
Fractional Flow Reserve in the Left Anterior Descending Artery

Abstract
1. Introduction
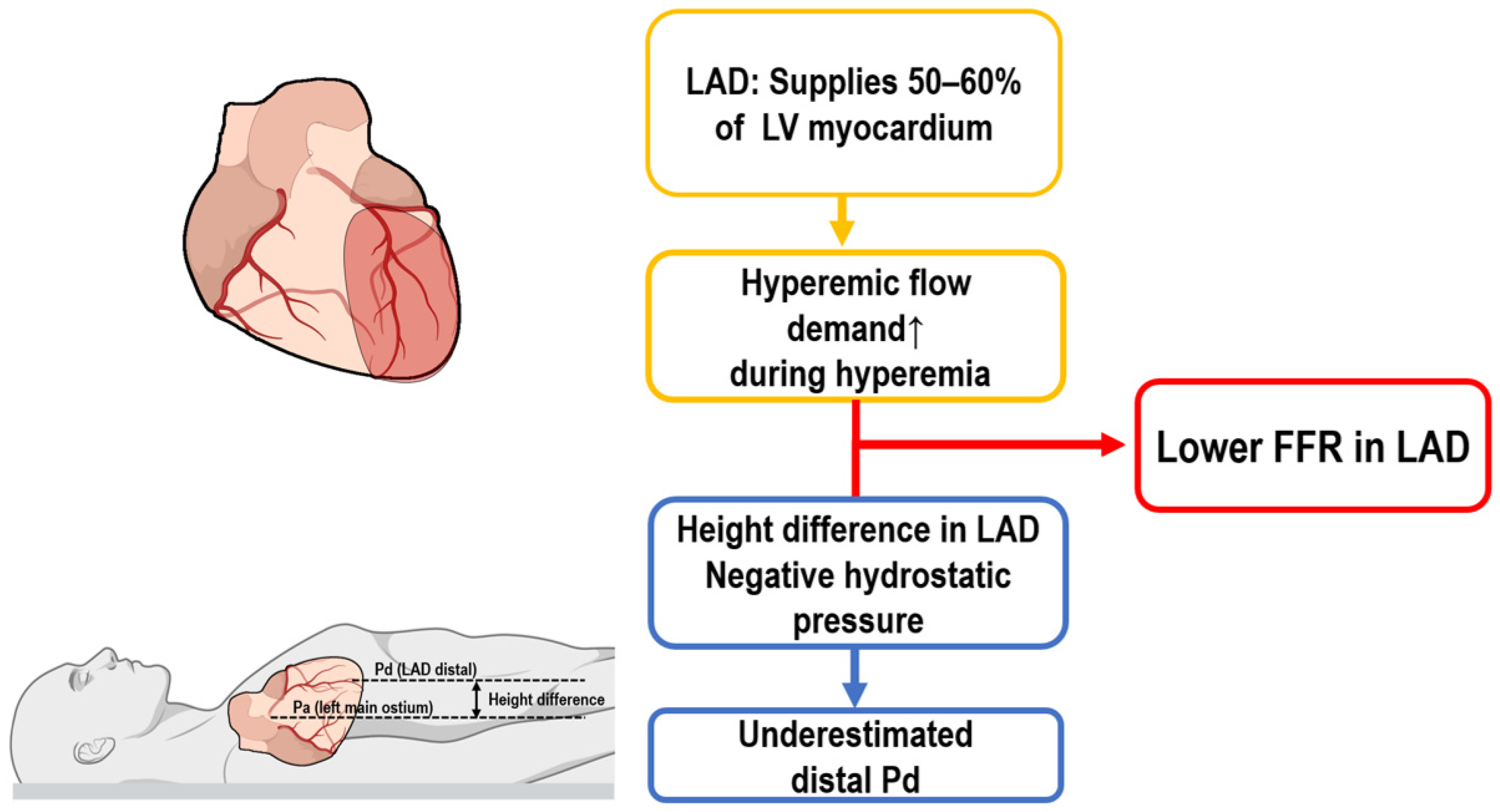
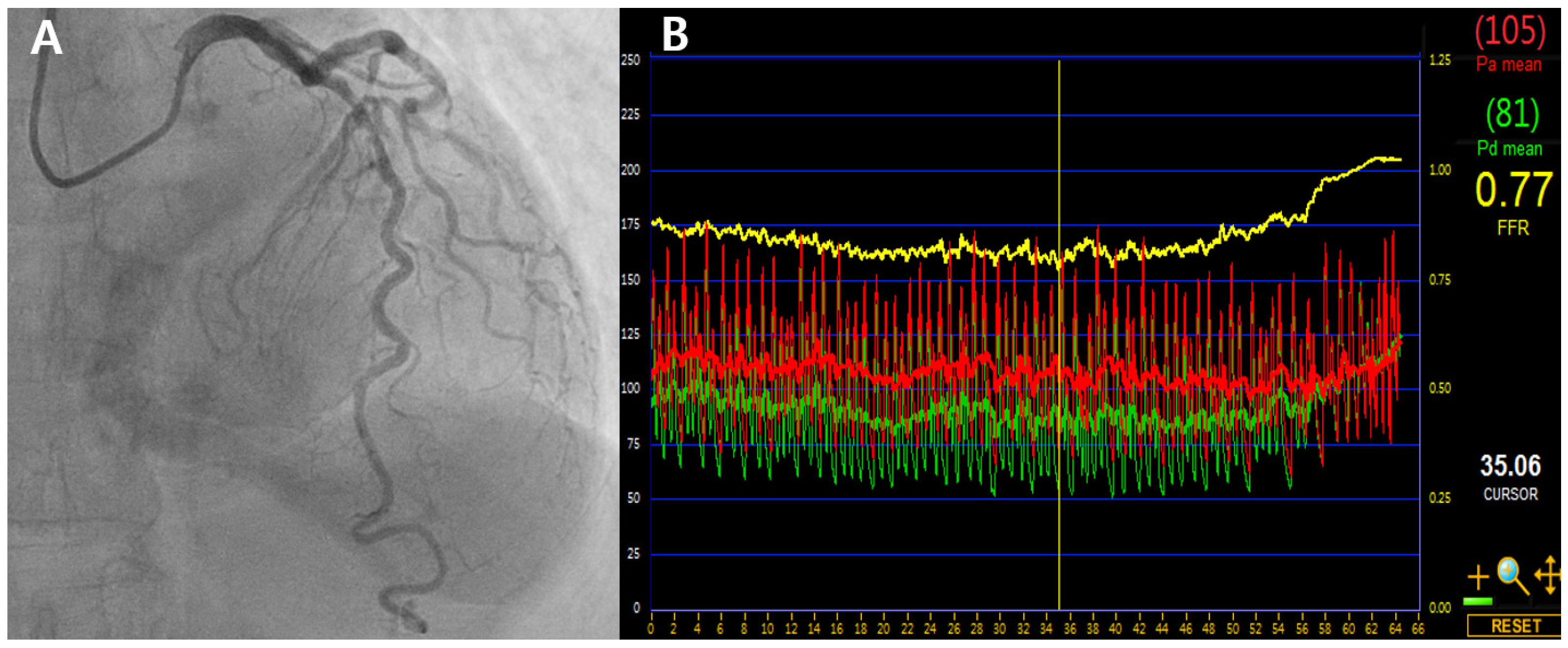
2. Differences in FFR Measurements in the LAD
3. FFR-Guided Deferral in LAD vs. Non-LAD Lesions: Insights from Clinical Data
4. Post-PCI FFR: LAD vs. Non-LAD
5. iFR vs. FFR in LAD Deferral
6. Non-Culprit Lesion FFR in AMI with MVD: LAD vs. Non-LAD
7. Is Vessel-Specific FFR Targeting Feasible and Justified?
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| AMI | Acute myocardial infarction |
| CAD | Coronary artery disease |
| CFR | Coronary flow reserve |
| CR | Complete revascularization |
| FFR | Fractional flow reserve |
| HPDs | Hydrostatic pressure differences |
| iFR | Instantaneous wave-free ratio |
| LAD | Left anterior descending artery |
| LCx | Left circumflex |
| MVD | Multivessel disease |
| PCI | Post-percutaneous coronary intervention |
| Pd | Distal coronary pressure |
| QFR | Quantitative flow ratio |
| RCA | Right coronary artery |
References
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on Myocardial Revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Pijls, N.H.; Van Son, J.A.; Kirkeeide, R.L.; De Bruyne, B.; Gould, K.L. Experimental Basis of Determining Maximum Coronary, Myocardial, and Collateral Blood Flow by Pressure Measurements for Assessing Functional Stenosis Severity before and after Percutaneous Transluminal Coronary Angioplasty. Circulation 1993, 87, 1354–1367. [Google Scholar] [CrossRef]
- Pijls, N.H.J.; De Bruyne, B.; Peels, K.; Van Der Voort, P.H.; Bonnier, H.J.R.M.; Bartunek, J.; Koolen, J.J. Measurement of Fractional Flow Reserve to Assess the Functional Severity of Coronary-Artery Stenoses. N. Engl. J. Med. 1996, 334, 1703–1708. [Google Scholar] [CrossRef]
- Bech, G.J.W.; De Bruyne, B.; Pijls, N.H.J.; De Muinck, E.D.; Hoorntje, J.C.A.; Escaned, J.; Stella, P.R.; Boersma, E.; Bartunek, J.; Koolen, J.J.; et al. Fractional Flow Reserve to Determine the Appropriateness of Angioplasty in Moderate Coronary Stenosis: A Randomized Trial. Circulation 2001, 103, 2928–2934. [Google Scholar] [CrossRef]
- Tonino, P.A.L.; De Bruyne, B.; Pijls, N.H.J.; Siebert, U.; Ikeno, F.; Vant Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional Flow Reserve versus Angiography for Guiding Percutaneous Coronary Intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef]
- De Bruyne, B.; Pijls, N.H.J.; Kalesan, B.; Barbato, E.; Tonino, P.A.L.; Piroth, Z.; Jagic, N.; Möbius-Winkler, S.; Rioufol, G.; Witt, N.; et al. Fractional Flow Reserve—Guided PCI versus Medical Therapy in Stable Coronary Disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef]
