

A Real-World Comparison of the Safety Profile for Immune Checkpoint Inhibitors in Oncology Patients
 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
Statistical Analysis
3. Results
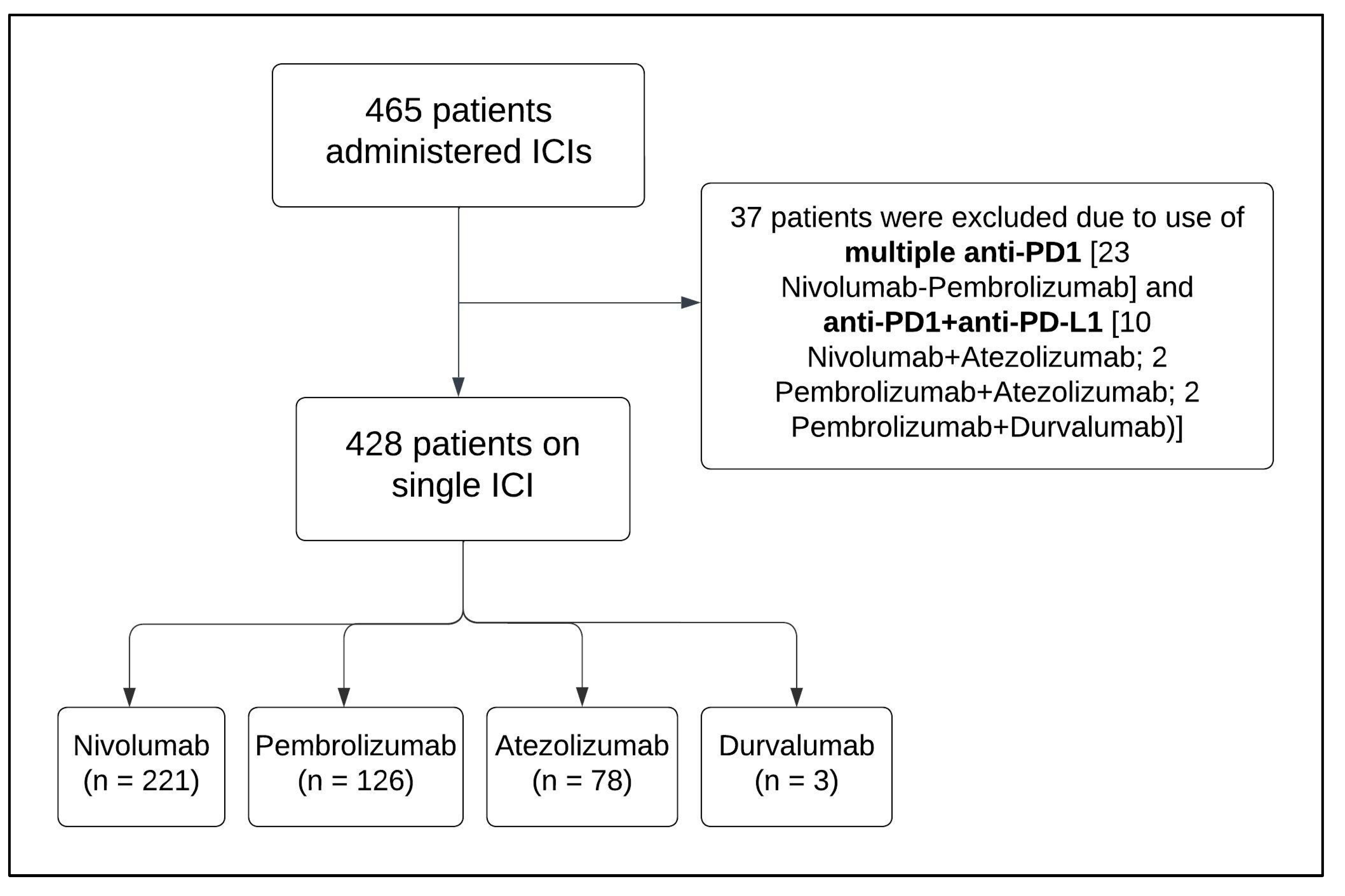
3.1. Patient Selection and Baseline Characteristics
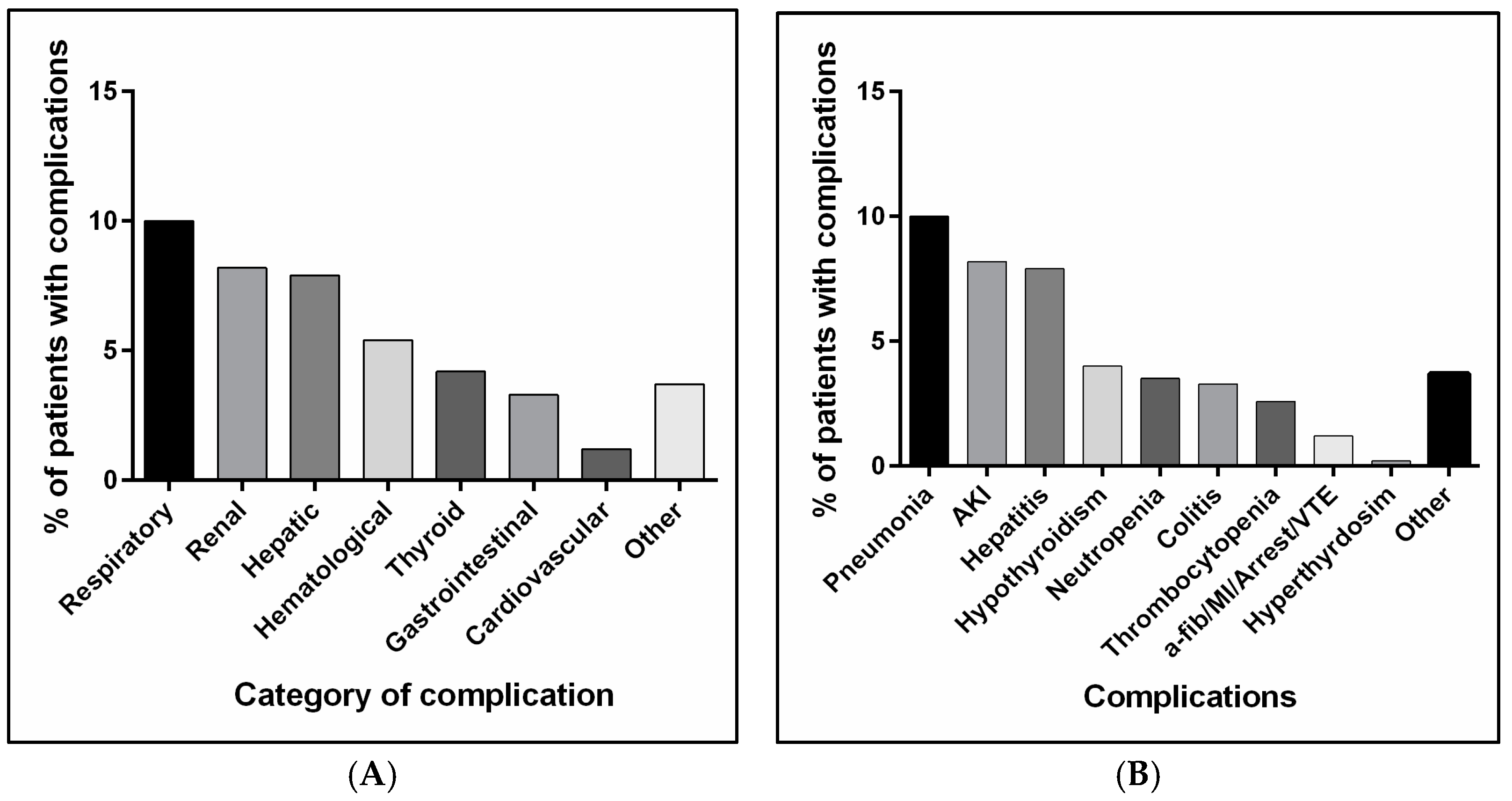
3.2. Complications and Side Effects Associated with Anti-PD1 or Anti-PD-L1 Administration
3.3. Onset of Complications/Side Effects Associated with Anti-PD1 or Anti-PD-L1
3.4. Assessment of Risk Factors Triggering Complications and Side Effect Occurrence with Anti-PD1 or Anti-PD-L1
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Homet Moreno, B.; Ribas, A. Anti-programmed cell death protein-1/ligand-1 therapy in different cancers. Br. J. Cancer 2015, 112, 1421–1427. [Google Scholar] [CrossRef]
- Johnson, D.B.; Nebhan, C.A.; Moslehi, J.J.; Balko, J.M. Immune-checkpoint inhibitors: Long-term implications of toxicity. Nat. Rev. Clin. Oncol. 2022, 19, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Wu, H.; Wu, J.; Ding, P.; He, J.; Sang, M.; Liu, L. Mechanisms of immune checkpoint inhibitors: Insights into the regulation of circular RNAS involved in cancer hallmarks. Cell Death Dis. 2024, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Vaddepally, R.K.; Kharel, P.; Pandey, R.; Garje, R.; Chandra, A.B. Review of Indications of FDA-Approved Immune Checkpoint Inhibitors per NCCN Guidelines with the Level of Evidence. Cancers 2020, 12, 738. [Google Scholar] [CrossRef]
- Hoshiko, S.; Makabe, O.; Nojiri, C.; Katsumata, K.; Satoh, E.; Nagaoka, K. Molecular cloning and characterization of the Streptomyces hygroscopicus alpha-amylase gene. J. Bacteriol. 1987, 169, 1029–1036. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brahmer, J.R.; Callahan, M.K.; Flores-Chávez, A.; Keegan, N.; Khamashta, M.A.; Lambotte, O.; Marlette, X.; Prat, A.; Suarez-Almazor, M.E. Immune-related adverse events of checkpoint inhibitors. Nat. Rev. Dis. Primers 2020, 6, 38. [Google Scholar] [CrossRef]
- Wang, F.; Yang, S.; Palmer, N.; Fox, K.; Kohane, I.S.; Liao, K.P.; Yu, K.H.; Kou, S.C. Real-world data analyses unveiled the immune-related adverse effects of immune checkpoint inhibitors across cancer types. NPJ Precis. Oncol. 2021, 5, 82. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Kim, R.; Yu, T.; Gayle, J.A.; Wassel, C.L.; Dreyfus, J.; Phatak, H.; George, S. Real-World Clinical and Economic Outcomes in Selected Immune-Related Adverse Events Among Patients with Cancer Receiving Immune Checkpoint Inhibitors. Oncologist 2021, 26, e2002–e2012. [Google Scholar] [CrossRef]
