
Once-Weekly Semaglutide Improves Body Composition in Spanish Obese Adults with Type 2 Diabetes: A 48-Week Prospective Real-Life Study



Abstract
1. Introduction
2. Materials and Methods
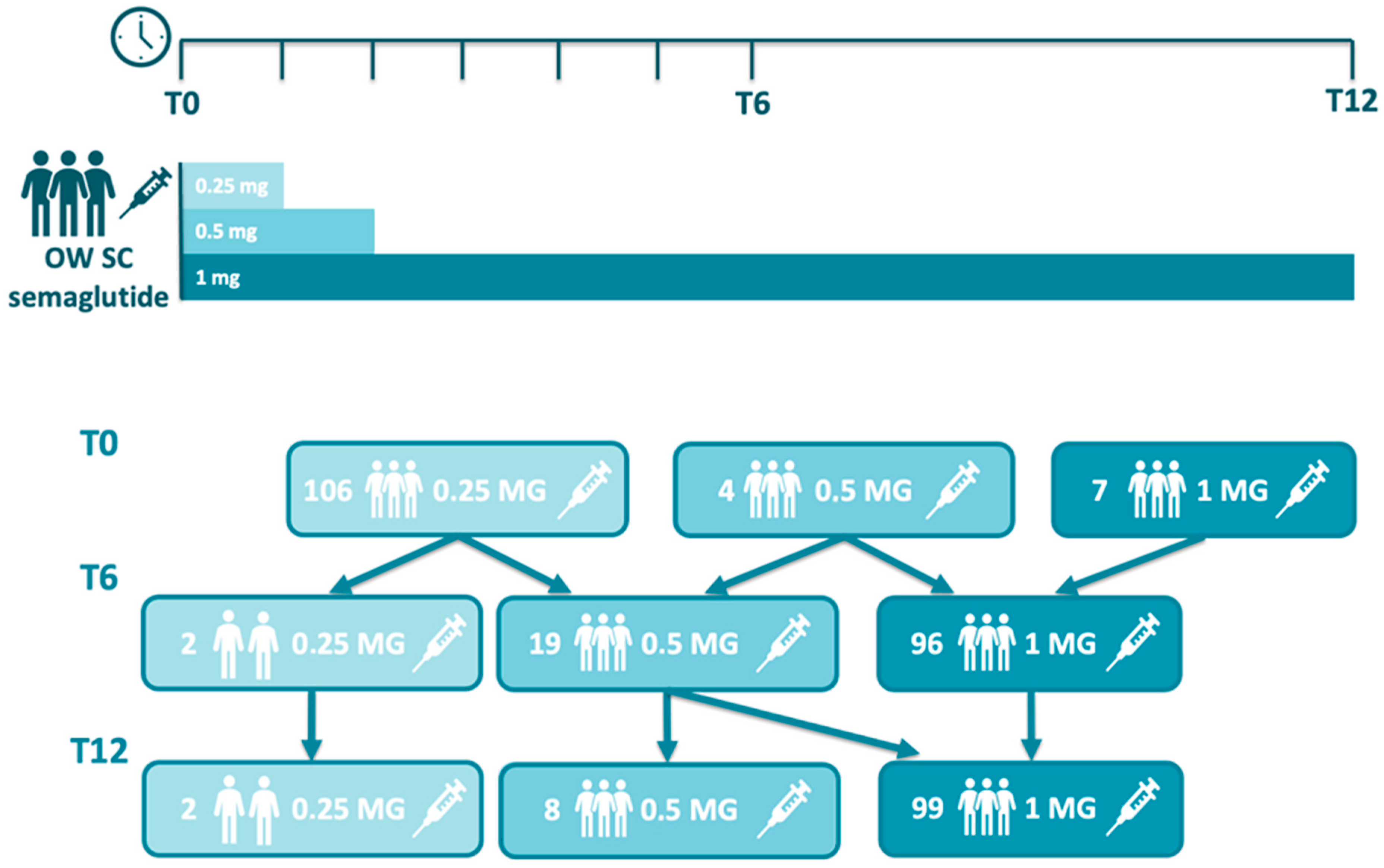
2.1. Design
2.2. Aims and Research Questions
2.3. Study Endpoints and Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Changes in Body Composition Parameters
3.3. Other Clinical Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| T2D | Type 2 diabetes |
| HbA1c | Glycated hemoglobin |
| BW | Body weight |
| GLP-1 RAs | Glucagon-like peptide-1 receptor agonists |
| SGLT | Sodium-glucose linked transporter |
| SMF-BIA | Segmental multifrequency bioelectrical impedance analysis |
| BMI | Body mass index |
| FM | Fat mass |
| FMI | Fat mass index |
| VAT | Visceral adipose tissue |
| FFM | Fat-free mass |
| FFMI | Fat-free mass index |
| SMM | Skeletal muscle mass |
| EW | Extracellular water |
| TBW | Total body water |
| PhA | Phase angle |
References
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Ruze, R.; Liu, T.; Zou, X.; Song, J.; Chen, Y.; Xu, R.; Yin, X.; Xu, Q. Obesity and type 2 diabetes mellitus: Connections in epidemiology, pathogenesis, and treatments. Front. Endocrinol. 2023, 14, 1161521. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, P.; Weiskirchen, R. The Role of Obesity in Type 2 Diabetes Mellitus-An Overview. Int. J. Mol. Sci. 2024, 25, 1882. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.; Gastaldelli, A.; Yki-Järvinen, H.; Scherer, P.E. Why does obesity cause diabetes? Cell Metab. 2022, 34, 11–20. [Google Scholar] [CrossRef]
- Brown, O.I.; Drozd, M.; McGowan, H.; Giannoudi, M.; Conning-Rowland, M.; Gierula, J.; Straw, S.; Wheatcroft, S.B.; Bridge, K.; Roberts, L.D.; et al. Relationship Among Diabetes, Obesity, and Cardiovascular Disease Phenotypes: A UK Biobank Cohort Study. Diabetes Care 2023, 46, 1531–1540. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef]
- Marx, N.; Federici, M.; Schütt, K.; Müller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; Di Angelantonio, E.; Eliasson, B.; et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur. Heart J. 2023, 44, 4043–4140. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 1. Improving Care and Promoting Health in Populations: Standards of Care in Diabetes—2025. Diabetes Care 2025, 48, S14–S26. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 8. Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standards of Care in Diabetes—2025. Diabetes Care 2025, 48, S167–S180. [Google Scholar] [CrossRef] [PubMed]
- Nadkarni, P.; Chepurny, O.G.; Holz, G.G. Regulation of glucose homeostasis by GLP-1. Prog. Mol. Biol. Transl. Sci. 2014, 121, 23–65. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A.; Quast, D.R.; Wefers, J.; Meier, J.J. GLP-1 receptor agonists in the treatment of type 2 diabetes-state-of-the-art. Mol. Metab. 2021, 46, 101102. [Google Scholar] [CrossRef]
