
Long-Term Clinical Relevance of Hyponatremia Identified During Acute Phase of Myocardial Infarction
 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
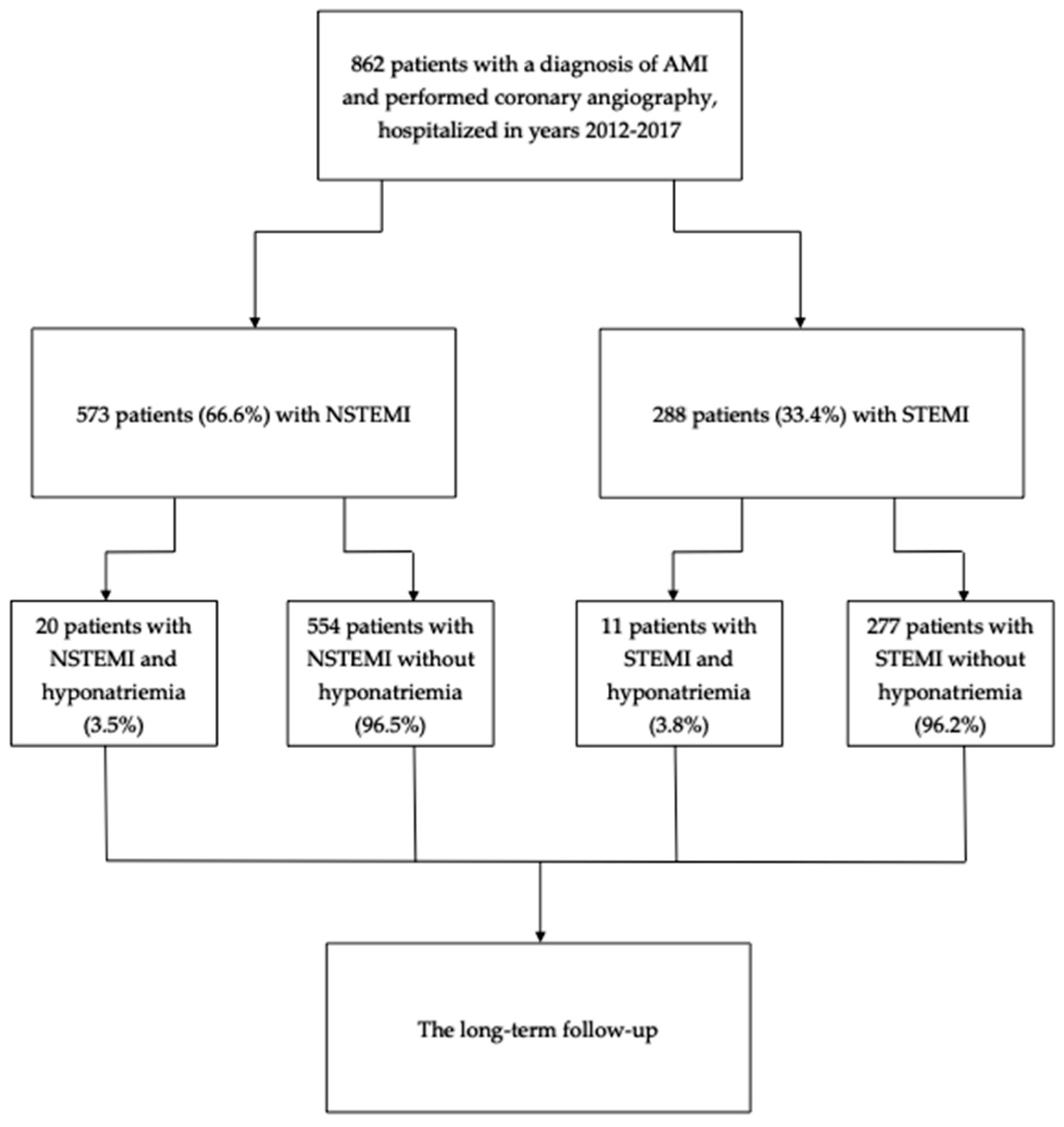
3. Results
3.1. Clinical Characteristics
3.2. Angiography and Revascularization Strategy
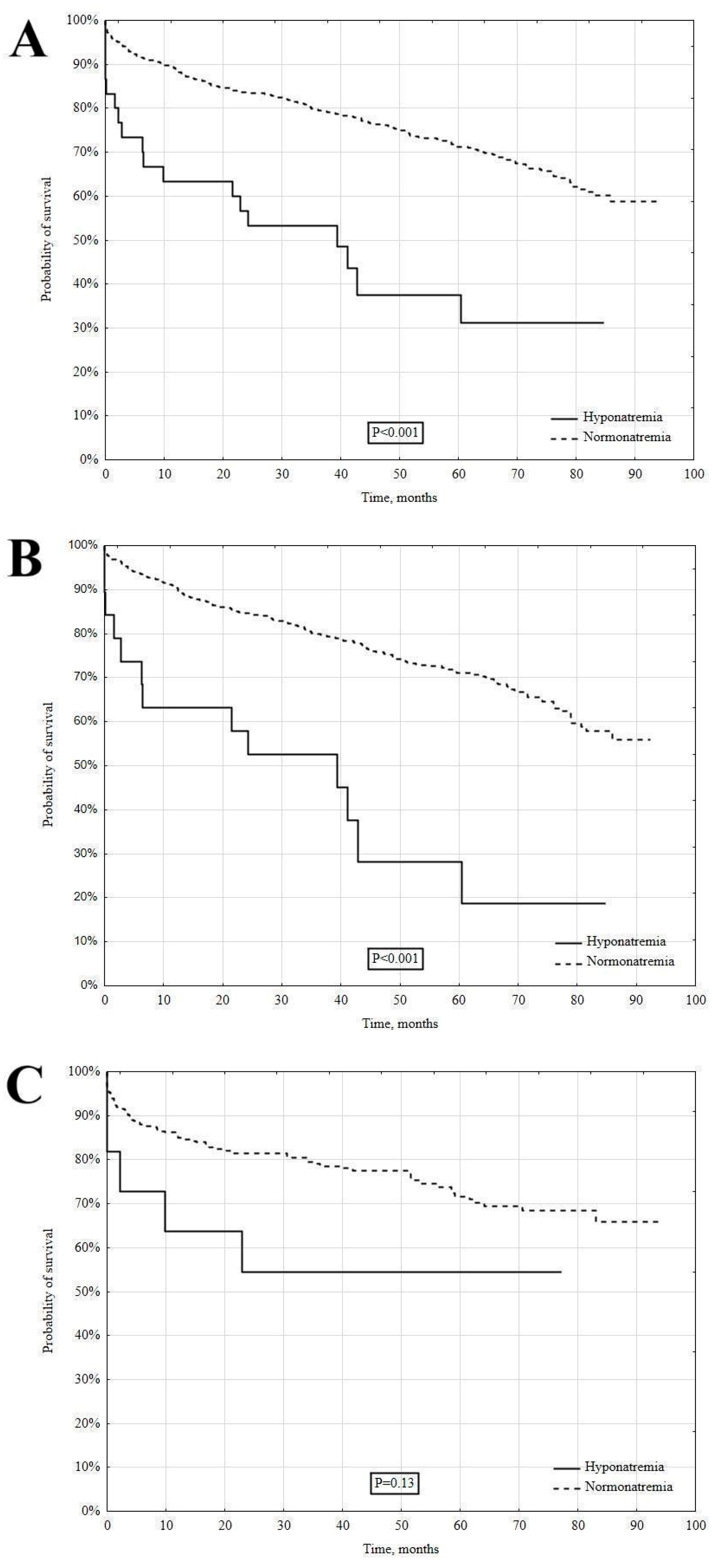
3.3. Long-Term Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tazmini, K.; Nymo, S.H.; Louch, W.E.; Ranhoff, A.H.; Øie, E. Electrolyte imbalances in an unselected population in an emergency department: A retrospective cohort study. PLoS ONE 2019, 14, e0215673. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, A.; Jaber, B.L.; Madias, N.E. Epidemiology of hyponatremia. Semin. Nephrol. 2009, 29, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Choi, D.J.; Yoon, C.H.; Oh, I.Y.; Jeon, E.S.; Kim, J.J.; Cho, M.C.; Chae, S.C.; Ryu, K.H.; Oh, B.H. Improvement of hyponatraemia during hospitalisation for acute heart failure is not associated with improvement of prognosis: An analysis from the Korean Heart Failure (KorHF) registry. Heart 2012, 98, 1798–1804. [Google Scholar] [CrossRef]
- Kapłon-Cieślicka, A.; Ozierański, K.; Balsam, P.; Tymińska, A.; Peller, M.; Galas, M.; Wyzgał, M.; Marchel, M.; Drożdż, J.; Opolski, G. Clinical characteristics and 1-year outcome of hyponatremic patients hospitalized for heart failure. Pol. Arch. Intern. Med. 2015, 125, 120–131. [Google Scholar] [CrossRef]
- Rywik, T.M.; Wiśniewska, A.; Cegłowska, U.; Drohomirecka, A.; Topór-Mądry, R.; Łazarczyk, H.; Połaska, P.; Zieliński, T.; Doryńska, A. Heart failure with reduced, mildly reduced, and preserved ejection fraction: Outcomes and predictors of prognosis. Pol. Arch. Intern. Med. 2023, 133, 16522. [Google Scholar] [CrossRef]
- Huang, W.Y.; Weng, W.C.; Peng, T.I.; Chien, Y.Y.; Wu, C.L.; Lee, M.; Hung, C.C.; Chen, K.H. Association of hyponatremia in acute stroke stage with three-year mortality in patients with first-ever ischemic stroke. Cerebrovasc. Dis. 2012, 34, 55–62. [Google Scholar] [CrossRef]
- Waikar, S.S.; Curhan, G.C.; Brunelli, S.M. Mortality associated with low serum sodium concentration in maintenance hemodialysis. Am. J. Med. 2011, 124, 77–84. [Google Scholar] [CrossRef]
