
How Much Variance Exists Among Published Definitions of Proximal Junctional Kyphosis? A Retrospective Cohort Study of Adult Spinal Deformity

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Limitations and Future Steps
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASD | Adult Spinal Deformity |
| PJK | Proximal Junctional Kyphosis |
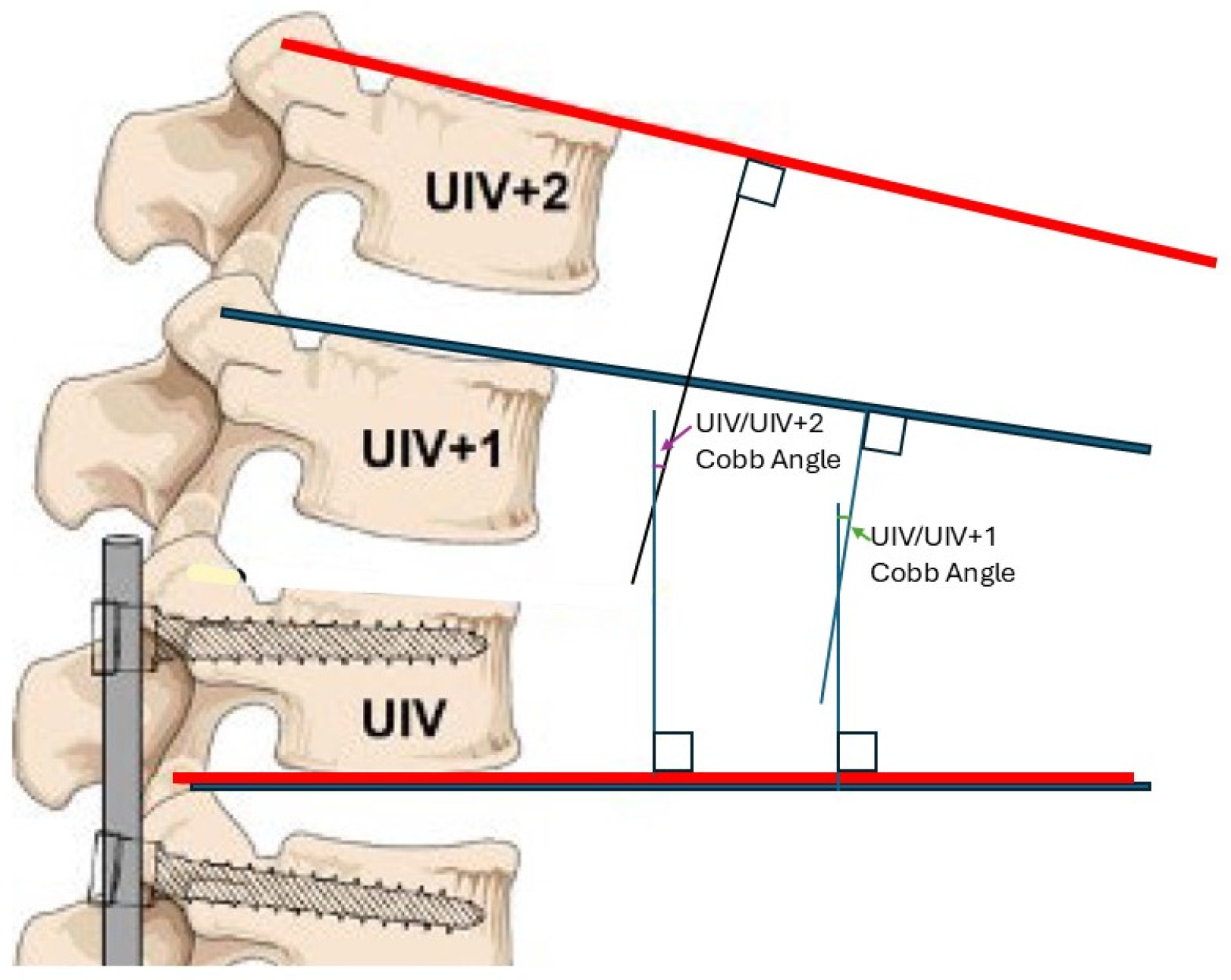
| UIV | Upper Instrumented Vertebra |
| SAV | Supra-adjacent Vertebra |
| EMR | Electronic Medical Record |
| BMI | Body Mass Index |
| SD | Standard Deviation |
| CI | Confidence Interval |
References
- Kim, H.J.; Iyer, S. Proximal Junctional Kyphosis. JAAOS-J. Am. Acad. Orthop. Surg. 2016, 24, 318–326. [Google Scholar] [CrossRef]
- Diebo, B.G.; Shah, N.V.; Boachie-Adjei, O.; Zhu, F.; Rothenfluh, D.A.; Paulino, C.B.; Schwab, F.J.; Lafage, V. Adult spinal deformity. Lancet 2019, 394, 160–172. [Google Scholar] [CrossRef]
- Bridwell, K.H.; Lenke, L.G.; Cho, S.K.; Pahys, J.M.; Zebala, L.P.; Dorward, I.G.; Cho, W.; Baldus, C.; Hill, B.W.; Kang, M.M. Proximal junctional kyphosis in primary adult deformity surgery: Evaluation of 20 degrees as a critical angle. Neurosurgery 2013, 72, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Sardar, Z.M.; Kim, Y.; Lafage, V.; Rand, F.; Lenke, L.; Klineberg, E. State of the art: Proximal junctional kyphosis-diagnosis, management and prevention. Spine Deform. 2021, 9, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Glattes, R.C.; Bridwell, K.H.; Lenke, L.G.; Kim, Y.J.; Rinella, A.; Edwards, C., 2nd. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: Incidence, outcomes, and risk factor analysis. Spine 2005, 30, 1643–1649. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lenke, L.G.; Shaffrey, C.I.; Van Alstyne, E.M.; Skelly, A.C. Proximal junctional kyphosis as a distinct form of adjacent segment pathology after spinal deformity surgery: A systematic review. Spine 2012, 37 (Suppl. S22), S144–S164. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, J.U.; Jang, J.S.; Lee, S.H. Analysis of the incidence and risk factors for the progression of proximal junctional kyphosis following surgical treatment for lumbar degenerative kyphosis: Minimum 2-year follow-up. Br. J. Neurosurg. 2014, 28, 252–258. [Google Scholar] [CrossRef]