- Caruso, I.; Cignarelli, A.; Sorice, G.P.; Natalicchio, A.; Perrini, S.; Laviola, L.; Giorgino, F. Cardiovascular and Renal Effectiveness of GLP-1 Receptor Agonists vs. Other Glucose-Lowering Drugs in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Real-World Studies. Metabolites 2022, 12, 183. [Google Scholar] [CrossRef]
- Li, Y.; Rosenblit, P.D. Glucagon-Like Peptide-1 Receptor Agonists and Cardiovascular Risk Reduction in Type 2 Diabetes Mellitus: Is It a Class Effect? Curr. Cardiol. Rep. 2018, 20, 113. [Google Scholar] [CrossRef]
- Näslund, E.; Bogefors, J.; Skogar, S.; Grybäck, P.; Jacobsson, H.; Holst, J.J.; Hellström, P.M. GLP-1 slows solid gastric emptying and inhibits insulin, glucagon, and PYY release in humans. Am. J. Physiol. 1999, 277, R910–R916. [Google Scholar] [CrossRef] [PubMed]
- Aroda, V.R.; Ahmann, A.; Cariou, B.; Chow, F.; Davies, M.J.; Jódar, E.; Mehta, R.; Woo, V.; Lingvay, I. Comparative efficacy, safety, and cardiovascular outcomes with once-weekly subcutaneous semaglutide in the treatment of type 2 diabetes: Insights from the SUSTAIN 1-7 trials. Diabetes Metab. 2019, 45, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Bucheit, J.D.; Pamulapati, L.G.; Carter, N.; Malloy, K.; Dixon, D.L.; Sisson, E.M. Oral Semaglutide: A Review of the First Oral Glucagon-Like Peptide 1 Receptor Agonist. Diabetes Technol. Ther. 2020, 22, 10–18. [Google Scholar] [CrossRef]
- Chudleigh, R.A.; Bain, S.C. Semaglutide injection for the treatment of adults with type 2 diabetes. Expert Rev. Clin. Pharmacol. 2020, 13, 675–684. [Google Scholar] [CrossRef]
- Garvey, W.T.; Birkenfeld, A.L.; Dicker, D.; Mingrone, G.; Pedersen, S.D.; Satylganova, A.; Skovgaard, D.; Sugimoto, D.; Jensen, C.; Mosenzon, O. Efficacy and Safety of Liraglutide 3.0 mg in Individuals With Overweight or Obesity and Type 2 Diabetes Treated With Basal Insulin: The SCALE Insulin Randomized Controlled Trial. Diabetes Care 2020, 43, 1085–1093. [Google Scholar] [CrossRef]
- Chen, S.; Wang, X.; Jin, Y.; Chen, X.; Song, Q.; Wei, G.; Li, L. Assessment of Changes in Body Composition After 3 Months of Dulaglutide Treatment. Diabetes Metab. Syndr. Obes. 2024, 17, 1301–1308. [Google Scholar] [CrossRef]
- Chanoine, J.P.; Hampl, S.; Jensen, C.; Boldrin, M.; Hauptman, J. Effect of orlistat on weight and body composition in obese adolescents: A randomized controlled trial. JAMA 2005, 293, 2873–2883. [Google Scholar] [CrossRef] [PubMed]
- Bolinder, J.; Ljunggren, Ö.; Johansson, L.; Wilding, J.; Langkilde, A.M.; Sjöström, C.D.; Sugg, J.; Parikh, S. Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin. Diabetes Obes. Metab. 2014, 16, 159–169. [Google Scholar] [CrossRef]
- Borga, M.; West, J.; Bell, J.D.; Harvey, N.C.; Romu, T.; Heymsfield, S.B.; Dahlqvist Leinhard, O. Advanced body composition assessment: From body mass index to body composition profiling. J. Investig. Med. 2018, 66, 1–9. [Google Scholar] [CrossRef]
