
Effectiveness of Robot-Assisted Gait Training in Stroke Rehabilitation: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection and Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Analysis
3. Result
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Risk of Bias Assessment
3.4. Effects of Combined Robotic and Conventional Gait Rehabilitation
3.4.1. Gait Function
3.4.2. Gait Speed
3.4.3. Gait Balance
3.4.4. Activities of Daily Living (ADLs)
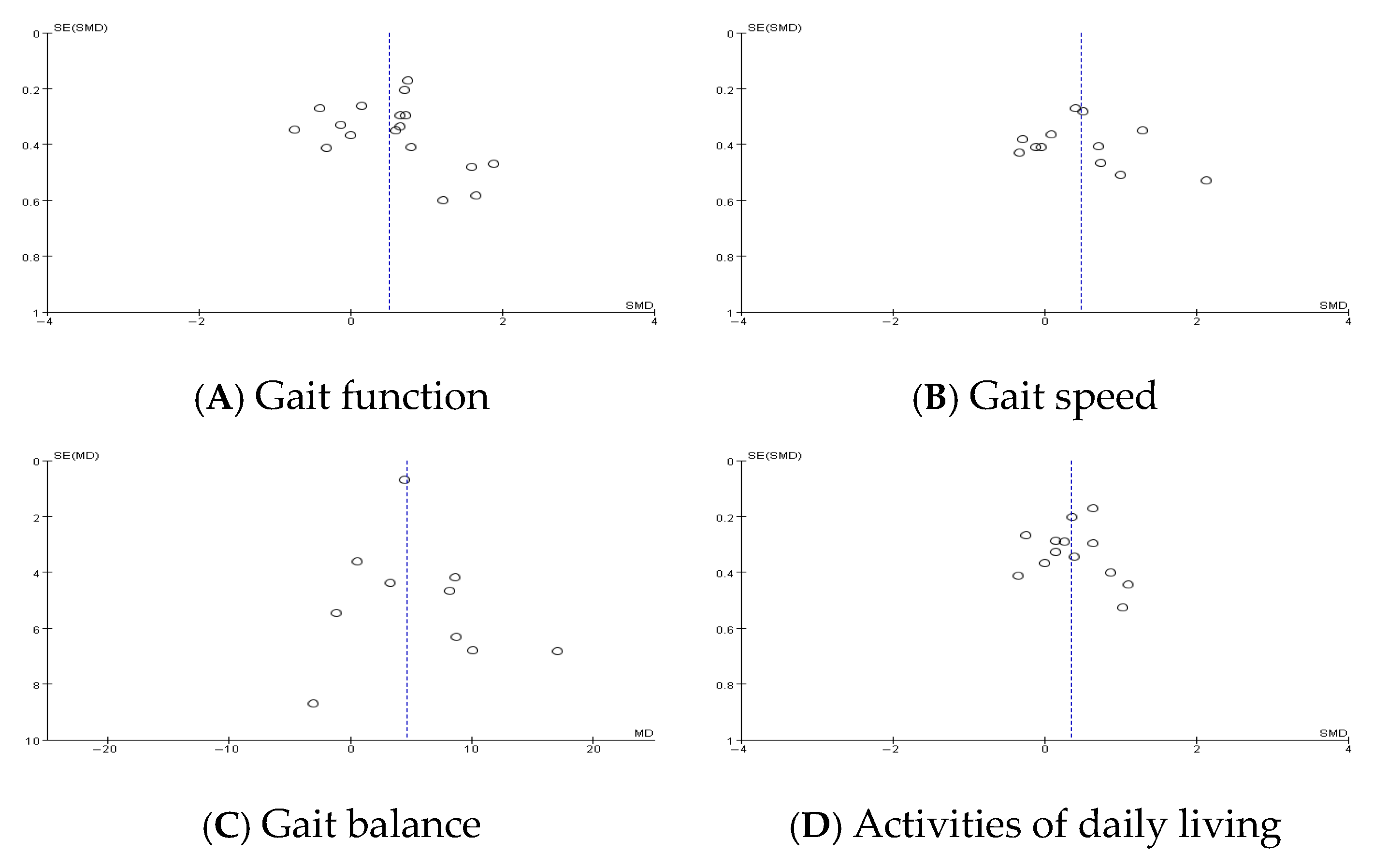
3.4.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, J.; Kim, D.Y.; Lee, S.H.; Kim, J.H.; Kim, D.Y.; Lim, K.B.; Yoo, J. End-effector lower limb robot-assisted gait training effects in subacute stroke patients: A randomized controlled pilot trial. Medicine 2023, 102, e35568. [Google Scholar] [CrossRef] [PubMed]
- Korea Disease Control and Prevention Agency. Trends in stroke incidence in Korea. Korean Statistical Information Service (KOSIS). Available online: https://kosis.kr/statHtml/statHtml.do?orgId=177&tblId=DT_177001_A017&conn_path=I2 (accessed on 19 May 2024).
