Abstract
Background/Objectives: Chronic subdural hematoma (CSDH) predominantly affects the elderly population. To optimize care and quality in this demographic, tailored, age-specific counseling and therapeutic decision-making are imperative. Accordingly, this study aimed to identify risk factors for in-hospital mortality and functional outcome at discharge following surgery using an age-stratified approach. Methods: We conducted a retrospective analysis of symptomatic CSDH patients who underwent surgery at our institution between June 2012 and December 2023. Subjects were categorized into three age cohorts: younger adults (18–64 years), older adults (65–79 years), and the oldest old (≥80 years). Clinical and neurological statuses at admission and discharge were evaluated using the Glasgow Coma Scale (GCS) and modified Rankin Scale (mRS), with mRS scores > 3 indicating poor functional outcomes. Results: Among 879 CSDH patients (mean age 75 ± 11.9 years), the sex ratio shifted progressively from a male predominance in younger adults (1:3.2) to a more balanced ratio in the oldest old (1:1.7). In the multivariate analysis, poor admission mRS and GCS score ≤ 7 predicted in-hospital mortality for older adults, while atrial fibrillation and postoperative pneumonia were significant in the oldest old. Poor admission mRS and multimorbidity consistently forecast unfavorable outcomes alongside other predictors, such as preoperative altered state of consciousness, epilepsy, dementia, unilateral CSDH, postoperative seizure, bleeding, and pneumonia varying by age cohort. Recurrence-free intervals were significantly extended with increasing age. Conclusions: This large-scale, age-stratified analysis delineates critical predictors of in-hospital mortality and unfavorable functional outcomes in surgically treated CSDH patients. These findings offer valuable guidance for neurosurgeons in preoperative risk assessment and inform age-specific counseling strategies to better communicate prognosis and tailor treatment plans.
1. Introduction
Chronic subdural hematoma (CSDH) is one of the most common neurosurgical conditions, with a markedly increased incidence in aging populations due to demographic shifts and greater longevity worldwide [1,2]. Epidemiological data indicate an annual incidence of approximately 58.1 per 100,000 in individuals over 65 years of age, compared to only 3.4 per 100,000 in those under 65 [2,3]. The disease typically arises from minor head traumas, leading to bridging vein rupture, followed by progressive hematoma expansion driven by fragile neo-membrane vasculature and inflammatory cascades [4,5]. While CSDH is traditionally associated with elderly patients, often presenting with neurological deficits such as limb weakness, gait disturbance, or cognitive impairment, it can also occur in younger adults, in whom symptoms more frequently reflect raised intracranial pressure, including headache and vomiting [6,7,8,9,10].
The clinical presentation, comorbidity profile, and prognosis of CSDH vary substantially with age. Younger patients often have identifiable predisposing factors, such as arachnoid cysts, ventriculoperitoneal shunts, or coagulation disorders, whereas elderly patients more commonly exhibit multimorbidity, brain atrophy, and antithrombotic therapy use [2,4,11,12,13]. Comparative studies have shown that while recurrence rates after surgery are not consistently higher in older cohorts, postoperative complication rates and in-hospital mortality increase with advancing age [2,8]. Moreover, functional outcomes tend to be more favorable in younger patients [2,14,15]. This underscores the importance of incorporating age-stratified risk assessment into both prognostication and perioperative management.
Given these age-dependent variations in presentation, comorbidity burden, and postoperative trajectories, a more granular, age-stratified evaluation of CSDH patients is warranted to optimize prognostication, guide perioperative management, and inform shared decision-making. Although several studies have compared surgical outcomes between younger and older adults, most have employed a dichotomous age classification or utilized broad age groups, potentially obscuring clinically relevant differences within the elderly population [2,4,8,10,16,17]. By adopting a three-tier age stratification, our study aims to delineate both common and age-specific predictors of in-hospital mortality and functional outcome at discharge in a large, contemporary surgical CSDH cohort. This approach allows for the identification of distinct risk profiles across the adult lifespan, thereby enabling more tailored perioperative strategies and evidence-based counseling for patients and their families.
2. Methods and Materials
2.1. Study Population
Between June 2012 and December 2023, 938 consecutive patients aged ≥18 years with symptomatic CSDH admitted at our institution were evaluated for the eligibility for this study. Patients with a history of brain surgery (intracranial tumor, acute subdural hematoma, aneurysm clipping, and CSDH), ventriculoperitoneal shunt, as well as patients with concomitant acute lesions (intracranial hemorrhage, traumatic brain injury) were excluded. The study flowchart shows the selection process and the main exclusion criteria in detail (Figure 1).
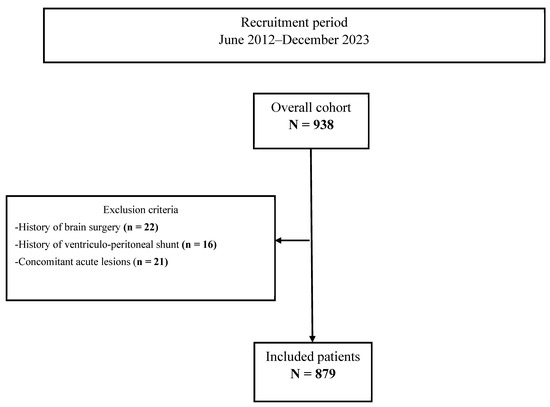
Figure 1.
Study flowchart.
This retrospective study was performed in accordance with the ethical standards of the institutional research committee and the Code of Ethics of the World Medical Association (Declaration of Helsinki). The Institutional Review Board approved the study protocol (Medical Faculty, University of Duisburg-Essen, Registration number: 22-10763-BO). All supporting data are available within this article. Anonymized data will be shared upon reasonable request from any qualified investigator.
2.2. Definition of Age-Related Groups in CSDH Patients
In accordance with contemporary clinical research practices and epidemiological literature, and consistent with German and international standards in gerontology and public health [18,19,20,21], patients were stratified into three age groups: younger adults (18–64 years), older adults (65–79 years), and the oldest old (≥80 years).