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580. [Google Scholar] [CrossRef]
- Corrigan-Curay, J.; Sacks, L.; Woodcock, J. Real-World Evidence and Real-World Data for Evaluating Drug Safety and Effectiveness. JAMA 2018, 320, 867–868. [Google Scholar] [CrossRef]
- Jarow, J.P.; LaVange, L.; Woodcock, J. Multidimensional Evidence Generation and FDA Regulatory Decision Making: Defining and Using “Real-World” Data. JAMA 2017, 318, 703–704. [Google Scholar] [CrossRef] [PubMed]
- Kao, J.C.; Liao, B.; Markovic, S.N.; Klein, C.J.; Naddaf, E.; Staff, N.P.; Liewluck, T.; Hammack, J.E.; Sandroni, P.; Finnes, H.; et al. Neurological Complications Associated With Anti-Programmed Death 1 (PD-1) Antibodies. JAMA Neurol. 2017, 74, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Mikami, T.; Liaw, B.; Asada, M.; Niimura, T.; Zamami, Y.; Green-LaRoche, D.; Pai, L.; Levy, M.; Jeyapalan, S. Neuroimmunological adverse events associated with immune checkpoint inhibitor: A retrospective, pharmacovigilance study using FAERS database. J. Neurooncol 2021, 152, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Hodi, F.S.; Giobbie-Hurder, A.; Ott, P.A.; Buchbinder, E.I.; Haq, R.; Tolaney, S.; Barroso-Sousa, R.; Zhang, K.; Donahue, H.; et al. Characterization of Thyroid Disorders in Patients Receiving Immune Checkpoint Inhibition Therapy. Cancer Immunol. Res. 2017, 5, 1133–1140. [Google Scholar] [CrossRef]
- Naidoo, J.; Wang, X.; Woo, K.M.; Iyriboz, T.; Halpenny, D.; Cunningham, J.; Chaft, J.E.; Segal, N.H.; Callahan, M.K.; Lesokhin, A.M.; et al. Pneumonitis in Patients Treated With Anti-Programmed Death-1/Programmed Death Ligand 1 Therapy. J. Clin. Oncol. 2017, 35, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Abu-Sbeih, H.; Mao, E.; Ali, N.; Ali, F.S.; Qiao, W.; Lum, P.; Raju, G.; Shuttlesworth, G.; Stroehlein, J.; et al. Immune-checkpoint inhibitor-induced diarrhea and colitis in patients with advanced malignancies: Retrospective review at MD Anderson. J. Immunother. Cancer 2018, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.C.; Lin, J.Y.; Hsu, M.Y.; Lin, P.C. Effectiveness and safety of immune checkpoint inhibitors: A retrospective study in Taiwan. PLoS ONE 2018, 13, e0202725. [Google Scholar] [CrossRef]
