
Dry Needling for Tension-Type Headache: A Scoping Review on Intervention Procedures, Muscle Targets, and Outcomes

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Identifying the Research Question
- What diagnostic criteria have been used to identify the presence or absence of trigger points in the target muscles for dry needling in patients with tension-type headache?
- What specific methodology has been applied in the administration of dry needling interventions?
- What are the potential adverse effects or unwanted reactions reported following dry needling application in muscles related to tension-type headache?
2.2. Identifying Relevant Studies
2.2.1. Eligibility Criteria
- Studies addressing tension-type headache as the primary diagnosis;
- Studies evaluating dry needling interventions, applied alone or as part of a combined treatment (provided the effect of dry needling is specified);
- Studies reporting the targeted muscles, diagnostic criteria for muscles, and/or characteristics of the dry needling protocol (frequency, duration, technique, adverse effects, or unwanted reactions);
- Articles published in English, French, or Spanish;
- Quantitative or mixed-methods studies: clinical trials, quasi-experimental studies, case reports, and case series;
- No restriction on the year of publication.
- Studies that do not clearly differentiate dry needling from other techniques;
- Studies where tension-type headache is not the primary diagnosis or is unspecified;
- Systematic reviews, meta-analyses, letters to the editor, editorials, or commentaries;
- Studies conducted on animals or non-human models.
