocrine and immune pathways. J. Reprod. Immunol. 2023, 158, 103952. [Google Scholar] [CrossRef] [PubMed]
- Mulroney, T.E.; Pöyry, T.; Yam-Puc, J.C.; Rust, M.; Harvey, R.F.; Kalmar, L.; Horner, E.; Booth, L.; Ferreira, A.P.; Stoneley, M. The Looming Effects of Estrogen in Covid-19: A Rocky Rollout. Front. Nutr. 2021, 18, 649128. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, M.H.; Park, S.J.; Choi, M.G.; Chun, E.M. Autoimmune adverse event following COVID-19 vaccination in Seoul, South Korea. J. Allergy Clin. Immunol. 2024, 156, 1711–1720. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Total (n = 1,748,133) | Vaccination | p | ||
|---|---|---|---|---|
| No (n = 289,576) | Yes (n= 1,458,557) | |||
| Gender, n (%) | 0.064 | |||
| Male | 861,301 (49.27%) | 143,128 (49.43%) | 718,173 (49.24%) | |
| Female | 886,832 (50.73%) | 146,448 (50.57%) | 740,384 (50.76%) | |
| Age, mean (SD), years | 53.32 (16.87) | 45.00 (16.89) | 54.97 (16.37) | <0.001 * |
| <0.001 | ||||
| 20–29 years, n (%) | 21,3267 (12.20%) | 54,748 (18.91%) | 158,519 (10.87%) | |
| 30–39 years, n (%) | 191,879 (10.98%) | 72,852 (25.16%) | 119,027 (8.16%) | |
| 40–49 years, n (%) | 231,285 (13.23%) | 63,163 (21.81%) | 168,122 (11.53%) | |
| 50–59 years, n (%) | 430,101 (24.60%) | 42,637 (14.72%) | 387,464 (26.56%) | |
| 60–69 years, n (%) | 398,344 (22.79%) | 28,757 (9.93%) | 369,587 (25.34%) | |
| 70–79 years, n (%) | 190,087 (10.87%) | 13,351 (4.61%) | 176,736 (12.12%) | |
| ≥80 years, n (%) | 93,170 (5.33%) | 14,068 (4.86%) | 79,102 (5.42%) | |
| Insurance level, n (%) | <0.001 | |||
| Low | 449,717 (25.73%) | 85,471 (29.52%) | 364,246 (24.97%) | |
| Moderate | 492,107 (28.15%) | 91,292 (31.53%) | 400,815 (27.48%) | |
| High | 806,309 (46.12%) | 112,813 (38.96%) | 693,496 (47.55%) | |
| CCI, n (%) | <0.001 | |||
| 0 | 1,226,052 (70.13%) | 249,643 (86.21%) | 976,409 (66.94%) | |
| 1 | 274,493 (15.70%) | 18,841 (6.51%) | 255,652 (17.53%) | |
| ≥2 | 247,588 (14.16%) | 21,092 (7.28%) | 226,496 (15.53%) | |
| Comorbidity, n (%) | ||||
| DM | 249,273 (14.26%) | 16,143 (5.57%) | 233,130 (15.98%) | <0.001 |
| Hyperlipidemia | 507,183 (29.01%) | 29,640 (10.24%) | 477,543 (32.74%) | <0.001 |
| HTN | 459,210 (26.27%) | 27,778 (9.59%) | 431,432 (29.58%) | <0.001 |
| COPD | 59,009 (3.38%) | 5414 (1.87%) | 53,595 (3.67%) | <0.001 |
| Prior COVID-19 infection, n (%) | 13,719 (0.78%) | 2970 (1.03%) | 10,749 (0.74%) | <0.001 |
| 1st vaccination product, n (%) | ||||
| AZD1222 | 609,023 (41.76%) | 609,023 (41.76%) | ||
| BNT162b2 | 826,953 (56.70%) | 826,953 (56.70%) | ||
| mRNA-1273 | 22,573 (1.55%) | 22,573 (1.55%) | ||
| JNJ-78436735 | 8 (0.00%) | 8 (0.00%) | ||
| 2nd vaccination product, n (%) | ||||
| AZD1222 | 510,261 (34.98%) | 510,261 (34.98%) | ||
| BNT162b2 | 925,692 (63.47%) | 925,692 (63.47%) | ||
| mRNA-1273 | 22,596 (1.55%) | 22,596 (1.55%) | ||
| JNJ-78436735 | 8 (0.00%) | 8 (0.00%) | ||
| 1st–2nd vaccination product, n (%) | ||||
| AZD1222–AZD1222 | 510,253 (34.98%) | 510,253 (34.98%) | ||