- Ide, T.; Araki, T.; Koizumi, T. Thromboembolism during immune checkpoint inhibitor therapy: Frequency and risk factors. Discov. Oncol. 2024, 15, 527. [Google Scholar] [CrossRef]
- Benkhadra, M.; Elazzazy, S.; Hamad, A.A.; Elkhatim, M.S.; Gulied, A.; Sahal, A.O.; Alasmar, A.; Jibril, F.I.; Afifi, H.M.; Nasser, S.; et al. Hematological Toxicity of Immune Checkpoint Inhibitors: Real-World Retrospective Outcomes from a Cohort Study in Qatar. Blood 2023, 142, 5378. [Google Scholar] [CrossRef]
- Hountondji, L.; Ferreira De Matos, C.; Lebosse, F.; Quantin, X.; Lesage, C.; Palassin, P.; Rivet, V.; Faure, S.; Pageaux, G.P.; Assenat, E.; et al. Clinical pattern of checkpoint inhibitor-induced liver injury in a multicentre cohort. JHEP Rep. 2023, 5, 100719. [Google Scholar] [CrossRef]
- Yin, Y.; Liu, B.J.; Zhang, Y.H.; Qiu, X.Y. Hepatitis B virus reactivation risk associated with immune checkpoint inhibitors in tumor treatment: A retrospective study. Jpn. J. Clin. Oncol. 2024, 54, 1288–1297. [Google Scholar] [CrossRef]
- She, J.; Liu, H.; Wu, H.; Tuerhongjiang, G.; Zheng, T.; Bai, L. Cardiotoxicity Related to Immune Checkpoint Inhibitors: A Real-World Retrospective Analysis. Front. Cardiovasc. Med. 2022, 9, 838488. [Google Scholar] [CrossRef]
- Waheed, N.; Fradley, M.G.; DeRemer, D.L.; Mahmoud, A.; Shah, C.P.; Langaee, T.Y.; Lipori, G.P.; March, K.; Pepine, C.J.; Cooper-DeHoff, R.M.; et al. Newly diagnosed cardiovascular disease in patients treated with immune checkpoint inhibitors: A retrospective analysis of patients at an academic tertiary care center. Cardiooncology 2021, 7, 10. [Google Scholar] [CrossRef]
- Chauhan, A.; Burkeen, G.; Houranieh, J.; Arnold, S.; Anthony, L. Immune checkpoint-associated cardiotoxicity: Case report with systematic review of literature. Ann. Oncol. 2017, 28, 2034–2038. [Google Scholar] [CrossRef] [PubMed]
- Barrios, C.; de Lima Lopes, G.; Yusof, M.M.; Rubagumya, F.; Rutkowski, P.; Sengar, M. Barriers in access to oncology drugs—A global crisis. Nat. Rev. Clin. Oncol. 2023, 20, 7–15. [Google Scholar] [CrossRef]
- Leheny, S. ‘Adverse Event’, Not the Same as ‘Side Effect’. 2017. Available online: https://www.pharmacytimes.com/view/adverse-event-not-the-same-as-side-effect#:~:text=Adverse%20events%20are%20unintended%20pharmacologic,occurs%20due%20to%20drug%20therapy (accessed on 3 November 2024).
