
Glasgow Coma Scale Score at Admission in Traumatic Brain Injury Patients: A Multicenter Observational Analysis

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Data
2.3. Statistical Analysis
3. Results
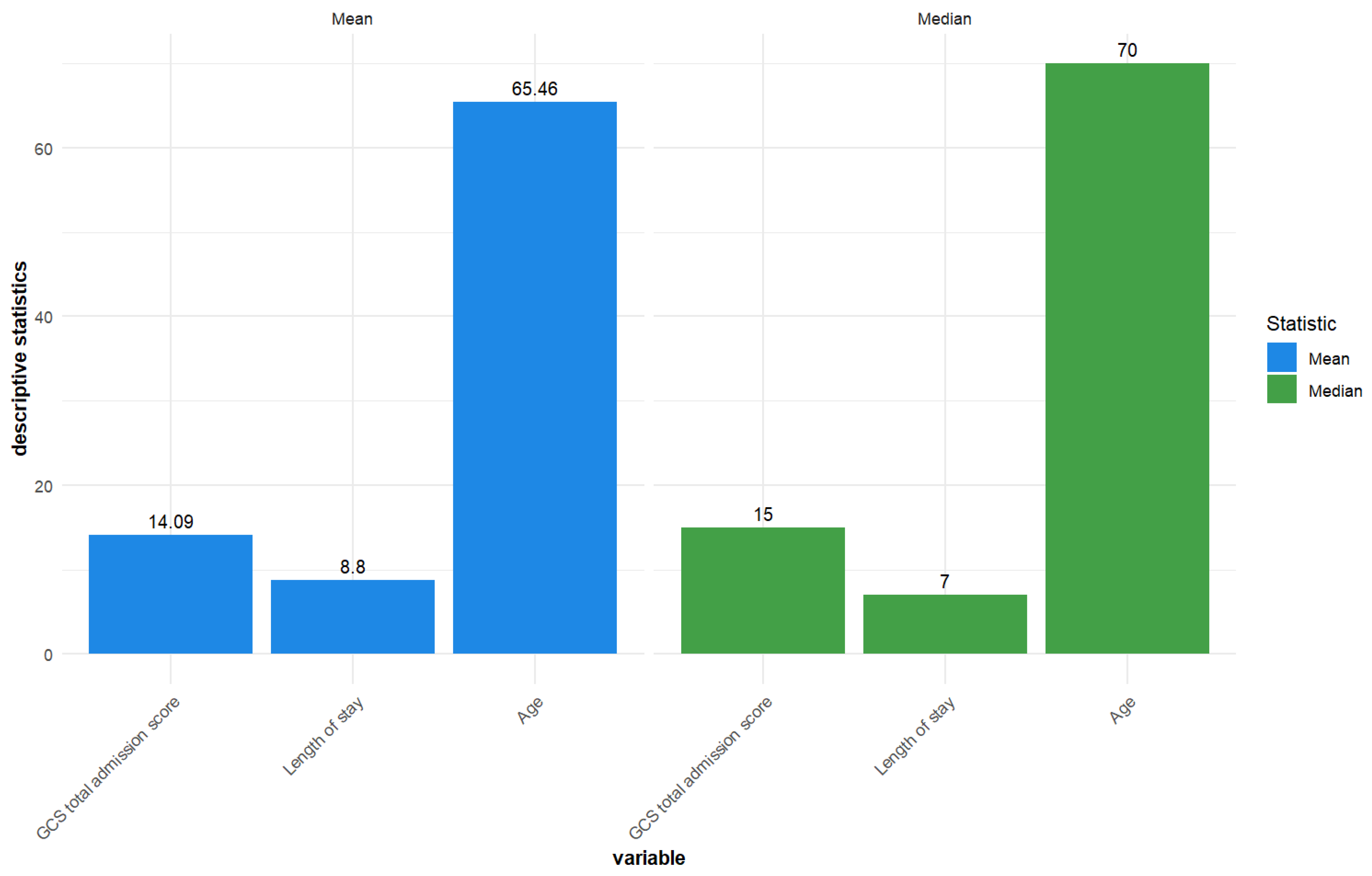
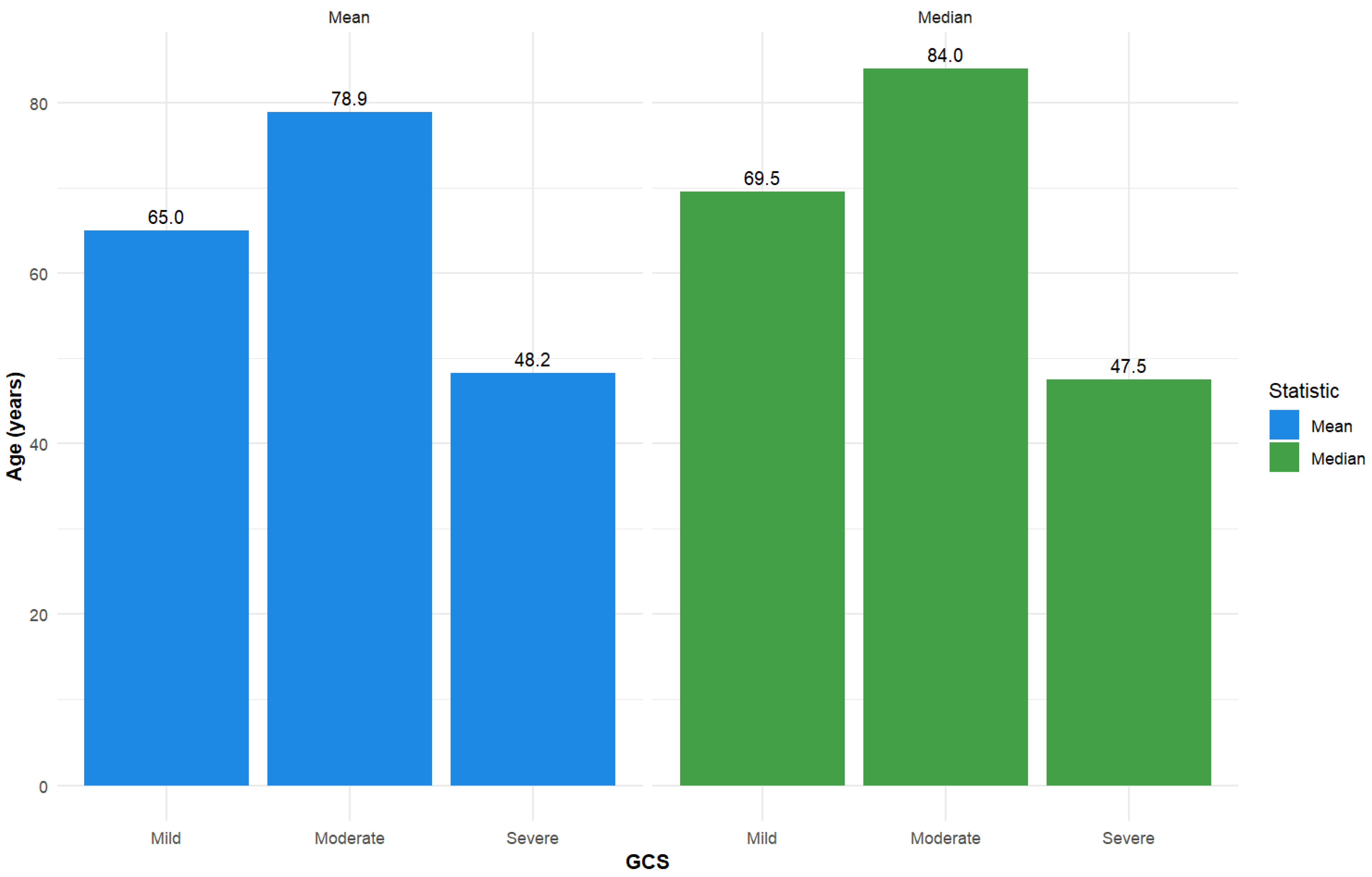
3.1. Descriptive Statistics
3.2. Wilcoxon Results
3.3. Kruskal–Wallis
3.4. Spearman Correlations
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kaplan, Z.L.R.; Van Der Vlegel, M.; Van Dijck, J.T.J.M.; Pisică, D.; Van Leeuwen, N.; Lingsma, H.F.; Steyerberg, E.W.; Haagsma, J.A.; Majdan, M.; Polinder, S.; et al. Intramural Healthcare Consumption and Costs After Traumatic Brain Injury: A Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Study. J. Neurotrauma 2023, 40, 2126–2145. [Google Scholar] [CrossRef]
- Wiles, M.D. Management of traumatic brain injury: A narrative review of current evidence. Anaesthesia 2022, 77, 102–112. [Google Scholar] [CrossRef]
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [PubMed]
- Rauchman, S.H.; Albert, J.; Pinkhasov, A.; Reiss, A.B. Mild-to-Moderate Traumatic Brain Injury: A Review with Focus on the Visual System. Neurol. Int. 2022, 14, 453–470. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, B.M.; Koskinen, L.-O.D. Classification and Characterization of Traumatic Brain Injuries in the Northern Region of Sweden. J. Clin. Med. 2023, 13, 8. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Pacheco, V.; Vargas-Medrano, J.; Tran, E.; Nicolas, M.; Price, D.; Patel, R.; Tonarelli, S.; Gadad, B.S. Prognosis and Diagnostic Biomarkers of Mild Traumatic Brain Injury: Current Status and Future Prospects. J. Alzheimer’s Dis. 2022, 86, 943–959. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Manley, G.T.; Abrams, M.; Åkerlund, C.; Andelic, N.; Aries, M.; Bashford, T.; Bell, M.J.; Bodien, Y.G.; et al. Traumatic brain injury: Progress and challenges in prevention, clinical care, and research. Lancet Neurol. 2022, 21, 1004–1060. [Google Scholar] [CrossRef]
- Wilson, M.H.; Ashworth, E.; Hutchinson, P.J.; On behalf of the British Neurotrauma Group. A proposed novel traumatic brain injury classification system—An overview and inter-rater reliability validation on behalf of the Society of British Neurological Surgeons. Br. J. Neurosurg. 2022, 36, 633–638. [Google Scholar] [CrossRef]