2.2.2. Information Sources
2.2.3. Search Strategy
- PubMed: Used MeSH terms (“Dry Needling”[MeSH Terms] OR “Dry Needling”[Title/Abstract]) AND (“Headache, Tension-Type”[MeSH Terms] OR “tension-type headache”[Title/Abstract] OR “headache”[Title/Abstract] OR “cervicogenic headache”[Title/Abstract]) AND (“Myofascial Pain Syndromes”[MeSH Terms] OR “trigger points”[Title/Abstract])
- Embase: Used EMTREE terms and synonyms (‘dry needling’/exp OR ‘dry needling’) AND (‘tension-type headache’/exp OR ‘tension-type headache’ OR ‘headache’ OR ‘cervicogenic headache’) AND (‘myofascial trigger point’/exp OR ‘trigger point’)
- Web of Science: Used the Topic (TS) field for free-text search:
- TS = (“dry needling” OR “intramuscular stimulation”) AND
- TS = (“tension-type headache” OR “tension headache” OR “TTH” OR “headache” OR “cervicogenic headache”) AND
- TS = (“myofascial trigger points” OR “trigger points” OR “myofascial pain”)
- Scopus: TITLE-ABS-KEY(“dry needling” OR “intramuscular stimulation”) AND
- TITLE-ABS-KEY(“tension-type headache” OR “tension headache” OR “TTH” OR “headache” OR “cervicogenic headache”) AND
- TITLE-ABS-KEY(“myofascial trigger points” OR “trigger points” OR “myofascial pain”)
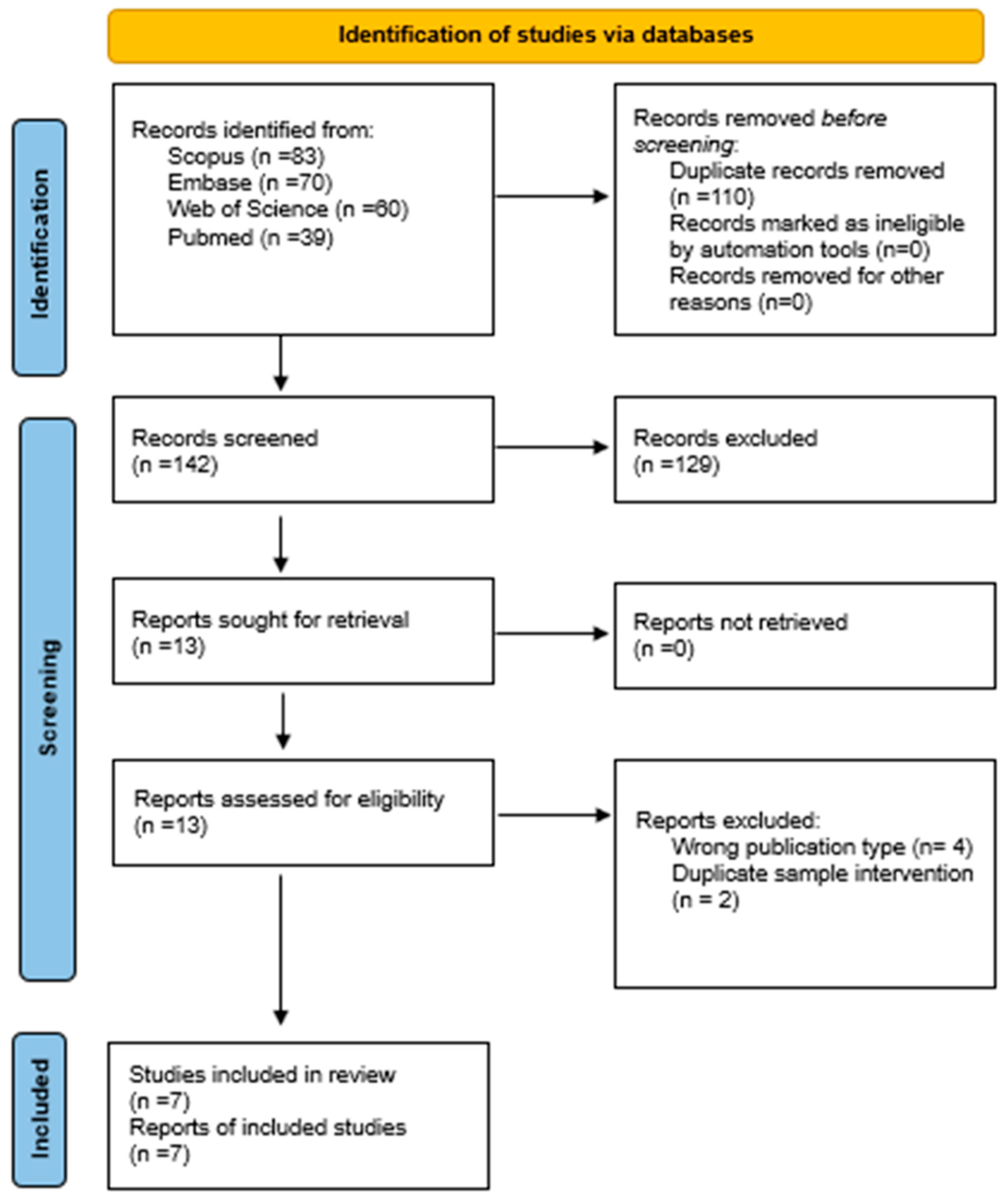
2.3. Study Selection
2.4. Data Charting
2.4.1. Data Extraction
2.4.2. Extracted Variables
- Study characteristics: author, year, country, study design;
- Participant characteristics: headache intensity and location, sample size, age, sex;
- Target muscles;
- Diagnostic criteria;
- Characteristics of dry needling interventions: technique, frequency, duration;
- Adverse effects or unwanted reactions.