- Funk, G.C.; Lindner, G.; Druml, W.; Metni, B.; Schwarz, C.; Bauer, P.; Metni, P.G. Incidence and prognosis of dysnatremias present on ICU admission. Intensive Care Med. 2010, 36, 304–311. [Google Scholar] [CrossRef]
- Ma, Q.Q.; Fan, X.D.; Li, T.; Hao, Y.Y.; Ma, F. Short- and long-term prognostic value of hyponatremia in patients with acute coronary syndrome: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0193857. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Commi ee on Clinical Practice Guidelines. Circulation 2022, 145, e4–e17. [Google Scholar] [CrossRef] [PubMed]
- Orzechowski, P.; Kowalik, I.; Piotrowicz, E. Feasibility of hybrid telerehabilitation as a component of the Managed Care after Acute Myocardial Infarction (MC-AMI) program in a 12-month follow-up: Experience from a single center. Pol. Arch. Intern. Med. 2023, 133, 16456. [Google Scholar] [CrossRef] [PubMed]
- Kaziród-Wolski, K.; Sielski, J.; Gąsior, M.; Bujak, K.; Hawranek, M.; Pyka, Ł.; Gierlotka, M.; Pawłowski, T.; Siudak, Z. Factors affecting short- and long-term survival of patients with acute coronary syndrome treated invasively using intravascular ultrasound and fractional flow reserve: Analysis of data from the Polish Registry of Acute Coronary Syndromes 2017–2020. Kardiol. Pol. 2023, 81, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Pruc, M.; Kubica, J.; Banach, M.; Swieczkowski, D.; Rafique, Z.; Peacock, W.F.; Siudak, Z.; Kurek, K.; Nanayakkara, P.; Szarpak, Ł. Diagnostic and prognostic performance of the neutrophil-to-lymphocyte ratio in acute coronary syndromes: A meta-analysis of 90 studies including 45,990 patients. Kardiol. Pol. 2024, 82, 276–284. [Google Scholar] [CrossRef]
- Kolarczyk-Haczyk, A.; Konopko, M.; Mazur, M.; Żurakowski, A.; Gąsior, M.; Rogala, M.; Jankowski, P.; Kaźmierczak, P.; Milewski, K.P.; Buszman, P.E.; et al. Long-term outcomes of the Coordinated Care Program in Patients after Myocardial Infarction (KOS-MI). Kardiol. Pol. 2023, 81, 587–596. [Google Scholar] [CrossRef]
- Cordova Sanchez, A.; Bhuta, K.; Shmorgon, G.; Angeloni, N.; Murphy, R.; Chaudhuri, D. The association of hyponatremia and clinical outcomes in patients with acute myocardial infarction: A cross-sectional study. BMC Cardiovasc. Disord. 2022, 22, 276. [Google Scholar] [CrossRef]