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef]
- Hu, S.; Tang, Z.; Harrison, J.P.; Hertel, N.; Penrod, J.R.; May, J.R.; Juarez-Garcia, A.; Holdgate, O. Economic Evaluation of Nivolumab Versus Docetaxel for the Treatment of Advanced Squamous and Non-squamous Non-small Cell Lung Cancer After Prior Chemotherapy in China. Pharmacoecon Open 2023, 7, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef]
- Winer, A.; Bodor, J.N.; Borghaei, H. Identifying and managing the adverse effects of immune checkpoint blockade. J. Thorac. Dis. 2018, 10, S480–S489. [Google Scholar] [CrossRef]
- Villadolid, J.; Amin, A. Immune checkpoint inhibitors in clinical practice: Update on management of immune-related toxicities. Transl. Lung Cancer Res. 2015, 4, 560–575. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef]
- Marin-Acevedo, J.A.; Chirila, R.M.; Dronca, R.S. Immune Checkpoint Inhibitor Toxicities. Mayo Clin. Proc. 2019, 94, 1321–1329. [Google Scholar] [CrossRef]
- Bajwa, R.; Cheema, A.; Khan, T.; Amirpour, A.; Paul, A.; Chaughtai, S.; Patel, S.; Patel, T.; Bramson, J.; Gupta, V.; et al. Adverse Effects of Immune Checkpoint Inhibitors (Programmed Death-1 Inhibitors and Cytotoxic T-Lymphocyte-Associated Protein-4 Inhibitors): Results of a Retrospective Study. J. Clin. Med. Res. 2019, 11, 225–236. [Google Scholar] [CrossRef]
- Pillai, R.N.; Behera, M.; Owonikoko, T.K.; Kamphorst, A.O.; Pakkala, S.; Belani, C.P.; Khuri, F.R.; Ahmed, R.; Ramalingam, S.S. Comparison of the toxicity profile of PD-1 versus PD-L1 inhibitors in non-small cell lung cancer: A systematic analysis of the literature. Cancer 2018, 124, 271–277. [Google Scholar] [CrossRef] [PubMed]
- El Majzoub, I.; Qdaisat, A.; Thein, K.Z.; Win, M.A.; Han, M.M.; Jacobson, K.; Chaftari, P.S.; Prejean, M.; Reyes-Gibby, C.; Yeung, S.J. Adverse Effects of Immune Checkpoint Therapy in Cancer Patients Visiting the Emergency Department of a Comprehensive Cancer Center. Ann. Emerg. Med. 2019, 73, 79–87. [Google Scholar] [CrossRef]
- Sengul Samanci, N.; Cikman, D.I.; Oruc, K.; Bedir, S.; Celik, E.; Degerli, E.; Derin, S.; Demirelli, F.H.; Ozguroglu, M. Immune-related adverse events associated with immune checkpoint inhibitors in patients with cancer. Tumori 2021, 107, 304–310. [Google Scholar] [CrossRef]
- Al Nuhait, M.; Bajnaid, E.; Al Otaibi, A.; Al Shammari, A.; Al Awlah, Y. Real-world safety experience with immune checkpoint inhibitors in Saudi Arabia. Sci. Prog. 2021, 104, 36850421997302. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Li, N.; Liang, X.; Zhang, S.; Fan, Q.; Yin, X.; Zhuang, Z.; Liu, Y.; Zhang, J.; et al. Immune checkpoint inhibitors-associated cardiotoxicity in immunotherapy trials on gastrointestinal cancer patients. Chin. Med. J. 2022, 135, 988–990. [Google Scholar] [CrossRef]
- Benz, S.; Sherman, K.A.; Dasanu, C.A.; Alvarez-Argote, J. Immune checkpoint inhibitor-related adverse events: Real-world experience from a single veterans’ affairs medical center. J. Oncol. Pharm. Pract. 2024, 30, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Gougis, P.; Jochum, F.; Abbar, B.; Dumas, E.; Bihan, K.; Lebrun-Vignes, B.; Moslehi, J.; Spano, J.P.; Laas, E.; Hotton, J.; et al. Clinical spectrum and evolution of immune-checkpoint inhibitors toxicities over a decade-a worldwide perspective. EClinicalMedicine 2024, 70, 102536. [Google Scholar] [CrossRef]
- Albarran-Artahona, V.; Laguna, J.C.; Gorria, T.; Torres-Jimenez, J.; Pascal, M.; Mezquita, L. Immune-Related Uncommon Adverse Events in Patients with Cancer Treated with Immunotherapy. Diagnostics 2022, 12, 2091. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhou, S.; Yang, F.; Qi, X.; Wang, X.; Guan, X.; Shen, C.; Duma, N.; Vera Aguilera, J.; Chintakuntlawar, A.; et al. Treatment-Related Adverse Events of PD-1 and PD-L1 Inhibitors in Clinical Trials: A Systematic Review and Meta-analysis. JAMA Oncol. 2019, 5, 1008–1019. [Google Scholar] [CrossRef] [PubMed]