| AZD1222–BNT162b2 | 98,762 (6.77%) | 98,762 (6.77%) | ||
| AZD1222–mRNA-1273 | 2 (0.00%) | 2 (0.00%) | ||
| AZD1222–JNJ-78436735 | 6 (0.00%) | 6 (0.00%) | ||
| BNT162b2–AZD1222 | 3 (0.00%) | 3 (0.00%) | ||
| BNT162b2–BNT162b2 | 826,925 (56.69%) | 826,925 (56.69%) | ||
| BNT162b2–mRNA-1273 | 23 (0.00%) | 23 (0.00%) | ||
| BNT162b2–JNJ-78436735 | 2 (0.00%) | 2 (0.00%) | ||
| mRNA-1273–BNT162b2 | 2 (0.00%) | 2 (0.00%) | ||
| mRNA-1273–mRNA-1273 | 22,571 (1.55%) | 22,571 (1.55%) | ||
| JNJ-78436735–AZD1222 | 5 (0.00%) | 5 (0.00%) | ||
| JNJ-78436735–BNT162b2 | 3 (0.00%) | 3 (0.00%) | ||
| 1st–2nd vaccination type, n (%) | ||||
| No vaccination | 289,576 (16.56%) | 289,576 (100%) | ||
| Only mRNA vaccine | 849,526 (48.60%) | 849,526 (58.24%) | ||
| Only cDNA vaccine | 510,253 (29.19%) | 510,253 (34.98%) | ||
| Heterologous vaccination | 98,778 (5.65%) | 98,778 (6.77%) | ||
| Vaccination interval, mean (SD), days | 50.88 (23.19) | 50.88 (23.19) | ||
| Disease | V | One Week | Two Weeks | One Month | Three Months | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| E | IR | 95% CI | p | E | cIR | 95% CI | p | E | cIR | 95% CI | p | E | cIR | 95% CI | p | ||
| Endometriosis | No | 4 | 0.14 | 0.00–0.27 | 0.389 | 13 | 0.45 | 0.20–0.69 | 0.877 | 35 | 1.21 | 0.81–1.61 | 0.704 | 99 | 3.42 | 2.75–4.09 | 0.15 |
| Yes | 34 | 0.23 | 0.15–0.31 | 63 | 0.43 | 0.33–0.54 | 165 | 1.13 | 0.96–1.30 | 584 | 4 | 3.68–4.33 | |||||
| Menstrual disorder | No | 82 | 2.83 | 2.22–3.44 | 0.638 | 161 | 5.56 | 4.70–6.42 | 0.096 | 346 | 11.95 | 10.69–13.21 | 0.002 | 1025 | 35.4 | 33.23–37.56 | <0.001 |
| Yes | 442 | 3.03 | 2.75–3.31 | 935 | 6.41 | 6.00–6.82 | 2081 | 14.27 | 13.65–14.88 | 6481 | 44.43 | 43.35–45.51 | |||||
| Bruise | No | 4 | 0.14 | 0.00–0.27 | <0.001 | 6 | 0.21 | 0.04–0.37 | <0.001 | 11 | 0.38 | 0.16–0.60 | <0.001 | 48 | 1.66 | 1.19–2.13 | <0.001 |
| Yes | 107 | 0.73 | 0.59–0.87 | 181 | 1.24 | 1.06–1.42 | 287 | 1.97 | 1.74–2.20 | 559 | 3.83 | 3.51–4.15 | |||||
| Herpes zoster | No | 31 | 1.07 | 0.69–1.45 | <0.001 | 66 | 2.28 | 1.73–2.83 | <0.001 | 162 | 5.59 | 4.73–6.46 | <0.001 | 454 | 15.68 | 14.24–17.12 | <0.001 |
| Yes | 472 | 3.24 | 2.94–3.53 | 1055 | 7.23 | 6.80–7.67 | 2270 | 15.56 | 14.92–16.20 | 6575 | 45.08 | 43.99–46.17 | |||||
| Alopecia | No | 6 | 0.21 | 0.04–0.37 | 0.101 | 10 | 0.35 | 0.13–0.56 | 0.003 | 23 | 0.79 | 0.47–1.12 | <0.001 | 80 | 2.76 | 2.16–3.37 | <0.001 |
| Yes | 61 | 0.42 | 0.31–0.52 | 122 | 0.84 | 0.69–0.98 | 266 | 1.82 | 1.60–2.04 | 766 | 5.25 | 4.88–5.62 | |||||
| Warts | No | 20 | 0.69 | 0.39–0.99 | 0.279 | 30 | 1.04 | 0.67–1.41 | <0.001 | 78 | 2.69 | 2.10–3.29 | <0.001 | 197 | 6.8 | 5.85–7.75 | <0.001 |
| Yes | 135 | 0.93 | 0.77–1.08 | 303 | 2.08 | 1.84–2.31 | 658 | 4.51 | 4.17–4.86 | 1811 | 12.42 | 11.84–12.99 | |||||
| Visual impairment | No | 0 | 0 | 0.00–0.00 | 1.00 | 0 | 0 | 0.00–0.00 | 0.372 | 0 | 0 | 0.00–0.00 | 0.024 | 2 | 0.07 | 0.00–0.16 | 0.008 |