2.3. Patient Data Collection
The patients’ medical records were retrospectively assessed to examine the following data points: age, sex, Charlson comorbidity Index (CCI), American Society of Anesthesiologists Physical Status Classification System (ASA status), traumatic event, as well as comorbidities such as epilepsy, dementia, arterial hypertension, diabetes mellitus, chronic kidney disease (CKD), atrial fibrillation (AF), chronic heart disease (CHD), cerebral vascular accident or transient ischemic accident (CVA/TIA), prior antiplatelet and/or anticoagulation therapy (AAT)–including acetylsalicylic acid (aspirin), clopidogrel, vitamin K antagonists (VKA), direct oral anticoagulants (DOAC), heparin, dual or triple AAT–seizure 24 h prior to admission, neurological condition, and functional status on admission using the GCS score and the modified Rankin Scale (mRS), respectively. Furthermore, the variable “altered state of consciousness” was assessed and defined as changes in awareness or perception that deviate qualitatively from a person’s usual, alert, and oriented condition. Radiographic variables, such as midline shift (MLS), hematoma thickness, presence of septations, and hematoma density, were assessed from the preoperative CT-scans. Along with the patients’ period of hospitalization, operative technique (one burr hole vs. minicraniotomy–unilateral CSDH–vs. two burr holes vs. minicraniotomy and one burr hole–bilateral CSDH), neurological condition on discharge, in-hospital mortality, and postoperative complications, such as postoperative bleeding requiring reoperation, postoperative seizure, recurrence, myocardial infarction (MI), pulmonary embolism (PE), and postoperative stroke were assessed. Recurrence was defined as an episode of radiological hematoma progression, with or without development of symptoms, that required reoperation. Functional status of the patients was also documented at discharge. Patients with a postoperative mRS score ≤ 3 were able to walk without assistance and although moderately disabled could be discharged home. Patients with an mRS score equal to 4 or 5 were transferred to rehabilitation. Therefore, an mRS score > 3 was considered to have a poor outcome. Prior to statistical analysis, the data were thoroughly reviewed and validated by the senior author (M.C.).
2.4. Routine Clinical Care and Treatment Protocol of CSDH
In all patients, hematoma evacuation was performed under general anesthesia using either a burr hole or a minicraniotomy with placement of a subdural drain whenever possible. Prior to surgery, a single dose of antibiotics was administrated prophylactically. Postoperatively, patients spent 48 h in the intermediate or intensive care unit and remained on bed rest. On the second postoperative day, a CT-scan was performed and the subdural drain was removed. Patients were usually discharged around day 7 after surgery.
2.5. Perioperative Management of AAT
AAT was discontinued prior to surgery (aspirin and clopidogrel 5–7 days, DOAC 48 h, and VKA until the Quick value exceeded 70%, i.e., INR < 1.3). AAT was reinitiated three weeks after surgery if the hematoma had completely resolved. In cases of neurological deterioration during the discontinuation period, Desmopressin or PPSB was administered to reverse the effects of aspirin and VKA, respectively, in order to normalize coagulation status and enable a safe emergency operation. Patients in whom AAT could not be discontinued (n = 18) either underwent surgery while continuing AAT (n = 13) or had at least one of the two antithrombotic drugs temporarily stopped. Patients, for whom AAT discontinuation was advised to be as brief as possible (n = 9), were operated on after a temporary cessation of AAT and were subsequently bridged with heparin during the first postoperative week until oral anticoagulation could be safely resumed.
2.6. Assessment of Radiographic Variables
Radiographic parameters were assessed from preoperative axial CT-scans. Hematoma thickness was measured as the maximum perpendicular thickness from the inner skull table to the inner margin of the hematoma. In case of bilateral hematomas, the sum of both maximum thicknesses was considered to represent total hematoma burden. MLS was measured at the foramen of Monro as the perpendicular distance from the ideal midline–connecting the most anterior and posterior visible points of the falx cerebri–to the septum pellucidum. The density of the hematoma was divided in hypodense, isodense, hyperdense, or mixed density. Septations within the hematoma were also assessed.
2.7. Statistical Analyses
All analyses were performed using SPSS version 29.0.2.0 (IBM, Chicago, IL, USA). Categorical data are presented as frequencies and percentages. Normally distributed continuous variables are expressed as the mean and standard deviation (SD). Non-normally distributed continuous variables are expressed as the median and interquartile range (IQR). The Mann–Whitney U test was used to assess statistical associations between the study endpoints (in-hospital mortality, functional outcome at discharge) and other continuous variables. Associations between study endpoints and other dichotomous variables were determined using the Chi-square test and Fisher’s exact test (when the expected cell frequency was <5). The factors in the univariate analysis, which were associated with the study endpoints with a p-value < 0.1, were implemented in the multivariate analysis. Binomial logistic regression (forward likelihood ratio method) was used to determine the predictors of the study endpoints, and the adjusted odds ratio (aOR) and 95% confidence intervals (95% CI) were calculated. Prediction models based on the results of the multivariate analysis were computed. p-values < 0.05 in two-sided testing were considered statistically significant. Receiver operating characteristic (ROC) curve analyses were conducted to determine the accuracy of the prediction models. Events per variable (EPV) between five and nine were considered to yield acceptable bias and coverage under well-behaved conditions [22]. For EPV lower than five, internal validation and bias correction of the logistic regression models was conducted by bootstrapping with 1000 resamples. Bias-corrected and accelerated (BCa) 95% CI were computed for all regression coefficients. Subsequently, using R software (version 4.5.1, R Foundation for Statistical Computing, Vienna, Austria), ROC curve analysis was conducted to evaluate the discriminatory ability of the model. Optimism-corrected AUC values and its 95% CIs were calculated using bootstrap resampling (1000 replicates) to internally validate the predictive performance.
2.8. Use of GenAI in Writing and Editing
AI-assisted copy-editing using Perplexity AI (GPT-4 architecture) was utilized to improve the readability, grammar, and style of the manuscript. This process involved refining human-generated text without altering the scientific content. All final text revisions were reviewed and approved by the authors to ensure accuracy and integrity.