- Yagi, M.; King, A.B.; Boachie-Adjei, O. Incidence, risk factors, and natural course of proximal junctional kyphosis: Surgical outcomes review of adult idiopathic scoliosis. Minimum 5 years of follow-up. Spine 2012, 37, 1479–1489. [Google Scholar] [CrossRef]
- Helgeson, M.D.; Shah, S.A.; Newton, P.O.; Clements, D.H., III; Betz, R.R.; Marks, M.C.; Bastrom, T. Evaluation of proximal junctional kyphosis in adolescent idiopathic scoliosis following pedicle screw, hook, or hybrid instrumentation. Spine 2010, 35, 177–181. [Google Scholar] [CrossRef]
- Lonner, B.S.; Newton, P.; Betz, R.; Scharf, C.; O’Brien, M.; Sponseller, P.; Lenke, L.; Crawford, A.; Lowe, T.; Letko, L.; et al. Operative management of Scheuermann’s kyphosis in 78 patients: Radiographic outcomes, complications, and technique. Spine 2007, 32, 2644–2652. [Google Scholar] [CrossRef]
- Hassanzadeh, H.; Gupta, S.; Jain, A.; El Dafrawy, M.H.; Skolasky, R.L.; Kebaish, K.M. Type of Anchor at the Proximal Fusion Level Has a Significant Effect on the Incidence of Proximal Junctional Kyphosis and Outcome in Adults After Long Posterior Spinal Fusion. Spine Deform. 2013, 1, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Bridwell, K.H.; Lenke, L.G.; Park, M.S.; Ahmad, A.; Song, K.-S.; Piyaskulkaew, C.; Hershman, S.; Fogelson, J.; Mesfin, A. Proximal junctional kyphosis results in inferior SRS pain subscores in adult deformity patients. Spine 2013, 38, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Bridwell, K.H.; Lenke, L.G.; Park, M.S.; Song, K.S.; Piyaskulkaew, C.; Chuntarapas, T. Patients with proximal junctional kyphosis requiring revision surgery have higher postoperative lumbar lordosis and larger sagittal balance corrections. Spine 2014, 39, E576–E580. [Google Scholar] [CrossRef] [PubMed]