- Salottolo, K.; Panchal, R.; Madayag, R.M.; Dhakal, L.; Rosenberg, W.; Banton, K.L.; Hamilton, D.; Bar-Or, D. Incorporating age improves the Glasgow Coma Scale score for predicting mortality from traumatic brain injury. Trauma Surg. Acute Care Open 2021, 6, e000641. [Google Scholar] [CrossRef]
- Teasdale, G.; Maas, A.; Lecky, F.; Manley, G.; Stocchetti, N.; Murray, G. The Glasgow Coma Scale at 40 years: Standing the test of time. Lancet Neurol. 2014, 13, 844–854. [Google Scholar] [CrossRef]
- Pisano, F.; Bilotta, F. The Predictive Value of the Verbal Glasgow Coma Scale in Traumatic Brain Injury: A Systematic Review. J. Head Trauma Rehabil. 2024, 39, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, S.; Sarveazad, A.; Babahajian, A.; Ahmadzadeh, K.; Yousefifard, M. Comparison of Glasgow Coma Scale and Full Outline of UnResponsiveness score for prediction of in-hospital mortality in traumatic brain injury patients: A systematic review and meta-analysis. Eur. J. Trauma Emerg. Surg. 2023, 49, 1693–1706. [Google Scholar] [CrossRef] [PubMed]
- Bae, I.-S.; Chun, H.-J.; Yi, H.-J.; Choi, K.-S. Using components of the Glasgow coma scale and Rotterdam CT scores for mortality risk stratification in adult patients with traumatic brain injury: A preliminary study. Clin. Neurol. Neurosurg. 2020, 188, 105599. [Google Scholar] [CrossRef] [PubMed]
- Ogunlade, J.; Elia, C.; Duong, J.; Yanez, P.J.; Dong, F.; Wacker, M.R.; Menoni, R.; Goldenberg, T.; Miulli, D.E. Severe Traumatic Brain Injury Requiring Surgical Decompression in the Young Adult: Factors Influencing Morbidity and Mortality—A Retrospective Analysis. Cureus 2018, 10, e3042. [Google Scholar] [CrossRef]
- Leitgeb, J.; Mauritz, W.; Brazinova, A.; Majdan, M.; Janciak, I.; Wilbacher, I.; Rusnak, M. Glasgow Coma Scale score at intensive care unit discharge predicts the 1-year outcome of patients with severe traumatic brain injury. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2013, 39, 285–292. [Google Scholar] [CrossRef]
- Sharbafshaaer, M. Impacts of cognitive impairment for different levels and causes of traumatic brain injury, and education status in TBI patients. Dement. Neuropsychol. 2018, 12, 415–420. [Google Scholar] [CrossRef]