- Spagnuolo, A.; Gridelli, C. “Comparison of the toxicity profile of PD-1 versus PD-L1 inhibitors in non-small cell lung cancer”: Is there a substantial difference or not? J. Thorac. Dis. 2018, 10, S4065–S4068. [Google Scholar] [CrossRef]
- Rofi, E.; Del Re, M.; Arrigoni, E.; Rizzo, M.; Fontanelli, L.; Crucitta, S.; Gianfilippo, G.; Restante, G.; Fogli, S.; Porta, C.; et al. Clinical pharmacology of monoclonal antibodies targeting anti-PD-1 axis in urothelial cancers. Crit. Rev. Oncol. Hematol. 2019, 144, 102812. [Google Scholar] [CrossRef]
- Banna, G.L.; Cantale, O.; Bersanelli, M.; Del Re, M.; Friedlaender, A.; Cortellini, A.; Addeo, A. Are anti-PD1 and anti-PD-L1 alike? The non-small-cell lung cancer paradigm. Oncol. Rev. 2020, 14, 490. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Gatti, M.; Gelsomino, F.; Ardizzoni, A.; Poluzzi, E.; De Ponti, F. Lessons to be Learnt from Real-World Studies on Immune-Related Adverse Events with Checkpoint Inhibitors: A Clinical Perspective from Pharmacovigilance. Target. Oncol. 2020, 15, 449–466. [Google Scholar] [CrossRef]
- Weber, J.S. Practical management of immune-related adverse events from immune checkpoint protein antibodies for the oncologist. Am. Soc. Clin. Oncol. Educ. Book. 2012, 32, 174–177. [Google Scholar] [CrossRef]
- Puzanov, I.; Diab, A.; Abdallah, K.; Bingham, C.O., 3rd; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; LeBoeuf, N.R.; et al. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5, 95. [Google Scholar] [CrossRef]
- Cheema, P.K.; Iafolla, M.A.J.; Abdel-Qadir, H.; Bellini, A.B.; Chatur, N.; Chandok, N.; Comondore, V.R.; Cunningham, M.; Halperin, I.; Hu, A.B.; et al. Managing Select Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitors. Curr. Oncol. 2024, 31, 6356–6383. [Google Scholar] [CrossRef] [PubMed]
- Schneider, B.J.; Naidoo, J.; Santomasso, B.D.; Lacchetti, C.; Adkins, S.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 4073–4126. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.S.; D’Angelo, S.P.; Minor, D.; Hodi, F.S.; Gutzmer, R.; Neyns, B.; Hoeller, C.; Khushalani, N.I.; Miller, W.H., Jr.; Lao, C.D.; et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): A randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015, 16, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Wanchoo, R.; Karam, S.; Uppal, N.N.; Barta, V.S.; Deray, G.; Devoe, C.; Launay-Vacher, V.; Jhaveri, K.D.; Cancer; Kidney International Network Workgroup on Immune Checkpoint, I. Adverse Renal Effects of Immune Checkpoint Inhibitors: A Narrative Review. Am. J. Nephrol. 2017, 45, 160–169. [Google Scholar] [CrossRef]
- Khan, O.F.; Monzon, J. Diagnosis, monitoring, and management of adverse events from immune checkpoint inhibitor therapy. Curr. Oncol. 2020, 27 (Suppl. S2), S43–S50. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 428) | Nivolumab (n = 221) | Pembrolizumab (n = 126) | Atezolizumab (n = 78) | Durvalumab (n = 3) | p-Value |
|---|---|---|---|---|---|---|
| Age [median (IQR)] | 64 (20) | 64 (21) | 61 (19) | 64 (17.75) | 67 (5.5) | 0.147 |
| Male gender, n (%) | 278 (65.0) | 154 (69.7) | 73 (57.9) | 48 (61.5) | 3 (100) | 0.075 |
| Age group, n (%) | 0.005 | |||||
| <30 yrs | 11 (2.6) | 10 (4.5) | 1 (0.8) | 0 | 0 | |
| 30 to <60 yrs | 154 (36.0) | 74 (33.5) | 59 (46.8) | 21 (26.9) | 0 | |
| ≥60 yrs | 263 (61.4) | 137 (62.0) | 66 (52.4) | 57 (73.1) | 3 (100.0) | |
| Primary diagnosed cancer, n (%) * | 0.046 | |||||
| Solid | 406 (95.3) | 203 (92.7) | 122 (96.8) | 78 (100.0) | 3 (100.0) | |
| Hematological | 20 (4.7) | 16 (7.3) | 4 (3.2) | 0 | 0 | |
| Cancer stage right before ICI initiation, n (%) * | 0.003 | |||||