- Tada, Y.; Nakamura, T.; Funayama, H.; Sugawara, Y.; Ako, J.; Ishikawa, S.E.; Momomura, S. Early development of hyponatremia implicates short- and long-term outcomes in ST-elevation acute myocardial infarction. Circ. J. 2011, 75, 1927–1933. [Google Scholar] [CrossRef]
- Singla, I.; Zahid, M.; Good, C.B.; Macioce, A.; Sonel, A.F. Effect of hyponatremia (<135 mEq/L) on outcome in patients with non-ST-elevation acute coronary syndrome. Am. J. Cardiol. 2007, 100, 406–408. [Google Scholar] [CrossRef]
- Stępień, K.; Nowak, K.; Kachnic, N.; Karcińska, A.; Del Carmen Yika, A.; Furczyński, J.; Platschek, M.; Skorupa, M.; Wyleciał, Z.; Zalewski, J.; et al. Clinical characteristics and long-term outcomes of patients with heart failure with improved ejection fraction. First Polish experience from LECRA-HF registry. Adv. Med. Sci. 2024, 69, 132–138. [Google Scholar] [CrossRef]
- Stepien, K.; Nowak, K.; Szlosarczyk, B.; Nessler, J.; Zalewski, J. Clinical Characteristics and Long-Term Outcomes of MINOCA Accompanied by Active Cancer: A Retrospective Insight Into a Cardio-Oncology Center Registry. Front. Cardiovasc. Med. 2022, 9, 785246. [Google Scholar] [CrossRef]
- Krawczyk, K.; Stepien, K.; Nowak, K.; Nessler, J.; Zalewski, J. ST-segment re-elevation following primary angioplasty in acute myocardial infarction with patent infarct-related artery: Impact on left ventricular function recovery and remodeling. Adv. Interv. Cardiol. 2019, 15, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Gu, S.; Parikh, A.; Radhakrishnan, J. Prevalence of hyponatremia and association with mortality: Results from NHANES. Am. J. Med. 2013, 126, 1127–1137.e1. [Google Scholar] [CrossRef] [PubMed]
- Stachenfeld, N.S. Hormonal changes during menopause and the impact on fluid regulation. Reprod. Sci. 2014, 21, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; McDonough, A.A.; Layton, A.T. Sex differences in solute and water handling in the human kidney: Modeling and functional implications. iScience 2021, 24, 102667. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.S.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Ahn, Y.K.; Jeong, M.H.; Kim, S.W. Prognostic impact of hyponatremia occurring at various time points during hospitalization on mortality in patients with acute myocardial infarction. Medicine 2017, 96, e7023. [Google Scholar] [CrossRef]