2.5. Collating, Summarizing, and Reporting the Results
3. Results
3.1. Study and Participant Characteristics
3.1.1. Diagnostic Criteria for TTH
3.1.2. Intensity, Frequency, and Duration of Headache
3.2. Intervention Characteristics
3.2.1. Target Muscles
3.2.2. Diagnostic Criteria
3.2.3. DN Intervention Characteristics
3.2.4. Outcomes
3.2.5. Adverse Effects or Unwanted Reactions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2133–2161.
- Meng, W.; Sui, L. Headache disorders: A persistent public health challenge for the under 50s. Front. Neurol. 2024, 15, 1501749. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef] [PubMed]
- Satapathy, P.; Chauhan, S.; Gaidhane, S.; Bishoyi, A.K.; Priya, G.P.; Jayabalan, K.; Mishra, S.; Sharma, S.; Bushi, G.; Shabil, M.; et al. Trends in migraine and tension-type headaches in South Asia: Findings from the Global Burden of Disease Study 2021 (1990–2021). Front. Neurol. 2025, 16, 1514712. [Google Scholar] [CrossRef]
- Arendt-Nielsen, L.; Castaldo, M.; Mechelli, F.; Fernández-de-Las-Peñas, C. Muscle Triggers as a Possible Source of Pain in a Subgroup of Tension-type Headache Patients? Clin. J. Pain. 2016, 32, 711–718. [Google Scholar] [CrossRef]
- Bendtsen, L.; Fernández-de-la-Peñas, C. The Role of Muscles in Tension-Type Headache. Curr. Pain. Headache Rep. 2011, 15, 451–458. [Google Scholar] [CrossRef]
- de Tommaso, M.; Fernández-de-Las-Penas, C. Tension Type Headache. Curr. Rheumatol. Rev. 2016, 12, 127–139. [Google Scholar] [CrossRef]
- Belvís, R.; Irimia, P.; Seijo-Fernández, F.; Paz, J.; García-March, G.; Santos-Lasaosa, S.; Latorre, G.; González-Oria, C.; Rodríguez, R.; Pozo-Rosich, P.; et al. Neuromodulation in headache and craniofacial neuralgia: Guidelines from the Spanish Society of Neurology and the Spanish Society of Neurosurgery. Neurologia 2020, 36, 61–79. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Cuadrado, M.; Arendt-Nielsen, L.; Simons, D.; Pareja, J. Myofascial Trigger Points and Sensitization: An Updated Pain Model for Tension-Type Headache. Cephalalgia 2007, 27, 383–393. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Madeleine, P.; Caminero, A.; Cuadrado, M.; Arendt-Nielsen, L.; Pareja, J. Generalized Neck-Shoulder Hyperalgesia in Chronic Tension-Type Headache and Unilateral Migraine Assessed by Pressure Pain Sensitivity Topographical Maps of the Trapezius Muscle. Cephalalgia 2010, 30, 77–86. [Google Scholar] [CrossRef]
- Arias-Buría, J.L.; Martín-Saborido, C.; Cleland, J.; Koppenhaver, S.L.; Plaza-Manzano, G.; Fernández-de-las-Peñas, C. Cost-effectiveness Evaluation of the Inclusion of Dry Needling into an Exercise Program for Subacromial Pain Syndrome: Evidence from a Randomized Clinical Trial. Pain Med. 2018, 19, 2336–2347. [Google Scholar] [CrossRef]
- Brady, S.; McEvoy Johnson Dommerholt Jan Doody, C. Adverse events following trigger point dry needling: A prospective survey of chartered physiotherapists. J. Man. Manip. Ther. 2014, 22, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Justes, D.; Yarzábal-Rodríguez, R.; Doménech-García, V.; Herrero, P.; Bellosta-López, P. Effectiveness of dry needling for headache: A systematic review. Neurologia 2022, 37, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Gattie, E.; Cleland, J.A.; Snodgrass, S. The Effectiveness of Trigger Point Dry Needling for Musculoskeletal Conditions by Physical Therapists: A Systematic Review and Meta-analysis. J. Orthop. Sports Phys. Ther. 2017, 47, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar]
- de Abreu Venancio, R.; Pereira, G.; Francisco, A.; Zamperini, C. Botulinum Toxin, Lidocaine, and Dry-Needling Injections in Patients with Myofascial Pain and Headaches. CRANIO® 2009, 27, 46–53. [Google Scholar] [CrossRef]
- Gagnon, P.; Dunning, J.; Bliton, P.; Charlebois, C.; Henry, N.; Gorby, P.; Mourad, F. Dry needling in the management of chronic tension-type headache associated with levator scapulae syndrome: A case report. Clin. Case Rep. 2024, 12, e8858. [Google Scholar] [CrossRef]
- Gildir, S.; Tüzün, E.H.; Eroğlu, G.; Eker, L. A randomized trial of trigger point dry needling versus sham needling for chronic tension-type headache. Medicine 2019, 98, e14520. [Google Scholar] [CrossRef]
