
Preoperative Outcome Predictors in Aortic Valve Replacement: A Single-Center Retrospective Study
 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pittams, A.P.; Iddawela, S.; Zaidi, S.; Tyson, N.; Harky, A. Scoring Systems for Risk Stratification in Patients Undergoing Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1148–1156. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease: Developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA guideline for the Management of Patients with Valvular Heart Disease: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Crawford, T.C.; Magruder, J.T.; Grimm, J.C.; Suarez-Pierre, A.; Sciortino, C.M.; Mandal, K.; Zehr, K.J.; Conte, J.V.; Higgins, R.S.; Cameron, D.E.; et al. Complications after cardiac operations: All are not created equal. Ann. Thorac. Surg. 2017, 103, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Ball, L.; Costantino, F.; Pelosi, P. Postoperative complications of patients undergoing cardiac surgery. Curr. Opin. Crit. Care 2016, 22, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.; Algotsson, L.; Höglund, P.; Lührs, C.; Brandt, J. Comparison of 19 pre-operative risk stratification models in open-heart surgery. Eur. Heart J. 2006, 27, 867–874. [Google Scholar] [CrossRef]
- Perry, L.A.; Liu, Z.; Loth, J.; Penny-Dimri, J.C.; Plummer, M.; Segal, R.; Smith, J. Perioperative Neutrophil-Lymphocyte Ratio Predicts Mortality After Cardiac Surgery: Systematic Review and Meta-Analysis. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1296–1303. [Google Scholar] [CrossRef]
- Pál, K.; Mănescu, I.B.; Lupu, S.; Dobreanu, M. Emerging Biomarkers for Predicting Clinical Outcomes in Patients with Heart Disease. Life 2023, 13, 230. [Google Scholar] [CrossRef]
- Ye, L.; Shi, H.; Wang, X.; Duan, Q.; Ge, P.; Shao, Y. Elevated blood urea nitrogen to serum albumin ratio is an adverse prognostic predictor for patients undergoing cardiac surgery. Front. Cardiovasc. Med. 2022, 9, 888736. [Google Scholar] [CrossRef]
- Badem, S.; Pekcolaklar, A. Inflammatory prognostic index predicts new-onset atrial fibrillation and mortality after on-pump coronary artery bypass grafting. Rev. Assoc. Med. Bras. 2023, 69, e20230226. [Google Scholar] [CrossRef]
- Chen, Q.J.; Qu, H.J.; Li, D.Z.; Li, X.M.; Zhu, J.J.; Xiang, Y.; Li, L.; Ma, Y.T.; Yang, Y.N. Prognostic nutritional index predicts clinical outcome in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Sci. Rep. 2017, 7, 3285. [Google Scholar] [CrossRef]
