
Gait Analysis After Anterior Cruciate Ligament Surgery Comparing Primary Repair and Reconstruction Techniques


Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Technique
2.3. Gait Analysis Protocol
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sherman, M.F.; Lieber, L.; Bonamo, J.R.; Podesta, L.; Reiter, I. The long-term follow-up of primary anterior cruciate ligament repair. Defining a rationale for augmentation. Am. J. Sports Med. 1991, 19, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Van der List, J.P.; DiFelice, G.S. Preoperative magnetic resonance imaging predict eligibility for arthroscopic primary anterior cruciate ligament repair. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 660–671. [Google Scholar] [CrossRef] [PubMed]
- Nixon, J.E. Acute injuries of the anterior cruciate ligament of the knee: Primary repair. Bull. N. Y. Acad. Med. 1980, 56, 483–487. [Google Scholar] [PubMed]
- Van der List, J.P.; DiFelice, G.S. Primary repair of the anterior cruciate ligament: A paradigm shift. Surgeon 2017, 15, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Van der List, J.P.; Jonkergouw, A.; Van Noort, A.; Kerkhoffs, G.M.M.J.; DiFelice, G.S. Identifying candidates for arthroscopic primary repair of the anterior cruciate ligament: A case-control study. Knee 2019, 26, 619–627. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira Silva, D.; Rathleff, M.S.; Petersen, K.; Azevedo, F.M.D.; Barton, C.J. Manifestations of pain sensitization across different painful knee disorders: A systematic review including meta-analysis and metaregression. Pain Med. 2019, 20, 335–358. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.C.; Luc-Harkey, B.A.; Seeley, M.K.; Troy Blackburn, J.; Pietrosimone, B. Sagittal plane walking biomechanics in individuals with knee osteoarthritis after quadriceps strengthening. Osteoarthr. Cartil. 2019, 27, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Capin, J.J.; Behrns, W.; Thatcher, K.; Arundale, A.; Smith, A.H.; Snyder-Mackler, L. On-ice return-to-hockey progression after anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 2017, 47, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Goetschius, J.; Hertel, J.; Saliba, S.A.; Brockmeier, S.F.; Hart, J.M. Gait biomechanics in anterior cruciate ligament-reconstructed knees at different time frames postsurgery. Med. Sci. Sports Exerc. 2018, 50, 2209–2216. [Google Scholar] [CrossRef] [PubMed]
- Majewska, J.; Szczepanik, M.; Szymczyk, D.; Bazarnik-Mucha, K.; Drużbicki, M.; Snela, S.; Jarmuziewicz, A.; Pyczuła, R. Evaluation of selected gait parameters in patients prior to and at 6 months following early anterior cruciate ligament reconstruction. Ortop. Traumatol. Rehabil. 2017, 19, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Erhart-Hledik, J.C.; Chu, C.R.; Asay, J.L.; Andriacchi, T.P. Longitudinal changes in knee gait mechanics between 2 and 8 years after anterior cruciate ligament reconstruction. J. Orthop. Res. 2018, 36, 1478–1486. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Manal, K.T.; Rudolph, K.S. Knee joint loading during gait in healthy controls and individuals with knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Min, S.; Park, S.H.; Yoo, J.; Jee, Y.A. Influence of isometric exercise combined with electromyostimulation on inflammatory cytokine levels, muscle strength, and knee joint function in elderly women with early knee osteoarthritis. Front. Physiol. 2021, 12, 688260. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Sawacha, Z.; Paolini, G.; Ingrosso, S.; Nativo, R.; Benedetti, M.G. A new anatomically based protocol for gait analysis in children. Gait Posture 2007, 26, 560–571. [Google Scholar] [CrossRef] [PubMed]
