
Pediatric Echocardiographic Nomograms: Twenty Years of Advances—Do We Now Have a Complete and Reliable Tool, or Are Gaps Still Present? An Up-to-Date Review


 , ,
, ,  ,
, 
Abstract
1. Introduction
1.1. Literature Search Criteria
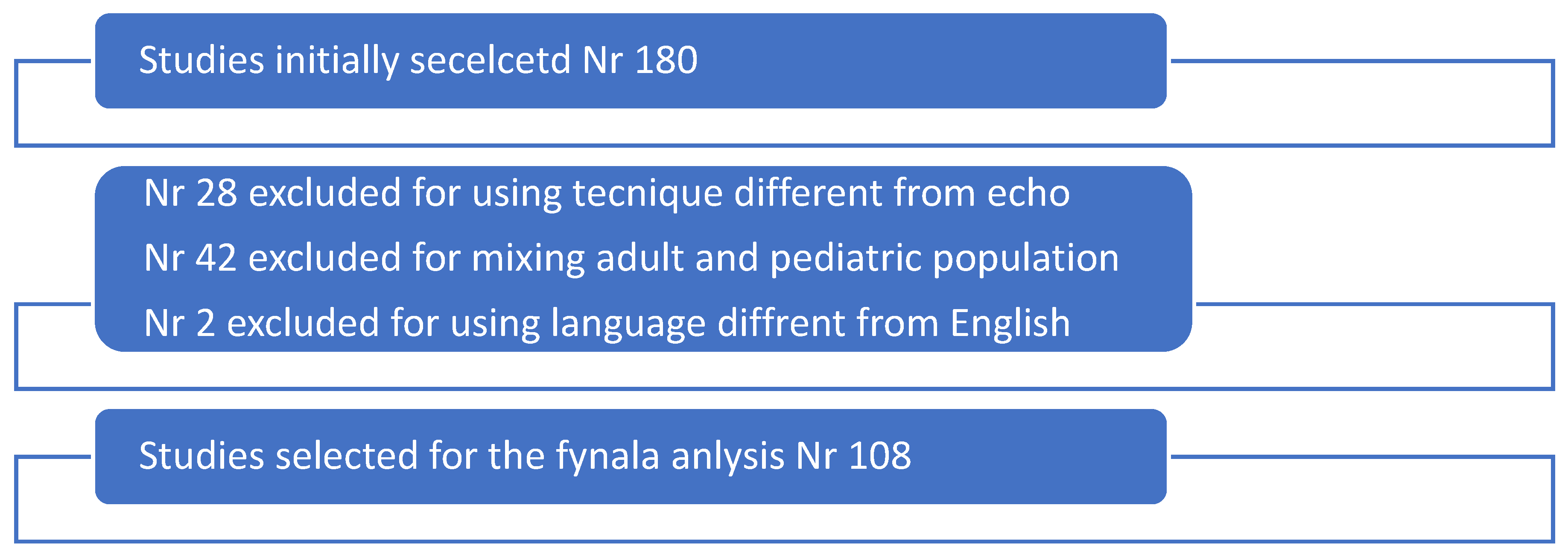
1.2. Search Results
2. General Aspects
- 1.
- Accuracy of a nomogram
- (a)
- Measurement Standardization
- (b)
- Inclusion and Exclusion Criteria
- (c)
- Sample Size Considerations
- (d)
- Normalization and Expression of Data
- (e)
- Statistical Modeling and Z-Score Calculation
- (f)
- Confounding Factors and Inherent Limitations
- 2.
- Nomograms for specific cardiac measurements
- a.
- Two-Dimensional Measurements
- b.
- Diastolic Function and Other Functional Parameters
- c.
- Strain Analysis
- (c1) Ventricular Strain
- (c2) Atrial Strain
- d.
- Three-Dimensional Measurements
3. Limitations of Current Nomograms
4. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lopez, L.; Colan, S.D.; Frommelt, P.C.; Ensing, G.J.; Kendall, K.; Younoszai, A.K.; Lai, W.W.; Geva, T. Recommendations for quantification methods during the performance of a pediatric echocardiogram: A report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J. Am. Soc. Echocardiogr. 2010, 23, 465–495. [Google Scholar] [CrossRef]
- Lopez, L.; Colan, S.; Stylianous, M.; Granger, S.; Trachtenberg, F.; Frommelt, P.; Pearson, G.; Camarda, J.; Cnota, J.; Cohen, M.; et al. Relationship of Echocardiographic Z Scores Adjusted for Body Surface Area to Age, Sex, Race, and Ethnicity: The Pediatric Heart Network Normal Echocardiogram Database. Circ. Cardiovasc. Imaging 2017, 10, e006979. [Google Scholar] [CrossRef]
- Cantinotti, M.; Scalese, M.; Murzi, B.; Assanta, N.; Spadoni, I.; Festa, P.; De Lucia, V.; Crocetti, M.; Marotta, M.; Molinaro, S.; et al. Echocardiographic nomograms for ventricular, valvular and arterial dimensions in Caucasian children with a special focus on neonates, infants and toddlers. J. Am. Soc. Echocardiogr. 2014, 27, 179–191.e2. [Google Scholar] [CrossRef]
- Cantinotti, M.; Giordano, R.; Scalese, M.; Murzi, B.; Assanta, N.; Spadoni, I.; Maura, C.; Marco, M.; Molinaro, S.; Kutty, S.; et al. Nomograms for two-dimensional echocardiography derived valvular and arterial dimensions in Caucasian children. J. Cardiol. 2017, 69, 208–215. [Google Scholar] [CrossRef]
- Cantinotti, M.; Scalese, M.; Giordano, R.; Franchi, E.; Marchese, P.; Vicava, C.; Assanta, N.; Iervasi, G.; Kutty, S.; Koestenberger, M. Pediatric nomograms for left ventricle biplane 2D volumes in healthy Caucasian children. Echocardiography 2020, 37, 971–975. [Google Scholar] [CrossRef]
- Gokhroo, R.K.; Anantharaj, A.; Bisht, D.; Kishor, K.; Plakkal, N.; Aghoram, R.; Mondal, N.; Pandey, S.K.; Roy, R. A pediatric echocardiographic Z-score nomogram for a developing country: Indian pediatric echocardiography study—The Z-score. Ann. Pediatr. Cardiol. 2017, 10, 31–38. [Google Scholar] [CrossRef]
- Singh, V.; Satheesh, S.; Ganapathy, S.; Nair, N.-P.S.; Mondal, N.; Selvaraj, R.; Mishra, N.; Anantharaj, A. Echocardiographic nomograms and Z-scores for term Indian neonates. Ann. Pediatr. Cardiol. 2023, 16, 11–17. [Google Scholar] [CrossRef]
- Cantinotti, M.; Scalese, M.; Contini, F.V.; Franchi, E.; Viacava, C.; Corana, G.; Pizzuto, A.; Pietro, M.; Santoro, G.; Assanta, N. Comprehensive Two-Dimensional Pediatric Echocardiographic Nomograms for Coronary Artery Sizes in Caucasian Children and Comparison among Major Nomograms. Diagnostics 2024, 14, 1029. [Google Scholar] [CrossRef]
- Kobayashi, T.; Fuse, S.; Sakamoto, N.; Mikami, M.; Ogawa, S.; Hamaoka, K.; Arakaki, Y.; Nakamura, T.; Nagasawa, H.; Kato, T.; et al. A New Z Score Curve of the Coronary Arterial Internal Diameter Using the Lambda-Mu-Sigma Method in a Pediatric Population. J. Am. Soc. Echocardiogr. 2016, 29, 794–801.e29. [Google Scholar] [CrossRef]
- Dallaire, F.; Dahdah, N. New equations and a critical appraisal of coronary artery Z scores in healthy children. J. Am. Soc. Echocardiogr. 2011, 24, 60–74. [Google Scholar] [CrossRef]
- Zhang, Y.Q.; Chen, S.B.; Huang, G.Y.; Zhang, H.Y.; Huang, M.R.; Wang, S.S.; Wu, L.; Hong, W.; Shen, R.; Liu, Y.; et al. Coronary artery indexed diameter and z score regression equations in healthy Chinese Han children. J. Clin. Ultrasound 2015, 43, 39–46. [Google Scholar] [CrossRef]
- Olivieri, L.; Arling, B.; Friberg, M.; Sable, C. Coronary artery Z score regression equations and calculators derived from a large heterogeneous population of children undergoing echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 159–164. [Google Scholar] [CrossRef]
- O’Leary, P.W. Pediatric diastology: Use and limitations of Doppler echocardiography in the evaluation of ventricular diastolic function in children. Prog. Pediatr. Cardiol. 1999, 10, 83–93. [Google Scholar] [CrossRef]
- Dallaire, F.; Slorach, C.; Hui, W.; Sarkola, T.; Friedberg, M.K.; Bradley, T.J.; Jaeggi, E.; Dragulescu, A.; Har, R.L.; Cherney, D.Z.; et al. Reference values for pulse wave Doppler and tissue Doppler imaging in pediatric echocardiography. Circ. Cardiovasc. Imaging 2015, 8, e002167. [Google Scholar] [CrossRef]
- Eidem, B.W.; McMahon, C.J.; Cohen, R.R.; Wu, J.; Finkelshteyn, I.; Kovalchin, J.P.; Ayres, N.A.; Bezold, L.I.; O’Brian Smith, E.; Pignatelli, R.H. Impact of cardiac growth on Doppler tissue imaging velocities: A study in healthy children. J. Am. Soc. Echocardiogr. 2004, 17, 212–221. [Google Scholar] [CrossRef]
- Cui, W.; Roberson, D.A. Left ventricular Tei index in children: Comparison of tissue Doppler imaging, pulsed wave Doppler and M-mode echocardiography normal values. J. Am. Soc. Echocardiogr. 2006, 19, 1438–1445. [Google Scholar] [CrossRef]