- Bax, A.M.; Van Rosendael, A.R.; Ma, X.; Van Den Hoogen, I.J.; Gianni, U.; Tantawy, S.W.; Hollenberg, E.J.; Andreini, D.; Al-Mallah, M.H.; Budoff, M.J.; et al. Comparative Differences in the Atherosclerotic Disease Burden between the Epicardial Coronary Arteries: Quantitative Plaque Analysis on Coronary Computed Tomography Angiography. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Bax, A.M.; Lin, F.Y.; Van Rosendael, A.R.; Ma, X.; Lu, Y.; Van Den Hoogen, I.J.; Gianni, U.; Tantawy, S.W.; Andreini, D.; Budoff, M.J.; et al. Marked Variation in Atherosclerotic Plaque Progression between the Major Epicardial Coronary Arteries. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1482–1491. [Google Scholar] [CrossRef]
- Entezarjou, A.; Mohammad, M.A.; Andell, P.; Koul, S. Culprit Vessel: Impact on Short-Term and Long-Term Prognosis in Patients with ST-Elevation Myocardial Infarction. Open Heart 2018, 5, e000852. [Google Scholar] [CrossRef]
- Park, D.-W.; Clare, R.M.; Schulte, P.J.; Pieper, K.S.; Shaw, L.K.; Califf, R.M.; Ohman, E.M.; Van De Werf, F.; Hirji, S.; Harrington, R.A.; et al. Extent, Location, and Clinical Significance of Non-Infarct-Related Coronary Artery Disease Among Patients with ST-Elevation Myocardial Infarction. JAMA 2014, 312, 2019–2027. [Google Scholar] [CrossRef] [PubMed]
- Yokota, S.; Borren, N.M.; Ottervanger, J.P.; Mouden, M.; Timmer, J.R.; Knollema, S.; Jager, P.L. Does Fractional Flow Reserve Overestimate Severity of LAD Lesions? J. Nucl. Cardiol. 2020, 27, 1306–1313. [Google Scholar] [CrossRef]
- Leone, A.M.; De Caterina, A.R.; Basile, E.; Gardi, A.; Laezza, D.; Mazzari, M.A.; Mongiardo, R.; Kharbanda, R.; Cuculi, F.; Porto, I.; et al. Influence of the Amount of Myocardium Subtended by a Stenosis on Fractional Flow Reserve. Circ. Cardiovasc. Interv. 2013, 6, 29–36. [Google Scholar] [CrossRef]
- Härle, T.; Luz, M.; Meyer, S.; Kronberg, K.; Nickau, B.; Escaned, J.; Davies, J.; Elsässer, A. Effect of Coronary Anatomy and Hydrostatic Pressure on Intracoronary Indices of Stenosis Severity. JACC Cardiovasc. Interv. 2017, 10, 764–773. [Google Scholar] [CrossRef]
- Nagamatsu, S.; Sakamoto, K.; Yamashita, T.; Sato, R.; Tabata, N.; Motozato, K.; Yamanaga, K.; Ito, M.; Fujisue, K.; Kanazawa, H.; et al. Impact of Hydrostatic Pressure on Fractional Flow Reserve: In Vivo Experimental Study of Anatomical Height Difference of Coronary Arteries. J. Cardiol. 2020, 76, 73–79. [Google Scholar] [CrossRef]
- Soh, M.-S.; Kim, H.; Kang, M.G.; Lee, H.J.; Lee, S.D.; Hwang, S.-J.; Hwang, J.-Y.; Kim, K.; Park, J.-R.; Kim, H.-R.; et al. Impact of Height Difference between Coronary Ostium and Location of Intracoronary Pressure Sensor on Fractional Flow Reserve Measurements. PLoS ONE 2023, 18, e0289646. [Google Scholar] [CrossRef]
- Matsumoto, H.; Masaki, R.; Higuchi, S.; Tanaka, H.; Kondo, S.; Tsujita, H.; Shinke, T. Impact of Overestimation of Fractional Flow Reserve by Adenosine on Anatomical–Functional Mismatch. Sci. Rep. 2022, 12, 14962. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Nakatsuma, K.; Shimada, T.; Ushimaru, S.; Mikuri, M.; Yamazaki, T.; Matsuda, T. Effect of Caffeine on Intravenous Adenosine-Induced Hyperemia in Fractional Flow Reserve Measurement. J. Invasive Cardiol. 2014, 26, 580–585. [Google Scholar] [PubMed]
