
Transforming Cancer Care: A Narrative Review on Leveraging Artificial Intelligence to Advance Immunotherapy in Underserved Communities

 , , , ,
, , , ,  , and
, and
Abstract
1. Introduction
1.1. A Paradigm Shift in Oncology
1.2. Disparities in Access to Cancer Immunotherapy
1.3. The Promise of Artificial Intelligence in Reducing Disparities
1.4. Expanding Access Through AI-Driven Care Models
1.5. Narrative Review Approach: Literature Search and Selection Strategy
- artificial intelligence” OR “machine learning” OR “deep learning”
- cancer immunotherapy” OR “immune checkpoint inhibitors” OR “tumor microenvironment”
- health disparities” OR “underserved populations” OR “minority health” OR “equity”
- Focused on AI applications in cancer immunotherapy (e.g., biomarker discovery, outcome prediction, treatment optimization).
- Reported outcomes related to model performance, clinical utility, or patient impact.
- Discussed or analyzed demographic variables, population diversity, or implications for underserved communities.
- Published in a peer-reviewed journal or reputable preprint repository.
- Focused solely on traditional (non-immunotherapy) cancer treatments.
- Lacked sufficient methodological detail or performance metrics.
- Were editorials, opinion pieces, or conference abstracts without data.
2. Disparities in Cancer Immunotherapy
2.1. Disparities in Access and Outcomes
2.2. Cognitive Influences on Clinical Decision-Making
2.3. Geographic Distribution of the Healthcare Workforce
2.4. Limited Access to Specialized Services in Medically Isolated Areas
2.5. Transportation Barriers and Continuity of Care
2.6. Gaps in Representation in Clinical Trials and Real-World Data
3. The Role of AI in Addressing Disparities
3.1. AI in Analyzing SES and SDOH
3.2. Predictive Modeling for Side Effects
3.3. Risk Stratification and Tailored Interventions
3.4. Neoantigen Identification Using AI in Underrepresented Populations
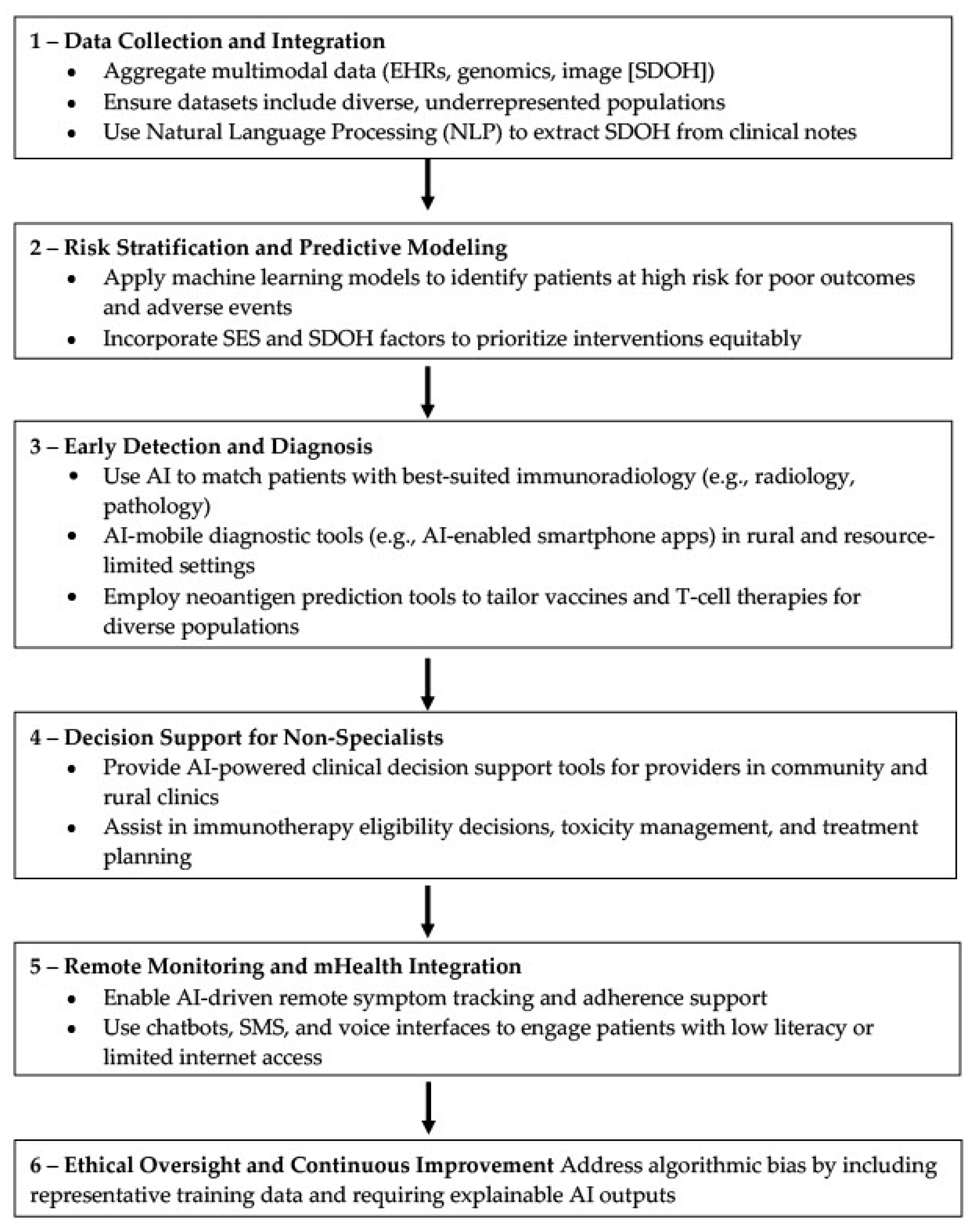
4. Applications of AI to Improve Care Quality
4.1. Natural Language Processing
4.2. Machine Learning and Real Word Evidence
5. Ethical Considerations and Challenges
5.1. Algorithmic Bias
5.2. Privacy
5.3. Need for Transparency
6. Case Studies and Emerging Applications
6.1. The Growing Need for Innovative Solutions in Resource-Limited U.S. Communities
6.2. Smartphone-Enabled Diagnostics and Personal Health Assistants
6.3. Diabetic Monitoring and AI-Enabled Screening Programs
6.4. Community-Level Applications of AI in Public Health
6.5. Considerations for Algorithm Design and Implementation
6.6. Navigating Privacy, Regulation, and Infrastructure Needs
6.7. Conclusion: Realizing the Potential of AI in Expanding Access to Immunotherapy
7. Research Gaps and Future Directions
7.1. Lack of Diverse and Representative Datasets
7.2. Technical Challenges in Multimodal Data Integration
7.3. Limited Clinical Integration and Implementation Science
7.4. Promising Models of Interdisciplinary Collaboration
7.5. Future Priorities for Objective AI Integration
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, A.R.; Devan, A.R.; Nair, B.; Vinod, B.S.; Nath, L.R. Harnessing the Immune System against Cancer: Current Immunotherapy Approaches and Therapeutic Targets. Mol. Biol. Rep. 2021, 48, 8075–8095. [Google Scholar] [CrossRef]