- Roberson, D.A.; Cui, W.; Chen, Z.; Madronero, L.F.; Cuneo, B.F. Annular and septal Doppler tissue imaging in children: Normal z-score tables and effects of age, heart rate, and body surface area. J. Am. Soc. Echocardiogr. 2007, 20, 1276–1284. [Google Scholar] [CrossRef]
- Cantinotti, M.; Giordano, R.; Scalese, M.; Murzi, B.; Assanta, N.; Spadoni, I.; Crocetti, M.; Marotta, M.; Molinaro, S.; Kutty, S.; et al. Nomograms for mitral inflow Doppler and tissue Doppler velocities in Caucasian children. J. Cardiol. 2016, 68, 288–299. [Google Scholar] [CrossRef]
- Schmitz, L.; Stiller, B.; Pees, C.; Koch, H.; Xanthopoulos, A.; Lange, P. Doppler-derived parameters of diastolic left ventricular function in preterm infants with a birth weight <1500 g: Reference values and differences to term infants. Early Hum. Dev. 2004, 76, 101–114. [Google Scholar] [CrossRef]
- Cantinotti, M.; Giordano, R.; Scalese, M.; Franchi, E.; Corana, G.; Assanta, N.; Maura, C.; Marco, M.; Molinaro, S.; Koestenberger, M.; et al. Nomograms for echocardiographic right ventricular sub-costal view dimensions in healthy Caucasian children: A new approach to measure the right ventricle. J. Cardiol. 2018, 71, 181–186. [Google Scholar] [CrossRef]
- Cantinotti, M.; Giordano, R.; Scalese, M.; Franchi, E.; Assanta, N.; Molinaro, S.; Marchese, P.; Paterni, M.; Iervasi, G.; Kutty, S.; et al. Nomograms of pulsed Doppler velocities, times, and velocity time integrals for semilunar valves and great arteries in healthy Caucasian children. Int. J. Cardiol. 2019, 285, 133–139. [Google Scholar] [CrossRef]
- Koestenberger, M.; Nage, B.; Ravekes, W.; Avian, A.; Burmas, A.; Grangl, G.; Cvirn, G.; Gamillscheg, A. Right Ventricular Outflow Tract Velocity Time Integral Determination in 570 Healthy Children and in 52 Pediatric Atrial Septal Defect Patients. Pediatr. Cardiol. 2015, 36, 1129–1134. [Google Scholar] [CrossRef]
- Núñez-Gil, I.J.; Rubio, M.D.; Cartón, A.J.; López-Romero, P.; Deiros, L.; García-Guereta, L.; Labrandero, C.; Gutiérrez-Larraya, F. Determination of normalized values of the tricuspid annular plane systolic excursion (TAPSE) in 405 Spanish children and adolescents. Rev. Esp. Cardiol. 2011, 64, 674–680. [Google Scholar] [CrossRef]
- Hashimoto, I.; Watanabe, K.; Kaneda, H. Z-values of tricuspid annular plane systolic excursion in Japanese children. Pediatr. Int. 2015, 57, 199–204. [Google Scholar] [CrossRef]
- Uysal, F.; Bostan, Ö.M.; Çil, E. Determination of reference values for tricuspid annular plane systolic excursion in healthy Turkish children. Anatol. J. Cardiol. 2016, 16, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Weismann, C.G.; Bamdad, M.C.; Abraham, S.; Ghiroli, S.; Dziura, J.; Hellenbrand, W.E. Normal pediatric data for isovolumic acceleration at the lateral tricuspid valve annulus-a heart rate—Dependent measure of right ventricular contractility. Echocardiography 2015, 32, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Koestenberger, M.; Nagel, B.; Ravekes, W.; Avian, A.; Heinzl, B.; Cvirn, G.; Fritsch, P.; Fandl, A.; Rehak, T.; Gamillscheg, A. Reference values of tricuspid annular peak systolic velocity in healthy pediatric patients, calculation of z score, and comparison to tricuspid annular plane systolic excursion. Am. J. Cardiol. 2012, 109, 116–121. [Google Scholar] [CrossRef]
- Terada, T.; Mori, K.; Inoue, M.; Yasunobu, H. Mitral annular plane systolic excursion/left ventricular length (MAPSE/L) as a simple index for assessing left ventricular longitudinal function in children. Echocardiography 2016, 33, 1703–1709. [Google Scholar] [CrossRef]
- Koestenberger, M.; Ravekes, W.; Nagel, B.; Avian, A.; Heinzl, B.; Cvirn, G.; Fritsch, P.; Fandl, A.; Rehak, T.; Gamillscheg, A. Reference values of the right ventricular outflow tract systolic excursion in 711 healthy children and calculation of z-score values. Eur. Heart J.-Cardiovasc. Imaging 2014, 15, 980–986. [Google Scholar] [CrossRef]
- Maffessanti, F.; Muraru, D.; Esposito, R.; Gripari, P.; Ermacora, D.; Santoro, C.; Tamborini, G.; Galderisi, M.; Pepi, M.; Badano, L.P. Age-, Body Size- and Gender-Specific Reference Values for Right Ventricular Volumes and Ejection Fraction by Three-Dimensional Echocardiography: A Multicenter Echocardiographic Study in 507 Healthy Volunteers. Circ. Cardiovasc. Imaging 2013, 6, 700–710. [Google Scholar] [CrossRef]
- Koestenberger, M.; Grangl, G.; Avian, A.; Gamillscheg, A.; Grillitsch, M.; Cvirn, G.; Burmas, A.; Hansmann, G. Normal Reference Values and z Scores of the Pulmonary Artery Acceleration Time in Children and Its Importance for the Assessment of Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2017, 10, e005336. [Google Scholar] [CrossRef]
- Koestenberger, M.; Ravekes, W.; Everett, A.D.; Stueger, H.P.; Heinzl, B.; Gamillscheg, A.; Cvirn, G.; Boysen, A.; Fandl, A.; Nagel, B. Right ventricular function in infants, children and adolescents: Reference values of the tricuspid annular plane systolic excursion (TAPSE) in 640 healthy patients and calculation of z score values. J. Am. Soc. Echocardiogr. 2009, 22, 715–719. [Google Scholar] [CrossRef]
- Marchese, P.; Scalese, M.; Giordano, R.; Assanta, N.; Franchi, E.; Koestenberger, M.; Ravaglioli, A.; Kutty, S.; Cantinotti, M. Pediatric ranges of normality for 2D speckle-tracking echocardiography atrial strain: Differences between p- and r-gating and among new (Atrial Designed) and conventional (Ventricular Specific) software’s. Echocardiography 2021, 38, 2025–2031. [Google Scholar] [CrossRef]
- Acheampong, B.; Parra, D.; Havens, C.; Jantzen, D.; Godown, J.; Soslow, J. Vendor independent myocardial strain values in children. Echocardiography 2023, 40, 30–36. [Google Scholar] [CrossRef]