- Zhao, Y.; Liao, X.; Gu, H.; Jiang, Y.; Wang, Y.; Zhang, Y. Gait speed at the acute phase predicts health-related quality of life at 3 and 12 months after stroke: A prospective cohort study. J. Rehabil. Med. 2024, 56, jrm24102. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.M.; Tan, M.P. Stroke and falls—Clash of the two titans in geriatrics. Geriatrics 2016, 1, 31. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.R.; Galvin, R.; Williams, D.J.P.; Harbison, J.A.; Murphy, S.; Collins, R.; McCabe, D.J.; Crowe, M.; Horgan, N.F. Falls after stroke: Results of the multi-centre prospective FREESE cohort study. Eur. Stroke J. 2018, 3, 58–66. [Google Scholar] [CrossRef]
- Patel, P.; Casamento-Moran, A.; Christou, E.A.; Lodha, N. Force-control vs. strength training: Effects on gait variability in chronic stroke survivors. Front. Neurol. 2021, 12, 667340. [Google Scholar] [CrossRef]
- Nedergård, H.; Arumugam, A.; Sandlund, M.; Bråndal, A.; Häger, C.K. Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2021, 18, 64. [Google Scholar] [CrossRef]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016, 11, CD006073. [Google Scholar] [CrossRef]
- Cramer, S.C.; Sur, M.; Dobkin, B.H.; O’Brien, C.; Sanger, T.D.; Trojanowski, J.Q.; Rumsey, J.M.; Hicks, R.; Cameron, J.; Chen, D.; et al. Harnessing neuroplasticity for clinical applications. Brain 2011, 134, 1591–1609. [Google Scholar] [CrossRef]
- Krakauer, J.W. Motor learning: Its relevance to stroke recovery and neurorehabilitation. Curr. Opin. Neurol. 2006, 19, 84–90. [Google Scholar] [CrossRef]
- Dietz, V.; Sinkjaer, T. Spastic movement disorder: Impaired reflex function and altered muscle mechanics. Lancet Neurol. 2007, 6, 725–733. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, D.Y.; Chun, M.H.; Kim, S.W.; Jeon, H.R.; Hwang, C.H.; Choi, J.K.; Bae, S. Effects of robot-(Morning Walk®) assisted gait training for patients after stroke: A randomized controlled trial. Clin. Rehabil. 2019, 33, 516–523. [Google Scholar] [CrossRef] [PubMed]
- English, C.; Hillier, S.L.; Lynch, E.A. Circuit class therapy for improving mobility after stroke. Cochrane Database Syst. Rev. 2017, 6, CD007513. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10, CD006185. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable taskforce. Neurorehabil. Neural. Repair. 2017, 31, 793–799. [Google Scholar] [CrossRef]
- Pohl, M.; Werner, C.; Holzgraefe, M.; Kroczek, G.; Mehrholz, J.; Wingendorf, I.; Hoölig, G.; Koch, R.; Hesse, S. Repetitive locomotor training and physiotherapy improve walking and basic activities of daily living after stroke: A single-blind, randomized multicentre trial (DEutsche GAngtrainerStudie, DEGAS). Clin. Rehabil. 2007, 21, 17–27. [Google Scholar] [CrossRef]
- Hwang, S.; Song, C.S. Assistive technology involving postural control and gait performance for adults with stroke: A systematic review and meta-analysis. Healthcare 2023, 11, 2225. [Google Scholar] [CrossRef]
- Moucheboeuf, G.; Griffier, R.; Gasq, D.; Glize, B.; Bouyer, L.; Dehail, P.; Cassoudesalle, H. Effects of robotic gait training after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 518–534. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, Version 6.4; Cochrane: London, UK, 2023; Available online: https://training.cochrane.org/handbook (accessed on 10 November 2024).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Review Manager (RevMan) [Computer Program], Version 5.4.1, The Cochrane Collaboration: London, UK, 2020. Available online: https://training.cochrane.org/revman (accessed on 17 October 2024).