- Sordo-Bahamonde, C.; Lorenzo-Herrero, S.; Gonzalez-Rodriguez, A.P.; Martínez-Pérez, A.; Rodrigo, J.P.; García-Pedrero, J.M.; Gonzalez, S. Chemo-Immunotherapy: A New Trend in Cancer Treatment. Cancers 2023, 15, 2912. [Google Scholar] [CrossRef]
- Hosseinkhani, N.; Derakhshani, A.; Kooshkaki, O.; Abdoli Shadbad, M.; Hajiasgharzadeh, K.; Baghbanzadeh, A.; Safarpour, H.; Mokhtarzadeh, A.; Brunetti, O.; Yue, S.C.; et al. Immune Checkpoints and CAR-T Cells: The Pioneers in Future Cancer Therapies? Int. J. Mol. Sci. 2020, 21, 8305. [Google Scholar] [CrossRef]
- Yarchoan, M.; Gane, E.J.; Marron, T.U.; Perales-Linares, R.; Yan, J.; Cooch, N.; Shu, D.H.; Fertig, E.J.; Kagohara, L.T.; Bartha, G.; et al. Personalized Neoantigen Vaccine and Pembrolizumab in Advanced Hepatocellular Carcinoma: A Phase 1/2 Trial. Nat. Med. 2024, 30, 1044–1053. [Google Scholar] [CrossRef] [PubMed]
- Gargett, T.; Truong, N.T.H.; Gardam, B.; Yu, W.; Ebert, L.M.; Johnson, A.; Yeo, E.C.F.; Wittwer, N.L.; Tapia Rico, G.; Logan, J.; et al. Safety and Biological Outcomes Following a Phase 1 Trial of GD2-Specific CAR-T Cells in Patients with GD2-Positive Metastatic Melanoma and Other Solid Cancers. J. Immunother. Cancer 2024, 12, e008659. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Sun, R.; Shi, B.; Wang, Y.; Di, S.; Luo, H.; Sun, Y.; Li, Z.; Zhou, M.; Jiang, H. Antitumor Efficacy of Chimeric Antigen Receptor T Cells against EGFRvIII-Expressing Glioblastoma in C57BL/6 Mice. Biomed. Pharmacother. Biomed. Pharmacother. 2019, 113, 108734. [Google Scholar] [CrossRef]
- Li, H.; Ding, J.; Lu, M.; Liu, H.; Miao, Y.; Li, L.; Wang, G.; Zheng, J.; Pei, D.; Zhang, Q. CAIX-Specific CAR-T Cells and Sunitinib Show Synergistic Effects Against Metastatic Renal Cancer Models. J. Immunother. 2020, 43, 16–28. [Google Scholar] [CrossRef]
- Winkfield, K.M.; Regnante, J.M.; Miller-Sonet, E.; González, E.T.; Freund, K.M.; Doykos, P.M. Development of an Actionable Framework to Address Cancer Care Disparities in Medically Underserved Populations in the United States: Expert Roundtable Recommendations. JCO Oncol. Pract. 2021, 17, e278–e293. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Wolsiefer, K.; Zestcott, C.A.; Chase, D.; Stone, J. Implicit Bias toward Cervical Cancer: Provider and Training Differences. Gynecol. Oncol. 2019, 153, 80–86. [Google Scholar] [CrossRef]
- Schatz, A.A.; Brooks-Coley, K.; Harrington, E.; Murray, M.S.; Carlson, R.W. Patient, Caregiver, and Oncologist Experiences with and Perceptions of Racial Bias and Discrimination in Cancer Care Delivery. J. Natl. Compr. Cancer Netw. JNCCN 2022, 20, 1092–1098.e2. [Google Scholar] [CrossRef]
- Abreu, A.A.; Murimwa, G.Z.; Farah, E.; Stewart, J.W.; Zhang, L.; Rodriguez, J.; Sweetenham, J.; Zeh, H.J.; Wang, S.C.; Polanco, P.M. Enhancing Readability of Online Patient-Facing Content: The Role of AI Chatbots in Improving Cancer Information Accessibility. J. Natl. Compr. Cancer Netw. JNCCN 2024, 22, e237334. [Google Scholar] [CrossRef]