- Smith, P.D.; Shukla, I.; Azam, F.; Trautmann, D.; Gee, E.; Korb, M.; Pitonak, M.; Srinivasan, S.; Caruso, J.P.; Caldwell, C.; et al. Predictive factors for traumatic cerebral contusion volume, expansion, and outcomes. J. Neurosurg. 2025, 142, 1616–1624. [Google Scholar] [CrossRef]
- Taussky, P. Outcome after acute traumatic subdural and epidural hematoma in Switzerland: A single center experience. Swiss Med. Wkly. 2008, 138, 281–285. [Google Scholar] [CrossRef]
- Kulesza, B.; Mazurek, M.; Nogalski, A.; Rola, R. Factors with the strongest prognostic value associated with in-hospital mortality rate among patients operated for acute subdural and epidural hematoma. Eur. J. Trauma Emerg. Surg. 2021, 47, 1517–1525. [Google Scholar] [CrossRef]
- Lazaridis, C.; Yang, M.; DeSantis, S.M.; Luo, S.T.; Robertson, C.S. Predictors of intensive care unit length of stay and intracranial pressure in severe traumatic brain injury. J. Crit. Care 2015, 30, 1258–1262. [Google Scholar] [CrossRef] [PubMed]
- Mkubwa, J.J.; Bedada, A.G.; Esterhuizen. Traumatic brain injury: Association between the Glasgow Coma Scale score and intensive care unit mortality. S. Afr. J. Crit. Care 2022, 38, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Karibe, H.; Hayashi, T.; Narisawa, A.; Kameyama, M.; Nakagawa, A.; Tominaga, T. Clinical Characteristics and Outcome in Elderly Patients with Traumatic Brain Injury: For Establishment of Management Strategy. Neurol. Med. Chir. 2017, 57, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Hui, J.; Yang, C.; Jiang, J.; Xie, L.I.; Feng, J. In-hospital mortality and risk factors among elderly patients with traumatic brain injury: Protocol for a systematic review and meta-analysis. BMJ Open 2023, 13, e065371. [Google Scholar] [CrossRef]
- Yang, C.; Lang, L.; He, Z.; Hui, J.; Jiang, J.; Gao, G.; Feng, J. Epidemiological Characteristics of Older Patients with Traumatic Brain Injury in China. J. Neurotrauma 2022, 39, 850–859. [Google Scholar] [CrossRef]
- Salottolo, K.; Levy, A.S.; Slone, D.S.; Mains, C.W.; Bar-Or, D. The effect of age on Glasgow Coma Scale score in patients with traumatic brain injury. JAMA Surg. 2014, 149, 727–734. [Google Scholar] [CrossRef]
- Kehoe, A.; Smith, J.E.; Bouamra, O.; Edwards, A.; Yates, D.; Lecky, F. Older patients with traumatic brain injury present with a higher GCS score than younger patients for a given severity of injury. Emerg. Med. J. 2016, 33, 381–385. [Google Scholar] [CrossRef]
