
Stability Comparison of Implants with Alumina Sandblasting and Acid Etching Surface Treatment: A Retrospective Cohort Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Data Collection
2.2. Implant Placement: Surgical Protocol
2.3. Measurement of ITV
2.4. Measurement of Implant Stability Quotient
2.5. Implant Survival and Failure
2.6. Statistical Analyses
3. Results
3.1. Classification by ITV
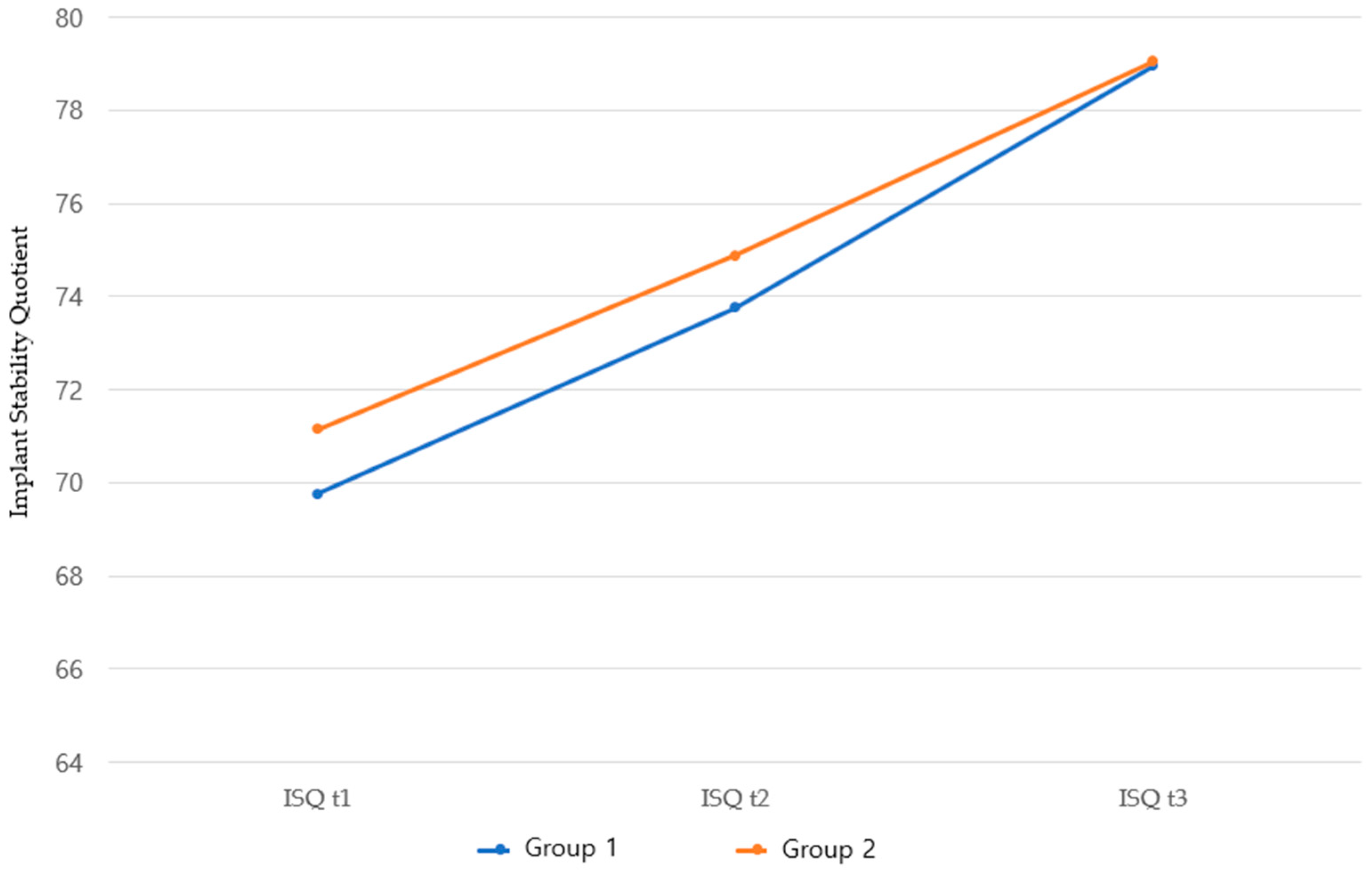
3.2. Comparison of Mean ISQ Between Group 1 and 2 Implants
3.3. Changes in ISQs According to Measurement Timing and Factors
3.4. Correlations Between ITV and ISQ
3.5. Implant Survival and Failure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Edelmayer, M.; Woletz, K.; Ulm, C.; Zechner, W.; Tepper, G. Patient information on treatment alternatives for missing single teeth—Systematic review. Eur. J. Oral Implantol. 2016, 9, 45–57. [Google Scholar] [CrossRef]
- Menini, M.; Bagnasco, F.; Calimodio, I.; Di Tullio, N.; Delucchi, F.; Baldi, D.; Pera, F. Influence of implant thread morphology on primary stability: A prospective clinical study. BioMed Res. Int. 2020, 2020, 697405. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.H.; Pyo, S.W.; Chang, J.S.; Kim, S.J. Up to a 15-year survival rate and marginal bone resorption of 1780 implants with or without microthreads: A multi center retrospective study. J. Clin. Med. 2023, 12, 2425. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lim, Y.J.; Kim, B.J.; Koo, K.T. Early loading of mandibular molar single implants: 1 year results of a randomized controlled clinical trial. Materials 2020, 13, 3912. [Google Scholar] [CrossRef]
- Lim, H.S.; Kim, S.G.; Oh, J.S. Comparison of clinical initial stability of hydroxy-apatite coated implant and sandblasted, large-grit and acid-etched implant. Maxillofac. Plast. Reconstr. Surg. 2012, 34, 112–116. [Google Scholar]
- Schupbach, P.; Glauser, R.; Bauer, S. Al2O3 particles on titanium dental implant systems following sandblasting and Acid-Etching process. Int. J. Biomater. 2019, 2019, 6318429. [Google Scholar] [CrossRef]
- Buser, D.; Nydegger, T.; Hirt, H.P.; Cochran, D.L.; Nolte, L.P. Removal torque values of titanium implants in the maxilla of miniature pigs. Int. J. Oral Maxillofac. Implant. 1998, 13, 611–619. [Google Scholar]