3. Results
3.1. Baseline Characteristics
Accordingly, 879 patients (mean age: 75 ± 11.9 years, female:male = 1:2.1, CCI: 4 (3), ASA status: 3 (0)) met the inclusion criteria. There were no statistically significant differences in the operative technique (p = 0.929) and CSDH location (p = 0.827) between the three age-related groups. However, statistically significant differences were observed in sex ratio (p = 0.001), CCI (p < 0.001), ASA status (p < 0.001), recent head trauma, several comorbidities (p < 0.001), as well as prior AAT use (p < 0.001), preoperative symptoms and neurological deficits (p < 0.05), postoperative pneumonia (p = 0.023), total hospital stay (p = 0.008), mRS at admission and discharge (p = 0.0005), and in-hospital mortality (p = 0.02). The sex ratio evolved from a strong predominance of males (female:male 1:3.2), gradually shifting to a less pronounced male predominance (1:2.4), and approaching a more balanced distribution (1:1.7). CCI and ASA status were highest in the oldest old. Comorbidities, such as dementia, arterial hypertension, diabetes mellitus, CKD, AF, CHD, and CVA/TIA, increased in frequency with age. In contrast, preoperative symptoms, such as nausea, headache, and seizure within 24 h prior to admission, were inversely related to age. Neurological deficits—including aphasia, dysarthria, hemiparesis—altered state of consciousness, cognitive decline, gait disturbances at admission, as well as functional statuses at admission and discharge, and in-hospital mortality, were all positively associated with advancing age. Preoperative CT-based severity criteria, such as hematoma thickness, midline shift greater than 10 mm, and hematoma density (especially mixed density), were significantly more frequent with increasing age (p < 0.001, p = 0.002, and p = 0.005, respectively). Postoperative pneumonia was also more frequent in the oldest old. Total length of hospital stay increased proportionally with age. Table 1 shows in detail all these findings.

Table 1.
Relevant differences in baseline characteristics between age groups.
3.2. Characteristics and Predictors of In-Hospital Mortality
In-hospital mortality was 3.6% in the general cohort and substantially increased from 1.4% in younger adults, to 2.9% in older adults, reaching up to 5.2% in the oldest old (p = 0.020). In the univariate analysis, in-hospital mortality among younger adults was significantly associated with age (p = 0.031) and CCI (p = 0.002). Postoperative bleeding requiring reoperation (p = 0.080) demonstrated a non-significant trend. Multivariate analysis identified no independent predictors of in-hospital mortality in this cohort (Table 2A).
Table 2.
(A): Predictors of in-hospital mortality in different age groups. (B): Predictors of in-hospital mortality in different age groups.
In the older adult group, univariate analysis revealed significant associations between in-hospital mortality and CCI (p = 0.017), operative technique (p = 0.005), mRS at admission (p = 0.016), preoperative altered state of consciousness (p = 0.048), preoperative GCS score ≤ 7 (p = 0.009), and third recurrence (p = 0.029). ASA status (p = 0.078), preoperative hemiplegia (p = 0.084), and postoperative bleeding requiring reoperation (p = 0.059) exhibited non-significant trends. In the multivariate model, mRS at admission (p = 0.041) and preoperative GCS score ≤ 7 (p = 0.040) were identified as independent predictors of in-hospital mortality, with an EPV of 5 (Table 2). The model’s discrimination ability, was indicated by an AUC of 0.83 (95% CI 0.66–0.99) in the ROC curve analysis (Figure 2A).
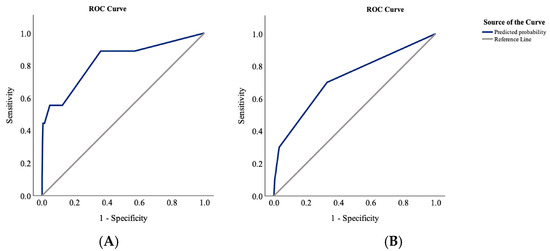
Figure 2.
ROC curve analyses of in-hospital mortality showing an AUC of 0.83 (95% CI 0.66–0.99) in older adults (A) and an AUC of 0.72 (95% CI 0.59–0.85) in the oldest old (B).
Among the oldest old patients, in-hospital mortality was significantly associated with ASA status (p = 0.043), epilepsy (p = 0.037), postoperative bleeding requiring reoperation (p < 0.001), and second recurrence (p = 0.014). Non-significant trends were observed for diabetes mellitus (p = 0.070), AF (p = 0.081), prior AAT use (p = 0.057), preoperative aphasia (p = 0.092), postoperative pneumonia (p = 0.054), and third recurrence (p = 0.052). In multivariate analysis, AF (p = 0.031) and postoperative pneumonia (p < 0.001) emerged as independent predictors of in-hospital mortality in this group, with an EPV of 10 (Table 2). The model’s discriminative capacity was determined by an ROC curve analysis and was, according to Hosmer et al. [23], acceptable with an AUC of 0.72 (95% CI 0.59–0.85) (Figure 2B).
3.3. Characteristics and Predictors of Functional Outcome at Discharge
Unfavorable functional outcome at discharge consistently increased from 14.3% in younger adults, to 28.2% in older adults, reaching up to 53.8% in the oldest old (p = 0.0005).
In the younger adult cohort, univariate analysis demonstrated that poorer functional outcomes at discharge were significantly associated with several factors: age (p = 0.038), sex (p = 0.049), ASA status (p < 0.001), admission mRS score (p < 0.001), presence of preoperative headache (p = 0.001), altered state of consciousness (p < 0.001), aphasia (p = 0.008), hemiparesis (p = 0.030), and postoperative seizures (p = 0.010). Variables such as CCI (p = 0.075), epilepsy (p = 0.052), behavioral changes prior to admission (p = 0.071), and preoperative neurological deficits (p = 0.058) approached but did not reach statistical significance. In multivariate analysis, significant independent predictors of poor functional outcome at discharge included female sex (p = 0.040), elevated ASA status (p = 0.010), epilepsy (p = 0.029), poor mRS at admission (p < 0.001), and postoperative seizure (p = 0.005) (Table 3A,B). Due to low EPV logistic regression model (EPV = 4.2), an internal validation was conducted using bootstrapping. This analysis showed that only elevated ASA status (p = 0.002, Bca 95% CI: 1.1–414.7), poor mRS at admission (p = 0.001, Bca 95% CI: 4–971.5), and postoperative seizure (p = 0.002, Bca 95% CI: 0.5–614.1) were independent predictors of poor functional outcome at discharge (Table 4). The predictive performance of the multivariate model was assessed using an ROC curve analysis in R software and showed an optimism-corrected AUC of 0.89 (95% CI: 0.76–0.95) (Figure 3A).
Table 3.
(A): Predictors of poor functional outcome at discharge. (B): Predictors of poor functional outcome at discharge.
Table 4.
Bootstrapped logistic regression for prediction of functional outcome at discharge in younger adults.
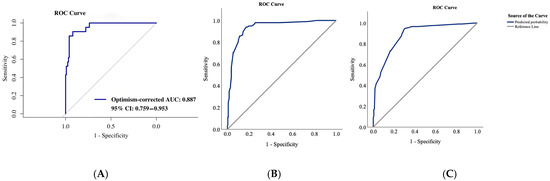
Figure 3.