- Sweatt, K.; Garvey, W.T.; Martins, C. Strengths and Limitations of BMI in the Diagnosis of Obesity: What is the Path Forward? Curr. Obes. Rep. 2024, 13, 584–595. [Google Scholar] [CrossRef]
- Wu, Y.; Li, D.; Vermund, S.H. Advantages and Limitations of the Body Mass Index (BMI) to Assess Adult Obesity. Int. J. Environ. Res. Public Health 2024, 21, 757. [Google Scholar] [CrossRef]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Merz, K.E.; Thurmond, D.C. Role of Skeletal Muscle in Insulin Resistance and Glucose Uptake. Compr. Physiol. 2020, 10, 785–809. [Google Scholar] [CrossRef]
- Izzo, A.; Massimino, E.; Riccardi, G.; Della Pepa, G. A Narrative Review on Sarcopenia in Type 2 Diabetes Mellitus: Prevalence and Associated Factors. Nutrients 2021, 13, 183. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Guo, Y.; Zheng, C. Type 2 diabetes mellitus related sarcopenia: A type of muscle loss distinct from sarcopenia and disuse muscle atrophy. Front. Endocrinol. 2024, 15, 1375610. [Google Scholar] [CrossRef]
- Salom Vendrell, C.; García Tercero, E.; Moro Hernández, J.B.; Cedeno-Veloz, B.A. Sarcopenia as a Little-Recognized Comorbidity of Type II Diabetes Mellitus: A Review of the Diagnosis and Treatment. Nutrients 2023, 15, 4149. [Google Scholar] [CrossRef]
- Ma, X.Y.; Chen, F.Q. Effects of anti-diabetic drugs on sarcopenia: Best treatment options for elderly patients with type 2 diabetes mellitus and sarcopenia. World J. Clin. Cases 2021, 9, 10064–10074. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, Y.; Chen, S.; Shao, H. Anti-diabetic drugs and sarcopenia: Emerging links, mechanistic insights, and clinical implications. J. Cachexia Sarcopenia Muscle 2021, 12, 1368–1379. [Google Scholar] [CrossRef]
- McCrimmon, R.J.; Catarig, A.M.; Frias, J.P.; Lausvig, N.L.; le Roux, C.W.; Thielke, D.; Lingvay, I. Effects of once-weekly semaglutide vs once-daily canagliflozin on body composition in type 2 diabetes: A substudy of the SUSTAIN 8 randomised controlled clinical trial. Diabetologia 2020, 63, 473–485. [Google Scholar] [CrossRef]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.D.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Ozeki, Y.; Masaki, T.; Kamata, A.; Miyamoto, S.; Yoshida, Y.; Okamoto, M.; Gotoh, K.; Shibata, H. The Effectiveness of GLP-1 Receptor Agonist Semaglutide on Body Composition in Elderly Obese Diabetic Patients: A Pilot Study. Medicines 2022, 9, 47. [Google Scholar] [CrossRef] [PubMed]
- Pantanetti, P.; Cangelosi, G.; Alberti, S.; Di Marco, S.; Michetti, G.; Cerasoli, G.; Di Giacinti, M.; Coacci, S.; Francucci, N.; Petrelli, F.; et al. Changes in body weight and composition, metabolic parameters, and quality of life in patients with type 2 diabetes treated with subcutaneous semaglutide in real-world clinical practice. Front. Endocrinol. 2024, 15, 1394506. [Google Scholar] [CrossRef]