- Cochran, D.L.; Schenk, R.K.; Lussi, A.; Higginbottom, F.L.; Buser, D. Bone response to unloaded and loaded titanium implants with a sandblasted and acid-etched surface: A histometric study in the canine mandible. J. Biomed. Mater. Res. 1998, 40, 1–11. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J. Implant insertion torque: Its role in achieving primary stability of restorable dental implants. Compend. Contin. Educ. Dent. 2017, 38, 88–95. [Google Scholar]
- Berardini, M.; Trisi, P.; Sinjari, B.; Rutjes, A.W.; Caputi, S. The effects of high insertion torque versus low insertion torque on marginal bone resorption and implant failure rates: A systematic review with meta-analyses. Implant. Dent. 2016, 25, 532–540. [Google Scholar] [CrossRef]
- Bavetta, G.; Bavetta, G.; Randazzo, V.; Cavataio, A.; Paderni, C.; Grassia, V.; Dipalma, G.; Isacco, C.G.; Scarano, A.; Vito, D.D.; et al. A retrospective study on insertion torque and implant stability quotient (ISQ) as stability parameters for immediate loading of implants in fresh extraction sockets. BioMed Res. Int. 2019, 2019, 9720419. [Google Scholar] [CrossRef] [PubMed]
- Naseri, R.; Yaghini, J.; Feizi, A. Levels of smoking and dental implants failure: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Contemporary Implant Dentistry; Mosby Ltd.: St. Louis, MO, USA, 2008. [Google Scholar]
- Benic, G.I.; Mir-Mari, J.; Hämmerle, C.H.F. Loading protocols for single-implant crowns: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implant. 2014, 29, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Guirado, J.L.C.; Bettach, R.; Fabbro, M.D.; Martínez, C.P.-A.; Shibli, J.A. Evaluation of the insertion torque, implant stability quotient and drilled hole quality for different drill design. Clin. Oral Implant. Res. 2018, 29, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Lages, F.S.; Douglas-de Oliveira, D.W.; Costa, F.O. Relationship between implant stability measurements obtained by insertion torque and resonance frequency analysis: A systematic review. Clin. Implant. Dent. Relat. Res. 2018, 20, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wu, G.; Hunziker, E. The clinical significance of implant stability quotient (ISQ) measurements: A literature review. J. Oral Biol. Craniofacial Res. 2020, 10, 629–638. [Google Scholar]
- Peeraprasompong, W.; Aunmeungtong, W.; Khongkhunthian, P. Correlation between implant stability quotient and percussion sound frequency. Clin. Exp. Dent. Res. 2024, 10, 917. [Google Scholar] [CrossRef]