ROC curve analyses of functional outcome at discharge showing an optimism-corrected AUC of 0.89 (95% CI: 0.76–0.95) in younger adults (A), an AUC of 0.94 (95% CI: 0.91–0.96) in the older adults (B), and an AUC of 0.88 (95% CI: 0.85–0.92) in the oldest old (C).
In older adults, univariate analysis found functional outcome at discharge to be significantly impacted by age (p = 0.012), CCI (p < 0.001), ASA status (p < 0.001), epilepsy (p = 0.009), dementia (p < 0.001), diabetes mellitus (p = 0.001), CKD (p = 0.01), AF (p = 0.038), CVA/TIA (p = 0.009), CSDH location (p = 0.043), year of surgery (p = 0.045), prior AAT use (p = 0.031), perioperative AAT stop and heparin bridging (p = 0.024), and mRS at admission (p < 0.001). Other associated variables included preoperative headache (p < 0.001), change in behavior (p = 0.049), cognitive deterioration (p < 0.001), seizure 24 h prior to admission (p = 0.035), neurological deficits (p = 0.005), altered state of consciousness (p < 0.001), preoperative GCS score ≤ 7 (p < 0.001), hemiparesis (p = 0.008), hemiplegia (p = 0.022), mixed hematoma density on CT-scan (p = 0.018), postoperative seizures (p < 0.001), postoperative bleeding requiring reoperation (p = 0.026), and postoperative pneumonia (p < 0.001). Trends toward significance were noted with dizziness (p = 0.091) and dysarthria (p = 0.073) (Table 3A). Multivariate analysis identified several independent predictors of poor discharge outcomes: high CCI (p = 0.036), dementia (p = 0.016), unilateral CSDH (p = 0.016), poor mRS at admission (p < 0.001), and postoperative pneumonia (p = 0.013), with an EPV of 19.6 (Table 3B). The model’s discriminative accuracy, evaluated via ROC analysis, was outstanding according to Hosmer et al. [23]. with an AUC of 0.94 (95% CI: 0.91–0.96) (Figure 3B).
For the oldest old subgroup, univariate associations revealed that impaired functional outcomes at discharge were significantly related to age (p = 0.004), CCI (p < 0.001), ASA status (p < 0.001), recent head trauma (p = 0.038), epilepsy (p = 0.015), dementia (p < 0.001), diabetes mellitus (p = 0.029), poor mRS at admission (p < 0.001), and presenting preoperative symptoms such as headache (p = 0.034), dizziness (p = 0.018), cognitive deterioration (p = 0.003), and altered state of consciousness (p < 0.001). Additional relevant factors included preoperative aphasia (p = 0.002), postoperative seizure (p = 0.006), postoperative bleeding requiring reoperation (p = 0.019), and postoperative pneumonia (p < 0.001). Arterial hypertension (p = 0.081), CKD (p = 0.054), year of surgery (p = 0.089), prior AAT use (p = 0.070), change in behavior (p = 0.089), preoperative GCS score ≤ 7 (p = 0.064), hematoma thickness (p = 0.057), and mixed hematoma density on CT-scan (p = 0.053) showed non-significant trends (Table 3A). Multivariate analysis identified several independent predictors of poor outcome at discharge: elevated ASA status (p = 0.014), epilepsy (p = 0.023), dementia (p = 0.003), poor mRS at admission (p < 0.001), altered state of consciousness (p = 0.035), and postoperative bleeding requiring reoperation (p = 0.007), with an EPV of 34.5 (Table 3B). The model’s discriminative strength, as assessed via ROC curve, was excellent according to Hosmer et al. [23]. with an AUC of 0.88 (95% CI: 0.85–0.92) (Figure 3C).
Figure 4 summarizes all these findings.
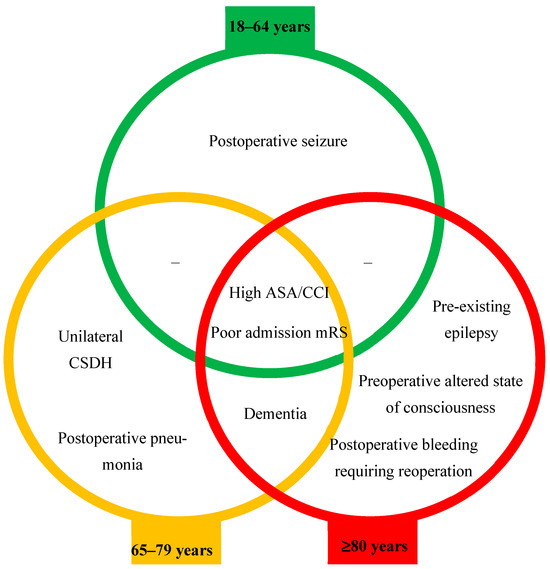
Figure 4.
Age-stratified risk assessment of poor functional outcome at discharge.
3.4. Characteristics of Recurrence
Interestingly, there was no statistically significant difference in recurrence rates between age groups (p = 0.932). However, time to first recurrence increased significantly with age (p = 0.001). The Kaplan–Meier survival analysis evaluated time to first recurrence across age groups. Censoring was defined as either death or discharge without recurrence. Mean time to first recurrence with 95% CI was estimated and reported in Table 1. Recurrence-free survival curves for each age group were plotted (Figure 5), and differences were assessed by log-rank test (p = 0.006).
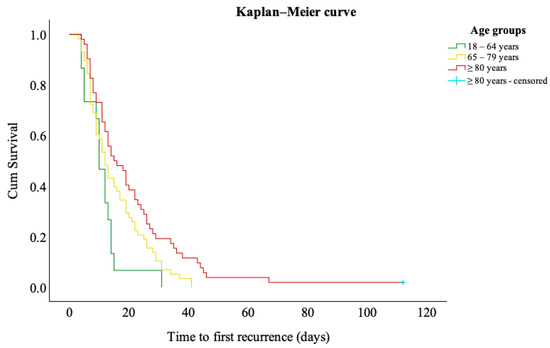
Figure 5.
Kaplan–Meier curves for time to first recurrence stratified by age groups.