- Xiong, S.; Fu, Z.; Deng, Z.; Li, S.; Zhan, X.; Zheng, F.; Yang, H.; Liu, X.; Xu, S.; Liu, H.; et al. Machine Learning-Based CT Radiomics Enhances Bladder Cancer Staging Predictions: A Comparative Study of Clinical, Radiomics, and Combined Models. Med. Phys. 2024, 51, 5965–5977. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Cao, B.; Wu, J.; Feng, C. Development and Validation of an Interpretable Machine Learning Prediction Model for Total Pathological Complete Response after Neoadjuvant Chemotherapy in Locally Advanced Breast Cancer: Multicenter Retrospective Analysis. J. Cancer 2024, 15, 5058–5071. [Google Scholar] [CrossRef] [PubMed]
- Montoya, C.; Spieler, B.; Welford, S.M.; Kwon, D.; Pra, A.D.; Lopes, G.; Mihaylov, I.B. Predicting Response to Immunotherapy in Non-Small Cell Lung Cancer- from Bench to Bedside. Front. Oncol. 2023, 13, 1225720. [Google Scholar] [CrossRef]
- Mørk, S.K.; Kadivar, M.; Bol, K.F.; Draghi, A.; Westergaard, M.C.W.; Skadborg, S.K.; Overgaard, N.; Sørensen, A.B.; Rasmussen, I.S.; Andreasen, L.V.; et al. Personalized Therapy with Peptide-Based Neoantigen Vaccine (EVX-01) Including a Novel Adjuvant, CAF®09b, in Patients with Metastatic Melanoma. Oncoimmunology 2022, 11, 2023255. [Google Scholar] [CrossRef]
- Li, J.; Yuan, Y.; Bian, L.; Lin, Q.; Yang, H.; Ma, L.; Xin, L.; Li, F.; Zhang, S.; Wang, T.; et al. A Comparison between Clinical Decision Support System and Clinicians in Breast Cancer. Heliyon 2023, 9, e16059. [Google Scholar] [CrossRef] [PubMed]
- Verdini, N.P.; Bryl, K.L.; Baser, R.E.; Lapen, K.; Mao, J.J.; Gillespie, E.F. Patient-Reported Outcomes as a Recruitment Strategy for Clinical Trial Enrollment. JAMA Oncol. 2024, 10, 784–788. [Google Scholar] [CrossRef]
- Parikh, R.B.; Guido, M.; Girard, A.; Li, Y.; Kolla, L.; Chen, J.; Emanuel, E.J. Human-AI Teams to Improve Accuracy and Timeliness of Oncology Trial Prescreening: Preplanned Interim Analysis of a Randomized Trial. J. Clin. Oncol. 2024, 42, 1524. [Google Scholar] [CrossRef]
- Da’Costa, A.; Teke, J.; Origbo, J.E.; Osonuga, A.; Egbon, E.; Olawade, D.B. AI-Driven Triage in Emergency Departments: A Review of Benefits, Challenges, and Future Directions. Int. J. Med. Inf. 2025, 197, 105838. [Google Scholar] [CrossRef]
- Tyler, S.; Olis, M.; Aust, N.; Patel, L.; Simon, L.; Triantafyllidis, C.; Patel, V.; Lee, D.W.; Ginsberg, B.; Ahmad, H.; et al. Use of Artificial Intelligence in Triage in Hospital Emergency Departments: A Scoping Review. Cureus 2024, 16, e59906. [Google Scholar] [CrossRef]
- Blue, B. Socioeconomic and Racial Disparity in Chimeric Antigen Receptor T Cell (CART)Therapy Access. Transplant. Cell. Ther. 2022, 28, 345–346. [Google Scholar] [CrossRef]
- Fiscella, K.; Sanders, M.R. Racial and Ethnic Disparities in the Quality of Health Care. Annu. Rev. Public Health 2016, 37, 375–394. [Google Scholar] [CrossRef] [PubMed]
- Naylor, K.B.; Tootoo, J.; Yakusheva, O.; Shipman, S.A.; Bynum, J.P.W.; Davis, M.A. Geographic Variation in Spatial Accessibility of U.S. Healthcare Providers. PLoS ONE 2019, 14, e0215016. [Google Scholar] [CrossRef]
- Syed, S.T.; Gerber, B.S.; Sharp, L.K. Traveling towards Disease: Transportation Barriers to Health Care Access. J. Community Health 2013, 38, 976–993. [Google Scholar] [CrossRef]
- Heiat, A.; Gross, C.P.; Krumholz, H.M. Representation of the Elderly, Women, and Minorities in Heart Failure Clinical Trials. Arch. Intern. Med. 2002, 162, 1682–1688. [Google Scholar] [CrossRef]