- Rodríguez Jiménez, B.; Rodríguez de Vera Gómez, P.; Belmonte Lomas, S.; Díaz, Á.M.M.; Caballero Mateos, I.; Galán, I.; Morales Portillo, C.; Martínez-Brocca, M.A. Transforming body composition with semaglutide in adults with obesity and type 2 diabetes mellitus. Front. Endocrinol. 2024, 15, 1386542. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, S.; Sada, Y.; Mihara, S.; Sasaki, Y.; Sone, M.; Tanaka, Y. Oral Semaglutide Induces Loss of Body Fat Mass Without Affecting Muscle Mass in Patients With Type 2 Diabetes. J. Clin. Med. Res. 2023, 15, 377–383. [Google Scholar] [CrossRef]
- Volpe, S.; Lisco, G.; Fanelli, M.; Racaniello, D.; Colaianni, V.; Lavarra, V.; Triggiani, D.; Crudele, L.; Triggiani, V.; Sabbà, C.; et al. Oral semaglutide improves body composition and preserves lean mass in patients with type 2 diabetes: A 26-week prospective real-life study. Front. Endocrinol. 2023, 14, 1240263. [Google Scholar] [CrossRef]
- Volpe, S.; Lisco, G.; Racaniello, D.; Fanelli, M.; Colaianni, V.; Vozza, A.; Triggiani, V.; Sabbà, C.; Tortorella, C.; De Pergola, G.; et al. Once-Weekly Semaglutide Induces an Early Improvement in Body Composition in Patients with Type 2 Diabetes: A 26-Week Prospective Real-Life Study. Nutrients 2022, 14, 2414. [Google Scholar] [CrossRef]
- Caballero Mateos, I.; García de Lucas, M.D.; Doulatram-Gamgaram, V.K.; Moreno-Moreno, P.; Jimenez-Millan, A.I.; Botana-López, M.; Merino-Torres, J.F.; Soto-Gónzalez, A.; Fernández-García, J.C.; Morales-Portillo, C. Real-World Evaluation of Once-Weekly Subcutaneous Semaglutide in Patients with Type 2 Diabetes Mellitus in Spain (SEMA-RW Study). Nutrients 2024, 16, 2545. [Google Scholar] [CrossRef]
- Castillo Castro, C.; González Arellanes, R.; Camacho Mondragón, C.G.; Farfán Esponda, H.R.; Del Razo Olvera, F.M.; Aguilar Salinas, C.A.; Martagon, A.J. Agreement Between Bioelectrical Impedance Analysis and Dual-Energy X-ray Absorptiometry to Estimate Fat Mass in Hispanic Adults With Type 2 Diabetes Mellitus: A Cross-Sectional Study. Clin. Med. Insights Endocrinol. Diabetes 2024, 17, 1–6. [Google Scholar] [CrossRef]
- Lin, C.L.; Yu, N.C.; Wu, H.C.; Lee, Y.Y.; Lin, W.C.; Chiu, I.Y.; Chien, W.C.; Liu, Y.C. Association of Body Composition with Type 2 Diabetes: A Retrospective Chart Review Study. Int. J. Environ. Res. Public Health 2021, 18, 4421. [Google Scholar] [CrossRef]
- Buch, A.; Ben-Yehuda, A.; Rouach, V.; Maier, A.B.; Greenman, Y.; Izkhakov, E.; Stern, N.; Eldor, R. Validation of a multi-frequency bioelectrical impedance analysis device for the assessment of body composition in older adults with type 2 diabetes. Nutr. Diabetes 2022, 12, 45. [Google Scholar] [CrossRef]
- Holmes, C.J.; Racette, S.B. The Utility of Body Composition Assessment in Nutrition and Clinical Practice: An Overview of Current Methodology. Nutrients 2021, 13, 2493. [Google Scholar] [CrossRef]