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Belas dos Santos, M.; de Oliveira, C.B.; dos Santos, A.; Pires, C.G.; Dylewski, V.; Arida, R.M. A comparative study of conventional physiotherapy versus robot-assisted gait training associated to physiotherapy in individuals with ataxia after stroke. Behav. Neurol. 2018, 2018, 2892065. [Google Scholar] [CrossRef] [PubMed]
- Calabro, R.S.; Naro, A.; Russo, M.; Bramanti, P.; Carioti, L.; Balletta, T.; Buda, A.; Manuli, A.; Filoni, S.; Bramanti, A. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: A randomized clinical trial. J. Neuroeng. Rehabil. 2018, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Kim, M.S.; Huh, J.P.; Lee, P.K.; Kim, Y.H. Effects of robot-assisted gait training on cardiopulmonary fitness in subacute stroke patients: A randomized controlled study. Neurorehabil. Neural. Repair. 2012, 26, 318–324. [Google Scholar] [CrossRef]
- Geroin, C.; Picelli, A.; Munari, D.; Waldner, A.; Tomelleri, C.; Smania, N. Combined transcranial direct current stimulation and robot-assisted gait training in patients with chronic stroke: A preliminary comparison. Clin. Rehabil. 2011, 25, 537–548. [Google Scholar] [CrossRef]
- Han, E.Y.; Im, S.H.; Kim, B.R.; Seo, M.J.; Kim, M.O. Robot-assisted gait training improves brachial-ankle pulse wave velocity and peak aerobic capacity in subacute stroke patients with totally dependent ambulation. Medicine 2016, 95, e5078. [Google Scholar] [CrossRef]
- Husemann, B.; Muller, F.; Krewer, C.; Heller, S.; Koenig, E. Effects of locomotion training with assistance of a robotic-driven gait orthosis in hemiparetic patients after stroke: A randomized controlled pilot study. Stroke 2007, 38, 349–354. [Google Scholar] [CrossRef]
- Kelley, C.P.; Childress, J.; Boake, C.; Noser, E.A. Over-ground and robotic-assisted locomotor training in adults with chronic stroke: A blinded randomized clinical trial. Disabil. Rehabil. Assist. Technol. 2013, 8, 161–168. [Google Scholar] [CrossRef]
- Louie, D.R.; Mortenson, W.B.; Durocher, M.; Schneeberg, A.; Teasell, R.; Yao, J.; Eng, J.J. Efficacy of an exoskeleton-based physical therapy program for non-ambulatory patients during subacute stroke rehabilitation: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 149. [Google Scholar] [CrossRef]
- Morone, G.; Bragoni, M.; Iosa, M.; De Angelis, D.; Venturiero, V.; Coiro, P.; Riso, R.; Pratesi, L.; Paolucci, S. Who may benefit from robotic-assisted gait training? A randomized clinical trial in patients with subacute stroke. Neurorehabil. Neural. Repair. 2011, 25, 636–644. [Google Scholar] [CrossRef]
- Morone, G.; Masiero, S.; Coiro, P.; De Angelis, D.; Venturiero, V.; Paolucci, S.; Iosa, M. Clinical features of patients who might benefit more from walking robotic training. Restor. Neurol. Neurosci. 2018, 36, 293–299. [Google Scholar] [CrossRef]