- Boeckenfoerde, K.; Schulze Boevingloh, A.; Gosheger, G.; Bockholt, S.; Lampe, L.P.; Lange, T. Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis-The Spinous Processes and Proximal Rod Contouring. J. Clin. Med. 2022, 11, 6098. [Google Scholar] [CrossRef]
- Hyun, S.J.; Lee, B.H.; Park, J.H.; Kim, K.J.; Jahng, T.A.; Kim, H.J. Proximal Junctional Kyphosis and Proximal Junctional Failure Following Adult Spinal Deformity Surgery. Korean J. Spine 2017, 14, 126–132. [Google Scholar] [CrossRef]
- Hills, J.; Mundis, G.M.; Klineberg, E.O.; Smith, J.S.; Line, B.; Gum, J.L.; Protopsaltis, T.S.; Hamilton, D.K.; Soroceanu, A.; Eastlack, R.; et al. The T4-L1-Hip Axis: Sagittal Spinal Realignment Targets in Long-Construct Adult Spinal Deformity Surgery: Early Impact. J. Bone Jt. Surg. Am. 2024, 106, e48. [Google Scholar] [CrossRef]
- Petrosyan, E.; Fares, J.; Ahuja, C.S.; Lesniak, M.S.; Koski, T.R.; Dahdaleh, N.S.; El Tecle, N.E. Genetics and pathogenesis of scoliosis. N. Am. Spine Soc. J. 2024, 20, 100556. [Google Scholar] [CrossRef]
- Lafage, R.; Beyer, G.; Schwab, F.; Klineberg, E.; Burton, D.; Bess, S.; Kim, H.J.; Smith, J.; Ames, C.; Hostin, R.; et al. Risk Factor Analysis for Proximal Junctional Kyphosis After Adult Spinal Deformity Surgery: A New Simple Scoring System to Identify High-Risk Patients. Glob. Spine J. 2020, 10, 863–870. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Glattes, C.R.; Rhim, S.; Cheh, G. Proximal junctional kyphosis in adult spinal deformity after segmental posterior spinal instrumentation and fusion: Minimum five-year follow-up. Spine 2008, 33, 2179–2184. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Rhim, S.; Cheh, G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: Causes, prevalence, and risk factor analysis. Spine 2006, 31, 2359–2366. [Google Scholar] [CrossRef]