- Lin, Z.; Zhao, Y.; Xiao, L.; Qi, C.; Chen, Q.; Li, Y. Blood urea nitrogen to serum albumin ratio as a new prognostic indicator in critical patients with chronic heart failure. ESC Heart Fail. 2022, 9, 1360–1369. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, T.; Ma, C.; Li, Q.; Liu, J.; Zhang, Z.; Xia, J. Predictive value of novel inflammatory indexes for in-hospital outcomes of patients with acute myocardial infarction. Chin. Circ. J. 2023, 38, 414–420. [Google Scholar]
- Thaden, J.J.; Nkomo, V.T.; Enriquez-Sarano, M. The global burden of aortic stenosis. Prog. Cardiovasc. Dis. 2014, 56, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Xie, W.; Wang, P.; Jiang, S.; Hua, Y.; Shao, G.; Li, Z. The relationship between blood urea nitrogen to serum albumin ratio and cardiovascular diseases, cardiovascular mortality, and all-cause mortality in patients with diabetes mellitus. Front. Endocrinol. 2025, 16, 1456731. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Duan, H.; Liu, J.; Shi, X.; Zhang, Y.; Zhang, Q.; Zhao, M.; Zhang, Y. Blood urea nitrogen to serum albumin ratio is associated with all-cause mortality in patients with AKI: A cohort study. Front. Nutr. 2024, 11, 1353956. [Google Scholar] [CrossRef]
- Wang, Y.; Gao, S.; Hong, L.; Hou, T.; Liu, H.; Li, M.; Yang, S.; Zhang, Y. Prognostic impact of blood urea nitrogen to albumin ratio on patients with sepsis: A retrospective cohort study. Sci. Rep. 2023, 13, 10013. [Google Scholar] [CrossRef]
- Fang, J.; Xu, B. Blood urea nitrogen to serum albumin ratio independently predicts mortality in critically ill patients with acute pulmonary embolism. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211010241. [Google Scholar] [CrossRef]
- Cauthen, C.A.; Lipinski, M.J.; Abbate, A.; Appleton, D.; Nusca, A.; Varma, A.; Goudreau, E.; Cowley, M.J.; Vetrovec, G.W. Relation of blood urea nitrogen to long-term mortality in patients with heart failure. Am. J. Cardiol. 2008, 101, 1643–1647. [Google Scholar] [CrossRef]
- Kazory, A. Emergence of blood urea nitrogen as a biomarker of neurohormonal activation in heart failure. Am. J. Cardiol. 2010, 106, 694–700. [Google Scholar] [CrossRef]