4. Discussion
Our retrospective study using an age-stratified approach showed that the sex ratio of CSDH patients shifted from a strong male predominance in the group of younger adults toward a more balanced distribution in the oldest old group. Additionally, this approach allowed stratification of age-category independent risk factors for in-hospital mortality and functional outcome at discharge. For in-hospital mortality, poor neurological status at admission—defined by a preoperative GCS score ≤ 7—and poor functional status at admission were key predictors in the older adult group, while AF and postoperative pneumonia were predictors in the oldest old group. Regarding poor functional outcome at discharge, independent predictors, such as poor functional status at admission and multimorbidity, were consistent across all three groups. Dementia was a relevant predictor in the older adult and oldest old groups. Postoperative seizures were significant only in the younger adult group; unilateral CSDH and postoperative pneumonia were relevant in the older adult group; and pre-existing epilepsy, preoperative altered state of consciousness, and postoperative bleeding requiring reoperation were predictors only in the oldest old group.
The evolution of the sex ratio in CSDH is notable for its gradual transition from strong male predominance in the young population toward a more equal distribution in the elderly. This trend is best observed by comparing age-related sex ratios, as demonstrated in our study. Early research in the 1970s reported that males significantly outnumbered females, with female:male ratios near 1:10 [10,24]. Kanat et al. proposed that the higher incidence of CSDH in males may be explained by greater exposure to head injuries among men and the protective role of estrogen on the blood vessel capillaries in women [25]. Over the following decades, this gap narrowed; by the 1980s, the ratio approached 1:3.5–1:4 [10,24], reflecting a rising proportion of elderly women being diagnosed [10], and a shift in the peak age of onset from 50 years in the 1970s to 70 years in 2010 [24]. Recent research documents this trend continuing, with contemporary studies noting a ratio of 1:2.4 [26], which aligns with the sex ratio of the general cohort in our study (1:2.1). This shift is attributed to factors such as increased female longevity and loss of hormonal protection in the postmenopausal period [27]. Although a male predominance persists, demographic changes including aging populations and female health advancements might drive a measurable rise in female CSDH cases, leading to a more equal sex distribution over time. Furthermore, aging populations led to an increase in in-hospital mortality rates and greater disparities in functional outcome at discharge.
In our study, the in-hospital mortality rate was 3.6%, consistent with recent large-scale epidemiological research on CSDH, reporting rates of 3% and 4.2% [1,28]. Furthermore, our findings reveal that in-hospital mortality predictive factors shifted between cohorts. In older adults, it was independently associated with poor admission neurological status and poor functional status at admission, which align with recent research findings [28,29,30,31]. In the oldest old, AF and postoperative pneumonia were the dominant predictors in our study. These factors are in line with recent study findings [28,32] and highlight the vulnerability of this cohort to systemic complications, underlining the importance of early mobilization, pulmonary hygiene [33,34,35], and overall thoughtful evaluation of risks and benefits of treatment modalities for cardiac diseases in this age group [10,36]. In younger adults, in-hospital mortality occurred in only two patients (1.4%), both of whom had a high CCI, indicating significant morbidity.
Regarding functional outcome at discharge, across all age groups in our study, poor functional status at admission and multimorbidity emerged as the most consistent predictors of unfavorable outcomes. These findings confirm that baseline neurological condition and overall systemic disease burden remain the strongest determinants of postoperative trajectory, irrespective of chronological age. The robustness of these associations aligns with the previous literature highlighting mRS as a powerful prognostic marker in CSDH [7,14,37]. Given their modifiable nature is limited, early identification of these factors should guide discussions with patients and families, set realistic expectations, and prompt aggressive optimization of comorbidities before surgery whenever possible.
While poor functional status at admission and multimorbidity were universal predictors of functional outcome at discharge, several age-specific factors emerged. In younger adults, postoperative seizures significantly impaired postoperative functional recovery with an incidence of 7.5%. A recent large cohort study corroborated our results, reporting a lower incidence rate of postoperative seizures (4.2%), though associated with significantly poorer clinical outcomes [38]. While the global prophylactic use of antiepileptic drugs in these patients has shown mixed evidence, individual case-based decision-making may be warranted in a specific set of patients [39,40]. In line with prior mixed-age series linking postoperative pulmonary complications to increased frailty and impaired recovery [41,42,43], our study identified postoperative pneumonia as an independent determinant of poor functional outcome among older adults, suggesting that systemic vulnerability amplifies the neurological burden in this population. Evidence comparing functional outcomes between unilateral and bilateral hematomas remains limited, often based on small, heterogeneous cohorts. Nevertheless, several reports have suggested less favorable outcomes in patients with bilateral CSDH [43,44,45]. In our large and tiered age-related study, we further clarified this issue by noting that unilateral hematomas independently predicted poorer functional outcomes only in older adults. In the oldest old, dementia, altered state of consciousness, pre-existing epilepsy, and postoperative bleeding requiring reoperation were identified as key determinants of outcome. Dementia likely reduces cognitive reserve, thereby impeding rehabilitation potential [5,46,47,48]. Previous studies have found no direct association between postoperative bleeding requiring reoperation and age [49,50], instead linking it to comorbidities such as arterial hypertension and CKD [13], both of which were significantly more prevalent in our study population, especially in the oldest old group. Furthermore, postoperative bleeding was frequently associated with neurological deterioration and disproportionately affected this elderly group, likely due to their increased neurological vulnerability and frailty, which explains its pronounced negative impact on short-term functional outcomes. Pre-existing epilepsy in CSDH patients is relatively uncommon—our study observed an incidence of 3.9% in the oldest old—but remains understudied. Nevertheless, it may increase the risk of postoperative seizures, thereby elevating the likelihood of poor functional outcomes. Our findings identified pre-existing epilepsy as an independent predictor of adverse functional recovery in this population.
Regarding recurrence, several meta-analyses have debated the role of aging, with some supporting an increased risk of recurrence in the elderly [51], while others found no significant association [6]. Our findings demonstrated that age does not affect recurrence risk; however, it had a significant impact on the time to first recurrence. To date, data on age-associated recurrence-free intervals remain scarce. Our findings demonstrated a statistically significant prolongation of the first recurrence-free interval with increasing age.
Our findings argue for a tiered, age-specific risk stratification model in CSDH surgery. In younger adults, optimizing seizure control could improve recovery. In older adults, the importance of timely surgical evacuation of unilateral CSDH and aggressive prevention of postoperative pneumonia are key. In the oldest old, meticulous surgical planning, strict intraoperative hemostasis to minimize the risk of postoperative bleeding requiring reoperation, and implementation of multidisciplinary strategies targeting comorbidities (such as pre-existing epilepsy and dementia), alongside tailored rehabilitation for cognitive impairment are paramount. Importantly, the absence of significant differences in recurrence rates between age groups suggests that age alone should not dictate surgical candidacy; rather, comorbidity and functional reserve should guide decision-making. Moreover, clinical and radiological vigilance regarding prolonged recurrence-free intervals in older adults and the oldest old are crucial.