- Adar, A.; Ghelani, S.J.; Sleeper, L.A.; Lu, M.; Marcus, E.; Ferraro, A.M.; Colan, S.D.; Banka, P.; Powell, A.J.; Harrild, D.M. Normal Values for Left Ventricular Strain and Synchrony in Children Based on Speckle Tracking Echocardiography. Am. J. Cardiol. 2019, 123, 1546–1554. [Google Scholar] [CrossRef] [PubMed]
- Jimbo, S.; Noto, N.; Okuma, H.; Kato, M.; Komori, A.; Ayusawa, M.; Morioka, I. Normal reference values for left atrial strains and strain rates in school children assessed using two-dimensional speckle-tracking echocardiography. Heart Vessels 2020, 35, 1270–1280. [Google Scholar] [CrossRef] [PubMed]
- Harrington, J.K.; Ferraro, A.M.; Colan, S.D.; Sleeper, L.A.; Lu, M.; Adar, A.; Powell, A.J.; Levy, P.T.; Harrild, D.M. Normal Left Ventricular Systolic and Diastolic Strain Rate Values in Children Derived from Two-Dimensional Speckle-Tracking Echocardiography. J. Am. Soc. Echocardiogr. 2021, 34, 1303–1315.e3. [Google Scholar] [CrossRef] [PubMed]
- Kotby, A.A.; Ebrahim, S.O.S.; Al-Fahham, M.M. Reference centiles for left ventricular longitudinal global and regional systolic strain by automated functional imaging in healthy Egyptian children. Cardiol. Young 2023, 33, 26–34. [Google Scholar] [CrossRef]
- Davarpasand, T.; Jalali, A.; Mohseni-Badalabadi, R.; Toofaninejad, N.; Hali, R.; Fallah, F.; Seilani, P.; Hosseinsabet, A. Normal ranges of left atrial phasic strains and strain rates by 2D speckle-tracking echocardiography in pediatrics: A systematic review and meta-analysis. Sci. Rep. 2024, 14, 25888. [Google Scholar] [CrossRef]
- Koopman, L.P.; Rebel, B.; Gnanam, D.; Menting, M.E.; Helbing, W.A.; Boersma, E. Reference values for two-dimensional myocardial strain echocardiography of the left ventricle in healthy children. Cardiol. Young 2019, 29, 325–337. [Google Scholar] [CrossRef]
- Zhang, L.; Gao, J.; Xie, M.; Yin, P.; Liu, W.; Li, Y.; Klas, B.; Sun, J.; Balluz, R.; Ge, S. Left ventricular three-dimensional global systolic strain by real-time three-dimensional speckle-tracking in children: Feasibility, reproducibility, maturational changes, and normal ranges. J. Am. Soc. Echocardiogr. 2013, 26, 853–859. [Google Scholar] [CrossRef]
- Kamel, H.; Elsayegh, A.T.; Nazmi, H.; Attia, H.M. Assessment of left ventricular systolic function using two- and three-dimensional speckle tracking echocardiography among healthy preschool-age pediatric children. Egypt. Heart J. 2022, 74, 21. [Google Scholar] [CrossRef]
- Aristizábal-Duque, C.H.; Fernández Cabeza, J.; Blancas Sánchez, I.M.; Delgado Ortega, M.; Aparicio Martinez, P.; Romero-Saldaña, M.; del Pozo, F.J.F.; Pan, M.; Ruiz Ortiz, M.; Mesa-Rubio, M.D. The Assessment of Myocardial Longitudinal Strain in a Paediatric Spanish Population Using a New Software Analysis. J. Clin. Med. 2022, 11, 3272. [Google Scholar] [CrossRef]
- Marcus, K.A.; Mavinkurve-Groothuis, A.M.; Barends, M.; van Dijk, A.; Feuth, T.; de Korte, C.; Kapusta, L. Reference values for myocardial two-dimensional strain echocardiography in a healthy pediatric and young adult cohort. J. Am. Soc. Echocardiogr. 2011, 24, 625–636. [Google Scholar] [CrossRef]
- Klitsie, L.M.; Roest, A.A.; van der Hulst, A.E.; Stijnen, T.; Blom, N.A.; Ten Harkel, A.D. Assessment of intraventricular time differences in healthy children using two-dimensional speckle tracking echocardiography. J. Am. Soc. Echocardiogr. 2013, 26, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Dallaire, F.; Slorach, C.; Bradley, T.; Hui, W.; Sarkola, T.; Friedberg, M.K.; Jaeggi, E.; Dragulescu, A.; Mahmud, F.H.; Daneman, D.; et al. Pediatric Reference Values and Z Score Equations for Left Ventricular Systolic Strain Measured by Two-Dimensional Speckle-Tracking Echocardiography. J. Am. Soc. Echocardiogr. 2016, 29, 786–793.e8. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M.; Scalese, M.; Giordano, R.; Franchi, E.; Assanta, N.; Marotta, M.; Viacava, C.; Molinaro, S.; Iervasi, G.; Santoro, G.; et al. Normative Data for Left and Right Ventricular Systolic Strain in Healthy Caucasian Italian Children by Two-Dimensional Speckle-Tracking Echocardiography. J. Am. Soc. Echocardiogr. 2018, 31, 712–720.e6. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.T.; Mejia, A.A.S.; Machefsky, A.; Fowler, S.; Holland, M.R.; Singh, G.K. Normal ranges of right ventricular systolic and diastolic strain measures in children: A systematic review and meta-analysis. J. Am. Soc. Echocardiogr. 2014, 27, 549–560.e3. [Google Scholar] [CrossRef]
- Ghelani, S.J.; Brown, D.W.; Kuebler, J.D.; Perrin, D.; Shakti, D.; Williams, D.N.; Marx, G.R.; Colan, S.D.; Geva, T.; Harrild, D.M. Left atrial volumes and strain in healthy children measured by three-dimensional echocardiography: Normal values and maturational changes. J. Am. Soc. Echocardiogr. 2018, 31, 187–193. [Google Scholar] [CrossRef]
- Kutty, S.; Padiyath, A.; Li, L.; Peng, Q.; Rangamani, S.; Schuster, A.; Danford, D.A. Functional Maturation of left and right atrial systolic and diastolic performance in infants, children, and adolescents. J. Am. Soc. Echocardiogr. 2013, 26, 398–4092. [Google Scholar] [CrossRef]
- Ramlogan, S.; Aly, D.; France, R.; Schmidt, S.; Hinzman, J.; Sherman, A.; Goudar, S.P.; Forsha, D. Reproducibility and Intervendor Agreement of Left Ventricular Global Systolic Strain in Children Using a Layer-Specific Analysis. J. Am. Soc. Echocardiogr. 2020, 33, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Romanowicz, J.; Ferraro, A.M.; Harrington, J.K.; Sleeper, L.A.; Adar, A.; Levy, P.T.; Powell, A.J.; Harrild, D.M. Pediatric Normal Values and Z Score Equations for Left and Right Ventricular Strain by Two-Dimensional Speckle-Tracking Echocardiography Derived from a Large Cohort of Healthy Children. J. Am. Soc. Echocardiogr. 2023, 36, 310–323. [Google Scholar] [CrossRef] [PubMed]