- Low, S.; Pek, S.; Liu, Y.L.; Moh, A.; Ang, K.; Tang, W.E.; Lim, Z.; Subramaniam, T.; Sum, C.F.; Lim, C.L.; et al. Higher extracellular water to total body water ratio was associated with chronic kidney disease progression in type 2 diabetes. J. Diabetes Complicat. 2021, 35, 107930. [Google Scholar] [CrossRef] [PubMed]
- Moh, M.C.; Low, S.; Shao, Y.M.; Subramaniam, T.; Sum, C.F.; Lim, S.C. Association between neutrophil/lymphocyte ratio and kidney impairment in type 2 diabetes mellitus: A role of extracellular water/total body water ratio. Diabetes Res. Clin. Pract. 2023, 199, 110634. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, C.J.; Jhee, J.H.; Yun, H.R.; Kim, H.; Jung, S.Y.; Kee, Y.K.; Yoon, C.Y.; Park, J.T.; Kim, H.C.; et al. Extracellular Fluid Excess Is Significantly Associated With Coronary Artery Calcification in Patients With Chronic Kidney Disease. J. Am. Heart Assoc. 2018, 7, e008935. [Google Scholar] [CrossRef]
- Lorenzo, I.; Serra-Prat, M.; Yébenes, J.C. The Role of Water Homeostasis in Muscle Function and Frailty: A Review. Nutrients 2019, 11, 1857. [Google Scholar] [CrossRef] [PubMed]
- Low, S.; Ng, T.P.; Lim, C.L.; Ang, S.F.; Moh, A.; Wang, J.; Yap, P.; Cheong, C.Y.; Goh, K.S.; Ang, K.; et al. Higher ratio of extracellular water to total body water was associated with reduced cognitive function in type 2 diabetes. J. Diabetes 2021, 13, 222–231. [Google Scholar] [CrossRef]
- Oyanagi, T.; Sada, Y.; Sasaki, Y.; Sone, M.; Tanaka, Y. Associations of phase angle obtained by bioelectrical impedance analysis with muscle mass and strength in Japanese patients with type 2 diabetes. Endocr. J. 2023, 70, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Cancello, R.; Brunani, A.; Brenna, E.; Soranna, D.; Bertoli, S.; Zambon, A.; Lukaski, H.C.; Capodaglio, P. Phase angle (PhA) in overweight and obesity: Evidence of applicability from diagnosis to weight changes in obesity treatment. Rev. Endocr. Metab. Disord. 2023, 24, 451–464. [Google Scholar] [CrossRef]
- Gonzalez, M.C.; Barbosa-Silva, T.G.; Bielemann, R.M.; Gallagher, D.; Heymsfield, S.B. Phase angle and its determinants in healthy subjects: Influence of body composition. Am. J. Clin. Nutr. 2016, 103, 712–716. [Google Scholar] [CrossRef]
- Sandsdal, R.M.; Juhl, C.R.; Jensen, S.B.K.; Lundgren, J.R.; Janus, C.; Blond, M.B.; Rosenkilde, M.; Bogh, A.F.; Gliemann, L.; Jensen, J.B.; et al. Combination of exercise and GLP-1 receptor agonist treatment reduces severity of metabolic syndrome, abdominal obesity, and inflammation: A randomized controlled trial. Cardiovasc. Diabetol. 2023, 22, 41. [Google Scholar] [CrossRef]
- Gaździńska, A.; Gaździński, S.; Jagielski, P.; Kler, P. Body Composition and Cardiovascular Risk: A Study of Polish Military Flying Personnel. Metabolites 2023, 13, 1102. [Google Scholar] [CrossRef]