- Dirican, N.; Dirican, A.; Anar, C.; Atalay, S.; Ozturk, O.; Bircan, A.; Akkaya, A.; Cakir, M. A new inflammatory prognostic index, based on C-reactive protein, the neutrophil to lymphocyte ratio and serum albumin is useful for predicting prognosis in non-small cell lung cancer cases. Asian Pac. J. Cancer Prev. 2016, 17, 5101–5106. [Google Scholar]
- Tomita, M.; Ayabe, T.; Maeda, R.; Nakamura, K. The inflammatory prognostic index predicts cancer-specific outcomes of patients with resected non-small cell lung cancer. Asian Pac. J. Cancer Prev. 2018, 19, 2867–2870. [Google Scholar] [CrossRef]
- Erdoğan, A.P.; Ekinci, F.; Karabaş, A.; Balçık, O.Y.; Barutça, S.; Dirican, A. Could the Inflammatory Prognostic Index Predict the Efficacy of Regorafenib in Patients with Metastatic Colorectal Cancer? J. Gastrointest. Cancer 2022, 53, 45–51. [Google Scholar] [CrossRef]
- Jiang, Y.; Luo, B.; Chen, Y.; Peng, Y.; Lu, W.; Chen, L.; Lin, Y. Predictive value of inflammatory prognostic index for contrast-induced nephropathy in patients undergoing coronary angiography and/or percutaneous coronary intervention. Sci. Rep. 2024, 14, 15861. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Tao, N.; Wang, T.; Zhang, Z.; Wu, Q. The relationship between composite inflammatory indicators and short-term outcomes in patients with heart failure. Int. J. Cardiol. 2025, 420, 132755. [Google Scholar] [CrossRef] [PubMed]
- Corti, M.-C.; Guralnik, J.M.; Salive, M.E.; Sorkin, J.D. Serum Albumin Level and Physical Disability as Predictors of Mortality in Older Persons. JAMA 1994, 272, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Kudsk, K.A.; Tolley, E.A.; DeWitt, R.C.; Janu, P.G.; Blackwell, A.P.; Yeary, S.; King, B.K. Preoperative albumin and surgical site identify surgical risk for major postoperative complications. J. Parenter. Enter. Nutr. 2003, 27, 1–9. [Google Scholar] [CrossRef]
- Gibbs, J.; Cull, W.; Henderson, W.; Daley, J.; Hur, K.; Khuri, S.F. Preoperative Serum Albumin Level as a Predictor of Operative Mortality and Morbidity: Results from the National VA Surgical Risk Study. Arch. Surg. 1999, 134, 36–42. [Google Scholar] [CrossRef]
- Chien, S.C.; Chen, C.Y.; Lin, C.F.; Yeh, H.I. Critical appraisal of the role of serum albumin in cardiovascular disease. Biomark. Res. 2017, 5, 31. [Google Scholar] [CrossRef]
- Cabrerizo, S.; Cuadras, D.; Gomez-Busto, F.; Artaza-Artabe, I.; Marín-Ciancas, F.; Malafarina, V. Serum albumin and health in older people: Review and meta analysis. Maturitas 2015, 81, 17–27. [Google Scholar] [CrossRef]