5. Limitations
This is a single-center retrospective study, which may limit generalizability of its findings, as institutional protocols and surgical expertise can significantly influence outcomes. Conducted at a tertiary care center in a large Western European city, referral patterns and baseline patient characteristics may differ from those at other institutions. While the large cohort size enhances statistical power, it introduces temporal heterogeneity, since evolving standards of care, including changes in operative techniques and reoperation strategies with the recent adoption of middle meningeal artery embolization, may impact outcomes and thresholds for reoperations over the study period. To mitigate this, the variable “year of surgery” was incorporated into the statistical analyses.
6. Conclusions
In surgically treated CSDH patients, age-stratified analysis reveals that poor baseline function and multimorbidity are universal predictors of unfavorable outcomes, while other risk factors vary with age. Older adults are most vulnerable to mortality from poor neurological and functional statuses at admission, whereas the oldest old are primarily threatened by pulmonary complications and cardiovascular history. Functional recovery is shaped by both shared and age-specific factors, including postoperative seizures in the younger adults; unilateral hematomas, dementia, and postoperative pneumonia in the older adults; pre-existing epilepsy, preoperative altered state of consciousness, postoperative bleeding requiring reoperation, and dementia in the oldest old. Moreover, recurrence-free intervals are prolonged with increasing age. These findings underscore the importance of individualized perioperative strategies that integrate age-specific risk profiles into surgical decision-making, counseling, and postoperative care planning.
Author Contributions
S.S. acquired, analyzed, and interpreted the data, drafted the initial manuscript, and reviewed and revised the final version of the manuscript; S.A.-R., M.A. and E.T. acquired the data, and reviewed and revised the final version of the manuscript.; J.R., T.F.D., O.G., L.S., R.J. and P.D. analyzed and interpreted the data, and reviewed and revised the final version of the manuscript.; U.S. reviewed and revised the final version of the manuscript for important intellectual content.; M.C. conceptualized and designed the study, analyzed and interpreted the data, drafted the initial manuscript, revised the manuscript for important intellectual content, and reviewed and revised the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This retrospective study was performed in accordance with the ethical standards of the institutional research committee and the Code of Ethics of the World Medical Association (Declaration of Helsinki). The Institutional Review Board approved the study protocol (Medical Faculty, University of Duisburg-Essen, Registration number: 22-10763-BO; approval date 9 February 2023).
Informed Consent Statement
In our study, since we analyzed only retrospective data from existing medical records of routine clinical practice, an informed consent was not required.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
AI-assisted copy-editing using Perplexity AI was utilized to improve the readability, grammar, and style of the manuscript. This process involved refining human-generated text without altering the scientific content. All final text revisions were reviewed and approved by the authors to ensure accuracy and integrity. We acknowledge support by the Open Access Publication Fund of the University of Duisburg-Essen.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rauhala, M.; Helén, P.; Huhtala, H.; Heikkilä, P.; Iverson, G.L.; Niskakangas, T.; Öhman, J.; Luoto, T.M. Chronic subdural hematoma—Incidence, complications, and financial impact. Acta Neurochir. 2020, 162, 2033–2043. [Google Scholar] [CrossRef] [PubMed]
- Ou, Y.; Dong, J.; Wu, L.; Xu, L.; Wang, L.; Liu, B.; Li, J.; Liu, W. A comparative study of chronic subdural hematoma in three age ranges: Below 40 years, 41–79 years, and 80 years and older. Clin. Neurol. Neurosurg. 2019, 178, 63–69. [Google Scholar] [CrossRef]
- Kudo, H.; Kuwamura, K.; Izawa, I.; Sawa, H.; Tamaki, N. Chronic Subdural Hematoma in Elderly People: Present Status on Awaji Island and Epidemiological Prospect. Neurol. Med.-Chir. 1992, 32, 207–209. [Google Scholar] [CrossRef]
- Dobran, M. Spontaneous chronic subdural hematoma in young adult: The role of missing coagulation facto. G. Di Chir. J. Surg. 2017, 38, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Gondar, R.; Schaller, K.; Meling, T. Chronic Subdural Hematoma (cSDH): A review of the current state of the art. Brain Spine 2021, 1, 100300. [Google Scholar] [CrossRef]
- Bartek, J.; Sjåvik, K.; Dhawan, S.; Sagberg, L.M.; Kristiansson, H.; Ståhl, F.; Förander, P.; Chen, C.C.; Jakola, A.S. Clinical Course in Chronic Subdural Hematoma Patients Aged 18–49 Compared to Patients 50 Years and Above: A Multicenter Study and Meta-Analysis. Front. Neurol. 2019, 10, 311. [Google Scholar] [CrossRef]
- Ou, Y.; Dong, J.; Wu, L.; Xu, L.; Wang, L.; Liu, B.; Li, J.; Liu, W. The Clinical Characteristics, Treatment, and Outcomes of Chronic Subdural Hematoma in Young Patients. World Neurosurg. 2019, 125, e1241–e1246. [Google Scholar] [CrossRef]
- Won, Y.D.; Yi, H.-J.; Lee, Y.J.; Chun, H.-J.; Cho, H.; Bak, K.-H. Chronic Subdural Hematoma in Young Adult: An Age Comparison Study. Korean J. Neurotrauma 2013, 9, 6–11. [Google Scholar] [CrossRef][Green Version]