- Amedro, P.; Bredy, C.; Guillaumont, S.; De La Villeon, G.; Gamon, L.; Lavastre, K.; Meli, A.C.; Richard, S.; Cazorla, O.; Lacampagne, A.; et al. Speckle tracking echocardiography in healthy children: Comparison between the QLAB by Philips and the EchoPAC by General Electric. Int. J. Cardiovasc. Imaging 2019, 35, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, A.M.; Adar, A.; Ghelani, S.J.; Sleeper, L.A.; Levy, P.T.; Rathod, R.H.; Marx, G.R.; Harrild, D.M. Speckle tracking echocardiographically-based analysis of ventricular strain in children: An intervendor comparison. Cardiovasc. Ultrasound 2020, 18, 15. [Google Scholar] [CrossRef]
- Palmer, C.; Truong, V.T.; Klas, B.; Wolking, S.; Ornella, A.; Young, M.; Ngo, T.N.M.; Tretter, J.T.; Nagueh, S.F.; Mazur, W. Left and right atrial speckle tracking: Comparison of three methods of time reference gating. Echocardiography 2020, 37, 1021–1029. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef]
- Kuebler, J.D.; Ghelani, S.; Williams, D.M.; Nathan, M.; Marx, G.; Colan, S.D.; Harrild, D.M. Normal Values and Growth-Related Changes of Left Ventricular Volumes, Stress, and Strain in Healthy Children Measured by 3-Dimensional Echocardiography. Am. J. Cardiol. 2018, 122, 331–339. [Google Scholar] [CrossRef]
- Jone, P.N.; Le, L.; Pan, Z.; Colen, T.; Shigemitsu, S.; Khoo, N.S.; Goot, B.H.; Parthiban, A.; Harrild, D.M.; Ferraro, A.M.; et al. A multicenter study of three-dimensional echocardiographic evaluation of normal pediatric left ventricular volumes and function. Echocardiography 2021, 38, 641–645. [Google Scholar] [CrossRef]
- Krell, K.; Laser, K.T.; Dalla-Pozza, R.; Winkler, C.; Hildebrandt, U.; Kececioglu, D.; Breuer, J.; Herberg, U. Real-time three-dimensional echocardiography of the left ventricle—Pediatric percentiles and head-to-head comparison of different contour finding algorithms: A multicenter study. J. Am. Soc. Echocardiogr. 2018, 31, 702–711.e13. [Google Scholar] [CrossRef]
- Herberg, U.; Smit, F.; Winkler, C.; Dalla-Pozza, R.; Breuer, J.; Laser, K.T. Real-time 3D-echocardiography of the right ventricle—Paediatric reference values for right ventricular volumes using knowledge-based reconstruction: A multicentre study. Quant. Imaging Med. Surg. 2021, 11, 2905–2917. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M.; Scalese, M.; Giordano, R.; Franchi, E.; Marchese, P.; Assanta, N.; Molinaro, S.; Paterni, M.; Iervasi, G.; Koestenberger, M.; et al. Three-Dimensional Echocardiography Derived Nomograms for Left Ventricular Volumes in Healthy Caucasian Italian Children. J. Am. Soc. Echocardiogr. 2019, 32, 794–797.e1. [Google Scholar] [CrossRef] [PubMed]
- Jone, P.N.; Schäfer, M.; Pan, Z.; Bremen, C.; Ivy, D.D. 3D echocardiographic evaluation of right ventricular function and strain: A prognostic study in paediatric pulmonary hypertension. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Linden, K.; Goldschmidt, F.; Laser, K.T.; Winkler, C.; Körperich, H.; Dalla-Pozza, R.; Breuer, J.; Herberg, U. Left Atrial Volumes and Phasic Function in Healthy Children: Reference Values Using Real-Time Three-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1036–1045.e9. [Google Scholar] [CrossRef]
- Sabatino, J.; Borrelli, N.; Fraisse, A.; Herberg, J.; Karagadova, E.; Avesani, M.; Bucciarelli, V.; Josen, M.; Paredes, J.; Piccinelli, E.; et al. Abnormal myocardial work in children with Kawasaki disease. Sci. Rep. 2021, 11, 7974. [Google Scholar] [CrossRef]
- Sabatino, J.; Leo, I.; Strangio, A.; La Bella, S.; Borrelli, N.; Avesani, M.; Josen, M.; Paredes, J.; Piccinelli, E.; Sirico, D.; et al. Echocardiographic Normal Reference Ranges for Non-invasive Myocardial Work Parameters in Pediatric Age: Results from an International Multi-Center Study. Front. Cardiovasc. Med. 2022, 9, 792622. [Google Scholar] [CrossRef]
- Cui, C.; Zheng, Q.; Li, Y.; Huang, D.; Hu, Y.; Wang, Y.; Liu, R.; Liu, L.; Zhang, L. Reference Values of Noninvasive Myocardial Work Indices Measured by Echocardiography in Healthy Children. Front. Pediatr. 2022, 10, 792526. [Google Scholar] [CrossRef]
- Pham, T.T.M.; Truong, V.T.; Vu, P.N.; Tran, T.X.; Nguyen, N.N.H.; Nguyen, L.P.T.; Tu, H.N.T.; Palmer, C.; Tretter, J.T.; Levy, P.; et al. Echocardiographic Reference Ranges of Non-invasive Myocardial Work Indices in Children. Pediatr. Cardiol. 2022, 43, 82–91. [Google Scholar] [CrossRef]
- Luo, X.; Ge, Q.; Su, J.; Zhou, N.; Li, P.; Xiao, X.; Chen, Y.; Wang, D.; Ma, Y.; Ma, L.; et al. Normal ranges of non-invasive left ventricular myocardial work indices in healthy young people. Front. Pediatr. 2022, 10, 1000556. [Google Scholar] [CrossRef]
- Tretter, J.T.; Pradhan, S.; Truong, V.T.; Mullikin, A.; Mazur, W.; Hill, G.D.; Redington, A.N.; Taylor, M.D. Non-invasive left ventricular myocardial work indices in healthy adolescents at rest. Int. J. Cardiovasc. Imaging 2021, 37, 2429–2438. [Google Scholar] [CrossRef]
- Marchese, P.; Scalese, M.; Assanta, N.; Franchi, E.; Viacava, C.; Santoro, G.; Corana, G.; Pizzuto, A.; Contini, F.V.; Kutty, S.; et al. Normal Values for Echocardiographic Myocardial Work in a Large Pediatric Population. Diagnostics 2024, 14, 1022. [Google Scholar] [CrossRef]
- Cantinotti, M.; Scalese, M.; Giordano, R.; Assanta, N.; Marchese, P.; Franchi, E.; Viacava, C.; Koestenberger, M.; Jani, V.; Kutty, S. A statistical comparison of reproducibility in current pediatric two-dimensional echocardiographic nomograms. Pediatr. Res. 2021, 89, 579–590. [Google Scholar] [CrossRef]
- Available online: https://zscore.chboston.org/ (accessed on 10 October 2024).