- Issa, T.S.; Huijbregts, P.A. Physical Therapy Diagnosis and Management of a Patient with Chronic Daily Headache: A Case Report. J. Man. Manip. Ther. 2006, 14, 88E–123E. [Google Scholar] [CrossRef]
- Kamali, F.; Mohamadi, M.; Fakheri, L.; Mohammadnejad, F. Dry needling versus friction massage to treat tension type headache: A randomized clinical trial. J. Bodyw. Mov. Ther. 2019, 23, 89–93. [Google Scholar] [CrossRef]
- Karakurum, B.; Karaalin, O.; Coskun, O.; Dora, B.; Uçler, S.; Inan, L. The “dry-needle technique”: Intramuscular stimulation in tension-type headache. Cephalalgia 2001, 21, 813–817. [Google Scholar] [CrossRef] [PubMed]
- Monti-Ballano, S.; Márquez-Gonzalvo, S.; Lucha-López, M.O.; Ferrández-Laliena, L.; Vicente-Pina, L.; Sánchez-Rodríguez, R.; Tricás-Vidal, H.J.; Tricás-Moreno, J.M. Effects of Dry Needling on Active Myofascial Trigger Points and Pain Intensity in Tension-Type Headache: A Randomized Controlled Study. J. Pers. Med. 2024, 14, 332. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.M.; Fernández-de-las-Peñas, C.F.; Finnegan, M.; Freeman, J.L. Dor e Disfunção Miofascial de Travell, Simons & Simons, 3rd ed.; Manual de Pontos-Gatilho; Artmed Editora: Rio Grande do Sul, Brazil, 2020; 998p. [Google Scholar]
- Fernández-de-Las-Peñas, C.; Ge, H.Y.; Arendt-Nielsen, L.; Cuadrado, M.L.; Pareja, J.A. The local and referred pain from myofascial trigger points in the temporalis muscle contributes to pain profile in chronic tension-type headache. Clin. J. Pain 2007, 23, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Simons, D.; Cuadrado, M.L.; Pareja, J. The role of myofascial trigger points in musculoskeletal pain syndromes of the head and neck. Curr. Pain Headache Rep. 2007, 11, 365–372. [Google Scholar] [CrossRef]
- Gunn, C.C. The Gunn Approach to the Treatment of Chronic Pain: Intramuscular Stimulation for Myofascial Pain of Radiculopathic Origin; Churchill Livingstone: London, UK, 1996; 192p. [Google Scholar]
- Fernández-de-Las-Peñas, C.; Florencio, L.L.; Plaza-Manzano, G.; Arias-Buría, J.L. Clinical Reasoning Behind Non-Pharmacological Interventions for the Management of Headaches: A Narrative Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 4126. [Google Scholar] [CrossRef]
- Steen, J.P.; Jaiswal, K.S.; Kumbhare, D. Myofascial Pain Syndrome: An Update on Clinical Characteristics, Etiopathogenesis, Diagnosis, and Treatment. Muscle Nerve 2025, 71, 889–910. [Google Scholar] [CrossRef]
- Zhai, T.; Jiang, F.; Chen, Y.; Wang, J.; Feng, W. Advancing musculoskeletal diagnosis and therapy: A comprehensive review of trigger point theory and muscle pain patterns. Front. Med. 2024, 11, 1433070. [Google Scholar] [CrossRef]
- American Physical Therapy Association. Guide to Physical Therapist Practice. Second Edition. American Physical Therapy Association. Phys. Ther. 2001, 81, 9–746.
- Lee, J.H.; Lee, H.; Jo, D.J. An acute cervical epidural hematoma as a complication of dry needling. Spine 2011, 36, E891–E893. [Google Scholar] [CrossRef]
- Hong, C.Z. Lidocaine injection versus dry needling to myofascial trigger point: The importance of the local twitch response. Am. J. Phys. Med. Rehabil. 1994, 73, 256–263. [Google Scholar] [CrossRef]
- Tough, E.A.; White, A.R.; Cummings, T.M.; Richards, S.H.; Campbell, J.L. Acupuncture and dry needling in the management of myofascial trigger point pain: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Pain. 2009, 13, 3–10. [Google Scholar] [CrossRef]
- Dommerholt, J.; Fernández-de-las-Peñas, C. (Eds.) Trigger Point Dry Needling: An Evidence and Clinical-Based Approach; Churchill Livingstone; Elsevier: Amsterdam, The Netherlands, 2013; 258p. [Google Scholar]
- Taşoğlu, Ö.; Şahin Onat, Ş.; Bölük, H.; Taşoğlu, İ.; Özgirgin, N. Comparision of two different dry-needling techniques in the treatment of myofascial pain syndrome. J. Turk. Soc. Algol. 2017, 29, 9–16. [Google Scholar]

{kind=link}
| Author, Year, Country | Study Design | Sample Size (N) Gender (F/M) Age | Intensity, Frequency and Duration Headache | Location Headache |
|---|---|---|---|---|