| Stage II | 40 (9.4) | 20 (9.1) | 8 (6.4) | 12 (15.4) | 0 | |
| Stage III | 65 (15.3) | 47 (21.5) | 9 (7.2) | 9 (11.5) | 0 | |
| Stage IV | 320 (75.3) | 152 (69.4) | 108 (86.4) | 57 (73.1) | 3 (100.0) | |
| Risk factors of heart diseases (HTN, DM, DLD, etc.) | 0.335 | |||||
| Yes | 232 (54.2) | 115 (52.0) | 72 (57.1) | 42 (53.8) | 3 (100.0) | |
| No | 196 (45.8) | 106 (48.0) | 54 (42.9) | 36 (46.2) | 0 | |
| Heart diseases | 0.002 | |||||
| Yes | 35 (8.2) | 15 (6.8) | 12 (9.5) | 6 (7.7) | 2 (66.7) | |
| No | 393 (91.8) | 206 (93.2) | 114 (90.5) | 72 (92.3) | 1 (33.3) | |
| Heart diseases | 35 (8.2) | 15 (6.8) | 12 (9.5) | 6 (7.7) | 2 (66.7) | |
| a-fib | 2 (5.7) | 1 (6.7) | 1 (8.3) | 0 | 0 | 0.882 |
| IHD | 21 (60) | 7 (46.7) | 8 (66.7) | 4 (66.7) | 2 (100.0) | 0.427 |
| CAD | 3 (8.6) | 2 (13.3) | 1 (8.3) | 0 | 0 | 0.757 |
| CABG | 4 (11.4) | 2 (13.3) | 1 (8.3) | 1 (16.7) | 0 | 0.899 |
| CHF | 5 (14.3) | 3 (20.0) | 1 (8.3) | 1 (16.7) | 0 | 0.775 |
| Other comorbidities | 0.091 | |||||
| Yes | 136 (31.8) | 75 (33.9) | 31 (24.6) | 30 (38.5) | 0 | |
| No | 292 (68.2) | 146 (66.1) | 95 (75.4) | 48 (61.5) | 3 (100.0) | |
| History of hepatitis, n (%) | 0.009 | |||||
| Yes | 36 (8.4) | 24 (10.9) | 2 (1.6) | 10 (12.8) | 0 | |
| No | 392 (91.6) | 197 (89.1) | 124 (98.4) | 68 (87.2) | 3 (100.0) | |
| Previous cancer therapy, n (%) | 0.565 | |||||
| Yes | 316 (73.8) | 165 (74.7) | 94 (74.6) | 54 (69.2) | 3 (100.0) | |
| No | 112 (26.2) | 56 (25.3) | 32 (25.4) | 24 (30.8) | 0 | |
| BMI, kg/m2 [median (IQR)] | 24.45 (7.8) | 24.03 (7.9) | 26.06 (9.6) | 24.48 (5.8) | 24.11 (0.24) | 0.027 |
| BMI, n (%) | 0.014 | |||||
| Underweight | 59 (13.8) | 40 (18.1) | 11 (8.7) | 8 (10.3) | 0 | |
| Healthy weight | 169 (39.5) | 85 (38.5) | 48 (38.1) | 33 (42.3) | 3 (100.0) | |
| Overweight | 111 (25.9) | 60 (27.1) | 28 (22.2) | 23 (29.5) | 2 (40) | |
| Obesity | 89 (20.8) | 36 (16.3) | 39 (31.0) | 14 (17.9) | 0 | |
| Labs [median (IQR)] | ||||||
| LDL (mmol/L) * | 2.93 (1.0) | 3.04 (1.56) | 2.81 (1.27) | 3.04 (1.08) | 2.77 (0.49) | 0.714 |
| HDL (mmol/L) * | 1.0 (0) | 1.04 (0.36) | 0.92 (0.31) | 0.99 (0.23) | 0.9 (0.26) | 0.299 |
| HbA1C% * | 6.55 (3.0) | 6.45 (3.13) | 6.6 (2.7) | 6.6 (2.5) | 7.85 (0.85) | 0.892 |
| ALT (U/L) * | 20.5 (20.8) | 23.0 (20.75) | 19.0 (16) | 22.0 (24) | 10 (3.5) | 0.017 |
| AST (U/L) * | 21 (16.0) | 22.0 (16.75) | 18.0 (8) | 23.0 (26) | 16.0 (2) | <0.001 |
| Bilirubin (Umol/L) * | 8.9 (6.5) | 9.5 (6.9) | 7.77 (5.53) | 10.0 (7.2) | 7.1 (1.05) | 0.003 |
| Scr (Umol/L) * | 70 (23) | 70 (23) | 69 (25) | 71 (17) | 74 (2) | 0.857 |
| CrCl (mL/min) * | 78 (43.5) | 74.5 (41.25) | 85 (47) | 78 (34) | 70 (19.5) | 0.148 |
| Troponin (ng/mL) | 5.4 (11) | 4.65 (8.27) | 9.55 (12.9) | 6.73 (10.58) | 7.85 (0) | 0.341 |
| Complication | All Patients (n = 428) | Nivolumab (n = 221) | Pembrolizumab (n = 126) | Atezolizumab (n = 78) | Durvalumab (n = 3) | p-Value |
|---|---|---|---|---|---|---|
| Respiratory, n (%) | 0.161 | |||||
| Pneumonia | ||||||
| Yes | 43 (10.0) | 23 (10.4) | 8 (6.3) | 11 (14.1) | 1 (33.3) | |
| No | 385 (90.0) | 198 (89.6) | 118 (93.7) | 67 (85.9) | 2 (66.7) | |
| Renal, n (%) | 0.426 | |||||
| Acute kidney injury | ||||||
| Yes | 35 (8.2) | 21 (9.5) | 11 (8.7) | 3 (3.8) | 0 | |
| No | 393 (91.8) | 200 (90.5) | 115 (91.3) | 75 (96.2) | 3 (100.0) | |
| Hepatic, n (%) | <0.001 | |||||
| Hepatitis | ||||||
| Yes | 34 (7.9) | 17 (7.7) | 3 (2.4) | 14 (17.9) | 0 | |
| No | 394 (92.1) | 204 (92.3) | 123 (97.6) | 64 (82.1) | 3 (100.0) | |
| Hematological, n (%) | 0.256 | |||||
| Yes | 23 (5.4) | 9 (4.1) | 11 (8.7) | 3 (3.8) | 0 | |
| No | 405 (94.6) | 212 (95.9) | 115 (91.3) | 75 (96.2) | 3 (100.0) | |
| Hematological, n (%) | 0.940 | |||||
| Neutropenia | ||||||
| Yes | 15 (3.5) | 8 (3.6) | 5 (4.0) | 2 (2.6) | 0 | |