- Ng, M.F.W.; Tong, R.K.Y.; Li, L.S.W. A pilot study of randomized clinical controlled trial of gait training in subacute stroke patients with partial body-weight support electromechanical gait trainer and functional electrical stimulation. Stroke 2008, 39, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Ochi, M.; Wada, F.; Saeki, S.; Hachisuka, K. Gait training in subacute non-ambulatory stroke patients using a full weight-bearing gait-assistance robot: A prospective, randomized, open, blinded-endpoint trial. J. Neurol. Sci. 2015, 353, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Chung, Y. The effects of robot-assisted gait training using virtual reality and auditory stimulation on balance and gait abilities in persons with stroke. Neurorehabilitation 2018, 43, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Oh-Park, M.; Dohle, C.; Bialek, A.; Friele, K.; Edwards, D.; Krebs, H.I.; You, J.S.H. Effects of innovative hip-knee-ankle interlimb coordinated robot training on ambulation, cardiopulmonary function, depression, and fall confidence in acute hemiplegia. Neurorehabilitation 2020, 46, 577–587. [Google Scholar] [CrossRef]
- Peurala, S.H.; Tarkka, I.M.; Pitkänen, K.; Sivenius, J. The effectiveness of body weight–supported gait training and conventional physical therapy on locomotion in chronic stroke. Arch. Phys. Med. Rehabil. 2005, 86, 1557–1564. [Google Scholar] [CrossRef]
- Taveggia, G.; Borboni, A.; Mulé, C.; Villafañe, J.H.; Negrini, S. Conflicting results of robot-assisted versus usual gait training during postacute rehabilitation of stroke patients: A randomized clinical trial. Int. J. Rehabil. Res. 2016, 39, 29–35. [Google Scholar] [CrossRef]
- Tong, R.K.; Ng, M.F.; Li, L.S. Effectiveness of gait training using an electromechanical gait trainer, with and without functional electric stimulation, in subacute stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2006, 87, 1298–1304. [Google Scholar] [CrossRef]
- Wu, H.; Gu, X.; Fu, J.; Yao, Y.; Li, J.; Xu, Z. Effects of rehabilitation robot for lower-limb on motor function in hemiplegic patients after stroke. Zhonghua Yi Xue Za Zhi 2012, 92, 2628–2631. [Google Scholar] [CrossRef]
- Yoo, H.J.; Bae, C.R.; Jeong, H.; Ko, M.H.; Kang, Y.K.; Pyun, S.B. Clinical efficacy of overground powered exoskeleton for gait training in patients with subacute stroke: A randomized controlled pilot trial. Medicine 2023, 102, e32761. [Google Scholar] [CrossRef]
- Pournajaf, S.; Calabrò, R.S.; Naro, A.; Goffredo, M.; Aprile, I.; Tamburella, F.; Filoni, S.; Waldner, A.; Mazzoleni, S.; Focacci, A.; et al. Robotic versus conventional overground gait training in subacute stroke survivors: A multicenter controlled clinical trial. J. Clin. Med. 2023, 12, 439. [Google Scholar] [CrossRef]
- Donoghue, D.; Stokes, E.K. How much change is true change? The minimum detectable change of the Berg Balance Scale in elderly people. J. Rehabil. Med. 2009, 41, 343–346. [Google Scholar] [CrossRef]
- Batchelor, F.A.; Mackintosh, S.F.; Said, C.M.; Hill, K.D. Falls after stroke. Int. J. Stroke. 2012, 7, 482–490. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Author (Year) [Ref No.] | Experimental Group | Control Group | Outcome Measures | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants (n) (Male/Female) | Type of Stroke | Age (Years) Mean (SD) | Time Since Onset (Days) Mean (SD) (Classification) | Robot Type | Intervention | Participants (n) (Male/Female) | Type of Stroke | Age (Years) Mean (SD) | Time Since Onset (Days) Mean (SD) (Classification) | Intervention | ||