- Liliang, P.-C.; Tsai, Y.-D.; Liang, C.-L.; Lee, T.-C.; Chen, H.-J. Chronic subdural haematoma in young and extremely aged adults: A comparative study of two age groups. Injury 2002, 33, 345–348. [Google Scholar] [CrossRef]
- Baechli, H.; Nordmann, A.; Bucher, H.C.; Gratzl, O. Demographics and prevalent risk factors of chronic subdural haematoma: Results of a large single-center cohort study. Neurosurg. Rev. 2004, 27, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Benek, H.B.; Akcay, E. Concomitant chronic subdural hematomas and arachnoid cysts in young adults. F1000Research 2022, 10, 421. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, K.; Sorimachi, T.; Honda, Y.; Ishizaka, H.; Baba, T.; Osada, T.; Nishiyama, J.; Inoue, G.; Matsumae, M. Chronic Subdural Hematomas Associated with Arachnoid Cysts: Significance in Young Patients with Chronic Subdural Hematomas. Neurol. Med.-Chir. 2015, 55, 727–734. [Google Scholar] [CrossRef]
- Younsi, A.; Riemann, L.; Habel, C.; Fischer, J.; Beynon, C.; Unterberg, A.W.; Zweckberger, K. Relevance of comorbidities and antithrombotic medication as risk factors for reoperation in patients with chronic subdural hematoma. Neurosurg. Rev. 2021, 45, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Leroy, H.-A.; Aboukaïs, R.; Reyns, N.; Bourgeois, P.; Labreuche, J.; Duhamel, A.; Lejeune, J.-P. Predictors of functional outcomes and recurrence of chronic subdural hematomas. J. Clin. Neurosci. 2015, 22, 1895–1900. [Google Scholar] [CrossRef] [PubMed]
- Cheon, T.M.; Kim, K.M.; Bae, J.W.; Shim, Y.S.; Hyun, D.-K. Functional outcomes of surgically treated chronic subdural hematoma and the factors associated with outcomes: A retrospective study. J. Korean Soc. Geriatr. Neurosurg. 2023, 19, 39–44. [Google Scholar] [CrossRef]
- Chandran, R.S.; Nagar, M.; Sharmad, M.S.; Prabhakar, R.B.; Peethambaran, A.K.; Kumar, S.; Sharma, S.; Jain, S.K. Single Parietal Burr-hole Craniostomy with Irrigation and Drainage for Unilateral Chronic Subdural Hematoma in Young Adults <40 Years: A Rationale behind the Procedure. J. Neurosci. Rural. Pract. 2019, 8, 389–394. [Google Scholar] [CrossRef]
- Amipara, R.; Winders, H.R.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Al-Hasan, M.N. Impact of follow up blood cultures on outcomes of patients with community-onset gram-negative bloodstream infection. EClinicalMedicine 2021, 34, 100811. [Google Scholar] [CrossRef]
- Fuchs, J.; Gaertner, B.; Perlitz, H.; Kuttig, T.; Klingner, A.; Baumert, J.; Hüther, A.; Kuhnert, R.; Wolff, J.; Scheidt-Nave, C. Study on Health of Older People in Germany (Gesundheit 65+): Objectives, design and implementation. J. Health Monit. 2023, 8, 61. [Google Scholar]
- Vrettos, I.; Anagnostopoulos, F.; Voukelatou, P.; Kyvetos, A.; Theotoka, D.; Niakas, D. Does old age comprise distinct subphases? Evidence from an analysis of the relationship between age and activities of daily living, comorbidities, and geriatric syndromes. Ann. Geriatr. Med. Res. 2024, 28, 65. [Google Scholar] [CrossRef]
- Wang, H.-y.; Lv, X.; Du, J.; Kong, G.; Zhang, L. Age-and gender-specific prevalence of frailty and its outcomes in the longevous population: The Chinese longitudinal healthy longevity study. Front. Med. 2021, 8, 719806. [Google Scholar] [CrossRef]
- Shenkin, S.D.; Harrison, J.K.; Wilkinson, T.; Dodds, R.M.; Ioannidis, J.P. Systematic reviews: Guidance relevant for studies of older people. Age Ageing 2017, 46, 722–728. [Google Scholar] [CrossRef]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the rule of ten events per variable in logistic and Cox regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Toi, H.; Kinoshita, K.; Hirai, S.; Takai, H.; Hara, K.; Matsushita, N.; Matsubara, S.; Otani, M.; Muramatsu, K.; Matsuda, S. Present epidemiology of chronic subdural hematoma in Japan: Analysis of 63,358 cases recorded in a national administrative database. J. Neurosurg. 2017, 128, 222–228. [Google Scholar] [CrossRef]
- Kanat, A.; Kayaci, S.; Kazdal, H.; Terzi, Y. Chronic subdural hematoma in adults: Why does it occur more often in males than females? Influence of patient’s sexual gender on occurrence. J. Neurosurg. Sci. 2010, 54, 99–103. [Google Scholar]
- Sioutas, G.S.; Sweid, A.; Chen, C.-J.; Becerril-Gaitan, A.; Al Saiegh, F.; El Naamani, K.; Abbas, R.; Amllay, A.; Birkenstock, L.; Cain, R.E. Surgical evacuation for chronic subdural hematoma: Predictors of reoperation and functional outcomes. World Neurosurg. X 2024, 21, 100246. [Google Scholar] [CrossRef]
- Ou, Y.; Fan, W.; Yu, X.; Wu, L.; Liu, W. A single-center analysis of sex differences in patients with chronic subdural hematoma in China. Front. Neurol. 2022, 13, 888526. [Google Scholar] [CrossRef]
- Posti, J.P.; Luoto, T.M.; Sipilä, J.O.; Rautava, P.; Kytö, V. Prognosis of patients with operated chronic subdural hematoma. Sci. Rep. 2022, 12, 7020. [Google Scholar] [CrossRef]
- Maeda, T.; Kikkawa, Y.; Ehara, T.; Tsuchiya, R.; Tabata, S.; Onodera, K.; Kimura, T.; Take, Y.; Suzuki, K.; Kurita, H. Clinical outcomes in elderly patients with chronic subdural hematoma: Validation of irrigation assignment based on hematoma characteristics. Life 2024, 14, 518. [Google Scholar] [CrossRef] [PubMed]
- De Bonis, P.; Olei, S.; Mongardi, L.; Cavallo, M.A.; Santantonio, M.; Trevisi, G.; Anile, C.; Mangiola, A. Chronic subdural hematoma in patients aged 80 years and older: A two-centre study. Clin. Neurol. Neurosurg. 2018, 170, 88–92. [Google Scholar] [CrossRef]