- Kammar-García, A.; Hernández-Hernández, M.E.; López-Moreno, P.; Ortíz-Bueno, A.M.; Martínez-Montaño, M.L. Relation of body composition indexes to cardiovascular disease risk factors in young adults. Semergen 2019, 45, 147–155. [Google Scholar] [CrossRef]
- Hu, T.; Shen, Y.; Cao, W.; Xu, Y.; Wang, Y.; Ma, X.; Bao, Y. Two-year changes in body composition and future cardiovascular events: A longitudinal community-based study. Nutr. Metab. 2023, 20, 4. [Google Scholar] [CrossRef] [PubMed]
- Yan, K.L.; Liang, I.; Ravellette, K.; Gornbein, J.; Srikanthan, P.; Horwich, T.B. Body Composition Risk Assessment of All-Cause Mortality in Patients With Coronary Artery Disease Completing Cardiac Rehabilitation. J. Am. Heart Assoc. 2025, 14, e035006. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Primary Objectives | Primary Endpoints |
|---|---|
| To assess the long-term effects of OW s.c semaglutide on body composition in T2D obese adults. | Variation in body composition from baseline (T0) to 6 months (T6) and 12 months (T12): FM, FMI, FFM, FMI, SMM, SMI, VAT, ECW, PhA |
| Variation in anthropometric parameters throughout T0, T6, and T12: BW, BMI, waist circumference | |
| Secondary Objective | Secondary Endpoints |
| To assess whether semaglutide-induced weight loss predominantly reflects reductions in fat mass versus lean mass. | Comparation of FFM vs. FM throughout T0, T6, and T12. |
| To explore the association between body composition changes and improvements in metabolic, renal, and cardiovascular risk markers. | Variations in different analytical parameters throughout T0, T6, and T12: HbA1c, FBG, eGFR, UACR, albumin, creatinine, uric acid, total cholesterol, HDL, LDL, triglycerides, SGPT, SGOT, FIB-4. |
| Baseline Demographic Variables | N = 117 |
|---|---|
| Age, years, median (IQR) | 56.0 (45.5, 64.5) |
| Gender, Female, n (%) | 50 (42.7) |
| Weight, kg, median (IQR) | 102.5 (93.2, 116.1) |
| Height, cm, median (IQR) | 167 (160, 173) |
| BMI, median (IQR) | 37.1 (33.2, 42.0) |
| Waist circumference, cm, median (IQR) | 124 (115, 132) |
| Years of evolution of T2D, median (IQR) | 3.0 (0.0, 9.5) |
| Diabetic retinopathy, n (%) | 4 * (3.4) |
| Hypertension, n (%) | 88 (75.2) |
| Dyslipidemia, n (%) | 81 (69.2) |
| SAHS, n (%) | 22 (18.8) |
| Chronic kidney disease, n (%) | 11 (9.4) |
| NAFLD, n (%) | 16 (13.7) |
| Ischemic cardiovascular disease, n (%) | 5 (4.3) |
| Ischemic stroke/TIA, n (%) | 0 (0) |
| Peripheral artery disease, n (%) | 4 (3.4) |
| Heart failure, n (%) | 3 (2.6) |
| Smoking | |
| 24/103 (23.3) |
| 21/103 (20.4) |
| 58/103 (56.3) |
| HbA1c (%), median (IQR) | 9.40 (7.90. 11.20) |
| FBG (mg/dL), median (IQR) | 206.5 (148.5, 257.8) |
| eGFR (mL/min/1.73 m2), median (IQR) | 99.0 (81.0, 110.0) |
| UACR (mg/g), median (IQR) | 9.20 (4.7, 45.3) |
| Albumin (g/dL), median (IQR) | 4.3 (1.7, 4.7) |
| Creatinine (mg/dL), median (IQR) | 0.8 (0.6, 0.9) |
| Uric acid (mg/dL), median (IQR) | 5.1 (4.2; 6.0) |