- Stoilov, M.; Shafaghi, R.; Stark, H.; Marder, M.; Kraus, D.; Enkling, N. Influence of implant macro-design, -length, and -diameter on primary implant stability depending on different bone qualities using standard drilling protocols—An in vitro analysis. J. Funct. Biomater. 2023, 14, 469. [Google Scholar] [CrossRef]
- Park, C.J.; Kim, D.G.; Cho, L.R. Initial changes of implant stability from installation during early bone healing. J. Dent. Rehabil. Appl. Sci. 2013, 29, 272–279. [Google Scholar] [CrossRef]
- Milillo, L.; Fiandaca, C.; Giannoulis, F.; Ottria, L.; Lucchese, A.; Silvestre, F.; Petruzzi, M. Immediate vs non-immediate loading post-extractive implants: A comparative study of implant stability quotient (ISQ). Oral Implantol. 2016, 13, 123–131. [Google Scholar]
- Satpathy, S.; Varalakshmi, U.; Tenglikar, P.; Chowdary, K.R.R.; Khader, A.A.; Parihar, A.S.; Yashavanth Kumar, D.S.; Samanta, A. Evaluation of implant stability quotient of sandblasted acid-etched (SAE) and chemical-modified SAE dental implants: A clinical study. J. Pharm. Bioallied Sci. 2024, 16, 2075–2077. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.M.; Malcangi, G.; Ferrante, L.; Del Vecchio, G.; Viapiano, F.; Inchingolo, A.D.; Mancini, A.; Annicchiarico, C.; Inchingolo, F.; Dipalma, G.; et al. Surface coatings of dental implants: A review. J. Funct. Biomater. 2023, 14, 287. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Yun, P.Y.; Chang, N.H.; Kim, Y.K. The long-term evaluation of the prognosis of implants with acid-etched surfaces sandblasted with alumina: A retrospective clinical study. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 10. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Group 1 (Osstem Implant) | Group 2 (Toplan Implant) |
|---|---|---|
| Manufacturer | Osstem Implant Co., Ltd. | Toplan Co., Ltd. |
| Model name | Osstem TS III | Toplan T01 |
| Body shape | Conical, 1.5° taper | Conical, Taper–-straight–-taper |
| Thread shape | Triangular thread | Triangular thread |
| Pitch height (mm) | 0.8 (double) | 0.9 (double) |
| Thread height (mm) | 0.45 | 0.4 |
| Implant–abutment interface | Internal hexagon | Internal hexagon |
| Inclination angle of the thread flank (°) | 40 | 30 |
| Surface treatment | SA | SA |
| Microthreads | None | None |
| Figure of the implant |  |  |
| Classification of ITVs | Group 1 (n = 57) | Group 2 (n = 87) |
|---|---|---|