- Patel, D.A.; Lavie, C.J.; Milani, R.V.; Shah, S.; Gilliland, Y. Clinical implications of left atrial enlargement: A review. Ochsner J. 2009, 9, 191–196. [Google Scholar]
- Casaclang-Verzosa, G.; Malouf, J.F.; Scott, C.G.; Juracan, E.M.; Nishimura, R.A.; Pellikka, P.A. Does left atrial size predict mortality in asymptomatic patients with severe aortic stenosis? Echocardiography 2010, 27, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Beach, J.M.; Mihaljevic, T.; Rajeswaran, J.; Marwick, T.; Edwards, S.T.; Nowicki, E.R.; Thomas, J.; Svensson, L.G.; Griffin, B.; Gillinov, A.M.; et al. Ventricular hypertrophy and left atrial dilatation persist and are associated with reduced survival after valve replacement for aortic stenosis. J. Thorac. Cardiovasc. Surg. 2014, 147, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Rusinaru, D.; Bohbot, Y.; Kowalski, C.; Ringle, A.; Maréchaux, S.; Tribouilloy, C. Left Atrial Volume and Mortality in Patients With Aortic Stenosis. J. Am. Heart Assoc. 2017, 6, e006615. [Google Scholar] [CrossRef] [PubMed]
- Christensen, N.L.; Dahl, J.S.; Carter-Storch, R.; Bakkestrøm, R.; Pecini, R.; Steffensen, F.H.; Søndergaard, E.V.; Videbæk, L.M.; Møller, J.E. Relation of Left Atrial Size, Cardiac Morphology, and Clinical Outcome in Asymptomatic Aortic Stenosis. Am. J. Cardiol. 2017, 120, 1877–1883. [Google Scholar] [CrossRef] [PubMed]
- Butcher, S.C.; Fortuni, F.; Kong, W.; Vollema, E.M.; Prevedello, F.; Perry, R.; Ng, A.C.T.; Poh, K.K.; Almeida, A.G.; González-Gómez, A.; et al. Prognostic implications of left atrial dilation in aortic regurgitation due to bicuspid aortic valve. Heart 2022, 108, 137–144. [Google Scholar] [CrossRef]
- Sullivan, P.G.; Wallach, J.D.; Ioannidis, J.P. Meta-Analysis Comparing Established Risk Prediction Models (EuroSCORE II, STS Score, and ACEF Score) for Perioperative Mortality During Cardiac Surgery. Am. J. Cardiol. 2016, 118, 1574–1582. [Google Scholar] [CrossRef]
- Cromhout, P.F.; Berg, S.K.; Moons, P.; Damgaard, S.; Nashef, S.; Thygesen, L.C. Updating EuroSCORE by including emotional, behavioural, social and functional factors to the risk assessment of patients undergoing cardiac surgery: A study protocol. BMJ Open 2019, 9, e026745. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Cohort (n = 195) |
|---|---|
| Age (years) mean ± SD | 66.1 ± 11.6 |