- Beard, D.J.; Soundarapandian, R.S.; O’Connor, J.J.; Dodd, C.A.F. Gait and electromyographic analysis of anterior cruciate ligament deficient subjects. Gait Posture 1996, 4, 83–88. [Google Scholar] [CrossRef]
- Bulgheroni, P.; Bulgheroni, M.V.; Andrini, L.; Guffanti, P.; Giughello, A. Gait patterns after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 1997, 5, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Knoll, Z.; Kocsis, L.; Kiss, R.M. Gait patterns before and after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2004, 12, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; McPherson, A.L.; Hewett, T.E.; Feller, J.A. Factors associated with a return to preinjury level of sport performance after anterior cruciate ligament reconstruction surgery. Am. J. Sports Med. 2019, 47, 2557–2562. [Google Scholar] [CrossRef] [PubMed]
- Scanlan, S.F.; Chaudhari, A.M.; Dyrby, C.O.; Andriacchi, T.P. Differences in tibial rotation during walking in ACL reconstructed and healthy contralateral knees. J. Biomech. 2010, 43, 1817–1822. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Stevermer, C.A.; Gillette, J.C. Gait analysis post anterior cruciate ligament reconstruction: Knee osteoarthritis perspective. Gait Posture 2012, 36, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Shabani, B.; Bytyqi, D.; Lustig, S.; Cheze, L.; Bytyqi, C.; Neyret, P. Gait changes of the ACL-deficient knee 3D kinematic assessment. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3259–3265. [Google Scholar] [CrossRef] [PubMed]
- Slater, L.V.; Hart, J.M.; Kelly, A.R.; Kuenze, C.M. Progressive changes in walking kinematics and kinetics after anterior cruciate ligament injury and reconstruction: A review and meta-analysis. J. Athl. Train. 2017, 52, 847–860. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Choi, M.H.; Lee, J.; Han, H.S.; Lee, M.C.; Ro, D.H. Gait deviations of patients with ruptured anterior cruciate ligament: A cross-sectional gait analysis study on male patients. Knee Surg. Relat. Res. 2021, 33, 45. [Google Scholar] [CrossRef] [PubMed]
- Ligia, R.; Mihnea, I.M.; Piele, D. Biomechanic pattern of knees after ACL reconstruction. Gait Posture 2024, 113, 197. [Google Scholar] [CrossRef]
- Scholes, C.; Ektas, N.; Harrison-Brown, M. Persistent knee extension deficits are common after anterior cruciate ligament reconstruction: A systematic review and meta-analysis of randomised controlled trials. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 3172–3185. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Zhou, H.; Jie, T.; Zhou, Z.; Yuan, Y.; Jemni, M.; Quan, W.; Gao, Z.; Xiang, L.; Gusztav, F.; et al. Data-Driven Deep Learning for Predicting Ligament Fatigue Failure Risk Mechanisms. Int. J. Mech. Sci. 2025, 301, 110519. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, G.; Han, B.; Wang, Z.; Yan, Y.; Ma, J.; Wei, P. Knee joint biomechanics in physiological conditions and how pathologies can affect it: A systematic review. Appl. Bionics Biomech. 2020, 2020, 7451683. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Hu, Z.; Zhao, D.; Huang, H.; Liang, Y.; Mao, B. Arthroscopic surgery is not superior to conservative treatment in knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trails. BMC Musculoskelet. Disord. 2024, 25, 712. [Google Scholar] [CrossRef] [PubMed]