- Kasumi, I.; Fujii, K.; Satoru, O.; Shin, T.; Katsuyuki, H.; Hiroto, T.; Rui, I.; Shingo, Y.; Sho, N.; Wataru, Y.; et al. Influence of Caffeine Intake on Intravenous Adenosine-Induced Fractional Flow Reserve. J. Cardiol. 2020, 76, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Curzen, N.; Rana, O.; Nicholas, Z.; Golledge, P.; Zaman, A.; Oldroyd, K.; Hanratty, C.; Banning, A.; Wheatcroft, S.; Hobson, A.; et al. Does Routine Pressure Wire Assessment Influence Management Strategy at Coronary Angiography for Diagnosis of Chest Pain?: The RIPCORD Study. Circ. Cardiovasc. Interv. 2014, 7, 248–255. [Google Scholar] [CrossRef]
- Lee, J.-H.; Ahn, S.G.; Jeon, H.S.; Lee, J.-W.; Youn, Y.J.; Zhang, J.; Hu, X.; Wang, J.; Lee, J.M.; Hahn, J.-Y.; et al. Discordance Between Angiographic Assessment and Fractional Flow Reserve or Intravascular Ultrasound in Intermediate Coronary Lesions: A Post-Hoc Analysis of the FLAVOUR Trial. Korean Circ. J. 2024, 54, 485. [Google Scholar] [CrossRef]
- Nakamura, M.; Yamagishi, M.; Ueno, T.; Hara, K.; Ishiwata, S.; Itoh, T.; Hamanaka, I.; Wakatsuki, T.; Sugano, T.; Kawai, K.; et al. Prevalence of Visual–Functional Mismatch Regarding Coronary Artery Stenosis in the CVIT-DEFER Registry. Cardiovasc. Interv. Ther. 2014, 29, 300–308. [Google Scholar] [CrossRef]
- Pijls, N.H.J.; Van Schaardenburgh, P.; Manoharan, G.; Boersma, E.; Bech, J.-W.; Van’T Veer, M.; Bär, F.; Hoorntje, J.; Koolen, J.; Wijns, W.; et al. Percutaneous Coronary Intervention of Functionally Nonsignificant Stenosis. J. Am. Coll. Cardiol. 2007, 49, 2105–2111. [Google Scholar] [CrossRef]
- Kuramitsu, S.; Matsuo, H.; Shinozaki, T.; Horie, K.; Takashima, H.; Terai, H.; Kikuta, Y.; Ishihara, T.; Saigusa, T.; Sakamoto, T.; et al. Five-Year Outcomes After Fractional Flow Reserve–Based Deferral of Revascularization in Chronic Coronary Syndrome: Final Results From the J-CONFIRM Registry. Circ. Cardiovasc. Interv. 2022, 15, e011387. [Google Scholar] [CrossRef] [PubMed]
- Ekmejian, A.; Brieger, D.; Bhat, A.; Sritharan, H.; Nour, D.; Allahwala, U.; Ward, M.; Bhindi, R. Vessel-Specific Outcomes of Deferred Revascularization Following Negative Fractional Flow Reserve. Am. J. Cardiol. 2023, 201, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.-M.; Park, D.-W.; Shin, E.-S.; Koo, B.-K.; Nam, C.-W.; Doh, J.-H.; Kim, J.H.; Chae, I.-H.; Yoon, J.-H.; Her, S.-H.; et al. Fractional Flow Reserve and Cardiac Events in Coronary Artery Disease: Data From a Prospective IRIS-FFR Registry (Interventional Cardiology Research Incooperation Society Fractional Flow Reserve). Circulation 2017, 135, 2241–2251. [Google Scholar] [CrossRef] [PubMed]