- O’Leary, P.T.; Bridwell, K.H.; Lenke, L.G.; Good, C.R.; Pichelmann, M.A.; Buchowski, J.M.; Kim, Y.J.; Flynn, J.B. Risk factors and outcomes for catastrophic failures at the top of long pedicle screw constructs: A matched cohort analysis performed at a single center. Spine 2009, 34, 2134–2139. [Google Scholar] [CrossRef]
- Naresh-Babu, J.; Kwan, K.Y.H.; Wu, Y.; Yilgor, C.; Alanay, A.; Cheung, K.M.C.; Polly, D.W.; Park, J.-B.; Ito, M.; Lenke, L.G.; et al. AO Spine Adult Spinal Deformity Patient Profile: A Paradigm Shift in Comprehensive Patient Evaluation in Order to Optimize Treatment and Improve Patient Care. Glob. Spine J. 2023, 13, 1490–1501. [Google Scholar] [CrossRef] [PubMed]
- Bess, S.; Boachie-Adjei, O.; Burton, D.; Cunningham, M.; Shaffrey, C.; Shelokov, A.; Hostin, R.; Schwab, F.; Wood, K.; Akbarnia, B. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine 2009, 34, 2186–2190. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Category | Frequency (%) or Mean (SD) |
|---|---|---|
| Sample Size | 116 | |
| Sex | Female | 79 (68.1%) |
| Male | 37 (31.9%) | |
| Race | White | 108 (93.1%) |
| Black | 7 (6.0%) | |
| Other | 1 (0.9%) | |
| Age (years) | - | 70.9 (4.3) |
| BMI | - | 28.9 (5.4) |
| Smoking History | Never Smoked | 68 (58.6%) |
| Smoked | 48 (41.4%) | |
| Average Follow-Up (days) | - | 865.9 (592.9) |
| Reoperations/Revisions | Yes | 27 (28.4%) |
| No | 89 (83.6%) | |
| Fusion Length | Short (UIV ≤ T10) | 49 (42.2%) |
| Long (UIV > T10) | 67 (57.8%) | |
| Final UIV/UIV+1 angle (°) | - | 9.04 (7.04) |
| Final UIV/UIV+2 angle (°) * | - | 13.40 (8.07) |
| Δ UIV/UIV+1 angle (°) | - | 5.15 (9.09) |
| Δ UIV/UIV+2 angle (°) * | - | 7.82 (11.31) |
| Number | Abbreviated Name | PJK Definition | Source DOI | Rate of PJK (%) | 95% CI |
|---|---|---|---|---|---|
| (1) | PJK20 | Final UIV/UIV+2 ≥ 20° | Bridwell et al., 2013 [3] | 20.7 | 13.8–29.7% |
| (2) | PJK10 | Final UIV/UIV+2 ≥ 10° and ΔUIV/UIV+2 > 10° | Glattes et al., 2005 [5] | 36.9 | 28.1–46.7% |
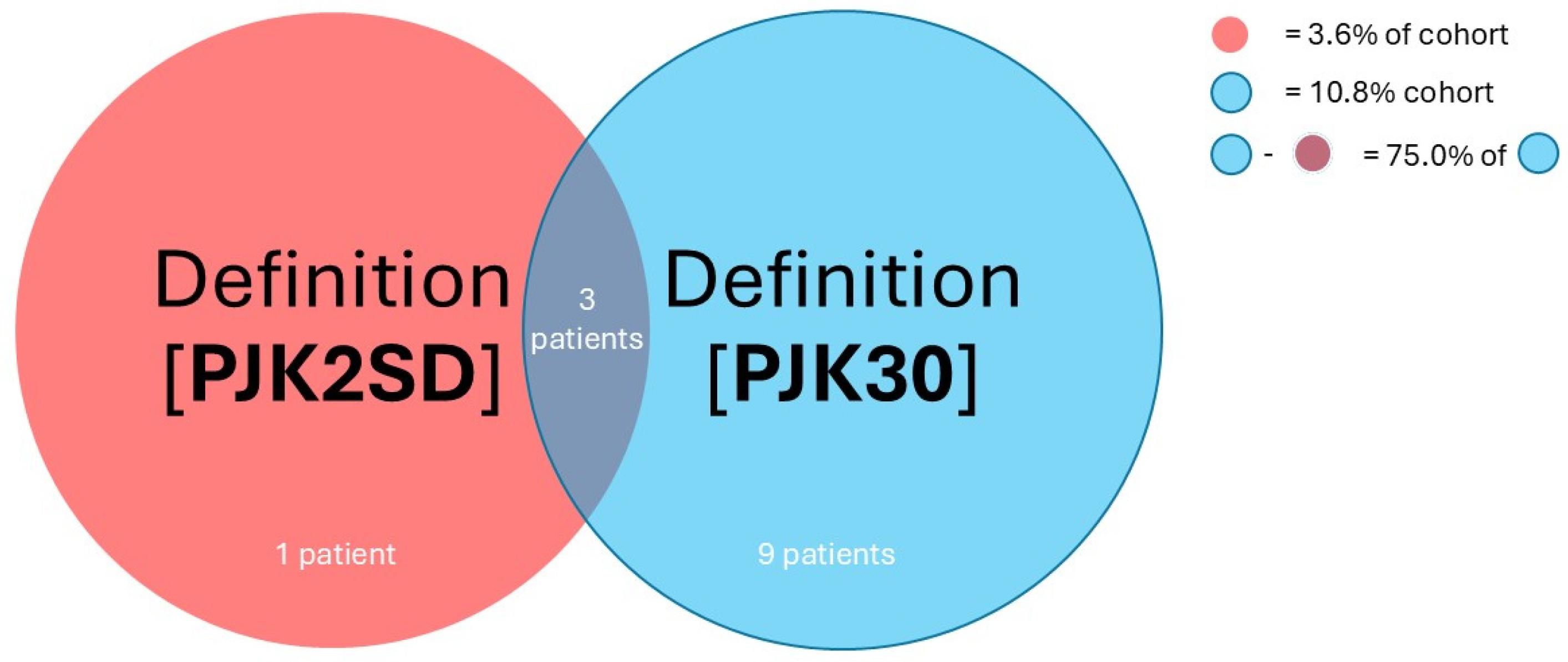
| (3) | PJK2SD | Final UIV/UIV+1 > 2 SD of average Final UIV/UIV+1 | Helgeson et al., 2010 [9] | 3.6 | 1.2–9.5% |