- Ma, Z.; He, Z.; Li, Z.; Gong, R.; Hui, J.; Weng, W.; Wu, X.; Yang, C.; Jiang, J.; Xie, L.; et al. Traumatic brain injury in elderly population: A global systematic review and meta-analysis of in-hospital mortality and risk factors among 2.22 million individuals. Ageing Res. Rev. 2024, 99, 102376. [Google Scholar] [CrossRef]
- Hukkelhoven, C.W.P.M.; Steyerberg, E.W.; Rampen, A.J.J.; Farace, E.; Habbema, J.D.F.; Marshall, L.F.; Murray, G.D.; Maas, A.I.R. Patient age and outcome following severe traumatic brain injury: An analysis of 5600 patients. J. Neurosurg. 2003, 99, 666–673. [Google Scholar] [CrossRef]
- Lu, H.-Y.; Li, T.-C.; Tu, Y.-K.; Tsai, J.-C.; Lai, H.-S.; Kuo, L.-T. Predicting long-term outcome after traumatic brain injury using repeated measurements of Glasgow Coma Scale and data mining methods. J. Med. Syst. 2015, 39, 14. [Google Scholar] [CrossRef]
- Kouloulas, E.J.; Papadeas, A.G.; Michail, X.; Sakas, D.E.; Boviatsis, E.J. Prognostic value of time-related Glasgow coma scale components in severe traumatic brain injury: A prospective evaluation with respect to 1-year survival and functional outcome. Int. J. Rehabil. Res. 2013, 36, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Ratcliff, J.J.; Adeoye, O.; Lindsell, C.J.; Hart, K.W.; Pancioli, A.; McMullan, J.T.; Yue, J.K.; Nishijima, D.K.; Gordon, W.A.; Valadka, A.B.; et al. ED disposition of the Glasgow Coma Scale 13 to 15 traumatic brain injury patient: Analysis of the Transforming Research and Clinical Knowledge in TBI study. Am. J. Emerg. Med. 2014, 32, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Haines, K.L.; Nguyen, B.P.; Vatsaas, C.; Alger, A.; Brooks, K.; Agarwal, S.K. Socioeconomic Status Affects Outcomes After Severity-Stratified Traumatic Brain Injury. J. Surg. Res. 2019, 235, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Humphries, T.J.; Ingram, S.; Sinha, S.; Lecky, F.; Dawson, J.; Singh, R. The effect of socioeconomic deprivation on 12 month Traumatic Brain Injury (TBI) outcome. Brain Inj. 2020, 34, 343–349. [Google Scholar] [CrossRef]
- Eom, K.S.; Kim, J.H.; Yoon, S.H.; Lee, S.; Park, K.-J.; Ha, S.-K.; Choi, J.; Jo, K.-W.; Kim, J.; Kang, S.H.; et al. Gender differences in adult traumatic brain injury according to the Glasgow coma scale: A multicenter descriptive study. Chin. J. Traumatol. 2021, 24, 333–343. [Google Scholar] [CrossRef]