- Won, K.-B.; Nam, C.-W.; Cho, Y.-K.; Yoon, H.-J.; Park, H.-S.; Kim, H.; Han, S.; Hur, S.-H.; Kim, Y.-N.; Park, S.-H.; et al. Clinical Outcomes in Patients with Deferred Coronary Lesions According to Disease Severity Assessed by Fractional Flow Reserve. J. Korean Med. Sci. 2016, 31, 1929. [Google Scholar] [CrossRef]
- Li, J.; Elrashidi, M.Y.; Flammer, A.J.; Lennon, R.J.; Bell, M.R.; Holmes, D.R.; Bresnahan, J.F.; Rihal, C.S.; Lerman, L.O.; Lerman, A. Long-Term Outcomes of Fractional Flow Reserve-Guided vs. Angiography-Guided Percutaneous Coronary Intervention in Contemporary Practice. Eur. Heart J. 2013, 34, 1375–1383. [Google Scholar] [CrossRef] [PubMed]
- Jeremias, A.; Davies, J.E.; Maehara, A.; Matsumura, M.; Schneider, J.; Tang, K.; Talwar, S.; Marques, K.; Shammas, N.W.; Gruberg, L.; et al. Blinded Physiological Assessment of Residual Ischemia After Successful Angiographic Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2019, 12, 1991–2001. [Google Scholar] [CrossRef]
- Leesar, M.A.; Satran, A.; Yalamanchili, V.; Helmy, T.; Abdul-Waheed, M.; Wongpraparut, N. The Impact of Fractional Flow Reserve Measurement on Clinical Outcomes after Transradial Coronary Stenting. EuroIntervention 2011, 7, 917–923. [Google Scholar] [CrossRef]
- Andersen, B.K.; Ding, D.; Mogensen, L.J.H.; Tu, S.; Holm, N.R.; Westra, J.; Wijns, W. Predictive Value of Post-Percutaneous Coronary Intervention Fractional Flow Reserve: A Systematic Review and Meta-Analysis. Eur. Heart J. Qual. Care Clin. Outcomes 2023, 9, 99–108. [Google Scholar] [CrossRef]
- Shin, D.; Lee, S.H.; Lee, J.M.; Choi, K.H.; Hwang, D.; Lee, H.-J.; Jang, H.-J.; Kim, H.K.; Kwak, J.-J.; Ha, S.J.; et al. Prognostic Implications of Post-Intervention Resting Pd/Pa and Fractional Flow Reserve in Patients with Stent Implantation. JACC Cardiovasc. Interv. 2020, 13, 1920–1933. [Google Scholar] [CrossRef]
- Rimac, G.; Fearon, W.F.; De Bruyne, B.; Ikeno, F.; Matsuo, H.; Piroth, Z.; Costerousse, O.; Bertrand, O.F. Clinical Value of Post-Percutaneous Coronary Intervention Fractional Flow Reserve Value: A Systematic Review and Meta-Analysis. Am. Heart J. 2017, 183, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-J.; Ge, Z.; Kan, J.; Zhang, J.-J.; Ye, F.; Kwan, T.W.; Santoso, T.; Yang, S.; Sheiban, I.; Qian, X.-S.; et al. Cutoff Value and Long-Term Prediction of Clinical Events by FFR Measured Immediately After Implantation of a Drug-Eluting Stent in Patients with Coronary Artery Disease. JACC Cardiovasc. Interv. 2017, 10, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Lee, J.M.; Lee, H.-J.; Kim, S.H.; Nam, C.-W.; Hahn, J.-Y.; Shin, E.-S.; Matsuo, A.; Tanaka, N.; Matsuo, H.; et al. Influence of Target Vessel on Prognostic Relevance of Fractional Flow Reserve after Coronary Stenting. EuroIntervention 2019, 15, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Collet, C.; Johnson, N.P.; Mizukami, T.; Fearon, W.F.; Berry, C.; Sonck, J.; Collison, D.; Koo, B.-K.; Meneveau, N.; Agarwal, S.K.; et al. Impact of Post-PCI FFR Stratified by Coronary Artery. JACC Cardiovasc. Interv. 2023, 16, 2396–2408. [Google Scholar] [CrossRef]