- Ektas, N.; Scholes, C.; Kulaga, S.; Kirwan, G.; Lee, B.; Bell, C. Recovery of knee extension and incidence of extension deficits following anterior cruciate ligament injury and treatment: A systematic review protocol. J. Orthop. Surg. Res. 2019, 14, 88. [Google Scholar] [CrossRef] [PubMed]
- Shelbourne, K.D.; Benner, R.; Gray, T.; Bauman, S. Range of motion, strength and function after ACL reconstruction using a contralateral patellar tendon graft. Orthop. J. Sports Med. 2022, 10, 23259671221138103. [Google Scholar] [CrossRef] [PubMed]
- Growney, E.; Meglan, D.; Johnson, M.; Cahalan, T.; An, K.N. Repeated measures of adult normal walking using a video tracking system. Gait Posture 1997, 6, 147–162. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E.; Gainey, J.; Gorton, G.; Cochran, G.V. Repeatability of kinematic, kinetic, and electromyo- graphic data in normal adult gait. J. Orthop. Res. 1989, 7, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Schache, A.G.; Blanch, P.D.; Rath, D.A.; Wrigley, T.V.; Starr, R.; Bennell, K.L. Intra-subject repeatability of the three dimensional angular kinematics within the lumbo-pelvic-hip complex during running. Gait Posture 2002, 15, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, K.; Staes, H.; Bruyninckx, H.; Busschots, E.; Jaspers, E.; Atre, A.; Desloovere, K. Repeatability in the assessment of multi-segment foot kinematics. Gait Posture 2012, 35, 2255–2260. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
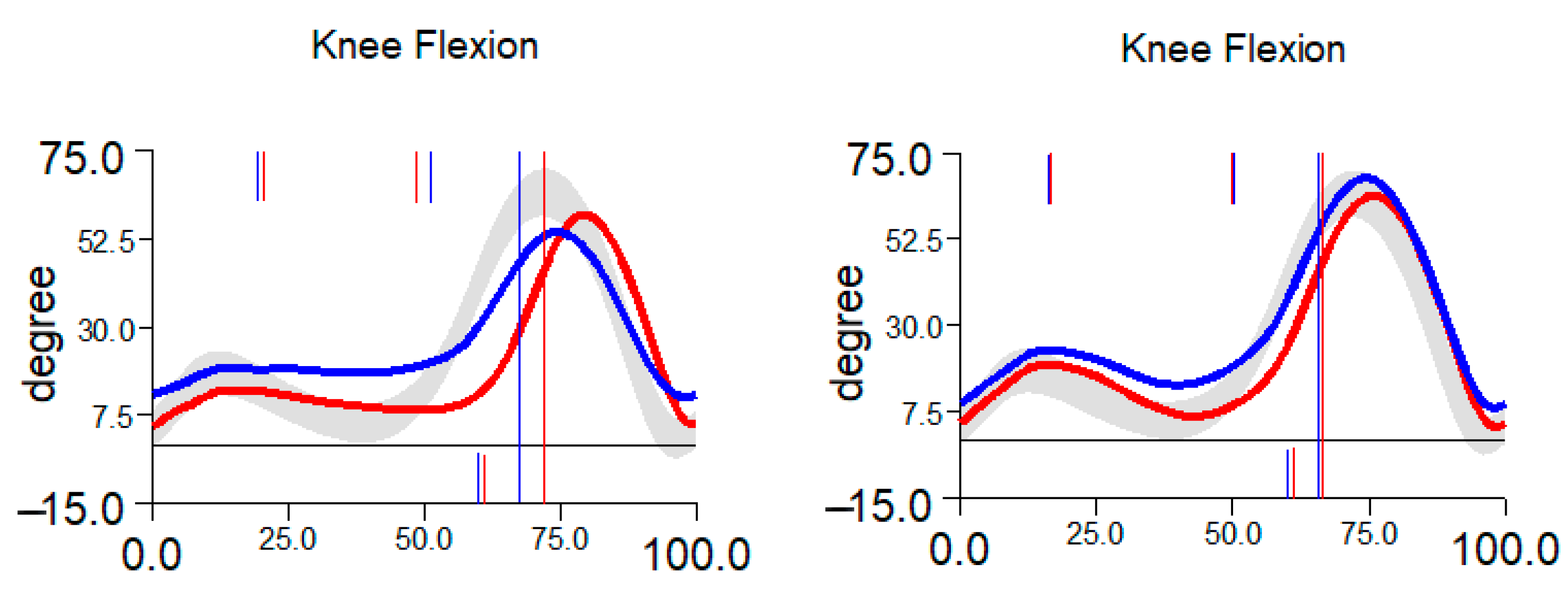
| 6 Weeks | 6 Months | |||
|---|---|---|---|---|
| Flexion [°] | Extension [°] | Flexion [°] | Extension [°] | |
| Brace | 63.3 ± 7.2 | 16.9 ± 5.9 | 64.4 ± 3.9 | 10.6 ± 4.8 |
| Graft | 63.8 ± 5.4 | 18.2 ± 5.4 | 67 ± 2.9 | 15.1 ± 5.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hušek, F.; Vitvar, J.; Mizera, R.; Horák, Z.; Čapek, L. Gait Analysis After Anterior Cruciate Ligament Surgery Comparing Primary Repair and Reconstruction Techniques. J. Clin. Med. 2025, 14, 5026. https://doi.org/10.3390/jcm14145026
Hušek F, Vitvar J, Mizera R, Horák Z, Čapek L. Gait Analysis After Anterior Cruciate Ligament Surgery Comparing Primary Repair and Reconstruction Techniques. Journal of Clinical Medicine. 2025; 14(14):5026. https://doi.org/10.3390/jcm14145026
Chicago/Turabian StyleHušek, Filip, Jiří Vitvar, Roman Mizera, Zdeněk Horák, and Lukáš Čapek. 2025. "Gait Analysis After Anterior Cruciate Ligament Surgery Comparing Primary Repair and Reconstruction Techniques" Journal of Clinical Medicine 14, no. 14: 5026. https://doi.org/10.3390/jcm14145026
APA StyleHušek, F., Vitvar, J., Mizera, R., Horák, Z., & Čapek, L. (2025). Gait Analysis After Anterior Cruciate Ligament Surgery Comparing Primary Repair and Reconstruction Techniques. Journal of Clinical Medicine, 14(14), 5026. https://doi.org/10.3390/jcm14145026