| Belas dos Santos et al. (2018) [24] | 7 (5/2) | I: 2 H: 5 | 44.40 (12.70) | 1752.00 (335.80) (chronic) | Lokomat 5.0 (Hocoma AG, Volketswil, Switzerland) | CT (60 min/day, 2 days/week, 20 weeks) + RAGT (60 min/day, 1 day/week, 20 weeks) | 8 (6/2) | I: 2 H: 6 | 56.40 (11.80) | 3832.50 (1971.00) (chronic) | CT (60 min/day, 2 days/week, 20 weeks) + CT (60 min/day, 1 day/week, 20 weeks) | BBS TUG FIM |
| Calabrò et al. (2018) [25] | 20 (12/8) | NR | 69.00 (4.00) | 300.00 (90.00) (chronic) | Ekso (Ekso Bionics, Richmond, CA, USA) | CT (60 min/day, 5 days/week, 8 weeks) + RAGT (45 min/day, 5 days/week, 8 weeks) | 20 (11/9) | NR | 67.00 (6.00) | 330.00 (90.00) (chronic) | CT (60 min/day, 5 days/week, 8 weeks) + CT (45 min/day, 5 days/week, 8 weeks) | 10 MWT RMI TUG |
| Chang et al. (2012) [26] | 20 (13/7) | I: 12 H: 8 | 55.50 (12.00) | 16.10 (4.90) (subacute) | Lokomat (Hocoma AG, Volketswil, Switzerland) | CT (60 min/day, 5 days/week, 2 weeks) + RAGT (40 min/day 5 days/week, 2 weeks) | 17 (10/7) | I: 11 H: 6 | 59.70 (12.10) | 18.20 (5.00) (subacute) | CT (60 min/day, 5 days/week, 2 weeks) + CT (40 min/day, 5 days/week, 2 weeks) | FMA-LE FAC |
| Geroin et al. (2011) [27] | 10 (6/4) | NR | 63.30 (6.40) | 801.00 (153.00) (chronic) | Gait Trainer (GT1 Reha-Stim, Berlin, Germany) | CT (30 min/day, 5 days/week, 2 weeks) + RAGT (20 min/day 5 days/week, 2 weeks) | 10 (9/1) | NR | 61.10 (6.30) | 807.00 (174.00) (chronic) | CT (30 min/day, 5 days/week, 2 weeks) + CT (20 min/day, 5 days/week, 2 weeks) | 6 MWT 10 MWT FAC RMI MI |
| Han et al. (2016) [28] | 30 (17/13) | I: 17 H: 3 | 67.89 (14.96) | 21.56 (7.98) (subacute) | Lokomat (Hocoma AG, Volketswil, Zürich, Switzerland) | CT (30 min/day, 5 days/week, 4 weeks) + RAGT (30 min/day, 5 days/week, 4 weeks) | 26 (15/11) | I: 16 H: 10 | 63.20 (10.62) | 18.10 (9.78) (subacute) | CT (30 min/day, 5 days/week, 4 weeks) + CT (30 min/day, 5 days/week, 4 weeks) | K-MBI BBS FAC FMA-L |
| Husemann et al. (2007) [29] | 16 (11/5) | I: 12 H: 4 | 60.00 (13.00) | 79.00 (56.00) (subacute) | Lokomat (Hocoma AG, Volketswil, Zürich, Switzerland) | CT (30 min/day, 5 days/week, 4 weeks) + RAGT (30 min/day, 5 days/week, 4 weeks) | 14 (10/4) | I: 10 H: 4 | 57.00 (11.00) | 89.00 (61.00) (subacute) | CT (30 min/day, 5 days/week, 4 weeks) + CT (30 min/day, 5 days/week, 4 weeks) | FAC BI |
| Kelley et al. (2013) [30] | 11 (7/4) | NR | 66.91 (8.50) | 1354.15 (chronic) | Lokomat (Hocoma AG, Volketswil, Zürich, Switzerland) | CT (30 min/day, 5 days/week, 8 weeks) + RAGT (35–40 min/day, 5 days/week, 8 weeks) | 9 (6/3) | NR | 64.33 (10.91) | 525.6 (chronic) | CT (30 min/day, 5 days/week, 8 weeks) + CT (35–40 min/day, 5 days/week, 8 weeks) | 10 MWT 6 MWT FMA-LE BI |
| Kim et al. (2019) [12] | 25 (20/5) | I: 14 H: 11 | 57.70 (12.90) | 60.00 (72.00) (subacute) | Morning Walk (CUREXO, Seoul, Republic of Korea) | CT (60 min/day, 5 days/week, 3 weeks) + RAGT (30 min/day 5 days/week, 3 weeks) | 23 (13/10) | I: 18 H: 5 | 60.40 (13.20) | 78.00 (93.00) (subacute) | CT (60 min/day, 5 days/week, 3 weeks) + CT (30 min/day 5 days/week, 3 weeks) | FAC 10 MWT MBI RMI BBS |