- Davies, J.E.; Sen, S.; Dehbi, H.-M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the Instantaneous Wave-Free Ratio or Fractional Flow Reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef]
- Götberg, M.; Christiansen, E.H.; Gudmundsdottir, I.J.; Sandhall, L.; Danielewicz, M.; Jakobsen, L.; Olsson, S.-E.; Öhagen, P.; Olsson, H.; Omerovic, E.; et al. Instantaneous Wave-Free Ratio versus Fractional Flow Reserve to Guide PCI. N. Engl. J. Med. 2017, 376, 1813–1823. [Google Scholar] [CrossRef]
- Warisawa, T.; Cook, C.M.; Seligman, H.; Howard, J.P.; Ahmad, Y.; Rajkumar, C.; Doi, S.; Nakayama, M.; Tanigaki, T.; Omori, H.; et al. Per-Vessel Level Analysis of Fractional Flow Reserve and Instantaneous Wave-Free Ratio Discordance―Insights From the AJIP Registry. Circ. J. 2020, 84, 1034–1038. [Google Scholar] [CrossRef]
- Balfe, C.; Jacob, B.; Hickey, N.; Moore, D.; Mulcahy, D.; Loo, B. Exploring Diastolic Pressure Ratio to Fractional Flow Reserve Discordance and a Hypothesis on Tailoring Diastolic Pressure Ratio Cut-off Values to Improve Diagnostic Accuracy in the Mid- and Distal-LAD. IJC Heart Vasc. 2021, 34, 100784. [Google Scholar] [CrossRef]
- Petraco, R.; Van De Hoef, T.P.; Nijjer, S.; Sen, S.; Van Lavieren, M.A.; Foale, R.A.; Meuwissen, M.; Broyd, C.; Echavarria-Pinto, M.; Foin, N.; et al. Baseline Instantaneous Wave-Free Ratio as a Pressure-Only Estimation of Underlying Coronary Flow Reserve: Results of the JUSTIFY-CFR Study (Joined Coronary Pressure and Flow Analysis to Determine Diagnostic Characteristics of Basal and Hyperemic Indices of Functional Lesion Severity–Coronary Flow Reserve). Circ. Cardiovasc. Interv. 2014, 7, 492–502. [Google Scholar] [CrossRef]
- Nijjer, S.S.; De Waard, G.A.; Sen, S.; Van De Hoef, T.P.; Petraco, R.; Echavarría-Pinto, M.; Van Lavieren, M.A.; Meuwissen, M.; Danad, I.; Knaapen, P.; et al. Coronary Pressure and Flow Relationships in Humans: Phasic Analysis of Normal and Pathological Vessels and the Implications for Stenosis Assessment: A Report from the Iberian–Dutch–English (IDEAL) Collaborators. Eur. Heart J. 2015, 37, 2069–2080. [Google Scholar] [CrossRef]
- Escaned, J.; Travieso, A.; Dehbi, H.-M.; Nijjer, S.S.; Sen, S.; Petraco, R.; Patel, M.; Serruys, P.W.; Davies, J.; DEFINE FLAIR Investigators; et al. Coronary Revascularization Guided with Fractional Flow Reserve or Instantaneous Wave-Free Ratio: A 5-Year Follow-Up of the DEFINE FLAIR Randomized Clinical Trial. JAMA Cardiol. 2025, 10, 25. [Google Scholar] [CrossRef]