| <30 N/cm | 3 (5.26) | 3 (3.45) |
| 30–40 N/cm | 38 (66.67) | 65 (74.71) |
| 40–50 N/cm | 14 (24.56) | 15 (17.24) |
| >50 N/cm | 2 (3.51) | 4 (4.60) |
| Groups | ISQ t1 | ISQ t2 | ISQ t3 | p-Value † |
|---|---|---|---|---|
| Group 1 (n = 57) | 69.76 ± 12.30 | 73.74 ± 10.10 | 78.94 ± 9.12 | <0.001 |
| Group 2 (n = 87) | 71.13 ± 7.86 | 74.88 ± 7.35 | 79.03 ± 5.64 | <0.001 |
| p-value ‡ | 0.416 | 0.462 | 0.944 |
| n | Group 1 | p-Value † | n | Group 2 | p-Value † | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ISQ t1 | ISQ t2 | ISQ t3 | ISQ t1 | ISQ t2 | ISQ t3 | ||||||
| Sex | Man | 33 | 71.00 a (64.25, 5.00) | 76.00 b (69.00, 0.50) | 82.00 c (77.75, 5.50) | <0.001 | 71 | 72.50 a (69.00, 6.50) | 74.50 b (70.00, 0.50) | 78.00 c (75.00, 2.50) | <0.001 |
| Woman | 24 | 72.50 a (65.50, 79.38) | 73.25 b (67.50, 2.00) | 76.50 b (71.63, 5.63) | 0.002 | 16 | 72.50 a (63.63, 9.50) | 75.50 b (71.25, 0.00) | 80.75 c (76.75, 5.00) | <0.001 | |
| p-value ‡ | 0.437 | 0.903 | 0.132 | 0.641 | 0.507 | 0.167 | |||||
| Bone type | D2 | 30 | 73.50 a (70.38, 80.13) | 78.50 b (71.50, 83.38) | 82.00 c (77.88, 86.00) | <0.001 | 42 | 74.25 a (68.75, 9.50) | 77.00 b (71.38, 80.50) | 80.00 c (77.50, 2.13) | <0.001 |
| D3 | 27 | 67.00 a (56.50, 74.00) | 69.00 a (66.00, 78.00) | 77.50 b (71.00, 85.00) | <0.001 | 45 | 72.00 a (66.25, 5.00) | 72.50 b (70.00, 80.00) | 77.00 c (74.25, 5.75) | <0.001 | |
| p-value ‡ | 0.001 | 0.001 | 0.095 | 0.159 | 0.156 | 0.465 | |||||
| Implant location | Maxilla | 24 | 64.75 a (56.13, 74.00) | 69.00 a (65.25, 75.75) | 76.50 b (71.00, 84.13) | <0.001 | 45 | 72.00 a (68.00, 5.00) | 74.00 b (70.25, 80.00) | 78.00 c (74.75, 5.75) | <0.001 |
| Mandible | 33 | 73.00 a (70.00, 79.75) | 78.50 b (71.50, 82.75) | 82.00 c (78.75, 86.00) | <0.001 | 42 | 74.25 a (67.00, 9.50) | 75.50 b (70.75, 80.50) | 79.75 c (75.38, 81.63) | <0.001 | |
| p-value ‡ | 0.001 | <0.001 | 0.027 | 0.219 | 0.743 | 0.643 | |||||
| Implant placement timing | Immediately implanted | 27 | 71.00 a (67.00, 75.00) | 76.00 b (66.50, 81.00) | 80.00 c (73.50, 82.50) | <0.001 | 47 | 72.50 a (68.50, 6.50) | 74.50 b (71.00, 0.00) | 79.00 c (75.00, 82.00) | <0.001 |
| Delayed placement | 30 | 71.00 a (63.13, 79.00) | 73.50 b (68.88, 80.63) | 82.50 c (77.50, 86.25) | <0.001 | 40 | 72.00 a (65.63, 6.50) | 75.00 b (70.00, 2.38) | 80.25 c (75.00, 84.75) | <0.001 | |
| p-value ‡ | 0.725 | 0.949 | 0.088 | 0.871 | 0.821 | 0.855 | |||||