- Duma, N.; Vera Aguilera, J.; Paludo, J.; Haddox, C.L.; Gonzalez Velez, M.; Wang, Y.; Leventakos, K.; Hubbard, J.M.; Mansfield, A.S.; Go, R.S.; et al. Representation of Minorities and Women in Oncology Clinical Trials: Review of the Past 14 Years. J. Oncol. Pract. 2018, 14, e1–e10. [Google Scholar] [CrossRef]
- Kwiatkowski, K.; Coe, K.; Bailar, J.C.; Swanson, G.M. Inclusion of Minorities and Women in Cancer Clinical Trials, a Decade Later: Have We Improved? Cancer 2013, 119, 2956–2963. [Google Scholar] [CrossRef]
- Abbott, E.E.; Apakama, D.; Richardson, L.D.; Chan, L.; Nadkarni, G.N. Leveraging Artificial Intelligence and Data Science for Integration of Social Determinants of Health in Emergency Medicine: Scoping Review. JMIR Med. Inform. 2024, 12, e57124. [Google Scholar] [CrossRef]
- Juhn, Y.J.; Ryu, E.; Wi, C.-I.; King, K.S.; Malik, M.; Romero-Brufau, S.; Weng, C.; Sohn, S.; Sharp, R.R.; Halamka, J.D. Assessing Socioeconomic Bias in Machine Learning Algorithms in Health Care: A Case Study of the HOUSES Index. J. Am. Med. Inform. Assoc. JAMIA 2022, 29, 1142–1151. [Google Scholar] [CrossRef] [PubMed]
- Carroll, N.W.; Jones, A.; Burkard, T.; Lulias, C.; Severson, K.; Posa, T. Improving Risk Stratification Using AI and Social Determinants of Health. Am. J. Manag. Care 2022, 28, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Huber, F.; Arnaud, M.; Kraemer, A.I.; Altimiras, E.R.; Michaux, J.; Taillandier-Coindard, M.; Chiffelle, J.; Murgues, B.; Gehret, T.; et al. Machine Learning Methods and Harmonized Datasets Improve Immunogenic Neoantigen Prediction. Immunity 2023, 56, 2650–2663.e6. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Li, Y.; Zhu, X.; He, Y.; Wu, Y.; Ying, T.; Xie, Z. Artificial Intelligence in Cancer Immunotherapy: Applications in Neoantigen Recognition, Antibody Design and Immunotherapy Response Prediction. Semin. Cancer Biol. 2023, 91, 50–69. [Google Scholar] [CrossRef]
- Cai, Y.; Chen, R.; Gao, S.; Li, W.; Liu, Y.; Su, G.; Song, M.; Jiang, M.; Jiang, C.; Zhang, X. Artificial Intelligence Applied in Neoantigen Identification Facilitates Personalized Cancer Immunotherapy. Front. Oncol. 2022, 12, 1054231. [Google Scholar] [CrossRef]
- Eysenbach, G. The Role of ChatGPT, Generative Language Models, and Artificial Intelligence in Medical Education: A Conversation with ChatGPT and a Call for Papers. JMIR Med. Educ. 2023, 9, e46885. [Google Scholar] [CrossRef]
- Al Shamsi, H.; Almutairi, A.G.; Al Mashrafi, S.; Al Kalbani, T. Implications of Language Barriers for Healthcare: A Systematic Review. Oman Med. J. 2020, 35, e122. [Google Scholar] [CrossRef]
- Fatima, A.; Shafique, M.A.; Alam, K.; Fadlalla Ahmed, T.K.; Mustafa, M.S. ChatGPT in Medicine: A Cross-Disciplinary Systematic Review of ChatGPT’s (Artificial Intelligence) Role in Research, Clinical Practice, Education, and Patient Interaction. Medicine 2024, 103, e39250. [Google Scholar] [CrossRef]
- Morrow, E.; Zidaru, T.; Ross, F.; Mason, C.; Patel, K.D.; Ream, M.; Stockley, R. Artificial Intelligence Technologies and Compassion in Healthcare: A Systematic Scoping Review. Front. Psychol. 2023, 13, 971044. [Google Scholar] [CrossRef] [PubMed]
- Milne-Ives, M.; De Cock, C.; Lim, E.; Shehadeh, M.H.; De Pennington, N.; Mole, G.; Normando, E.; Meinert, E. The Effectiveness of Artificial Intelligence Conversational Agents in Health Care: Systematic Review. J. Med. Internet Res. 2020, 22, e20346. [Google Scholar] [CrossRef]