- Goldberg, A.; Hammerman, H.; Petcherski, S.; Nassar, M.; Zdorovyak, A.; Yalonetsky, S.; Kapeliovich, M.; Agmon, Y.; Beyar, R.; Markiewicz, W.; et al. Hyponatremia and long-term mortality in survivors of acute ST-elevation myocardial infarction. Arch. Intern. Med. 2006, 166, 781–786. [Google Scholar] [CrossRef]
- Havránek, Š.; Bělohlávek, J.; Škulec, R.; Kovárník, T.; Dytrych, V.; Linhart, A. Long-term prognostic impact of hyponatremia in the ST-elevation myocardial infarction. Scand. J. Clin. Lab. Investig. 2011, 71, 38–44. [Google Scholar] [CrossRef]
- Burkhardt, K.; Kirchberger, I.; Heier, M.; Zirngibl, A.; Kling, E.; von Scheidt, W.; Kuch, B.; Meisinger, C. Hyponatraemia on admission to hospital is associated with increased long-term risk of mortality in survivors of myocardial infarction. Eur. J. Prev. Cardiol. 2015, 22, 1419–1426. [Google Scholar] [CrossRef]
- Palmer, B.R.; Pilbrow, A.P.; Frampton, C.M.; Yandle, T.G.; Skelton, L.; Nicholls, M.G.; Richards, A.M. Plasma aldosterone levels during hospitalization are predictive of survival post-myocardial infarction. Eur. Heart J. 2008, 29, 2489–2496. [Google Scholar] [CrossRef]
- Correale, M.; Tricarico, L.; Fortunato, M.; Mazzeo, P.; Nodari, S.; Di Biase, M.; Brune, N.D. New Targets in Heart Failure Drug Therapy. Front. Cardiovasc. Med. 2021, 8, 665797. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Mota, K.O.; Elimban, V.; Shah, A.K.; de Vasconcelos, C.M.L.; Bhullar, S.K. Role of Vasoactive Hormone-Induced Signal Transduction in Cardiac Hypertrophy and Heart Failure. Cells 2024, 13, 856. [Google Scholar] [CrossRef] [PubMed]
- Movafagh, S.; Cleemann, L.; Morad, M. Regulation of cardiac Ca2+ channel by extracellular Na+. Cell Calcium 2011, 49, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Oniki, T.; Teshima, Y.; Nishio, S.; Ishii, Y.; Kira, S.; Abe, I.; Yufu, K.; Takahashi, N. Hyponatraemia aggravates cardiac susceptibility to ischaemia/reperfusion injury. Int. J. Exp. Pathol. 