| (4) | PJK10+10 | Final UIV/UIV+1 ≥ 10° and ΔUIV/UIV+1 > 10° | Lonner et al., 2007 [10] | 23.4 | 16.1–32.6% |
| (5) | PJK15 | Final UIV/UIV+1 > 15° | Hyun et al., 2017 [15] | 15.3 | 9.4–23.7% |
| (6) | PJK30 | Final UIV/UIV+2 > 30° or displaced rod fracture or reoperation within 2 years for junctional failure, pseudoarthrosis, or rod fracture | Hills et al., 2024 [16] | 10.8 | 6.0–18.5% |
| PJK Definitions | PJK Definitions: Pairwise Difference (95% CI) * | ||||||
| PJK20 | PJK10 | PJK2SD | PJK10+10 | PJK15 | PJK30 | ||
| PJK20 | - | 0.16 (0.045–0.28) | 0.17 (0.088–0.25) | 0.027 (−0.082 to 0.14) | 0.054 (−0.047 to 0.15) | 0.099 (4.1 × 10−3–0.19) | |
| PJK10 | - | - | 0.33 (0.24–0.43) | 0.14 (0.016–0.25) | 0.22 (0.10–0.33) | 0.26 (0.15–0.37) | |
| PJK2SD | - | - | - | 0.20 (0.11–0.28) | 0.12 (0.042–0.19) | 0.072 (4.7 × 10−3–0.14) | |
| PJK10+10 | - | - | - | - | 0.081 (−0.022 to 0.18) | 0.13 (0.028–0.22) | |
| PJK15 | - | - | - | - | - | 0.045 (−0.043 to 0.13) | |
| PJK30 | - | - | - | - | - | - | |
| PJK Definitions | PJK Definitions: p-Value with Holm Correction | ||||||
| PJK20 | PJK10 | PJK2SD | PJK10+10 | PJK15 | PJK30 | ||
| PJK20 | - | 0.106 | 2.63 × 10−3 | 1.00 | 1.00 | 0.393 | |
| PJK10 | - | - | 2.80 × 10−8 | 0.285 | 4.9 × 10−3 | 1.50 × 10−4 | |
| PJK2SD | - | - | - | 4.90 × 10−4 | 0.0592 | 0.393 | |
| PJK10+10 | - | - | - | - | 0.697 | 0.164 | |
| PJK15 | - | - | - | - | - | 1.00 | |
| PJK30 | - | - | - | - | - | - | |
| PJK Definitions | PJK Definitions: Percent Agreement (95% CI) | ||||||
| PJK20 | PJK10 | PJK2SD | PJK10+10 | PJK15 | PJK30 | ||
| PJK20 | 100% | 78.4% (69.4–85.4%) | 82.9% (74.3–89.1%) | 77.5% (68.4–84.6%) | 85.6% (77.3–91.3%) | 72.1% (62.6–80.0%) | |
| PJK10 | - | 100% | 66.7% (57.0–75.2%) | 77.5% (68.4–84.6%) | 76.6% (67.4–83.9%) | 61.3% (51.5–70.2%) | |
| PJK2SD | - | - | 100% | 80.2% (71.3–86.9%) | 88.3% (80.5–93.4%) | 89.2% (81.5–94.0%) | |
| PJK10+10 | - | - | - | 100% | 90.1% (82.6–94.7%) | 73.0% (63.6–80.8%) | |