- Slewa-Younan, S.; Green, A.M.; Baguley, I.J.; Gurka, J.A.; Marosszeky, J.E. Sex differences in injury severity and outcome measures after traumatic brain injury. Arch. Phys. Med. Rehabil. 2004, 85, 376–379. [Google Scholar] [CrossRef]
- Joshi, S.; Paudel, P.; Shah, D.B.; Karki, P.; Sharma, G.R. Association of the Presenting Glasgow Coma Scale in patients who requires ICU admission or operative intervention following traumatic brain injury with the Marshall computed tomography (CT) classification of traumatic brain injury. Nepal Mediciti Med. J. 2022, 3, 8–11. [Google Scholar] [CrossRef]
- Armstrong, R.A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef]
- Rau, C.-S.; Wu, S.-C.; Chen, Y.-C.; Chien, P.-C.; Hsieh, H.-Y.; Kuo, P.-J.; Hsieh, C.-H. Effect of Age on Glasgow Coma Scale in Patients with Moderate and Severe Traumatic Brain Injury: An Approach with Propensity Score-Matched Population. Int. J. Environ. Res. Public Health 2017, 14, 1378. [Google Scholar] [CrossRef]
- Kehoe, A.; Rennie, S.; Smith, J.E. Glasgow Coma Scale is unreliable for the prediction of severe head injury in elderly trauma patients. Emerg. Med. J. 2015, 32, 613–615. [Google Scholar] [CrossRef]
- Basak, D.; Chatterjee, S.; Attergrim, J.; Sharma, M.R.; Soni, K.D.; Verma, S.; GerdinWärnberg, M.; Roy, N. Glasgow coma scale compared to other trauma scores in discriminating in-hospital mortality of traumatic brain injury patients admitted to urban Indian hospitals: A multicentre prospective cohort study. Injury 2023, 54, 93–99. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Mild (n, %) | Moderate (n, %) | Severe (n, %) | Total (n, %) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Sex | Female | 35 | 33.02% | 6 | 66.67% | 1 | 25.00% | 42 | 35.29% |
| Male | 71 | 66.98% | 3 | 33.33% | 3 | 75.00% | 77 | 64.71% | |
| Education | University (13+ years) | 58 | 54.72% | 1 | 11.11% | 0 | 0.00% | 59 | 49.58% |
| High School (9–12 years) | 26 | 24.53% | 2 | 22.22% | 1 | 25.00% | 29 | 24.37% | |
| Unknown | 14 | 13.21% | 3 | 33.33% | 2 | 50.00% | 19 | 15.97% | |
| Secondary School (5–8 years) | 3 | 2.83% | 3 | 33.33% | 0 | 0.00% | 6 | 5.04% | |
| Primary School (1–4 years) | 3 | 2.83% | 0 | 0.00% | 0 | 0.00% | 3 | 2.52% | |
| No Formal Education | 2 | 1.89% | 0 | 0.00% | 1 | 25.00% | 3 | 2.52% | |