2019, 100, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Kułach, A.; Wilkosz, K.; Wybraniec, M.; Wieczorek, P.; Gąsior, Z.; Mizia-Stec, K.; Wojakowski, W.; Zdrojewski, T.; Wojtyniak, B.; Gąsior, M.; et al. Managed Care after Acute Myocardial Infarction (MC-AMI)—Poland’s nationwide program of comprehensive post-MI care improves prognosis in 2-year follow-up. A single high-volume center intention-to-treat analysis. Kardiol. Pol. 2023, 81, 123–131. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Hyponatremia N = 31 | Non-Hyponatremia N = 831 | p-Value | |
|---|---|---|---|
| Male gender | 12 (38.7) | 585 (70.4) | <0.001 |
| Age, years | 74 (60–81) | 68 (60–78) | 0.10 |
| Body mass index, kg/m2 | 27.3 (23.5–31.1) | 27.6 (24.9–30.9) | 0.32 |
| Diabetes mellitus | 15 (50.0) | 309 (37.3) | 0.16 |
| Hypertension | 24 (80.0) | 731 (88.2) | 0.18 |
| Dyslipidemia | 24 (80.0) | 701 (84.6) | 0.50 |
| Impaired renal function | 10 (32.3) | 129 (15.5) | 0.013 |
| Active smoking | 5 (16.7) | 198 (23.9) | 0.36 |
| Chronic heart failure | 11 (36.7) | 276 (33.3) | 0.70 |
| Peripheral arterial disease | 4 (13.3) | 84 (10.1) | 0.57 |
| Prior stroke | 4 (13.3) | 53 (6.4) | 0.13 |
| Prior myocardial infarction | 11 (36.7) | 235 (28.4) | 0.32 |
| Prior revascularization | |||
| Percutaneous coronary intervention | 7 (23.3) | 150 (18.1) | 0.45 |
| Coronary artery bypass surgery | 0 (0.0) | 34 (4.1) | |
| Both percutaneous coronary intervention and coronary artery bypass surgery | 0 (0.0) | 27 (3.3) | |
| Killip class on admission: | |||
| I | 19 (63.3) | 665 (80.0) | 0.024 |
| II | 5 (16.7) | 101 (12.2) | |
| III | 1 (3.3) | 29 (3.5) | |
| IV | 5 (16.7) | 35 (4.2) | |
| Left ventricular ejection fraction | 45 (30–55) | 50 (40–55) | 0.14 |
| Clinical presentation | |||
| NSTEMI | 20 (64.5) | 554 (66.7) | 0.80 |
| STEMI | 11 (35.5) | 277 (33.3) | |
| Laboratory tests on admission | |||
| Troponin T, ng/mL | 0.426 (0.043–1.88) | 0.106 (0.029–0.382) | 0.003 |
| Creatine kinase, IU/L | 239 (159–711) | 177 (106–368) | 0.07 |
| Isoenzyme MB of creatine kinase, IU/L | 32 (22–92) | 21 (15–40) | 0.006 |
| Sodium, mEq/L | 132 (130–133) | 140 (138–142) | <0.001 |
| Potassium, mEq/L | 4.2 (3.8–4.8) | 4.1 (3.8–4.5) | 0.89 |