| Total cholesterol (mg/dL), median (IQR) | 184.5 (161.5, 208.3) |
| HDL (mg/dL), median (IQR) | 40.5 (34.0. 49.7) |
| LDL (mg/dL), median (IQR) | 101.0 (84.0, 126.0) |
| Triglycerides (mg/dL), median (IQR) | 183.0 (135.5, 265.0) |
| SGPT (U/L), median (IQR) | 30.0 (21.0, 54.0) |
| SGOT (U/L), median (IQR) | 28.5 (19.7, 41.2) |
| FIB-4 SGPT, median (IQR) | 1.0 (0.7, 1.3) |
| Type of Treatment | N = 117 |
|---|---|
| Antihyperglycemic Drugs | |
| Insulin, n (%) | 45 (38.5) |
| Total dose, units, median (IQR) | 31.0 (20.0, 60.0) |
| Basal insulin, n (%) | 45 (38.5) |
| Basal dose, units, median (IQR) | 18.0 (14.0, 35.0) |
| Bolus insulin, n (%) | 25 (21.4) |
| Bolus dose, units, median (IQR) | 18.0 (12.0, 33.0) |
| Oral antihyperglycemic drugs | |
| Metformin, n (%) | 83 (70.9) |
| Sulfonylurea, n (%) | 14 (12.0) |
| iDPP-4, n (%) | 29 (24.8) |
| Pioglitazones, n (%) | 2 (1.7) |
| Drugs with dual action on glycemia and weight | |
| iSGLT2, n (%) | 32 (27.3) |
| GLP-1 RA other than semaglutide *, n (%) | 10 * (8.5) |
| Antihypertensive drugs | |
| ACE inhibitors, n (%) | 75 (64.1) |
| Beta blockers, n/N (%) | 18/116 (15.5) a |
| Alpha blockers, n (%) | 1 (0.8) |
| Diuretics, n (%) | 42 (35.9) |
| Calcium channel blockers, n (%) | 22 (18.8) |
| Potassium-conserving drugs, n/N (%) | 2/115 (1.7) b |
| Lipid-lowering drugs | |
| Statins, n (%) | 50 (42.7) |
| PCSK9 inhibitors, n (%) | 0 (0) |
| Fibrates, n (%) | 8 (6.8) |
| Ezetimibe, n (%) | 8 (6.8) |
| Anticoagulant drugs, n (%) | 7 (6.0) |
| Platelet-lowering drugs, n (%) | 21 (17.9) |
| Variable | Basal Value (n = 117) | Δ 6 Months vs. Baseline | n | p | Δ 12 Months vs. Baseline | n | p |
|---|---|---|---|---|---|---|---|
| Body weight (kg) | 102.5 (93.2, 116.1) | −9.3 (−13.8, −6.7) | 117 | <0.001 | −11.20 (−17.00, −8.50) | 83 | <0.001 |
| FM (kg) | 47.75 (37.30, 55.15) | −7.55 (−11.18, −5.10) | 116 | <0.001 | −9.70 (−13.10, −6.30) | 61 | <0.001 |
| FFM (kg) | 57.30 (49.35, 64.40) | −1.80 (−3.45, −0.10) | 109 | <0.001 | −2.20 (−3.92, −0.77) | 50 | <0.001 |
| Visceral fat (cm2) | 240.10 (189.00, 261.10) | −32.90 (−49.30, −18.60) | 119 | <0.001 | −37.70 (−62.13, −19.35) | 58 | <0.001 |
| SMM (kg) | 31.85 (26.60, 35.95) | −1.20 (−2.00, −0.20) | 117 | <0.001 | −1.20 (−2.10, −0.60) | 60 | <0.001 |
| FMI (kg/m2) | 16.93 (13.47, 20.72) | −2.80 (−3.89, −1.94) | 116 | <0.001 | −3.63 (−4.84, −2.42) | 61 | <0.001 |
| FFMI | 20.57 (18.73, 22.19) | −0.63 (−1.37, −0.03) | 109 | <0.001 | −0.72 (−1.44, −0.29) | 50 | <0.001 |
| SMI (kg/m2) | 8.40 (7.70, 9.30) | −0.30 (−0.50, −0.10) | 92 | <0.001 | −0.40 (−0.65, −0.10) | 21 | <0.001 |
| HbA1c (%) | 9.40 (7.90, 11.20) | −3.10 (−5.27, −1.80) | 116 | <0.001 | −3.30 (−5.30, −1.50) | 83 | <0.001 |
| ECW (L) | 16.15 (14.35, 19.05) | −0.40 (−0.80, 0.0) | 73 | <0.001 | −0.90 (−2.20, −0.02) | 10 | 0.029 |
| ECW/TBW | 0.388 (0.379, 0.395) | 0.001 (−0.003, 0.004) | 91 | 0.043 | 0.0 (−0.003, 0.003) | 30 | 0.409 |