- Available online: https://parameterz.com (accessed on 10 October 2024).
- Available online: https://www.pediatricheartnetwork.org/z-scores-calculator/ (accessed on 10 October 2024).
- Available online: https://www.prisma-statement.org/ (accessed on 10 October 2024).
- Lopez, L.; Saurers, D.L.; Barker, P.C.A.; Cohen, M.S.; Colan, S.D.; Dwyer, J.; Forsha, D.; Friedberg, M.K.; Lai, W.W.; Printz, B.F.; et al. Guidelines for Performing a Comprehensive Pediatric Transthoracic Echocardiogram: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2024, 37, 119–170. [Google Scholar] [CrossRef] [PubMed]
- Simpson, J.; Lopez, L.; Acar, P.; Friedberg, M.K.; Khoo, N.S.; Ko, H.H.; Marek, J.; Marx, G.; McGhie, J.S.; Meijboom, F.; et al. Three-dimensional Echocardiography in Congenital Heart Disease: An Expert Consensus Document from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Mahgerefteh, J.; Lai, W.; Colan, S.; Trachtenberg, F.; Gongwer, R.; Stylianou, M.; Bhat, A.H.; Goldberg, D.; McCrindle, B.; Frommelt, P.; et al. Height Versus Body Surface Area to Normalize Cardiovascular Measurements in Children Using the Pediatric Heart Network Echocardiographic Z-Score Database. Pediatr. Cardiol. 2021, 42, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Thomson, D.; Seto, I.; Contopoulos-Ioannidis, D.G.; Ioannidis, J.P.; Curtis, S.; Constantin, E.; Batmanabane, G.; Hartling, L.; Klassen, T. Standard 6: Age groups for pediatric trials. Pediatrics 2012, 129, S153–S160. [Google Scholar] [CrossRef]
- Thompson, W.; Endriss, J. The required sample size when estimating variances. Am. Stat. 1961, 15, 22–23. [Google Scholar] [CrossRef]
- Kish, L. Survey Sampling; John Wiley & Sons, Inc.: New York, NY, USA, 1965. [Google Scholar]
- Plante, V.; Gobeil, L.; Xiong, W.T.; Touré, M.; Dahdah, N.; Greenway, S.C.; Drolet, C.; Wong, K.K.; Mackie, A.S.; Bradley, T.J.; et al. Alternative to Body Surface Area as a Solution to Correct Systematic Bias in Pediatric Echocardiography Z Scores. Can. J. Cardiol. 2021, 37, 1790–1797. [Google Scholar] [CrossRef]
- Haycock, G.B.; Schwartz, G.J.; Wisotsky, D.H. Geometric method for measuring body surface area: A height-weight formula validated in infants, children, and adults. J. Pediatr. 1978, 93, 62–66. [Google Scholar] [CrossRef]
- Bonatto, R.C.; Fioretto, J.R.; Okoshi, K.; Matsubara, B.B.; Padovani, C.R.; Manfrin, T.C.R.; Gobbi, M.; Martino, R.S.; Bregagnollo, E.A. Percentile curves of normal values of echocardiographic measurements in normal children from the central-southern region of the State of Sao Paulo, Brazil. Arq. Bras. Cardiol. 2006, 87, 711–721. [Google Scholar]
- White, H.A. Heteroscedasticity-consistent covariance matrix estimator and a direct test for heteroscedasticity. Econometrica 1980, 48, 817–838. [Google Scholar] [CrossRef]
- Breusch, T.S.; Pagan, A.R. A Simple test for heteroscedasticity and random coefficient variation. Econometrica 1979, 47, 1287–1294. [Google Scholar] [CrossRef]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Lilliefors, H. On the Kolmogorov–Smirnov test for normality with mean and variance unknown. J. Am. Stat. Assoc. 1967, 62, 399–402. [Google Scholar] [CrossRef]
- Sluysmans, T.; Colan, S.D. Theoretical and empirical derivation of cardiovascular allometric relationships in children. J. Appl. Physiol. 2005, 99, 445–457. [Google Scholar] [CrossRef]
- Pettersen, M.D.; Du, W.; Skeens, M.E.; Humes, R.A. Regression equations for calculation of z scores of cardiac structures in a large cohort of healthy infants, children, and adolescents: An echocardiographic study. J. Am. Soc. Echocardiogr. 2008, 21, 922–934. [Google Scholar] [CrossRef]
- Majonga, E.D.; Rehman, A.M.; McHugh, G.; Mujuru, H.A.; Nathoo, K.; Patel, M.S.; Munyati, S.; Odland, J.O.; Kranzer, K.; Kaski, J.P.; et al. Echocardiographic reference ranges in older children and adolescents in sub-Saharan Africa. Int. J. Cardiol. 2017, 248, 409–413. [Google Scholar] [CrossRef]
- Majonga, E.D.; Norrish, G.; Rehman, A.M.; Kranzer, K.; Mujuru, H.A.; Nathoo, K.; Odland, J.O.; Kaski, J.P.; Ferrand, R.A. Racial Variation in Echocardiographic Reference Ranges for Left Chamber Dimensions in Children and Adolescents: A Systematic Review. Pediatr. Cardiol. 2018, 39, 859–868. [Google Scholar] [CrossRef]
- Zilberman, M.V.; Khoury, P.R.; Kimball, R.T. Two-dimensional echocardiographic valve measurements in healthy children: Gender-specific differences. Pediatr. Cardiol. 2005, 26, 356–360. [Google Scholar] [CrossRef]
- Gautier, M.; Detaint, D.; Fermanian, C.; Aegerter, P.; Delorme, G.; Arnoult, F.; Milleron, O.; Raoux, F.; Stheneur, C.; Boileau, C.; et al. Nomograms for aortic root diameters in children using two-dimensional echocardiography. Am. J. Cardiol. 2010, 105, 888–894. [Google Scholar] [CrossRef]
- Cantinotti, M.; Scalese, M.; Murzi, B.; Assanta, N.; Spadoni, I.; De Lucia, V.; Crocetti, M.; Cresti, A.; Gallotta, M.; Marotta, M.; et al. Echocardiographic nomograms for chamber diameters and areas in Caucasian children. J. Am. Soc. Echocardiogr. 2014, 27, 1279–1292.e2. [Google Scholar] [CrossRef]