| Hemoglobin, g/dL | 12.9 (11.5–14.1) | 14.1 (12.9–15) | 0.001 |
| Hematocrit, % | 38 (34–42) | 42 (39–45) | <0.001 |
| White blood cells, ×103/µL | 10.7 (8.6–15) | 9.2 (7.4–11.7) | 0.014 |
| Platelet count, ×103/µL | 248 (179–286) | 221 (184–270) | 0.46 |
| Glucose, mmol/L | 9.9 (5.7–14.9) | 6.8 (5.8–8.9) | 0.012 |
| Creatinine, µmol/L | 112 (80–140) | 88 (76–103) | 0.007 |
| Glomerular filtration rate, mL/min | 47 (34–79) | 71 (58–86) | <0.001 |
| Total cholesterol, mmol/L | 4.1 (3.2–5.6) | 4.4 (3.6–5.3) | 0.31 |
| LDL cholesterol, mmol/L | 2.2 (1.6–3.2) | 2.6 (1.7–3.4) | 0.64 |
| HDL cholesterol, mmol/L | 1.1 (0.9–1.5) | 1.3 (1–1.7) | 0.23 |
| Triglycerides, mmol | 1.2 (0.8–2) | 1.3 (0.9–1.7) | 0.79 |
| Medications on discharge | |||
| Aspirin | 31 (100.0) | 831 (100.0) | 1.00 |
| P2Y12 inhibitor | 30 (96.8) | 828 (99.6) | 0.83 |
| ACE-I | 21 (72.4) | 669 (80.6) | 0.28 |
| Beta-adrenolytic | 27 (93.1) | 743 (89.5) | 0.53 |
| Statin | 27 (90.0) | 775 (93.4) | 0.47 |
| Loop diuretic | 9 (29.0) | 194 (23.3) | 0.67 |
| Hyponatremia N = 31 | Non-Hyponatremia N = 831 | p-Value | |
|---|---|---|---|
| Infarct-related artery: | |||
| Left main | 3 (9.7) | 31 (3.7) | 0.10 |
| Left anterior descending/diagonal branch | 10 (32.3) | 269 (34.4) | |
| Left circumflex/marginal branch | 4 (12.9) | 175 (21.1) | |
| Right coronary artery | 14 (45.2) | 279 (33.6) | |
| Undetermined | 0 (0.0) | 77 (9.3) | |
| Diagnosis of MINOCA | 0 (0.0) | 66 (7.9) | 0.10 |
| Treatment: | |||
| Primary percutaneous coronary intervention | 27 (87.1) | 674 (81.1) | 0.56 |
| Coronary artery bypass surgery | 0 (0.0) | 22 (2.7) | |
| Conservative | 4 (12.9) | 135 (16.3) |
| Independent Variable | Univariable Model | Multivariable Model | ||||
|---|---|---|---|---|---|---|
| Beta | 95% CI for Beta | p-Value | Beta | 95% CI for Beta | p-Value | |
| Sex, female vs. male | 0.094 | 0.028–0.160 | 0.006 | 0.061 | −0.014–0.124 | 0.117 |
| Hematocrit, per 1% | 0.181 | 0.116–0.248 | <0.001 | 0.138 | 0.070–0.206 | <0.001 |
| Creatinine, per 1 µmol/L | −0.129 | −0.204–−0.074 | <0.001 | −0.104 | −0.173–−0.035 | 0.002 |
| Isoenzyme MB of creatine kinase, per 1 IU/L | −0.147 | −0.208–−0.083 | <0.001 | −0.111 | −0.178–−0.044 | <0.001 |