| PhA (o) | 5.100 (4.500, 5.700) | −0.150 (−0.325, 0.125) | 102 | <0.001 | −0.200 (−0.350, 0.100) | 49 | 0.001 |
| Variables | Δ 6 Months vs. Baseline | n | p | Δ 12 Months vs. Baseline | n | p |
|---|---|---|---|---|---|---|
| Body weight (kg) | −9.3 (−13.8, −6.7) | 117 | <0.001 | −11.7 (−17.8, −8.7) | 72 | <0.001 |
| HbA1c (%) | −3.10 (−5.27, −1.80) | 116 | <0.001 | −3.70 (−5.27, −1.72) | 72 | <0.001 |
| BMI (kg/m2) | −3.67 (−5.16, −2.39) | 117 | <0.001 | −4.22 (−6.25, −2.89) | 72 | <0.001 |
| FBG (mg/dL) | −90.0 (−171.0, −43.0) | 95 | <0.001 | −96.0 (−143.3, −42.2) | 54 | <0.001 |
| eGFR (mL/min/1.73 m2) | −1.0 (−7.7, 4.0) | 84 | 0.049 | 0.0 (−11.0, 4.0) | 47 | 0.156 |
| UACR (mg/g) | −1.70 (−10.00, 2.40) | 29 | 0.140 | −5.10 (−21.23, 1.02) | 10 | 0.042 |
| Albumin (g/dL) | 0.30 (−0.47, 0.77) | 8 | 0.312 | −0.10 (−0.32, 2.88) | 4 | 0.427 |
| Creatinine (mg/dL) | 0.02 (−0.05, 0.11) | 89 | 0.051 | −0.01 (−0.07, 0.14) | 51 | 0.195 |
| Uric acid (mg/dL) | −0.20 (−0.90, 0.40) | 27 | 0.052 | −1.70 (−2.10, 0.0) | 15 | 0.003 |
| Total cholesterol (mg/dL) | −24.0 (−57.0, −3.5) | 85 | <0.001 | −15.0 (−43.0, −1.0) | 43 | <0.001 |
| HDL (mg/dL) | 1.0 (−4.0, 4.0) | 69 | 0.298 | 4.0 (0.0, 8.0) | 31 | <0.001 |
| LDL (mg/dL) | −20.5 (−56.5, 2.7) | 52 | <0.001 | −7.5 (−26.0, 6.2) | 20 | 0.068 |
| Triglycerides (mg/dL) | −64.5 (−94.2, −1.5) | 86 | <0.001 | −43.0 (−133.0, −5.5) | 45 | <0.001 |
| SGPT (U/L) | −11.0 (−33.5, −4.0) | 81 | <0.001 | −11.0 (−29.0, −5.0) | 37 | <0.001 |
| SGOT (U/L) | −9.0 (−25.5, −2.5) | 33 | <0.001 | −10.5 (−25.2, −4.0) | 16 | <0.001 |
| FIB−4 | −0.21 (−0.42, 0.01) | 29 | 0.003 | −0.16 (−0.56, 0.05) | 12 | 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caballero-Mateos, I.; Morales-Portillo, C.; González Aguilera, B. Once-Weekly Semaglutide Improves Body Composition in Spanish Obese Adults with Type 2 Diabetes: A 48-Week Prospective Real-Life Study. J. Clin. Med. 2025, 14, 5434. https://doi.org/10.3390/jcm14155434
Caballero-Mateos I, Morales-Portillo C, González Aguilera B. Once-Weekly Semaglutide Improves Body Composition in Spanish Obese Adults with Type 2 Diabetes: A 48-Week Prospective Real-Life Study. Journal of Clinical Medicine. 2025; 14(15):5434. https://doi.org/10.3390/jcm14155434
Chicago/Turabian StyleCaballero-Mateos, Irene, Cristóbal Morales-Portillo, and Beatriz González Aguilera. 2025. "Once-Weekly Semaglutide Improves Body Composition in Spanish Obese Adults with Type 2 Diabetes: A 48-Week Prospective Real-Life Study" Journal of Clinical Medicine 14, no. 15: 5434. https://doi.org/10.3390/jcm14155434
APA StyleCaballero-Mateos, I., Morales-Portillo, C., & González Aguilera, B. (2025). Once-Weekly Semaglutide Improves Body Composition in Spanish Obese Adults with Type 2 Diabetes: A 48-Week Prospective Real-Life Study. Journal of Clinical Medicine, 14(15), 5434. https://doi.org/10.3390/jcm14155434