| Yes | 5 | 0.03 | 0.00–0.06 | 9 | 0.06 | 0.02–0.10 | 23 | 0.16 | 0.09–0.22 | 50 | 0.34 | 0.25–0.44 | |||||
| Glaucoma | No | 43 | 1.48 | 1.04–1.93 | <0.001 | 80 | 2.76 | 2.16–3.37 | <0.001 | 199 | 6.87 | 5.92–7.83 | <0.001 | 534 | 18.44 | 16.88–20.00 | <0.001 |
| Yes | 430 | 2.95 | 2.67–3.23 | 901 | 6.18 | 5.77–6.58 | 1892 | 12.97 | 12.39–13.56 | 5749 | 39.42 | 38.40–40.43 | |||||
| Tinnitus | No | 11 | 0.38 | 0.16–0.60 | 0.013 | 26 | 0.9 | 0.55–1.24 | 0.003 | 54 | 1.86 | 1.37–2.36 | <0.001 | 171 | 5.91 | 5.02–6.79 | <0.001 |
| Yes | 119 | 0.82 | 0.67–0.96 | 237 | 1.62 | 1.42–1.83 | 534 | 3.66 | 3.35–3.97 | 1789 | 12.27 | 11.70–12.83 | |||||
| Inner ear disease | No | 43 | 1.48 | 1.04–1.93 | <0.001 | 71 | 2.45 | 1.88–3.02 | <0.001 | 152 | 5.25 | 4.41–6.08 | <0.001 | 466 | 16.09 | 14.63–17.55 | <0.001 |
| Yes | 553 | 3.79 | 3.48–4.11 | 1094 | 7.5 | 7.06–7.94 | 2381 | 16.32 | 15.67–16.98 | 6870 | 47.1 | 45.99–48.21 | |||||
| Middle ear disease | No | 14 | 0.48 | 0.23–0.74 | <0.001 | 42 | 1.45 | 1.01–1.89 | <0.001 | 93 | 3.21 | 2.56–3.86 | <0.001 | 290 | 10.01 | 8.86–11.17 | <0.001 |
| Yes | 218 | 1.49 | 1.30–1.69 | 468 | 3.21 | 2.92–3.50 | 1058 | 7.25 | 6.82–7.69 | 3343 | 22.92 | 22.14–23.70 | |||||
| Other ear disease | No | 43 | 1.48 | 1.04–1.93 | <0.001 | 86 | 2.97 | 2.34–3.60 | <0.001 | 202 | 6.98 | 6.01–7.94 | <0.001 | 607 | 20.96 | 19.30–22.63 | <0.001 |
| Yes | 550 | 3.77 | 3.46–4.09 | 1112 | 7.62 | 7.18–8.07 | 2441 | 16.74 | 16.07–17.40 | 7552 | 51.78 | 50.61–52.94 | |||||
| Periodontal disease | No | 5 | 0.17 | 0.02–0.32 | 1.00 | 6 | 0.21 | 0.04–0.37 | 0.044 | 14 | 0.48 | 0.23–0.74 | 0.001 | 31 | 1.07 | 0.69–1.45 | <0.001 |
| Yes | 30 | 0.21 | 0.13–0.28 | 70 | 0.48 | 0.37–0.59 | 160 | 1.1 | 0.93–1.27 | 488 | 3.35 | 3.05–3.64 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Suh, J.H.; Kim, M.-H.; Choi, M.G.; Chun, E.M. Broad-Spectrum Adverse Events of Special Interests Based on Immune Response Following COVID-19 Vaccination: A Large-Scale Population-Based Cohort Study. J. Clin. Med. 2025, 14, 1767. https://doi.org/10.3390/jcm14051767
Kim HJ, Suh JH, Kim M-H, Choi MG, Chun EM. Broad-Spectrum Adverse Events of Special Interests Based on Immune Response Following COVID-19 Vaccination: A Large-Scale Population-Based Cohort Study. Journal of Clinical Medicine. 2025; 14(5):1767. https://doi.org/10.3390/jcm14051767
Chicago/Turabian StyleKim, Hong Jin, Jee Hyun Suh, Min-Ho Kim, Myeong Geun Choi, and Eun Mi Chun. 2025. "Broad-Spectrum Adverse Events of Special Interests Based on Immune Response Following COVID-19 Vaccination: A Large-Scale Population-Based Cohort Study" Journal of Clinical Medicine 14, no. 5: 1767. https://doi.org/10.3390/jcm14051767
APA StyleKim, H. J., Suh, J. H., Kim, M.-H., Choi, M. G., & Chun, E. M. (2025). Broad-Spectrum Adverse Events of Special Interests Based on Immune Response Following COVID-19 Vaccination: A Large-Scale Population-Based Cohort Study. Journal of Clinical Medicine, 14(5), 1767. https://doi.org/10.3390/jcm14051767