| Male (%) | 62.5 |
| BMI (kg/m2) ± SD | 26.9 ± 4.2 |
| Smoking (%) | 16 |
| Hypertension (%) | 63.5 |
| Dyslipidemia (%) | 44.6 |
| Diabetes mellitus (%) | 17.9 |
| Hospital stay, day, mean ± SD | 8.5 ± 4 |
| Valve disease | |
| Aortic stenosis (%) | 64.6 |
| Aortic regurgitation (%) | 35.4 |
| Bicuspid valve (%) | 43.5 |
| Therapy | |
| Anti-hyperlipidemic (%) | 41.5 |
| Anti-hypertensive (%) | 73.3 |
| Antiplatelet (%) | 33.3 |
| Anticoagulant (%) | 7.2 |
| Antidiabetic drugs | 17.9 |
| Type of surgery | |
| AVR (%) | 56.5 |
| AVR and CABG (%) | 7.3 |
| AVR and Aorta surgery (%) | 23.2 |
| Aortic, mitral valve surgery (%) | 4.6 |
| Aortic, mitral and aorta valve surgery (%) | 2.7 |
| AVR and LAAC (%) | 1.5 |
| AVR, Aorta, LAAC (%) | 1.05 |
| AVR, Aorta, CABG (%) | 0.6 |
| Aortic, mitral valve and LAAC (%) | 1.5 |
| Aortic, mitral valve and CABG (%) | 1.05 |
| Surgical incisions | |
| Full sternotomy (%) | 29.3 |
| Mini-sternotomy (%) | 51.7 |
| Mini-thoracotomies (%) | 19 |
| Major adverse complications | |
| Surgical re-exploration n, (%) | 23 (11.8) |
| Cerebral ischemia n, (%) | 1 (0.5) |
| Death n, (%) | 1 (0.5) |
| Characteristics | MAC Group (n = 25) | noMAC Group (n = 170) | p Value |
|---|---|---|---|
| Clinical characteristics | |||
| Age (years) mean ± SD | 67.7 ± 11.6 | 65.8 ± 11.6 | ns |
| Male (%) | 60 | 63.5 | ns |
| BMI (kg/m2) ± SD | 26.8 ± 5.1 | 26.9 ± 4.1 | ns |
| Smoking (%) | 15.3 | 24 | ns |
| Hypertension (%) | 52 | 65.3 | ns |
| Dyslipidemia (%) | 48 | 44.1 | ns |
| Diabetes mellitus (%) | 20 | 17.6 | ns |
| Atrial fibrillation (%) | 12 | 7.6 | ns |
| Post-operative atrial fibrillation (%) | 44 | 35.3 | ns |
| Hospital stay (day), mean ± SD | 16.3 ± 7 | 9.5 ± 3.3 | <0.0001 |
| Valve disease | |||
| Aortic stenosis (%) | 60 | 65.3 | ns |
| Aortic regurgitation (%) | 40 | 34.7 | ns |
| Type of valve | |||
| Bicuspid valve (%) | 28 | 47 | 0.04 |
| Tricuspid valve (%) | 72 | 53 | 0.04 |
| Therapy | |||
| Anti-hyperlipidemic (%) | 40 | 42.1 | ns |
| Anti-hypertensive (%) | 72 | 74 | ns |
| Antiplatelet (%) | 36 | 32.9 | ns |
| Anticoagulant (%) | 12 | 5.9 | ns |
| Antidiabetic drugs(%) | 16 | 18.3 | ns |
| Type of surgery | |||
| AVR (%) | 44 | 58 | ns |
| AVR and CABG (%) | 8 | 7 | ns |
| AVR and aorta surgery (%) | 16 | 24 | ns |
| Aortic, mitral valve surgery (%) | 16 | 3 | ns |
| Aortic, mitral valve and aorta surgery (%) | 8 | 2 | ns |