- Klann, J.G.; Szolovits, P. An Intelligent Listening Framework for Capturing Encounter Notes from a Doctor-Patient Dialog. BMC Med. Inform. Decis. Mak. 2009, 9 (Suppl. 1), S3. [Google Scholar] [CrossRef] [PubMed]
- Deliberato, R.O.; Celi, L.A.; Stone, D.J. Clinical Note Creation, Binning, and Artificial Intelligence. JMIR Med. Inform. 2017, 5, e24. [Google Scholar] [CrossRef]
- Peterson Health Technology Institute AI Taskforce. Adoption of Artificial Intelligence in Healthcare Delivery Systems: Early Applications and Impacts; Peterson Health Technology Institute: New York, NY, USA, 2025. [Google Scholar]
- Lee, C.; Britto, S.; Diwan, K. Evaluating the Impact of Artificial Intelligence (AI) on Clinical Documentation Efficiency and Accuracy Across Clinical Settings: A Scoping Review. Cureus 2024, 16, e73994. [Google Scholar] [CrossRef] [PubMed]
- Goss, F.R.; Blackley, S.V.; Ortega, C.A.; Kowalski, L.T.; Landman, A.B.; Lin, C.-T.; Meteer, M.; Bakes, S.; Gradwohl, S.C.; Bates, D.W.; et al. A Clinician Survey of Using Speech Recognition for Clinical Documentation in the Electronic Health Record. Int. J. Med. Inf. 2019, 130, 103938. [Google Scholar] [CrossRef] [PubMed]
- Kernberg, A.; Gold, J.A.; Mohan, V. Using ChatGPT-4 to Create Structured Medical Notes From Audio Recordings of Physician-Patient Encounters: Comparative Study. J. Med. Internet Res. 2024, 26, e54419. [Google Scholar] [CrossRef] [PubMed]
- Toole, J.; Kohansieh, M.; Khan, U.; Romero, S.; Ghali, M.; Zeltser, R.; Makaryus, A.N. Does Your Patient Understand Their Treatment Plan? Factors Affecting Patient Understanding of Their Medical Care Treatment Plan in the Inpatient Setting. J. Patient Exp. 2020, 7, 1151–1157. [Google Scholar] [CrossRef]
- Jin, Q.; Wang, Z.; Floudas, C.S.; Chen, F.; Gong, C.; Bracken-Clarke, D.; Xue, E.; Yang, Y.; Sun, J.; Lu, Z. Matching Patients to Clinical Trials with Large Language Models. Nat. Commun. 2024, 15, 9074. [Google Scholar] [CrossRef]
- Calaprice-Whitty, D.; Galil, K.; Salloum, W.; Zariv, A.; Jimenez, B. Improving Clinical Trial Participant Prescreening with Artificial Intelligence (AI): A Comparison of the Results of AI-Assisted vs Standard Methods in 3 Oncology Trials. Ther. Innov. Regul. Sci. 2020, 54, 69–74. [Google Scholar] [CrossRef]
- Rajwal, S.; Zhang, Z.; Chen, Y.; Rogers, H.; Sarker, A.; Xiao, Y. Applications of Natural Language Processing and Large Language Models for Social Determinants of Health: Protocol for a Systematic Review. JMIR Res. Protoc. 2025, 14, e66094. [Google Scholar] [CrossRef]
- Jerfy, A.; Selden, O.; Balkrishnan, R. The Growing Impact of Natural Language Processing in Healthcare and Public Health. Inq. J. Med. Care Organ. Provis. Financ. 2024, 61, 469580241290095. [Google Scholar] [CrossRef]
- Kelley, K. How Does AI Work? A Beginner’s Guide; BlueDot Impact: London, UK, 2024. [Google Scholar]
- Jain, R.; Singh, M.; Rao, A.R.; Garg, R. Predicting Hospital Length of Stay Using Machine Learning on a Large Open Health Dataset. BMC Health Serv. Res. 2024, 24, 860. [Google Scholar] [CrossRef]
- Symum, H.; Zayas-Castro, J.L. Prediction of Chronic Disease-Related Inpatient Prolonged Length of Stay Using Machine Learning Algorithms. Healthc. Inform. Res. 2020, 26, 20–33. [Google Scholar] [CrossRef]