- Sreenivasan, J.; Jamil, Y.; Ahmad, Y. Revascularization and Mortality at 5 Years After Treatment Guided By Instantaneous Wave-Free Ratio and Fractional Flow Reserve: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2023, 12, e032015. [Google Scholar] [CrossRef] [PubMed]
- Engstrøm, T.; Kelbæk, H.; Helqvist, S.; Høfsten, D.E.; Kløvgaard, L.; Holmvang, L.; Jørgensen, E.; Pedersen, F.; Saunamäki, K.; Clemmensen, P.; et al. Complete Revascularisation versus Treatment of the Culprit Lesion Only in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Disease (DANAMI-3—PRIMULTI): An Open-Label, Randomised Controlled Trial. Lancet 2015, 386, 665–671. [Google Scholar] [CrossRef]
- Smits, P.C.; Abdel-Wahab, M.; Neumann, F.-J.; Boxma-de Klerk, B.M.; Lunde, K.; Schotborgh, C.E.; Piroth, Z.; Horak, D.; Wlodarczak, A.; Ong, P.J.; et al. Fractional Flow Reserve–Guided Multivessel Angioplasty in Myocardial Infarction. N. Engl. J. Med. 2017, 376, 1234–1244. [Google Scholar] [CrossRef] [PubMed]
- Böhm, F.; Mogensen, B.; Engstrøm, T.; Stankovic, G.; Srdanovic, I.; Lønborg, J.; Zwackman, S.; Hamid, M.; Kellerth, T.; Lauermann, J.; et al. FFR-Guided Complete or Culprit-Only PCI in Patients with Myocardial Infarction. N. Engl. J. Med. 2024, 390, 1481–1492. [Google Scholar] [CrossRef]
- Lee, J.M.; Kim, H.K.; Park, K.H.; Choo, E.H.; Kim, C.J.; Lee, S.H.; Kim, M.C.; Hong, Y.J.; Ahn, S.G.; Doh, J.-H.; et al. Fractional Flow Reserve versus Angiography-Guided Strategy in Acute Myocardial Infarction with Multivessel Disease: A Randomized Trial. Eur. Heart J. 2023, 44, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Puymirat, E.; Cayla, G.; Simon, T.; Steg, P.G.; Montalescot, G.; Durand-Zaleski, I.; Le Bras, A.; Gallet, R.; Khalife, K.; Morelle, J.-F.; et al. Multivessel PCI Guided by FFR or Angiography for Myocardial Infarction. N. Engl. J. Med. 2021, 385, 297–308. [Google Scholar] [CrossRef]
- Piróth, Z.; Boxma-de Klerk, B.M.; Omerovic, E.; Andréka, P.; Fontos, G.; Fülöp, G.; Abdel-Wahab, M.; Neumann, F.-J.; Richardt, G.; Abdelghani, M.; et al. The Natural History of Nonculprit Lesions in STEMI. JACC Cardiovasc. Interv. 2020, 13, 954–961. [Google Scholar] [CrossRef]
- Jeon, H.S.; Lee, J.-H.; Lee, J.-W.; Youn, Y.J.; Lee, J.M.; Kim, H.K.; Park, K.H.; Choo, E.H.; Kim, C.J.; Lee, S.H.; et al. Non-Culprit Lesion Location and FFR-Guided Revascularization in Acute Myocardial Infarction with Multivessel Disease: FRAME-AMI Substudy. Korean Circ. J. 2024, 55, e91. [Google Scholar] [CrossRef]
- Uren, N.G.; Crake, T.; Lefroy, D.C.; De Silva, R.; Davies, G.J.; Maseri, A. Reduced Coronary Vasodilator Function in Infarcted and Normal Myocardium after Myocardial Infarction. N. Engl. J. Med. 1994, 331, 222–227. [Google Scholar] [CrossRef]