| AVR and LAAC (%) | 0 | 2 | ns |
| AVR, aorta, LAAC | 0 | 1 | ns |
| AVR, aorta, CABG | 0 | 1 | ns |
| Aortic, mitral valve and LAAC | 4 | 1 | ns |
| Aortic, mitral valve and CABG | 4 | 1 | ns |
| Surgical incisions | |||
| Full sternotomy (%) | 52 | 25.9 | 0.01 |
| Mini-sternotomy (%) | 24 | 55.3 | 0.003 |
| Mini-thoracotomies (%) | 24 | 18.2 | ns |
| Echocardiographic parameters | |||
| Aorta diameter (mm), mean ± SD | 36.20 ± 9.8 | 39.1 ± 8.1 | ns |
| Aortic root diameter (mm), mean ± SD | 35.2 ± 9.3 | 35.8 ± 6.1 | ns |
| Left atrium volume (mL), mean ± SD | 47.3 ± 29.2 | 36.6 ± 13.4 | 0.004 |
| Left atrium volume index (LAVI) (mL/m2) mean ± SD | 26.1 ± 20.4 | 19.5 ± 7.4 | 0.004 |
| Left atrium area (cm2), mean ± SD | 24.8 ± 5.9 | 22.3 ± 8.2 | ns |
| Left ventricular end-systolic dimension (mm), mean ± SD | 51.3 ± 7.4 | 52.9 ± 11.8 | ns |
| Left ventricular end-systolic volume (mL), mean ± SD | 131.2 ± 48.4 | 134.9 ± 57.6 | ns |
| Ejection fraction (%), mean ± SD | 61.4 ± 6.9 | 60.8 ± 8.5 | ns |
| Peak velocity (m/sec), mean ± SD | 3.56 ± 1.24 | 3.55 ± 1.26 | ns |
| Mean gradient (mmHg), mean ± SD | 42.5 ± 21.9 | 40.9 ± 21.7 | ns |
| Posterior wall thickness (mm), mean ± SD | 10.5 ± 2.3 | 10.8 ± 7.8 | ns |
| Interventricular septum thickness (mm), mean ± SD | 12.5 ± 2.9 | 12.2 ± 2.1 | ns |
| Laboratory clinical-chemistry data | |||
| Hemoglobin (Hb), g/dL | 13.6 ± 1.8 | 13.8 ± 1.5 | ns |
| Erythrocytes, ×106/μL | 4.6 ± 0.5 | 4.7 ± 0.6 | ns |
| Neutrophils, ×103/μL | 4.15 ± 1.34 | 4.1 ± 1.46 | ns |
| Lymphocytes, ×103/μL | 1.89 ± 0.7 | 1.85 ± 0.5 | ns |
| Monocytes, ×103/μL | 0.61 ± 0.17 | 0.61 ± 0.6 | ns |
| Platelets, ×103/μL | 204 ± 58.8 | 226 ± 64.2 | ns |
| Erythrocyte sedimentary rate, mm/h | 10.2 ± 11.7 | 10.8 ± 9.1 | ns |
| C-reactive protein (CRP), mg/dL | 0.37 ± 0.4 | 0.28 ± 0.4 | ns |
| Fibrinogen, mg/dL | 346.4 ± 115.2 | 349.8 ± 90.5 | ns |
| Glucose mg/dL | 95.7 ± 15 | 101.6 ± 19 | ns |
| Total cholesterol, mg/dL | 162.7 ± 38.2 | 176.8 ± 38.8 | ns |
| Low-density lipoprotein cholesterol, mg/dL | 91 ± 34.6 | 102 ± 35.2 | ns |
| High-density lipoprotein cholesterol, mg/dL | 53.4 ± 15.1 | 55.2 ± 15.6 | ns |
| Triglycerides, mg/dL | 91.2 ± 43.2 | 101.3 ± 49.2 | ns |
| Lipoprotein(a), nmol/L | 51.3 ± 70.5 | 54.1 ± 66.7 | ns |
| Creatinine, mg/dL | 0.99 ± 0.2 | 0.92 ± 0.5 | ns |
| Creatine phosphokinase, IU/L | 106.7 ± 65.1 | 110 ± 80.5 | ns |