- Ciccone, M.M.; Scicchitano, P.; Zito, A.; Gesualdo, M.; Sassara, M.; Calderoni, G.; Di Mauro, F.; Ladisa, G.; Di Mauro, A.; Laforgia, N. Different functional cardiac characteristics observed in term/preterm neonates by echocardiography and tissue Doppler imaging. Early Hum. Dev. 2011, 87, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Lorch, S.M.; Ludomirsky, A.; Singh, G.K. Maturational and growth-related changes in left ventricular longitudinal strain and strain rate measured by two-dimensional speckle tracking echocardiography in healthy pediatric population. J. Am. Soc. Echocardiogr. 2008, 21, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M.; Kutty, S.; Giordano, R.; Assanta, N.; Murzi, B.; Crocetti, M.; Marotta, M.; Iervasi, G. Review and status report of pediatric left ventricular systolic strain and strain rate nomograms. Heart Fail. Rev. 2015, 20, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Al Naami, G.; Thompson, R.; Inage, A.; Mackie, A.S.; Smallhorn, J.F. Normal rotational, torsion and untwisting data in children, adolescents and young adults. J. Am. Soc. Echocardiogr. 2010, 23, 286–293. [Google Scholar] [CrossRef]
- Kaku, K.; Takeuchi, M.; Tsang, W.; Takigiku, K.; Yasukochi, S.; Patel, A.R.; Mor-Avi, V.; Lang, R.M.; Otsuji, Y. Age-related normal range of left ventricular strain and torsion using three-dimensional speckle-tracking echocardiography. J. Am. Soc. Echocardiogr. 2014, 27, 55–64. [Google Scholar] [CrossRef]
- Kim, H.J.; Yoon, J.H.; Lee, E.J.; Oh, J.H.; Lee, J.Y.; Lee, S.J.; Han, J.W. Normal left ventricular torsion mechanics in healthy children: Age related changes of torsion parameters are closely related to changes in heart rate. Korean Circ. J. 2015, 45, 131–140. [Google Scholar] [CrossRef]
- Poutanen, T.; Jokinen, E. Left ventricular mass in 169 healthy children and young adults assessed by three-dimensional echocardiography. Pediatr. Cardiol. 2007, 28, 201–207. [Google Scholar] [CrossRef]
- Boettler, P.; Hartmann, M.; Watzl, K.; Maroula, E.; Schulte-Moenting, J.; Knirsch, W.; Dittrich, S.; Kececioglu, D. Heart rate effects on strain and strain rate in healthy children. J. Am. Soc. Echocardiogr. 2005, 18, 1121–1130. [Google Scholar] [CrossRef]
- Poutanen, T.; Jokinen, E.; Sairanen, H.; Tikanoja, T. Left atrial and left ventricular function in healthy children and young adults assessed by three dimensional echocardiography. Heart 2003, 89, 544–549. [Google Scholar] [CrossRef]
- Poutanen, T.; Tikanoja, T.; Sairanen, H.; Jokinen, E. Normal mitral and aortic valve areas assessed by three- and two-dimensional echocardiography in 168 children and young adults. Pediatr. Cardiol. 2006, 27, 217–225. [Google Scholar] [CrossRef]
- Lu, D.F.; Tong, X.M.; Liu, Y.F.; Zhang, H. Reference Values for Point-of-Care Echocardiographic Measurements of Preterm Infants in China. Front. Pediatr. 2022, 10, 894152. [Google Scholar] [CrossRef]
- Ashrafi, A.H.; Lai, W.; Gaffar, S.; Renella, P. Normative Echocardiographic Values for Right and Left Ventricular Function in Extremely Premature Neonates. J. Pediatr. 2021, 236, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Fu, J.; Wu, L.; Liu, X.Y.; Zhang, Y. Percentile curves of normal echocardiographic measurements values for left heart structures in 1570 Han Chinese preterm and term infants. J. Clin. Ultrasound 2022, 50, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Calado, C.; Collins, C.; Drew, S.; Holberton, J. Reference echocardiographic measurements in very low birth weight preterm infants. Am. J. Perinatol. 2019, 36, 303–310. [Google Scholar] [PubMed]
- Skelton, R.; Gill, A.B.; Parsons, J.M. Reference ranges for cardiac dimensions and blood flow velocity in preterm infants. Heart 1998, 80, 281–285. [Google Scholar] [CrossRef]
- Abushaban, L.; Vel, M.T.; Rathinasamy, J.; Sharma, P.N. Normal reference ranges for pulmonary artery diameters in preterm infants. Pediatr. Cardiol. 2017, 38, 1377–1384. [Google Scholar] [CrossRef]
- Choudhry, S.; Salter, A.; Cunningham, T.W.; Levy, P.T.; Nguyen, H.H.; Wallendorf, M.; Singh, G.K.; Johnson, M.C. Normative Left Ventricular M-Mode Echocardiographic Values in Preterm Infants up to 2 kg. J. Am. Soc. Echocardiogr. 2017, 30, 781–789.e4. [Google Scholar] [CrossRef]
- Krysztofiak, H.; Młyńczak, M.; Folga, A.; Braksator, W.; Małek, Ł.A. Normal values for left ventricular mass in relation to lean body mass in child and adolescent athletes. Pediatr. Cardiol. 2019, 40, 204–208. [Google Scholar] [CrossRef]
- Cavarretta, E.; Maffessanti, F.; Sperandii, F.; Guerra, E.; Quaranta, F.; Nigro, A.; Minati, M.; Rebecchi, M.; Fossati, C.; Calò, L.; et al. Reference values of left heart echocardiographic dimensions and mass in male peri-pubertal athletes. Eur. J. Prev. Cardiol. 2018, 25, 1204–1215. [Google Scholar] [CrossRef]
- Sharma, S.; Maron, B.J.; Whyte, G.; Firoozi, S.; Elliott, P.M.; McKenna, W.J. Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete’s heart and hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2002, 40, 1431–1436. [Google Scholar] [CrossRef]
- Makan, J.; Sharma, S.; Firoozi, S.; Whyte, G.; Jackson, P.G.; McKenna, W.J. Physiological upper limits of ventricular cavity size in highly trained adolescent athletes. Heart 2005, 9, 495–499. [Google Scholar] [CrossRef]
- George, K.; Sharma, S.; Batterham, A.; Whyte, G.; McKenna, W. Allometric analysis of the association between cardiac dimensions and body size variables in 464 junior athletes. Clin. Sci. 2001, 100, 47–54. [Google Scholar] [CrossRef]
- Chen, L.; Chen, W.; Zhu, Y.; Zhang, Z.; Liu, T.; Zhang, L. Global research landscape on artificial intelligence in echocardiography from 1997 to 2024: Bibliometric analysis. Digit. Health 2025, 11, 20552076251351201. [Google Scholar]