| De Abreu Venancio et al., 2009 Brazil [19] | RCT (G1: dry needling G2: lidocaine G3: botulinum toxin) | N = 45 40 F/5 M 18–65 years | Symptom Severity Index (SSI) = three subscales of pain: frequency, intensity, duration. SSI (pretreatment–posttreatment): G1: 0.5-0.3 G2: 0.6-0.4 G3: 0.4-0.4 | Orofacial or cervical region |
| Gagnon et al., 2024 USA [20] | A case report | N = 1 1 M/0 F 63 years | Intensity (cm of VAS): Pretreatment: 6 Posttreatment session 1: 3 Posttreatment session 3: 1 Posttreatment session 5: 0 Frequency: Not specified Duration: Not specified | Near the medial aspect of the superior angle of the scapula, bilaterally and progressively radiating upward toward the occiput |
| Gildir et al., 2019 Turkey [21] | RCT (IG: dry needling CG: sham dry needling) | IG: N = 80 41 F/39 M 36.7 years CG: N = 80 44 F/39 M 36 years | (Pretreatment- posttreatment- follow up) Intensity (cm of VAS): IG: 4.5-0.7-0.9 CG: 4.6-4.6-4.9 Frequency (days/month): IG: 18.5-3.8-4.9 CG: 18-7.9-16.3 Duration (hours/day): IG: 3.9-0.7-0.7 CG: 3.8-3.9-4.1 | Not specified |
| Issa et Huijbregts, 2006 USA [22] | A case report | N = 1 1 F/0 M 48 years | Intensity (pretreatment–posttreatment): severe–mild Frequency (pretreatment–posttreatment): 1/week- 1 to 4/month Duration: 4–72 h | Bilateral frontal head region, left cheek and jaw region, bilateral suboccipital, lower neck, and left back of neck |
| Kamali et al., 2019 Iran [23] | RCT (IG: dry needling CG: friction massages) | IG: N = 20 16 F/4 M 37.4 years CG: N = 20 19 F/1 M 33.7 years | Intensity (pretreatment–posttreatment): IG: 8-5 (VAS) CG: 9.5-5.3 (VAS) Frequency (pretreatment–posttreatment): IG: 5-3.1 (day/week) CG: 7-4.2 (day/week) Duration: not specified | Not specified |
| Karakurum et al., 2001 Turkey [24] | RCT (IG: dry needling; CG: subcutaneous insertions) | IG: N = 15 15 F/0 M 28.4 years CG: N = 15 15 F/0 M 27.9 years | Frequency: IG: 29.6 days/month CG: 25.2 days/ month Headache index = intensity × days (pretreatment–posttreatment): IG: 30.4-10.8 CG: 37.4-15.4 Muscle tenderness = palpating the neck muscles (pretreatment–posttreatment: IG: 1.67-0.6 CG: 1.67-1.47 Duration: not specified | Not specified |
| Monti-Ballano et al., 2019 Spain [25] | RCT | IG: N = 16 31.7 years CG: N = 16 41.4 years | Frequency: IG: 13.7 days/month CG: 13.2 days/month Intensity (pretreatment–posttreatment): IG: 19.2-10.5 (VAS) CG: 19.4-27.9 (VAS) Duration: not specified | Not specified |
| Study | Target Muscles | Diagnostic Criteria | Dry Needling Interventions Characteristics | Outcomes | Adverse Effects or Unwanted Reactions |
|---|---|---|---|---|---|
| De Abreu Venancio et al., 2009 [19] | Masseter, temporalis, occiput, and trapezius | Anamnesis and a physical exam to confirm the diagnosis of myofascial pain and headache. MTPs were located using digital palpation and the clinical exam was calibrated using a pressure algometer (1.5 kg of pressure) | Skin was cleansed with alcohol; the clinician inserts the needle 1–2 cm away from the trigger point, so that the needle may advance into the trigger point at an acute angle of 30 degrees to the skin | All the groups showed favorable results. The use of lidocaine or botulinum toxin made the technique less painful | Did not register any serious adverse events |
| Gagnon et al., 2024 [20] | Levator scapulae | Pincer grasp palpation to the distal levator scapulae muscles bilaterally | The patient was in a prone position with his arm internally rotated behind the back and a rolled towel was placed under the anterior shoulder. The needles were inserted obliquely from lateral to medial, superior to inferior, and posterior to anterior through the upper trapezius and into the levator scapulae muscle belly. Needle dimensions: 0.30 × 50 mm 5 sessions/2 months | Improvement in the patient’s headache symptoms | Not specified |
| Gildir et al., 2019 [21] | Masseter, temporalis, frontalis, splenius, upper trapezius, and suboccipital | Patients with active MTPs (referred pain after 10 s of palpation of the muscle). Pincer palpation method for upper trapezius muscle Flat palpation method for other muscles | Firstly, the area was cleaned with alcohol; then, with patients sitting, the needle was inserted into active MTPs for 20 min. Needle dimensions: 0.25 × 40 mm/0.25 × 25 mm 3 sessions per week for 3 weeks | Dry needling was effective and safe in reducing headache frequency, intensity, and duration, and increasing health-related quality of life | Five of the patients in each group experienced pain and fear during the procedure |