| No | 413 (96.5) | 213 (96.4) | 121 (96.0) | 76 (97.4) | 3 (100.0) | |
| Thrombocytopenia | 0.072 | |||||
| Yes | 11 (2.6) | 2 (0.9) | 7 (5.6) | 2 (2.6) | 0 | |
| No | 417 (97.4) | 219 (99.1) | 119 (94.4) | 76 (97.4) | 3 (100.0) | |
| Thyroid, n (%) | 0.692 | |||||
| Yes | 18 (4.2) | 7 (3.2) | 7 (5.6) | 4 (5.1) | 0 | |
| No | 410 (95.8) | 214 (96.8) | 119 (94.4) | 74 (94.4) | 3 (100.0) | |
| Thyroid, n (%) | 0.722 | |||||
| Hypothyroidism | ||||||
| Yes | 17 (4.0) | 7 (3.2) | 7 (5.6) | 3 (3.8) | 0 | |
| No | 411 (96) | 214 (96.8) | 119 (94.4) | 75 (96.2) | 3 (100.0) | |
| Hyperthyroidism | 0.212 | |||||
| Yes | 1 (0.2) | 0 | 0 | 1 (1.3) | 0 | |
| No | 427 (99.8) | 221 (100.0) | 126 (100.0) | 77 (98.7) | 3 (100.0) | |
| Gastrointestinal complications, n (%) | 0.008 | |||||
| Colitis | ||||||
| Yes | 14 (3.3) | 10 (4.5) | 2 (1.6) | 1 (1.3) | 1 (33.3) | |
| No | 414 (96.7) | 211 (95.5) | 124 (98.4) | 77 (98.7) | 2 (66.7) | |
| Cardiovascular, n (%) | <0.001 | |||||
| Yes | 5 (1.2) | 1 (0.5) | 0 | 3 (3.8) | 1 (33.3) | |
| No | 423 (498.8) | 220 (99.5) | 126 (100.0) | 75 (96.2) | 2 (66.7) | |
| Others, n (%) | 0.039 | |||||
| Yes | 16 (3.7) | 4 (1.8) | 5 (4.0) | 7 (9.0) | 0 | |
| No | 412 (96.3) | 217 (98.2) | 121 (96.0) | 71 (91.0) | 3 (100.0) |
| Side Effect | All Patients (n = 428) | Nivolumab (n = 221) | Pembrolizumab (n = 126) | Atezolizumab (n = 78) | Durvalumab (n = 3) | p-Value |
|---|---|---|---|---|---|---|
| Musculoskeletal, n (%) | 0.663 | |||||
| Fatigue/arthralgia | ||||||
| Yes | 169 (39.5) | 83 (37.6) | 51 (40.5) | 33 (42.3) | 2 (66.7) | |
| No | 259 (60.5) | 138 (62.4) | 75 (59.5) | 45 (57.7) | 1 (33.3) | |
| Musculoskeletal, n (%) | 0.625 | |||||
| Fatigue | ||||||
| Yes | 164 (38.3) | 80 (36.2) | 51 (40.5) | 31 (39.7) | 2 (66.7) | |
| No | 264 (61.7) | 141 (63.8) | 75 (59.5) | 47 (60.3) | 1 (33.3) | |
| Musculoskeletal, n (%) | 0.007 | |||||
| Arthralgia | ||||||
| Yes | 19 (4.4) | 17 (7.7) | 0 | 2 (2.6) | 0 | |
| No | 409 (95.6) | 204 (92.3) | 126 (100.0) | 76 (97.4) | 3 (100.0) | |
| Gastrointestinal, n (%) | 0.144 | |||||
| Nausea/vomiting/diarrhea | ||||||
| Yes | 153 (35.7) | 68 (30.8) | 54 (42.9) | 30 (38.5) | 1 (33.3) | |
| No | 275 (64.3) | 153 (69.2) | 72 (57.1) | 48 (61.5) | 3 (66.7) | |
| Gastrointestinal, n (%) | 0.273 | |||||
| Nausea and vomiting | ||||||
| Yes | 128 (29.9) | 59 (26.7) | 42 (33.3) | 27 (34.6) | 0 | |
| No | 300 (70.1) | 162 (73.3) | 84 (66.7) | 51 (65.4) | 3 (100.0) | |
| Gastrointestinal, n (%) | 0.324 | |||||
| Diarrhea | ||||||
| Yes | 53 (12.4) | 22 (10.0) | 19 (15.1) | 11 (14.1) | 1 (33.3) | |
| No | 375 (87.6) | 199 (90.0) | 107 (84.9) | 67 (85.9) | 2 (66.7) | |
| Dermatological (pruritis–dermatitis–eczema), n (%) | 0.298 | |||||
| Yes | 32 (7.5) | 18 (8.1) | 9 (7.1) | 4 (5.1) | 1 (33.3) | |
| No | 396 (92.5) | 203 (91.1) | 117 (92.9) | 74 (94.9) | 2 (66.7) |
| Characteristics | All Patients (n = 428) | Nivolumab (n = 221) | Pembrolizumab (n = 126) | Atezolizumab (n = 78) | Durvalumab (n = 3) | p-Value |
|---|---|---|---|---|---|---|
| Total complications | 0.162 | |||||
| 0 | 276 (64.5) | 145 (65.6) | 84 (66.7) | 46 (59) | 1 (33.3) | |
| 1 | 122 (28.5) | 62 (28.1) | 38 (30.2) | 21 (26.9) | 1 (33.3) | |
| 2 | 25 (5.8) | 12 (5.4) | 3 (2.4) | 9 (11.5) | 1 (33.3) | |
| 3 | 4 (0.9) | 2 (0.9) | 1 (0.8) | 1 (1.3) | 0 (0.0) | |
| 4 | 1 (0.2) | 0 (0.0) | 0 (0.0) | 1 (1.3) | 0 (0.0) | |
| Total side effects | 0.173 | |||||
| 0 | 176 (41.1) | 100 (45.2) | 47 (37.3) | 29 (37.2) | 0 (0.0) | |
| 1 | 140 (32.7) | 68 (30.8) | 41 (32.5) | 29 (37.2) | 2 (66.7) | |
| 2 | 82 (19.2) | 33 (14.9) | 34 (27.0) | 14 (17.9) | 1 (33.3) | |
| 3 | 28 (6.5) | 18 (8.1) | 4 (3.2) | 6 (7.7) | 0 (0.0) | |