| Employment | Employed | 24 | 22.64% | 0 | 0.00% | 2 | 50.00% | 26 | 21.85% |
| Retired | 64 | 60.38% | 7 | 77.78% | 0 | 0.00% | 71 | 59.66% | |
| Unknown | 9 | 8.49% | 1 | 11.11% | 1 | 25.00% | 11 | 9.24% | |
| Other | 2 | 1.89% | 0 | 0.00% | 0 | 0.00% | 2 | 1.68% | |
| Unemployed | 7 | 6.60% | 1 | 11.11% | 1 | 25.00% | 9 | 7.56% | |
| Marital status | Married | 49 | 46.23% | 4 | 44.44% | 1 | 25.00% | 54 | 45.38% |
| Single | 19 | 17.92% | 2 | 22.22% | 1 | 25.00% | 22 | 18.49% | |
| Unknown | 14 | 13.21% | 2 | 22.22% | 2 | 50.00% | 18 | 15.13% | |
| Living Together | 2 | 1.89% | 0 | 0.00% | 0 | 0.00% | 2 | 1.68% | |
| Separated | 3 | 2.83% | 0 | 0.00% | 0 | 0.00% | 3 | 2.52% | |
| Widowed | 19 | 17.92% | 1 | 11.11% | 0 | 0.00% | 20 | 16.81% | |
| Residence | Urban | 75 | 70.75% | 9 | 100.00% | 3 | 75.00% | 87 | 73.11% |
| Rural | 31 | 29.25% | 0 | 0.00% | 1 | 25.00% | 32 | 26.89% | |
| Post-traumatic amnesia | No | 78 | 73.58% | 6 | 66.67% | 2 | 50.00% | 86 | 72.27% |
| Yes | 28 | 26.42% | 3 | 33.33% | 2 | 50.00% | 33 | 27.73% | |
| Place of injury | Home | 69 | 65.09% | 7 | 77.78% | 0 | 0.00% | 76 | 63.87% |
| Work | 1 | 0.94% | 0 | 0.00% | 1 | 25.00% | 2 | 1.68% | |
| Other | 7 | 6.60% | 0 | 0.00% | 0 | 0.00% | 7 | 5.88% | |
| Street | 28 | 26.42% | 2 | 22.22% | 3 | 75.00% | 33 | 27.73% | |
| Sports Facility | 1 | 0.94% | 0 | 0.00% | 0 | 0.00% | 1 | 0.84% | |
| Cause of injury | Fall | 80 | 75.47% | 8 | 88.89% | 3 | 75.00% | 91 | 76.47% |
| Other | 2 | 1.89% | 0 | 0.00% | 0 | 0.00% | 2 | 1.68% | |
| Aggression | 3 | 2.83% | 0 | 0.00% | 0 | 0.00% | 3 | 2.52% | |
| Road Traffic Accident | 21 | 19.81% | 1 | 11.11% | 1 | 25.00% | 23 | 19.33% | |
| Mechanism injury | Fall From Height > 1 m (3ft) | 16 | 15.09% | 2 | 22.22% | 0 | 0.00% | 18 | 15.13% |
| Ground-level Fall | 65 | 61.32% | 5 | 55.56% | 2 | 50.00% | 72 | 60.50% | |
| Other Non-penetrating TBIs | 1 | 0.94% | 0 | 0.00% | 0 | 0.00% | 1 | 0.84% | |
| Direct Impact: Blow To the Head | 4 | 3.77% | 0 | 0.00% | 0 | 0.00% | 4 | 3.36% | |
| Missing Data | 3 | 2.83% | 1 | 11.11% | 0 | 0.00% | 4 | 3.36% | |
| Acceleration/Deceleration | 4 | 3.77% | 1 | 11.11% | 0 | 0.00% | 5 | 4.20% | |
| Crush | 1 | 0.94% | 0 | 0.00% | 1 | 25.00% | 2 | 1.68% | |
| Direct Impact: Head Against an Object | 12 | 11.32% | 0 | 0.00% | 1 | 25.00% | 13 | 10.92% | |