| Issa et Huijbregt, 2006 [22] | Upper trapezius, sternocleidomastoid, splenius capitis, suboccipital, masseter, and temporalis | Active MTP were diagnosed by way of subjective history, neck mobility tests, and manual palpation | The needle was fixed in the suspected area using a pincer grip or flat palpation depending on the muscle orientation, location, and direction of penetration; the needle was gently loosened from the tube and then a flick or tap of the top of the needle was performed to quickly penetrate the layers of the skin; the needle was then guided towards the taut band until resistance was felt in a particular direction and deep, gentle, small-amplitude withdrawals and penetrations of the needle were performed until a trigger point zone was reached; the needle was removed once palpable and/or visible release of the taut band had been determined. Needle dimensions: 0.3 × 30 mm/0.3 × 50 mm/0.2 × 13 mm 3 sessions/week for 6 weeks | Participant was reported to do very well with no headache | Not specified |
| Kamali et al., 2019 [23] | Sub-occipital, temporalis, sternocleidomastoid, and upper trapezius | Active MTPs were diagnosed by the presence of a taut band and the jump sign | Specific position for needling each muscle, and needling was carried out directly on MTPs. 3 sessions for 1 week | The frequency and intensity of headaches improved significantly in both study groups. IG increased the pain threshold significantly more than CG | Not specified |
| Karakurum et al., 2001 [24] | Splenius capitis, splenius cervicis, and mid-trapezius | Diagnosis was based upon the history given | The needles were left inserted in the muscle for 30 min. Needle dimensions: 0.3 × 25.4 mm 1 session/week, 4 weeks | There was significant improvement in IG compared with CG in muscle tenderness | Not specified |
| Monti-Ballano et al., 2019 [25] | Upper trapezius, splenius capitis and cervicis, semispinalis, rectus capitis posterior major, superior and inferior obliquus capitis, posterior and anterior occipitofrontalis, temporalis, masseter, clavicular and sternal head of sternocleidomastoid, zygomaticus major, and levator scapulae | MTP was considered active if the pain elicited during the pressure replication (using digital algometer) reproduced at least a portion of the TTH pain pattern typically reported by the patient | Specific patient position and needle insertion adapted to the muscle. In-and-out needling or needle winding in muscles with a large-diameter muscular belly and no nearby dangerous structures, and the bidirectional rotation technique was employed in muscles with a very flat muscular belly and those with structures like blood vessels and nerves nearby. Needle dimensions: 0.32 × 40 mm/0.32 × 25 mm 3 sessions | In IG, the intensity (VAS) significantly decreased | Did not register any serious adverse events |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bravo-Vazquez, A.; Anarte-Lazo, E.; Rodriguez-Blanco, C.; Bernal-Utrera, C. Dry Needling for Tension-Type Headache: A Scoping Review on Intervention Procedures, Muscle Targets, and Outcomes. J. Clin. Med. 2025, 14, 5320. https://doi.org/10.3390/jcm14155320
Bravo-Vazquez A, Anarte-Lazo E, Rodriguez-Blanco C, Bernal-Utrera C. Dry Needling for Tension-Type Headache: A Scoping Review on Intervention Procedures, Muscle Targets, and Outcomes. Journal of Clinical Medicine. 2025; 14(15):5320. https://doi.org/10.3390/jcm14155320
Chicago/Turabian StyleBravo-Vazquez, Ana, Ernesto Anarte-Lazo, Cleofas Rodriguez-Blanco, and Carlos Bernal-Utrera. 2025. "Dry Needling for Tension-Type Headache: A Scoping Review on Intervention Procedures, Muscle Targets, and Outcomes" Journal of Clinical Medicine 14, no. 15: 5320. https://doi.org/10.3390/jcm14155320
APA StyleBravo-Vazquez, A., Anarte-Lazo, E., Rodriguez-Blanco, C., & Bernal-Utrera, C. (2025). Dry Needling for Tension-Type Headache: A Scoping Review on Intervention Procedures, Muscle Targets, and Outcomes. Journal of Clinical Medicine, 14(15), 5320. https://doi.org/10.3390/jcm14155320