- Nordling, L. A Fairer Way Forward for AI in Health Care. Nature 2019, 573, S103–S105. [Google Scholar] [CrossRef]
- Álvarez-Machancoses, Ó.; DeAndrés Galiana, E.J.; Cernea, A.; Fernández Sánchez De La Viña, J.; Fernández-Martínez, J.L. On the Role of Artificial Intelligence in Genomics to Enhance Precision Medicine. Pharmacogenom. Pers. Med. 2020, 13, 105–119. [Google Scholar] [CrossRef]
- Duong, D.; Solomon, B.D. Artificial Intelligence in Clinical Genetics. Eur. J. Hum. Genet. 2025, 33, 281–288. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Summary of the HIPAA Privacy Rule; U.S. Department of Health and Human Services: Washington, DC, USA, 2025.
- Vilhekar, R.S.; Rawekar, A. Artificial Intelligence in Genetics. Cureus 2024, 16, e52035. [Google Scholar] [CrossRef]
- Sullivan, H.R.; Schweikart, S.J. Are Current Tort Liability Doctrines Adequate for Addressing Injury Caused by AI? AMA J. Ethics 2019, 21, E160–E166. [Google Scholar] [CrossRef]
- Bhatt, P.; Liu, J.; Gong, Y.; Wang, J.; Guo, Y. Emerging Artificial Intelligence-Empowered mHealth: Scoping Review. JMIR mHealth uHealth 2022, 10, e35053. [Google Scholar] [CrossRef] [PubMed]
- Maleki Varnosfaderani, S.; Forouzanfar, M. The Role of AI in Hospitals and Clinics: Transforming Healthcare in the 21st Century. Bioengineering 2024, 11, 337. [Google Scholar] [CrossRef] [PubMed]
- van Veen, T.; Binz, S.; Muminovic, M.; Chaudhry, K.; Rose, K.; Calo, S.; Rammal, J.-A.; France, J.; Miller, J.B. Potential of Mobile Health Technology to Reduce Health Disparities in Underserved Communities. West. J. Emerg. Med. 2019, 20, 799–802. [Google Scholar] [CrossRef]
- Topol, E.J. High-Performance Medicine: The Convergence of Human and Artificial Intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Mackenzie, S.C.; Sainsbury, C.A.R.; Wake, D.J. Diabetes and Artificial Intelligence beyond the Closed Loop: A Review of the Landscape, Promise and Challenges. Diabetologia 2024, 67, 223–235. [Google Scholar] [CrossRef]
- Bajwa, J.; Munir, U.; Nori, A.; Williams, B. Artificial Intelligence in Healthcare: Transforming the Practice of Medicine. Future Healthc. J. 2021, 8, e188–e194. [Google Scholar] [CrossRef]
- d’Elia, A.; Gabbay, M.; Rodgers, S.; Kierans, C.; Jones, E.; Durrani, I.; Thomas, A.; Frith, L. Artificial Intelligence and Health Inequities in Primary Care: A Systematic Scoping Review and Framework. Fam. Med. Community Health 2022, 10, e001670. [Google Scholar] [CrossRef]
- Green, B.L.; Murphy, A.; Robinson, E. Accelerating Health Disparities Research with Artificial Intelligence. Front. Digit. Health 2024, 6, 1330160. [Google Scholar] [CrossRef]
- George, S.; Duran, N.; Norris, K. A Systematic Review of Barriers and Facilitators to Minority Research Participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. Am. J. Public Health 2014, 104, e16–e31. [Google Scholar] [CrossRef]
- D’Amiano, A.J.; Cheunkarndee, T.; Azoba, C.; Chen, K.Y.; Mak, R.H.; Perni, S. Transparency and Representation in Clinical Research Utilizing Artificial Intelligence in Oncology: A Scoping Review. Cancer Med. 2025, 14, e70728. [Google Scholar] [CrossRef]