| Alanine aminotransferase, IU/L | 22.7 ± 18.9 | 20.6 ± 15.3 | ns |
| Gamma-glutamyl transferase, IU/L | 37.2 ± 41 | 42 ± 81 | ns |
| Thyroid-stimulating hormone, mU/L | 5.8 ± 15 | 7.4 ± 60 | ns |
| Albumin, g/dL | 4.2 ± 0.3 | 4.3 ± 0.2 | ns |
| Urea mg/dL | 45.6 ± 13.9 | 39.8 ± 12.8 | 0.04 |
| BAR, mean ± SD | 10.8 ±3.7 | 8.8 ± 3.8 | 0.02 |
| IPI, mean ± SD | 0.28 ± 0.4 | 0.14 ± 0.2 | 0.01 |
| Variables | OR | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Univariate analysis | |||
| LAVI | 1.03 | 1.005–1.05 | 0.01 |
| BAR | 1.1 | 1.0–1.2 | 0.03 |
| IPI | 4.06 | 1.15–14.2 | 0.02 |
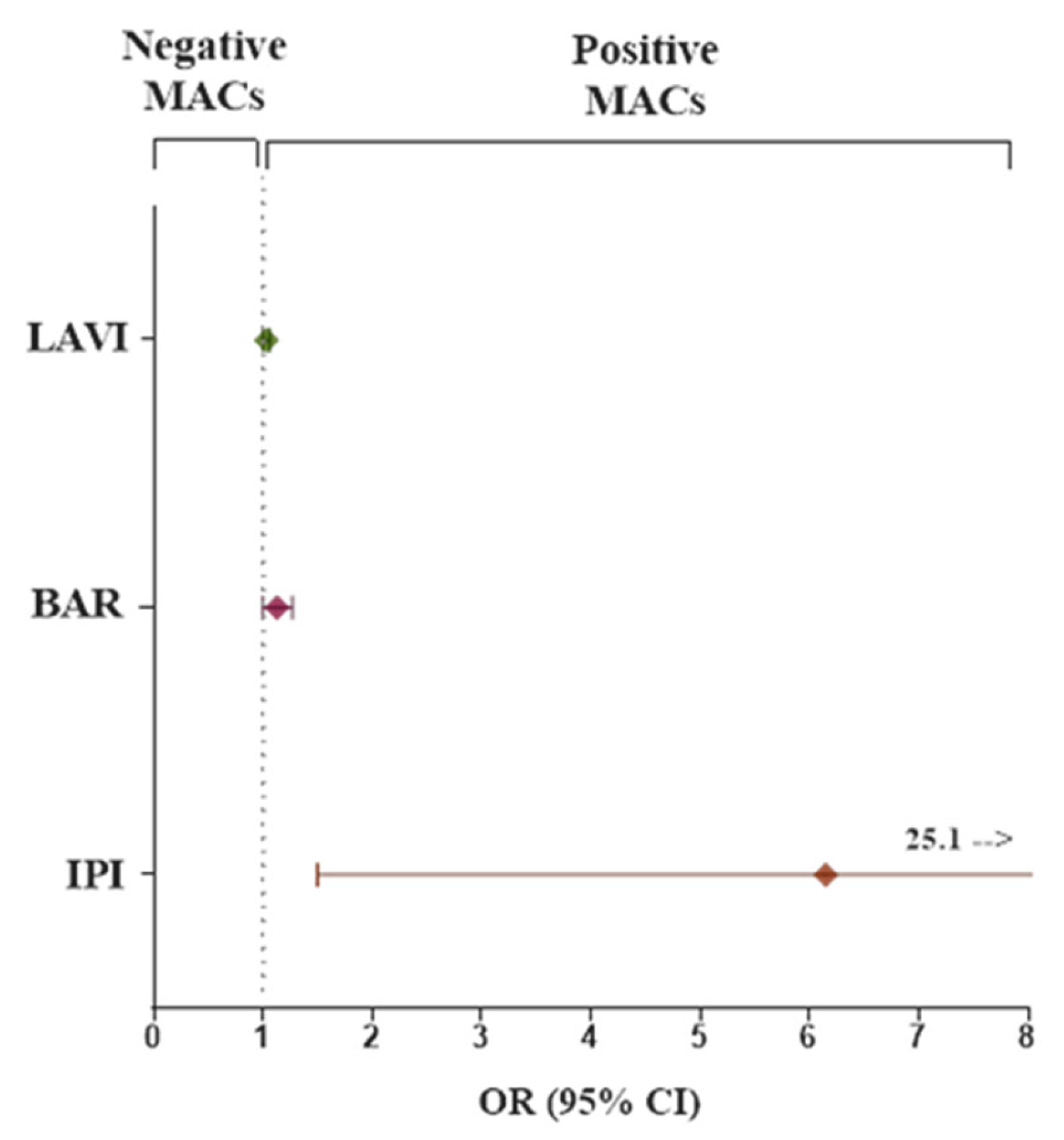
| Multivariate analysis * | |||
| LAVI | 1.031 | 1.001–1.062 | 0.04 |
| BAR | 1.13 | 1–1.27 | 0.04 |
| IPI | 6.15 | 1.5–25.1 | 0.01 |
| Variables | OR | 95% Confidence Interval | p-Value |
|---|---|---|---|
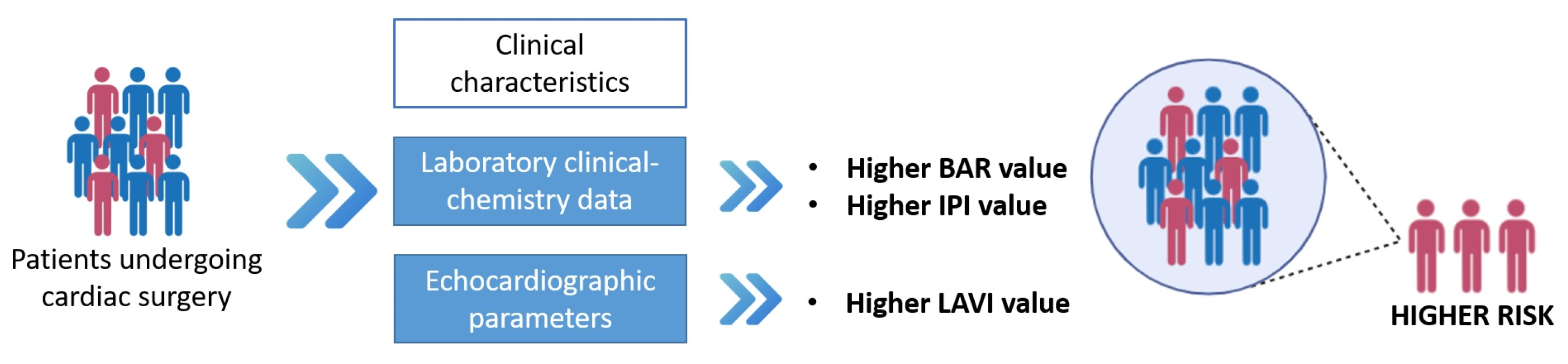
| higher LAVI | 2.5 | 1.1–5.9 | 0.04 |
| higher IPI | 1.7 | 1.0–4.3 | 0.05 |
| higher BAR | 3.7 | 1.5–9.0 | 0.004 |
| higher LAVI + higher BAR | 9.8 | 2.8–34.3 | 0.0003 |
| higher LAVI + higher IPI | 4.5 | 1.3–16.5 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foffa, I.; Esposito, A.; Simonini, L.; Lombardi, R.; Parri, M.S.; Monteleone, A.; Farneti, P.A.; Vecoli, C. Preoperative Outcome Predictors in Aortic Valve Replacement: A Single-Center Retrospective Study. J. Clin. Med. 2025, 14, 5196. https://doi.org/10.3390/jcm14155196
Foffa I, Esposito A, Simonini L, Lombardi R, Parri MS, Monteleone A, Farneti PA, Vecoli C. Preoperative Outcome Predictors in Aortic Valve Replacement: A Single-Center Retrospective Study. Journal of Clinical Medicine. 2025; 14(15):5196. https://doi.org/10.3390/jcm14155196
Chicago/Turabian StyleFoffa, Ilenia, Augusto Esposito, Ludovica Simonini, Roberta Lombardi, Maria Serena Parri, Angelo Monteleone, Pier Andrea Farneti, and Cecilia Vecoli. 2025. "Preoperative Outcome Predictors in Aortic Valve Replacement: A Single-Center Retrospective Study" Journal of Clinical Medicine 14, no. 15: 5196. https://doi.org/10.3390/jcm14155196
APA StyleFoffa, I., Esposito, A., Simonini, L., Lombardi, R., Parri, M. S., Monteleone, A., Farneti, P. A., & Vecoli, C. (2025). Preoperative Outcome Predictors in Aortic Valve Replacement: A Single-Center Retrospective Study. Journal of Clinical Medicine, 14(15), 5196. https://doi.org/10.3390/jcm14155196