| Implant diameter | ≤4.0 mm | 3 | 71.00 a (60.00, 73.00) | 76.00 a (43.00, 78.50) | 77.00 a (42.50, 80.00) | 0.717 | 27 | 70.00 a (62.00, 4.00) | 74.00 b (69.50, 0.50) | 79.50 c (75.00, 85.50) | <0.001 |
| >4.0 mm | 54 | 71.00 a (64.88, 77.50) | 74.50 b (68.88, 81.00) | 81.25 c (74.00, 86.00) | <0.001 | 60 | 74.50 a (69.13, 7.25) | 75.00 b (71.13, 0.00) | 78.75 c (75.00, 82.38) | <0.001 | |
| p-value ‡ | 0.579 | 0.532 | 0.138 | 0.021 | 0.666 | 0.797 | |||||
| Implant length | ≤10 mm | 17 | 70.00 a (63.75, 77.50) | 72.00 b (69.00, 80.50) | 81.00 b (73.75, 85.50) | <0.001 | 32 | 72.00 a (64.25, 75.00) | 72.50 b (70.00, 79.13) | 77.75 c (75.00, 81.38) | <0.001 |
| >10 mm | 40 | 71.25 a (65.38, 77.38) | 76.00 b (68.50, 80.88) | 80.50 c (74.00, 85.75) | <0.001 | 55 | 72.50 a (68.50, 77.50) | 75.50 b (71.00, 80.50) | 79.50 c (75.00, 85.00) | <0.001 | |
| p-value ‡ | 0.663 | 0.972 | 0.727 | 0.197 | 0.137 | 0.420 | |||||
| ITV | ISQ t1 | ISQ t2 | ISQ t3 | |
|---|---|---|---|---|
| ITV | 1 | |||
| ISQ t1 | 0.349 ** | 1 | ||
| ISQ t2 | 0.204 | 0.666 *** | 1 | |
| ISQ t3 | −0.190 | 0.202 | 0.340 ** | 1 |
| ITV | ISQ t1 | ISQ t2 | ISQ t3 | |
|---|---|---|---|---|
| ITV | 1 | |||
| ISQ t1 | 0.026 | 1 | ||
| ISQ t2 | −0.011 | 0.557 *** | 1 | |
| ISQ t3 | 0.075 | 0.359 *** | 0.781 *** | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Back, S.-I.; Chung, M.-J.; Jeong, H.-G.; Min, J.-H. Stability Comparison of Implants with Alumina Sandblasting and Acid Etching Surface Treatment: A Retrospective Cohort Study. J. Clin. Med. 2025, 14, 740. https://doi.org/10.3390/jcm14030740
Back S-I, Chung M-J, Jeong H-G, Min J-H. Stability Comparison of Implants with Alumina Sandblasting and Acid Etching Surface Treatment: A Retrospective Cohort Study. Journal of Clinical Medicine. 2025; 14(3):740. https://doi.org/10.3390/jcm14030740
Chicago/Turabian StyleBack, Song-I, Myung-Jin Chung, Ho-Gul Jeong, and Ji-Hyun Min. 2025. "Stability Comparison of Implants with Alumina Sandblasting and Acid Etching Surface Treatment: A Retrospective Cohort Study" Journal of Clinical Medicine 14, no. 3: 740. https://doi.org/10.3390/jcm14030740
APA StyleBack, S.-I., Chung, M.-J., Jeong, H.-G., & Min, J.-H. (2025). Stability Comparison of Implants with Alumina Sandblasting and Acid Etching Surface Treatment: A Retrospective Cohort Study. Journal of Clinical Medicine, 14(3), 740. https://doi.org/10.3390/jcm14030740