- Van Der Hoeven, N.W.; Janssens, G.N.; De Waard, G.A.; Everaars, H.; Broyd, C.J.; Beijnink, C.W.H.; Van De Ven, P.M.; Nijveldt, R.; Cook, C.M.; Petraco, R.; et al. Temporal Changes in Coronary Hyperemic and Resting Hemodynamic Indices in Nonculprit Vessels of Patients with ST-Segment Elevation Myocardial Infarction. JAMA Cardiol. 2019, 4, 736. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, H.K.; Lee, J.M.; Hong, Y.J.; Lim, K.S.; Kim, H.B.; Choi, K.H.; Shin, E.-S.; Nam, C.-W.; Doh, J.-H.; et al. Coronary Circulatory Indexes in Non-Infarct-Related Vascular Territories in a Porcine Acute Myocardial Infarction Model. JACC Cardiovasc. Interv. 2020, 13, 1155–1167. [Google Scholar] [CrossRef]
- Mahendiran, T.; Thanou, D.; Senouf, O.; Jamaa, Y.; Fournier, S.; De Bruyne, B.; Abbé, E.; Muller, O.; Andò, E. AngioPy Segmentation: An Open-Source, User-Guided Deep Learning Tool for Coronary Artery Segmentation. Int. J. Cardiol. 2025, 418, 132598. [Google Scholar] [CrossRef]
- Mahendiran, T.; Thanou, D.; Senouf, O.; Meier, D.; Dayer, N.; Aminfar, F.; Auberson, D.; Raita, O.; Frossard, P.; Pagnoni, M.; et al. Deep Learning-Based Prediction of Future Myocardial Infarction Using Invasive Coronary Angiography: A Feasibility Study. Open Heart 2023, 10, e002237. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Wang, Z.; Chen, T.; Liu, S.; Tan, J.; Sun, Y.; Feng, L.; Zhang, D.; Ma, L.; Liu, H.; et al. Artificial Intelligence Driven Plaque Characterization and Functional Assessment from CCTA Using OCT-Based Automation: A Prospective Study. Int. J. Cardiol. 2025, 428, 133140. [Google Scholar] [CrossRef] [PubMed]
- Peters, B.; Paul, J.-F.; Symons, R.; Franssen, W.M.A.; Nchimi, A.; Ghekiere, O. Invasive Fractional-Flow-Reserve Prediction by Coronary CT Angiography Using Artificial Intelligence vs. Computational Fluid Dynamics Software in Intermediate-Grade Stenosis. Int. J. Cardiovasc. Imaging 2024, 40, 1875–1880. [Google Scholar] [CrossRef] [PubMed]
- Von Knebel Doeberitz, P.L.; De Cecco, C.N.; Schoepf, U.J.; Duguay, T.M.; Albrecht, M.H.; Van Assen, M.; Bauer, M.J.; Savage, R.H.; Pannell, J.T.; De Santis, D.; et al. Coronary CT Angiography–Derived Plaque Quantification with Artificial Intelligence CT Fractional Flow Reserve for the Identification of Lesion-Specific Ischemia. Eur. Radiol. 2019, 29, 2378–2387. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| STUDY | Angiographic Stenosis Criteria (QCA) | LAD (FFR ≤ 0.80, %) | LCx (FFR ≤ 0.80, %) | RCA (FFR ≤ 0.80, %) |
|---|---|---|---|---|
| RIPCORD [19] | <50% | 18.0% | 13.5% | 8.5% |
| FLAVOUR [20] | <60% | 82.2% | 3.4% | 14.4% |
| CVIT-DEFER [21] | <75% | 33.4% | 8.7% | 9.7% |
| Study | Study Type | LAD-Specific Outcomes | Implications for LAD |
|---|---|---|---|
| DEFER [22] | Pioneering RCT | LAD lesions (>50%), no specific outcomes reported | Indirect safety evidence |
| FAME 1/2 [5,6] | Large-scale RCTs | No vessel-specific outcomes | No direct LAD-specific data |
| J-CONFIRM [23] | Multicenter Registry | LAD deferral: ↓TVF (HR 0.42, p = 0.003) RCA deferral: ↑TVF (HR 1.78, p = 0.042) LCx deferral: NS | Supports safety of LAD deferral |