| 4 | 2 (0.5) | 2 (0.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Complication/Side Effect | Average Week Elapsed Until Complication [Median (IQR)] | Weeks Elapsed Since Treatment Initiation Until Adverse Effect Occurrence [Median (IQR)] | p-Value | |||
|---|---|---|---|---|---|---|
| Nivolumab (n = 221) | Pembrolizumab (n = 126) | Atezolizumab (n = 78) | Durvalumab (n = 3) | |||
| Hepatic (hepatitis) | 6.0 (14.0) | 6.0 (12.5) | 10.0 (31.5) | 2.0 (3.5) | NA | 0.084 |
| Cardiovascular | 7.5 (14.0) | NA | NA | 5.0 (8.5) | 10.0 (0.0) | 0.655 |
| Hematological | 8.0 (26.0) | 24.0 (31.0) | 6.0 (9.5) | 30.0 (6.5) | NA | 0.145 |
| Neutropenia | 22.0 (30.0) | 25.0 (35.25) | 7.0 (18.0) | 34.5 (4.5) | NA | 0.174 |
| Thrombocytopenia | 7.0 (24.0) | 4.0 (3.0) | 6.0 (11.0) | 32.5 (6.5) | NA | 0.222 |
| Respiratory (pneumonia) | 8.0 (27.0) | 10.0 (35.0) | 11.0 (38.0) | 4.0 (5.0) | 8.0 (0.0) | 0.182 |
| Renal (AKI) | 10.0 (15.0) | 10.0 (9.0) | 2.0 (3.0) | 26.0 (10.5) | NA | 0.062 |
| Gastrointestinal complications (colitis) | 10.0 (22.0) | 8.5 (18.5) | 6.0 (38.0) | 16.0 (0.0) | 27.0 (0.0) | 0.631 |
| Thyroid | 10.5 (22.0) | 8.0 (11.5) | 23.0 (7.0) | 6.0 (14.5) | NA | 0.218 |
| Hypothyroidism | 12 (19) | 8.0 (11.5) | 23.0 (7.0) | 9.0 (20) | NA | 0.385 |
| Skin reaction | 12.0 (21.25) | 11.5 (19.0) | 10 (42) | 18.5 (65) | NA | 0.414 |
| Complication/Side Effect | Patients’ Factors | Coef (B) | S.E | Odds Ratio | 95% CI | p-Value | |
|---|---|---|---|---|---|---|---|
| Hepatic complication | Gender | Male | Ref | ||||
| Female | 0.996 | 0.473 | 2.71 | 1.07–6.85 | 0.035 | ||
| History of hepatitis | No | Ref | |||||
| Yes | 2.41 | 0.597 | 11.14 | 3.46–35.88 | <0.001 | ||
| Respiratory complication | Previous cancer therapy | No | Ref | ||||
| Yes | 1.125 | 0.515 | 3.08 | 1.12–8.85 | 0.029 | ||
| Hematological complication | Type of malignancy | Solid | Ref | ||||
| Liquid | 2.84 | 0.736 | 17.18 | 4.06–72.71 | <0.001 | ||
| Neutropenia | Type of malignancy | Solid | |||||
| Liquid | 1.79 | 0.816 | 6.01 | 1.21–29.75 | 0.028 | ||
| Thrombocytopenia | Type of malignancy | Solid | |||||
| Liquid | 3.28 | 1.08 | 26.5 | 3.22–218.38 | 0.002 | ||
| Musculoskeletal | Gender | Male | |||||
| Female | 0.419 | 0.21 | 1.52 | 1.01–2.29 | 0.046 | ||
| Arthralgia | Previous cancer therapy | No | Ref | ||||
| Yes | −1.07 | 0.531 | 0.344 | 0.121–0.974 | 0.045 | ||
| Fatigue | Gender | Male | Ref | ||||
| Female | 0.503 | 0.212 | 1.65 | 1.09–2.51 | 0.018 | ||
| Nausea and vomiting | Gender | Male | Ref | ||||
| Female | 0.731 | 0.222 | 2.08 | 1.34–3.21 | 0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alwhaibi, A.; Alenazi, M.A.; Alghadeer, S.; Mansy, W.; Alsaif, R.A.; Abualreesh, N.E.; Alanazi, R.J.; Alroumi, A.; Alanazi, S.A. A Real-World Comparison of the Safety Profile for Immune Checkpoint Inhibitors in Oncology Patients. J. Clin. Med. 2025, 14, 388. https://doi.org/10.3390/jcm14020388
Alwhaibi A, Alenazi MA, Alghadeer S, Mansy W, Alsaif RA, Abualreesh NE, Alanazi RJ, Alroumi A, Alanazi SA. A Real-World Comparison of the Safety Profile for Immune Checkpoint Inhibitors in Oncology Patients. Journal of Clinical Medicine. 2025; 14(2):388. https://doi.org/10.3390/jcm14020388
Chicago/Turabian StyleAlwhaibi, Abdulrahman, Miteb A. Alenazi, Sultan Alghadeer, Wael Mansy, Reem A. Alsaif, Nawaf E. Abualreesh, Rakan J. Alanazi, Abdullah Alroumi, and Saleh A. Alanazi. 2025. "A Real-World Comparison of the Safety Profile for Immune Checkpoint Inhibitors in Oncology Patients" Journal of Clinical Medicine 14, no. 2: 388. https://doi.org/10.3390/jcm14020388
APA StyleAlwhaibi, A., Alenazi, M. A., Alghadeer, S., Mansy, W., Alsaif, R. A., Abualreesh, N. E., Alanazi, R. J., Alroumi, A., & Alanazi, S. A. (2025). A Real-World Comparison of the Safety Profile for Immune Checkpoint Inhibitors in Oncology Patients. Journal of Clinical Medicine, 14(2), 388. https://doi.org/10.3390/jcm14020388