- Mayourian, J.; Asztalos, I.B.; El-Bokl, A.; Lukyanenko, P.; Kobayashi, R.L.; La Cava, W.G.; Ghelani, S.J.; Vetter, V.L.; Triedman, J.K. Electrocardiogram-based deep learning to predict left ventricular systolic dysfunction in paediatric and adult congenital heart disease in the USA: A multicentre modelling study. Lancet Digit. Health 2025, 7, e264–e274. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author | Parameters Evaluated | Sample Size | Normalization | Data Expression | R2 |
|---|---|---|---|---|---|
| Pettersen MD USA 2008 [91] | Aortic arch at 3 levels, Abd Ao, pulmonary annulus, MPA, RPA, LPA, aortic annulus, Ao root, Asc Ao, (PLA), MV and TV annulus; LV M-mode | n. 748 0–18 yrs | BSA NR | Z-score | 0.992–0604 |
| Zilberman MV USA 2005 [94] | Annulus of aorta, pulmonary, MV, TV | N. 748 0–18 yrs | BSA DuBois | Z-score | 0.91–0.70 |
| Gautier M USA 2010 [95] | Ao annulus, Ao root, STJ, Asc. Ao | n. 353 2–18 yrs | BSA Dubois | Z-score | NR |
| Cantinotti M Italy 2014 [3] | Aortic arch (IA-LCA, LCA-LSA, after LSA, isthmus), thoracic aorta, Ao annulus, Ao root, STJ; Asc. Ao, aorta at the diagram, pulmonary annulus, MPA, RPA, LPA, IVC, LV M-mode | n. 445 0–36 months | BSA Haycock | Z-score | 0.89–0.49 |
| Cantinotti M Italy 2014 [96] | LV, diameters and area in 4 and 2 ch views, 4 ch RV, RA, LA diameters and areas | n. 1091 0–17 yrs | BSA Haycock | Z-score | 0.96–0.86 |
| Cantinotti M Italy 2017 [4] | Aortic arch (IA-LCA, LCA-LSA, after LSA, isthmus), thoracic aorta, Ao annulus, Ao root, STJ; Asc Ao, aorta at the diagram, pulmonary annulus, MPA, RPA, LPA, IVC, LV M-mode | n. 1151 0–17 yrs | BSA Haycock | Z-score | 0.93–0.85 |
| Lopez L 2017 Multicenter USA [2] | Ao, PA, MV (AP and lat) and TV (Ap and lat) annulus, Asc Ao, STJ, Asc Ao, MPA; LPA; RPA, MVA, TVA, arch (prox, dist, isthmus), LVEDA (PSA), LVEDV (5/6 × LVEDA × LVEDL), LVEDL (4 ch). LVM. | n. 3215 0–18 yrs (35% whites, 31% black, 34% other) | BSA Haycock | Z-score | NA |
| Gokhroo RK 2017, India [6] | Ao annulus, Ao root, STJ, Asc Ao, MVA, TVA. LA and RA diameters, RV basal, and mid-cavity diameter, RV length | n. 746 4–15 yrs | BSA Haycock | Z-score | 0.35–0.114 |
| Author | Sample Size | Coronary Artery | Normalization | Data Expression | R2 |
|---|---|---|---|---|---|
| Kobayashi T 2016 Japan [9] | n. 3851 <18 yrs | RCA, LMCA, LCX, LAD | BSA Haycock | Z-score | NA |
| Dallaire F 2010 Canada [10] | n. 1033 Age NR | RCA, LMCA, LCX, LAD | BSA Haycock | Z-score | 0.71–0.79 |
| Zhang Y et al., 2014 China [11] | n. 506 1 day–18 yrs | RCA, LMCA, LCX, LAD | BSA Haycock | Z-score | 0.50–0.51 |
| Olivieri L, USA 2009 [12] | n. 432 0–20 yrs | LMCA, LAD, RCA | BSA DuBois | Z-score | 0.79–0.84 |
| Lopez L et al., 2017, USA [2] | n. 3215 0–18 yrs | LMCA, LAD, RCA | BSA Haycock | Z-score | NA |
| Cantinotti et al. 2016 Italy [18] | n. 606 0–18 yrs | LMCA, LAD, RCA, LCX Proximal LMCA and RCA | BSA Haycock | Z-score | 0.6–0.628 |
| Author | Parameter Evaluated | Sample Size | Normalization | Data Expression |
|---|---|---|---|---|
| O’ Leary PW 1998 USA [13] | Pwd MV: E, A, E/A, EDT, IVRT | n. 223 3–17 yrs | Age Groups | Mean ± SD |
| Schmitz L. 2004 Germany [19] | Pwd MV: E, A, EDT, IVRT | n. 311 0–19 yrs | Age Groups | Mean ± SD |
| Eidem BW 2004 USA [15] | Pwd MV E, A, E/A Pwd TV: E, A, E/A TDI MV: e′, a′, E/e′ TDI TV: e′, a′, E/e′ | n. 325 0–18 yrs | Age groups | Mean ± SD |
| Ciccone M. 2011 Italy [97] | Pwd MV E, A, E/A Pwd TV: E, A, E/A TDI MV: e′, a′, E/e′ | n. 53 (neonates) | Term and Preterm | Mean ± SD |
| Dallaire F. 2015 Canada [10] | Pwd MV E, A, E/A, DT, TDI MV: e′, a′, E/e′, | n. 233 1–18 yrs | BSA (Haycock) | Z-scores |
| Cantinotti M. 2016 Italy [18] | Pwd MV E, A, E/A, DT TDI MV: e′, a′, E/e′ | n. 904 0–17 yrs | Age and BSA (Haycock) | Percentiles |
| Roberson DA 2007 USA [17] | TDI MV: e′, a′, s′ TV s′ | n. 634 0–18 yrs | Age, Heart rate | Z score charts only for e′, s′. TV s′ Z score equation not provided, R2 not provided |
| Cui W 2007 USA [16] | TDI, Pwd, M-mode: LV and RV Tei index | n. 289 0–18 yrs | Age groups | Mean ± SD |
| Author | Population | Measures | Software | Data Norm | Data Expression |
|---|---|---|---|---|---|
| Adar A 2019 USA [35] | N = 312 3 days–20.5 yrs | LV LS, CS, and synchrony; | Echo: Philips Epiq Software: QLAB v.10.5 (Philips) | Age groups | Mean, SD |
| Harrington JK 2021 USA [37] | N = 577 1–18 yrs | LV SR | Echo: Philips Software: QLAB 9.0 (Philips) | Age | Z-scores |
| Koopman LP 2019 The Netherlands [40] | N = 103 mean 10.8 yrs IQR 7.3–14.3 years. | LV LS, CS | Echo: Philips IE33 Software: QLAB 9.0 (Philips) | Age groups | Mean, SD Percentiles |
| Romanowicz J 2023 USA [52] | N = 1032 <21 years old | LV and RV LS, LV CS | Echo: Philips Epiq Software: Auto-strain, QLab 10.5 10.8 | Age | Mean, SD Z-scores |
| Kamel H 2022 Egypt [9] | N = 200 3.832 ± 1.522 yrs range 0.1–5.9 yrs | LV GLS, GCS, GRS 2d and 3D | Echo: Vivid E9 (GE). Software: EchoPAC V113 (GE) | Age groups | Mean, SD |
| Kotby AA 2023, Egypt [42] | N = 250 1–16 yrs | LV LS | Echo: GE Software: EchoPAC | Age groups | Mean, SD |
| Aristizábal-Duque CH 2022 Spain [43] | N = 156 6 t- 17 yrs | LVGLS, RVGLS, RV free wall LS, LA | Echo: Philips IE33 Software: 13.0 of QLab 13 (Philips) | Age groups, BSA | Mean, SD |
| Klistisic L, 2013 The Netherlands [45] | N = 183 0–19 yrs | LV LS, CS, RS | Echo: Vivid 7 GE Software: EchoPAC GE | Age groups | Mean, SD |
| Marcus K, 2011 USA [44] | N = 144 0–19 yrs | LV LS, CS, RS | Echo: Vivid 7 GE Software: EchoPAC GE | Age groups | Mean, SD |