| Type of injury | Closed | 104 | 98.11% | 8 | 88.89% | 2 | 50.00% | 114 | 95.80% |
| Penetrating | 1 | 0.94% | 0 | 0.00% | 1 | 25.00% | 2 | 1.68% | |
| Crush | 1 | 0.94% | 1 | 11.11% | 1 | 25.00% | 3 | 2.52% | |
| Modified Marshall Score | II | 91 | 85.85% | 7 | 77.78% | 2 | 50.00% | 100 | 84.03% |
| III | 7 | 6.60% | 1 | 11.11% | 1 | 25.00% | 9 | 7.56% | |
| I | 7 | 6.60% | 1 | 11.11% | 0 | 0.00% | 8 | 6.72% | |
| IV | 1 | 0.94% | 0 | 0.00% | 0 | 0.00% | 1 | 0.84% | |
| V | 0 | 0.00% | 0 | 0.00% | 1 | 25.00% | 1 | 0.84% | |
| Discharge status | Alive | 100 | 94.34% | 4 | 44.44% | 3 | 75.00% | 107 | 89.92% |
| Dead | 6 | 5.66% | 5 | 55.56% | 1 | 25.00% | 12 | 10.08% | |
| Discharge to | Home | 98 | 92.45% | 4 | 44.44% | 2 | 50.00% | 104 | 87.39% |
| Another Hospital | 1 | 0.94% | 0 | 0.00% | 1 | 25.00% | 2 | 1.68% | |
| Other | 6 | 5.66% | 5 | 55.56% | 1 | 25.00% | 12 | 10.08% | |
| Rehabilitation | 1 | 0.94% | 0 | 0.00% | 0 | 0.00% | 1 | 0.84% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vadan, I.-M.; Grad, D.; Strilciuc, S.; Stefanescu, E.; Verisezan Rosu, O.; Michalak, M.; Blesneag, A.V.; Muresanu, D. Glasgow Coma Scale Score at Admission in Traumatic Brain Injury Patients: A Multicenter Observational Analysis. J. Clin. Med. 2025, 14, 5195. https://doi.org/10.3390/jcm14155195
Vadan I-M, Grad D, Strilciuc S, Stefanescu E, Verisezan Rosu O, Michalak M, Blesneag AV, Muresanu D. Glasgow Coma Scale Score at Admission in Traumatic Brain Injury Patients: A Multicenter Observational Analysis. Journal of Clinical Medicine. 2025; 14(15):5195. https://doi.org/10.3390/jcm14155195
Chicago/Turabian StyleVadan, Iulia-Maria, Diana Grad, Stefan Strilciuc, Emanuel Stefanescu, Olivia Verisezan Rosu, Marcin Michalak, Alina Vasilica Blesneag, and Dafin Muresanu. 2025. "Glasgow Coma Scale Score at Admission in Traumatic Brain Injury Patients: A Multicenter Observational Analysis" Journal of Clinical Medicine 14, no. 15: 5195. https://doi.org/10.3390/jcm14155195
APA StyleVadan, I.-M., Grad, D., Strilciuc, S., Stefanescu, E., Verisezan Rosu, O., Michalak, M., Blesneag, A. V., & Muresanu, D. (2025). Glasgow Coma Scale Score at Admission in Traumatic Brain Injury Patients: A Multicenter Observational Analysis. Journal of Clinical Medicine, 14(15), 5195. https://doi.org/10.3390/jcm14155195