- Blaauw, J.; Jacobs, B.; Hertog, H.M.D.; van der Gaag, N.A.; Jellema, K.; Dammers, R.; Kho, K.H.; Groen, R.J.M.; van der Naalt, J.; Lingsma, H.F. Mortality after chronic subdural hematoma is associated with frailty. Acta Neurochir. 2022, 164, 3133–3141. [Google Scholar] [CrossRef] [PubMed]
- Rohde, V.; Graf, G.; Hassler, W. Complications of burr-hole craniostomy and closed-system drainage for chronic subdural hematomas: A retrospective analysis of 376 patients. Neurosurg. Rev. 2002, 25, 89–94. [Google Scholar] [CrossRef]
- Nozawa, Y.; Harada, K.; Noma, K.; Katayama, Y.; Hamada, M.; Ozaki, T. Association Between Early Mobilization and Postoperative Pneumonia Following Robot-assisted Minimally Invasive Esophagectomy in Patients with Thoracic Esophageal Squamous Cell Carcinoma. Phys. Ther. Res. 2024, 27, 121–127. [Google Scholar] [CrossRef]
- Sigona, A.; Richman, D.C. Identifying and reducing risks of postoperative pulmonary complications. J. Oral Maxillofac. Anesth. 2023, 2, 30. [Google Scholar] [CrossRef]
- Chebib, N.; Cuvelier, C.; Malézieux-Picard, A.; Parent, T.; Roux, X.; Fassier, T.; Müller, F.; Prendki, V. Correction to: Pneumonia prevention in the elderly patients: The other sides. Aging Clin. Exp. Res. 2020, 33, 3149. [Google Scholar] [CrossRef]
- ten Cate, H.; De Bonis, P.; Trevisi, G.; de Waure, C.; Sferrazza, A.; Volpe, M.; Pompucci, A.; Anile, C.; Mangiola, A. Antiplatelet/Anticoagulant Agents and Chronic Subdural Hematoma in the Elderly. PLoS ONE 2013, 8, e68732. [Google Scholar] [CrossRef]
- Weimer, J.M.; Gordon, E.; Frontera, J.A. Predictors of Functional Outcome After Subdural Hematoma: A Prospective Study. Neurocritical Care 2016, 26, 70–79. [Google Scholar] [CrossRef]
- Wu, L.; Guo, X.; Ou, Y.; Yu, X.; Zhu, B.; Li, Y.; Liu, W. Seizure after chronic subdural hematoma evacuation: Associated factors and effect on clinical outcome. Front. Neurol. 2023, 14, 1190878. [Google Scholar] [CrossRef] [PubMed]
- Grobelny, B.T.; Ducruet, A.F.; Zacharia, B.E.; Hickman, Z.L.; Andersen, K.N.; Sussman, E.; Carpenter, A.; Connolly, E.S. Preoperative antiepileptic drug administration and the incidence of postoperative seizures following bur hole–treated chronic subdural hematoma. J. Neurosurg. 2009, 111, 1257–1262. [Google Scholar] [CrossRef]
- Lavergne, P.; Labidi, M.; Brunet, M.-C.; Lessard Bonaventure, P.; Zetchi, A.; Carrondo Cottin, S.; Simonyan, D.; Turmel, A. Efficacy of antiseizure prophylaxis in chronic subdural hematoma: A cohort study on routinely collected health data. J. Neurosurg. 2020, 132, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Brennan, P.M.; Kolias, A.G.; Joannides, A.J.; Shapey, J.; Marcus, H.J.; Gregson, B.A.; Grover, P.J.; Hutchinson, P.J.; Coulter, I.C. The management and outcome for patients with chronic subdural hematoma: A prospective, multicenter, observational cohort study in the United Kingdom. J. Neurosurg. 2017, 127, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Ma, Y.; Zhao, X.; Yang, C.; Gu, J.; Weng, W.; Hui, J.; Mao, Q.; Gao, G.; Feng, J. Risk factors of hospital mortality in chronic subdural hematoma: A retrospective analysis of 1117 patients, a single institute experience. J. Clin. Neurosci. 2019, 67, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, J.H. Clinical Characteristics of Bilateral versus Unilateral Chronic Subdural Hematoma. Korean J. Neurotrauma 2014, 10, 49–54. [Google Scholar] [CrossRef]
- Park, H.S.; Park, E.S.; Park, J.B.; Kwon, S.C.; Lyo, I.U.; Kim, M.H.; Sim, H.B. Chronic Subdural Hematomas: Comparison between Unilateral and Bilateral Involvement. Korean J. Neurotrauma 2014, 10, 55–59. [Google Scholar] [CrossRef]
- Agawa, Y.; Mineharu, Y.; Tani, S.; Adachi, H.; Imamura, H.; Sakai, N. Bilateral Chronic Subdural Hematoma is Associated with Rapid Progression and Poor Clinical Outcome. Neurol. Med. Chir. 2016, 56, 198–203. [Google Scholar] [CrossRef]
- Raj, R.; Tommiska, P.; Luoto, T.; Leinonen, V.; Koivisto, T.; Tetri, S.; Posti, J.; Lönnrot, K. Failure to improve—Identifying risk factors for poor functional recovery following chronic subdural hematoma surgery. Age Ageing 2025, 54, afaf056. [Google Scholar] [CrossRef]
- Feinkohl, I.; Winterer, G.; Spies, C.D.; Pischon, T. Cognitive Reserve and the Risk of Postoperative Cognitive Dysfunction. Dtsch. Ärzteblatt Int. 2017, 114, 110. [Google Scholar] [CrossRef]
- Chen, L.; Au, E.; Saripella, A.; Kapoor, P.; Yan, E.; Wong, J.; Tang-Wai, D.F.; Gold, D.; Riazi, S.; Suen, C.; et al. Postoperative outcomes in older surgical patients with preoperative cognitive impairment: A systematic review and meta-analysis. J. Clin. Anesth. 2022, 80, 110883. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wang, H.; Zhao, J.; Wang, C.; Liu, H.; Wang, C.; Li, A.; Hu, J. Preoperative Fibrinogen Levels and Function as Predictive Factors for Acute Bleeding in the Hematoma Cavity After Burr Hole Drainage in Patients with CSDH. World Neurosurg. 2023, 180, e364–e375. [Google Scholar] [CrossRef]
- Pang, C.H.; Lee, S.E.; Kim, C.H.; Kim, J.E.; Kang, H.S.; Park, C.K.; Paek, S.H.; Kim, C.H.; Jahng, T.A.; Kim, J.W.; et al. Acute intracranial bleeding and recurrence after bur hole craniostomy for chronic subdural hematoma. J. Neurosurg. 2015, 123, 65–74. [Google Scholar] [CrossRef]
- Mishra, R.; Deora, H.; Florez-Perdomo, W.A.; Moscote-Salazar, L.R.; Garcia-Ballestas, E.; Rahman, M.M.; Shrivastava, A.; Raj, S.; Chavda, V.; Montemurro, N.; et al. Clinical and Radiological Characteristics for Recurrence of Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis. Neurol. Int. 2022, 14, 683–695. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).