| Zhang L, 2013 China [41] | N = 226 0–18 yrs | LV 3D STE LS, CS, RS | Echo: Philips IE33 Software: TomTec TTA2.00.03 | Age groups | Mean, SD |
| Cantinotti M, 2018 Italy [47] | N = 721 31 days–18 yrs | LV, LS, CS RV LS | Echo: Epiq/IE33 (Philips) Software: Q-LAB 9 Philips | Age groups, gender | Mean, SD |
| Dallaire F, 2016 Canada [46] | N = 233 1–18 yrs | LV LS, CS | Echo: Vivid 7 GE Software: EchoPAC GE 7 | BSA | Z-scores |
| Acheampong B, 2023 USA [34] | N 142 0–18 yrs | LV LS, CS, RS | Echo: Philips and Siemens Software: Cardiac Performance Analysis version 3.0 * | Age groups | Percentiles |
| Author | Population | Measures | Software | Data Norm | Data Expression |
|---|---|---|---|---|---|
| Cantinotti M, Italy [33] | N = 836 31 days–18 yrs | 2D LA and RA strain | Echo: Epiq/IE33 (Philips) Software: Q-LAB, and Q- LAB 10 (Philips) | Age groups | Mean, SD |
| Ghelani S, 2013 USA [49] [21] | N = 196 4 days–20.9 yrs | 3D LA volumes and strain | Echo: Philips IE33 Software: 4D LV Analysis, TomTec 3.1 | Age | Z-scores |
| Kutty S 2013, USA [50] | N = 153 3–20 yrs | 2D LA and RA strain | Echo: GE Vivid 7, Software: EchoPAC Bt11 GE | Age groups | Mean, SD |
| Jimbo S 2020 Japan [36] | N = 112 (median 12.0 years; range 6–16 years) | 2D LA strain and SR | Echo: NR Software: TomTec | Age groups | z-scores |
| Aristizábal-Duque CH 2022 Spain [43] | N = 156 6 t- 17 yrs | 2D LA strain | Echo: Philips IE33 Software: 13.0 of QLAB 13 (Philips) ° | Age groups, BSA | Mean, SD |
| Author | Sample Size | Measures | Echo Machine | Software | Normalization |
|---|---|---|---|---|---|
| Kubler JD 2018, Boston USA [58] | n. 238 0.4–17.9 yrs | 3D LV volumes, stress, and strain | Philips IE33 and Epiq | 4D LV Analysis; TomTec 3.1 | Z-score R2 NR |
| Jone PN 2021, Multicenter USA [59] | n. 698 0–18 yrs | 3D LV volumes | GE Vivid E9/E95; IE33/EPIQ, Siemens SC2000, | 4D LV Analysis, TomTec 4.0, | Z-score R2 NR |
| Krell K 2018 Multicenter Germany [60] | n. 370 1 day–219 months | 3D LV volumes | IE33, Philips | QLab 9.0 (Philips) and TomTec 4DLV2.7 | Percentiles |
| Cantinotti M 2019, Italy [62] | n. 800 118 yrs | 3D LV volumes | IE33, Philips | QLab 9.0 (Philips) | Z score R2 0.83–0.84 |
| Herberg U 2021 Multicenter Germany [61] | n. 545 1 day–216 months | 3D RV Volumes | IE33, Philips or Vivid 7, GE) | VMS, Ventripoint | Percentiles |
| Ghelani S, 2017 USA [49] | n. 196 4 days-20.9 yrs | LA volumes and strain | Philips IE33 | 4D LV Analysis; TomTec 3.1 | Z score R2 0.79–0.98 |
| Linden K, 2019, Germany [64] | n. 432 0 days–22 months | 3D LA volumes | Philips IE33 or Vivid E9/95) (GE) | 4D LV Analysis; TomTec 3.1 | Z score R2 NR |
| Poutnaen T, 2016, Finland [106] | n. 168 2–27 yrs | MVA, AVA | GE Vingmed System Five | GE | Mean SD |
| Poutanen T, 2003, Finland [103,105] | n.169 2-27 yrs | 3D LV and LA volumes, LV mass | GE Vingmed System Five | GE | Mean SD |
| Author | Population | Parameters Evaluated | Normalized By | Data Expression |
|---|---|---|---|---|
| Lu DF 2022, China [107] | 489, 264 M GA 32 (24–36.7) weeks BW 1700 (650–3180) g BSA 0.13 (0.07–0.20) m2 | M-mode: LV, LA, Ao, MV A, E, E/A | GA BW BSA | Percentiles R 0.07–0.616 |
| Wang S, 2022 China [109] | 1570 term and preterm | M-mode: LV, LA, Ao, | GA BW BSA L | Percentiles |
| Calado C, 2021 Australia [110] | 1244 Preterm infants ≤32 weeks ≤ 1500 g GA 27.3 ± 2.2 (22–32), weeks Age 2.2 ± 1.5 (1–7) days BW 999 ± 266.9 (349–1500) g BSA 0.10 ± 0.02 (0.05–0.14) m2 | M-mode: LV, LA, Ao, RVED | BW | Mean SD Percentiles |
| Abushaban L 2017 Kuwait [112] | 268, 26 M GA 29.8 (±2.38) weeks BW 1479 (±413 SD) g BSA 0.123 (0.07 to 0.19) m2 | MPA, LPA, RPA | BSA | Z-score, mean SD, R not reported, scatterplot indicates low R2 |
| Choudry S,2017, USA [113] | 503 < 2 kg BW 1.2 ± 0.74 kg GA 21.29 ± 22.56 BSA 0.11 ± 0.03 | M-mode: LV | Weight, L, BSA | Percentiles Z-score R2 NR |
| Skelton R 1998 UK [111] | 79 < 34 weeks BW 500–2499 g GW 23–33 weeks | M-mode: LV, Ao Doppler velocity: Asc Ao, Desc Ao, PA, MV, TV | BW, GA | Mean, range |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantinotti, M.; Marchese, P.; Capponi, G.; Franchi, E.; Santoro, G.; Pizzuto, A.; Assanta, N.; Giordano, R. Pediatric Echocardiographic Nomograms: Twenty Years of Advances—Do We Now Have a Complete and Reliable Tool, or Are Gaps Still Present? An Up-to-Date Review. J. Clin. Med. 2025, 14, 5215. https://doi.org/10.3390/jcm14155215
Cantinotti M, Marchese P, Capponi G, Franchi E, Santoro G, Pizzuto A, Assanta N, Giordano R. Pediatric Echocardiographic Nomograms: Twenty Years of Advances—Do We Now Have a Complete and Reliable Tool, or Are Gaps Still Present? An Up-to-Date Review. Journal of Clinical Medicine. 2025; 14(15):5215. https://doi.org/10.3390/jcm14155215
Chicago/Turabian StyleCantinotti, Massimiliano, Pietro Marchese, Guglielmo Capponi, Eliana Franchi, Giuseppe Santoro, Alessandra Pizzuto, Nadia Assanta, and Raffaele Giordano. 2025. "Pediatric Echocardiographic Nomograms: Twenty Years of Advances—Do We Now Have a Complete and Reliable Tool, or Are Gaps Still Present? An Up-to-Date Review" Journal of Clinical Medicine 14, no. 15: 5215. https://doi.org/10.3390/jcm14155215
APA StyleCantinotti, M., Marchese, P., Capponi, G., Franchi, E., Santoro, G., Pizzuto, A., Assanta, N., & Giordano, R. (2025). Pediatric Echocardiographic Nomograms: Twenty Years of Advances—Do We Now Have a Complete and Reliable Tool, or Are Gaps Still Present? An Up-to-Date Review. Journal of Clinical Medicine, 14(15), 5215. https://doi.org/10.3390/jcm14155215