| Ekmejian et al. [24] | Multicenter Registry | Mean FFR: LAD lowest (0.82), LCx (0.88), RCA (0.88) TLF similar (10.2% LAD vs. 11.5% LCx, 11.0% RCA, NS) TLMI lower in LAD (1.45%, NS) | Lower FFR but comparable outcomes in LAD |
| IRIS-FFR [25] | Multicenter Registry | Annual MACEs: LAD 1.7%, LCx 1.47%, RCA 1.25% | Similar outcomes across vessels |
| Korean FFR [26] | Multicenter Registry | LAD deferred: lower MACE trend vs. non-LAD (HR 0.57, NS). | Possible LAD benefit (limited evidence) |
| Mayo FFR [27] | Single-center Registry | Similar PCI rates after deferral (LAD 5.4%, LCx 6.2%, RCA 6.9%) | Similar outcomes across vessels |
| Study | LAD Post-PCI Cutoff | Non-LAD Post-PCI Cutoff | Key Findings | Limitations |
|---|---|---|---|---|
| DKCRUSH VII [33] | 0.905 | 0.88 | Higher cutoff for LAD improved prediction; Lower success rate in LAD (59% vs. 85.7%) | High-risk bifurcation lesions |
| Hwang et al. [34] | 0.82 | 0.88 | Lower post-PCI FFR in LAD (0.85 vs. 0.92); TVF in LAD (10.9% vs. 2.5%, HR 4.8), non-LAD (8.0% vs. 1.9%, HR 6.0); AUC: LAD 0.70, non-LAD 0.76 | Observational registry |
| Collet et al. [35] | 0.86 | 0.93 (LCX 0.93 + RCA 0.91) | Lower FFR and prognostic accuracy in LAD; (AUC: 0.52 LAD vs. 0.66 Non-LAD) | Post hoc meta-analysis |
| Trial | Main Result | Vessel-Level Findings (LAD) | Key Point |
|---|---|---|---|
| COMPARE-ACUTE [49] | FFR↓ in event lesions (vs. no event) | FFR in event lesions vs. no event LAD: 0.77 vs. 0.82 (p = 0.002) LCx: 0.83 vs. 0.89 (p < 0.001) RCA: 0.82 vs. 0.87 (p = 0.013) | Lower FFR linked to events; LAD lowest |
| FRAME-AMI [50] | MACEs: Total: 6.3% (FFR) vs. 14.4% (Angio), p = 0.001 LAD: 5.7% (FFR) vs. 14.3% (Angio), p = 0.001 Non-LAD: 7.4% (FFR) vs. 14.5% (Angio), p = 0.081 | LAD vs. Non-LAD Mean FFR: 0.77 vs. 0.83 FFR ≤ 0.80: 62.1% vs. 36.8% | Clear FFR benefit in LAD |
| FULL REVASC [46] | No difference in MACEs over median 4.8 years | HR for MACEs: LAD 0.91, LCx 0.85, RCA 1.16; proximal LAD HR 0.81 (NS) | No FFR benefit overall or by vessel |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, C.-O.; Kim, H.; Koh, J.-S. Fractional Flow Reserve in the Left Anterior Descending Artery. J. Clin. Med. 2025, 14, 5429. https://doi.org/10.3390/jcm14155429
Seo C-O, Kim H, Koh J-S. Fractional Flow Reserve in the Left Anterior Descending Artery. Journal of Clinical Medicine. 2025; 14(15):5429. https://doi.org/10.3390/jcm14155429
Chicago/Turabian StyleSeo, Chang-Ok, Hangyul Kim, and Jin-Sin Koh. 2025. "Fractional Flow Reserve in the Left Anterior Descending Artery" Journal of Clinical Medicine 14, no. 15: 5429. https://doi.org/10.3390/jcm14155429
APA StyleSeo, C.-O., Kim, H., & Koh, J.-S. (2025). Fractional Flow Reserve in the Left Anterior Descending Artery. Journal of Clinical Medicine, 14(15), 5429. https://doi.org/10.3390/jcm14155429