| PJK15 | - | - | - | - | 100% | 79.3% (70.3–86.2%) | |
| PJK30 | - | - | - | - | - | 100% | |
| Reoperation | 69.3% (59.8–77.6%) | 60.4% (50.6–69.4%) | 79.3% (70.3–86.2%) | 64.9% (55.2–73.5%) | 71.2% (61.7–79.2%) | 82.9% (74.3–89.1%) | |
| Percentage of Additional PJK Definitions Met (%) | ||||||
|---|---|---|---|---|---|---|
| Definition | 1 | 2 | 3 | 4 | 5 | Mean (Across Rows) |
| PJK20 | 91.3 | 56.5 | 43.5 | 17.4 | 8.70 | 43.5 |
| PJK10 | 78.0 | 41.5 | 26.8 | 9.76 | 4.88 | 32.2 |
| PJK2SD | 100 | 100 | 100 | 100 | 50 | 90 |
| PJK10+10 | 88.5 | 65.4 | 42.3 | 15.4 | 7.69 | 43.9 |
| PJK15 | 100 | 76.5 | 64.7 | 23.5 | 11.8 | 55.3 |
| PJK30 | 29.4 | 11.8 | 11.8 | 11.8 | 11.8 | 15.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bui, T.T.; Joseph, K.; Yahanda, A.T.; Vogl, S.; Ruiz-Cardozo, M.; Molina, C.A. How Much Variance Exists Among Published Definitions of Proximal Junctional Kyphosis? A Retrospective Cohort Study of Adult Spinal Deformity. J. Clin. Med. 2025, 14, 5469. https://doi.org/10.3390/jcm14155469
Bui TT, Joseph K, Yahanda AT, Vogl S, Ruiz-Cardozo M, Molina CA. How Much Variance Exists Among Published Definitions of Proximal Junctional Kyphosis? A Retrospective Cohort Study of Adult Spinal Deformity. Journal of Clinical Medicine. 2025; 14(15):5469. https://doi.org/10.3390/jcm14155469
Chicago/Turabian StyleBui, Tim T., Karan Joseph, Alexander T. Yahanda, Samuel Vogl, Miguel Ruiz-Cardozo, and Camilo A. Molina. 2025. "How Much Variance Exists Among Published Definitions of Proximal Junctional Kyphosis? A Retrospective Cohort Study of Adult Spinal Deformity" Journal of Clinical Medicine 14, no. 15: 5469. https://doi.org/10.3390/jcm14155469
APA StyleBui, T. T., Joseph, K., Yahanda, A. T., Vogl, S., Ruiz-Cardozo, M., & Molina, C. A. (2025). How Much Variance Exists Among Published Definitions of Proximal Junctional Kyphosis? A Retrospective Cohort Study of Adult Spinal Deformity. Journal of Clinical Medicine, 14(15), 5469. https://doi.org/10.3390/jcm14155469