- Lipkova, J.; Chen, R.J.; Chen, B.; Lu, M.Y.; Barbieri, M.; Shao, D.; Vaidya, A.J.; Chen, C.; Zhuang, L.; Williamson, D.F.K.; et al. Artificial Intelligence for Multimodal Data Integration in Oncology. Cancer Cell 2022, 40, 1095–1110. [Google Scholar] [CrossRef]
- Sun, Y.; Song, N.; Han, Y.; Ding, S. Organic Base-Facilitated Thiol-Thioalkyne Reaction with Exclusive Regio- and Stereoselectivity. J. Org. Chem. 2023, 88, 15130–15141. [Google Scholar] [CrossRef] [PubMed]
- Miller, G. Drug Targeting. Breaking down Barriers. Science 2002, 297, 1116–1118. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.J.; Lu, M.Y.; Williamson, D.F.K.; Chen, T.Y.; Lipkova, J.; Noor, Z.; Shaban, M.; Shady, M.; Williams, M.; Joo, B.; et al. Pan-Cancer Integrative Histology-Genomic Analysis via Multimodal Deep Learning. Cancer Cell 2022, 40, 865–878.e6. [Google Scholar] [CrossRef] [PubMed]
- Mahootiha, M.; Tak, D.; Ye, Z.; Zapaishchykova, A.; Likitlersuang, J.; Climent Pardo, J.C.; Boyd, A.; Vajapeyam, S.; Chopra, R.; Prabhu, S.P.; et al. Multimodal Deep Learning Improves Recurrence Risk Prediction in Pediatric Low-Grade Gliomas. Neuro-Oncol. 2025, 27, 277–290. [Google Scholar] [CrossRef]
- Macheka, S.; Ng, P.Y.; Ginsburg, O.; Hope, A.; Sullivan, R.; Aggarwal, A. Prospective Evaluation of Artificial Intelligence (AI) Applications for Use in Cancer Pathways Following Diagnosis: A Systematic Review. BMJ Oncol. 2024, 3, e000255. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.; Liu, X.; Denniston, A.; Esteva, A.; Ko, J.; Daneshjou, R.; Chan, A.-W. SPIRIT-AI and CONSORT-AI Working Group Raising the Bar for Randomized Trials Involving Artificial Intelligence: The SPIRIT-Artificial Intelligence and CONSORT-Artificial Intelligence Guidelines. J. Investig. Dermatol. 2021, 141, 2109–2111. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Lin, X.; Hong, Y.; Li, Y.; Li, Y.; Chen, W.-T.; Chen, W. The Feasibility and Cost-Effectiveness of Implementing Mobile Low-Dose Computed Tomography with an AI-Based Diagnostic System in Underserved Populations. BMC Cancer 2025, 25, 345. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| AI Tool/Model | Application | Key Features | Performance Metrics | Impact on Disparities |
|---|---|---|---|---|
| Natural Language Processing (NLP) | Extracting clinical notes, chatbot interfaces | Multilingual processing, unstructured data analysis | Context-specific; varies by implementation | Improves access via multilingual support and outreach to diverse populations |
| Machine Learning | Disease diagnosis, outcome prediction | Supervised/unsupervised learning, pattern recognition | Accuracy: variable; e.g., AUC > 0.80 in some cases | Can reduce care variability; risks perpetuating bias if training data lacks representation |
| Predictive Analytics | Risk stratification, resource allocation | Statistical modeling with clinical + social data | ROC AUC: 0.75–0.90 typically | Enables proactive interventions when SDOH data are included |
| Computer Vision | Radiology, histopathology, dermatology | CNNs, image segmentation and classification | AUC > 0.90 in radiology/dermatology | May underperform on darker skin tones if training datasets lack diversity |
| Recommendation Algorithms | Clinical decision support, personalized treatments | Knowledge graphs, EHR integration | Concordance with clinicians: 70–90% | Can promote equity in care delivery; risks disparities without transparency |