| Glucose, per 1 mmol/L | −0.289 | −0.354–−0.223 | <0.001 | −0.248 | −0.314–−0.181 | <0.001 |
| Independent Variable | Univariable Model | Multivariable Model | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI for HR | p-Value | HR | 95% CI for HR | p-Value | |
| Age, per 1 year | 1.058 | 1.046–1.071 | <0.001 | 1.046 | 1.033–1.059 | <0.001 |
| Impaired renal function, no vs. yes | 2.616 | 2.006–3.412 | <0.001 | 1.307 | 0.974–1.752 | 0.074 |
| LVEF, per 1% | 0.948 | 0.939–0.957 | <0.001 | 0.967 | 0.956–0.977 | <0.001 |
| Killip class, per 1 class | 2.271 | 2.019–2.555 | <0.001 | 1.677 | 1.426–1.971 | <0.001 |
| Hyponatremia, no vs. yes | 2.734 | 1.693–4.415 | <0.001 | 2.222 | 1.309–3.773 | 0.003 |
| Hemoglobin, per 1 g/dL | 0.787 | 0.751–0.826 | <0.001 | 0.825 | 0.778–0.876 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eliasz, K.; Stępień, K.; Wojtylak, M.; Andrasz, O.; Majka, K.; Mazurek, G.; Horosin, G.; Plizga, J.; Nowak, K.; Krawczyk, K.; et al. Long-Term Clinical Relevance of Hyponatremia Identified During Acute Phase of Myocardial Infarction. J. Clin. Med. 2025, 14, 962. https://doi.org/10.3390/jcm14030962
Eliasz K, Stępień K, Wojtylak M, Andrasz O, Majka K, Mazurek G, Horosin G, Plizga J, Nowak K, Krawczyk K, et al. Long-Term Clinical Relevance of Hyponatremia Identified During Acute Phase of Myocardial Infarction. Journal of Clinical Medicine. 2025; 14(3):962. https://doi.org/10.3390/jcm14030962
Chicago/Turabian StyleEliasz, Karolina, Konrad Stępień, Maja Wojtylak, Oliwia Andrasz, Katarzyna Majka, Gabriela Mazurek, Grzegorz Horosin, Jakub Plizga, Karol Nowak, Krzysztof Krawczyk, and et al. 2025. "Long-Term Clinical Relevance of Hyponatremia Identified During Acute Phase of Myocardial Infarction" Journal of Clinical Medicine 14, no. 3: 962. https://doi.org/10.3390/jcm14030962
APA StyleEliasz, K., Stępień, K., Wojtylak, M., Andrasz, O., Majka, K., Mazurek, G., Horosin, G., Plizga, J., Nowak, K., Krawczyk, K., Podolec, M., Nessler, J., & Zalewski, J. (2025). Long-Term Clinical Relevance of Hyponatremia Identified During Acute Phase of Myocardial Infarction. Journal of Clinical Medicine, 14(3), 962. https://doi.org/10.3390/jcm14030962