| Speech Recognition | Patient interaction, low-literacy communication | Voice-to-text AI, language understanding | Word error rate varies by accent/language | Enhances access for patients with low literacy or physical disabilities |
| PathAI | Histopathology image analysis | CNN-based H&E tissue interpretation | AUC: 0.93 (breast cancer); accuracy: ~90% | Limited demographic testing; currently focused on TCGA datasets |
| DeepSurv | Prognostic modeling | Deep neural Cox model for survival prediction | C-index: 0.74–0.82 | Limited validation in underserved populations |
| Tempus xT Platform | Genomic profiling + therapy response | AI-driven NGS + clinical decision support | Clinical utility: ~85% actionable findings | Limited data from diverse or global cohorts |
| Lunit SCOPE IO | Immune microenvironment profiling | AI-based spatial tissue analysis | AUC: 0.89 (NSCLC); specificity: 88% | Needs broader population testing |
| Ethical Challenge | Example | Proposed Solution |
|---|---|---|
| Algorithmic Bias | Higher false-negative rates in AI-based skin cancer detection on darker skin tones | Incorporate diverse datasets and perform subgroup performance validation |
| Data Diversity | Underrepresentation of rural and minority populations in training data | Engage community stakeholders and build inclusive data collection protocols |
| Transparency | Black-box AI systems in clinical decision-making | Mandate explainable AI tools and clinician education on AI interpretation |
| Privacy Concerns | Use of patient data without clear consent or anonymization | Establish strong governance frameworks and patient-centered data sharing policies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasquez, V.M., Jr.; McCabe, M.; McKee, J.C.; Siby, S.; Hussain, U.; Faizuddin, F.; Sheikh, A.; Nguyen, T.; Mayer, G.; Grier, J.; et al. Transforming Cancer Care: A Narrative Review on Leveraging Artificial Intelligence to Advance Immunotherapy in Underserved Communities. J. Clin. Med. 2025, 14, 5346. https://doi.org/10.3390/jcm14155346
Vasquez VM Jr., McCabe M, McKee JC, Siby S, Hussain U, Faizuddin F, Sheikh A, Nguyen T, Mayer G, Grier J, et al. Transforming Cancer Care: A Narrative Review on Leveraging Artificial Intelligence to Advance Immunotherapy in Underserved Communities. Journal of Clinical Medicine. 2025; 14(15):5346. https://doi.org/10.3390/jcm14155346
Chicago/Turabian StyleVasquez, Victor M., Jr., Molly McCabe, Jack C. McKee, Sharon Siby, Usman Hussain, Farah Faizuddin, Aadil Sheikh, Thien Nguyen, Ghislaine Mayer, Jennifer Grier, and et al. 2025. "Transforming Cancer Care: A Narrative Review on Leveraging Artificial Intelligence to Advance Immunotherapy in Underserved Communities" Journal of Clinical Medicine 14, no. 15: 5346. https://doi.org/10.3390/jcm14155346
APA StyleVasquez, V. M., Jr., McCabe, M., McKee, J. C., Siby, S., Hussain, U., Faizuddin, F., Sheikh, A., Nguyen, T., Mayer, G., Grier, J., Dhandayuthapani, S., Gadad, S. S., & Chacon, J. (2025). Transforming Cancer Care: A Narrative Review on Leveraging Artificial Intelligence to Advance Immunotherapy in Underserved Communities. Journal of Clinical Medicine, 14(15), 5346. https://doi.org/10.3390/jcm14155346