| Lee et al. (2023) [1] | 26 (15/11) | I: 20 H: 6 | 63.04 (15.69) | 27.90 (20.70) (subacute) | Morning Walk (CUREXO, Seoul, Republic of Korea) | CT (90 min/day, 5 days/week, 4 weeks) + RAGT (30 min/day 5 days/week, 4 weeks) | 23 (11/12) | I: 20 H: 3 | 64.78 (12.81) | 27.30 (21.30) (subacute) | CT (90 min/day, 5 days/week, 4 weeks) + CT (30 min/day, 5 days/week, 4 weeks) | FAC RMI 10 MWT BBS MBI |
| Louie et al. (2021) [31] | 19 (16/3) | I: 12 H: 7 | 59.60 (15.80) | 36.70 (19.0) (subacute) | EksoGT (Ekso Bionics, Richmond, CA, USA) | CT (25%) (45–60 min/day, 1–2 days/week, 8 weeks +RAGT(75%) (60 min/day, 3 days/week, 8 weeks) | 17 (10/7) | I: 13 H: 4 | 55.30 (10.60) | 40.90 (19.80) (subacute) | CT (100%) (45–60 min/day, 4–5 days/week, 8 weeks) | FAC 6 MWT FMA-LE BBS |
| Morone et al. (2011) HM [32] | 12 (8/4) | I: 9 H: 3 | 68.33 (9.11) | 21.92 (10.72) (subacute) | Gait Trainer (GT Reha-Stim, Berlin, Germany) | CT (140 min/day, 5 days/week, 4 weeks) + RAGT (20 min/day, 5 days/week, 4 weeks) | 12 (7/5) | I: 12 H: 0 | 62.92 (17.43) | 20.00 (16.58) (subacute) | CT (140 min/day, 5 days/week, 4 weeks) + CT (20 min/day, 5 days/week, 4 weeks) | FAC MI BI 10 MWT |
| Morone et al. (2011) LM [32] | 12 (7/5) | I: 9 H: 3 | 55.58 (13.35) | 16.25 (11.33) (subacute) | Gait Trainer (GT Reha-Stim, Berlin, Germany) | CT (140 min/day, 5 days/week, 4 weeks) + RAGT (20 min/day 5 days/week, 4 weeks) | 12 (6/6) | I: 11 H: 1 | 60.17 (9.59) | 20.00 (12.76) (subacute) | CT (140 min/day, 5 days/week, 4 weeks) + CT (20 min/day, 5 days/week, 4 weeks) | FAC MI BI 10 MWT |
| Morone et al. (2018) [33] | 50 (35/15) | I: 38 H: 12 | 61.90 (11.94) | 19.30 (14.30) (subacute) | Gait Trainer (GT Reha-Stim, Berlin, Germany) | CT (180 min/day, 5 days/week, 2 weeks) + RAGT (40 min/day 5 days/week, 2 weeks) | 50 (31/19) | I: 43 H: 7 | 63.48 (12.93) | 16.50 (11.20) (subacute) | CT (180 min/day, 5 days/week, 2 weeks) + CT (40 min/day 5 days/week, 2 weeks) | FAC BI |
| Ng et al. (2007) [34] | 17 (11/6) | I: 13 H: 4 | 66.60 (11.30) | 18.90 (8.40) (subacute) | Gait Trainer (GT Reha-Stim, Berlin, Germany) | CT (100 min/day 5 days/week, 4 weeks) + RAGT (20 min/day 5 days/week, 4 weeks) | 21 (13/8) | I: 18 H: 3 | 73.4 (11.50) | 17.50 (8.40) (subacute) | CT (100 min/day 5 days/week, 4 weeks) + CT (20 min/day 5 days/week, 4 weeks) | MI BBS FAC BI FIM |
| Ochi et al. (2015) [35] | 13 (11/2) | I: 5 H: 8 | 61.80 (7.50) | 22.9 (7.40) (subacute) | Gait-Assistance Robot (GAR) | CT (60 min/day, 5 days/week, 4 weeks) + RAGT (20 min/day 5 days/week, 4 weeks) | 13 (9/4) | I: 5 H: 8 | 65.50 (12.10) | 26.10 (8.00) (subacute) | CT (60 min/day, 5 days/week, 4 weeks) + CT (20 min/day, 5 days/week, 4 weeks) | FMA FAC 10 MWT FIM |
| Park et al. (2018) [36] | 12 (7/5) | I: 9 H: 3 | 55.58 (10.42) | 219.90 (33.00) (chronic) | Lokomat Pro (Hocoma AG, Zurich, Switzerland) | CT (30 min/day, 5 days/week, 6 weeks) + RAGT (45 min/day, 3 days/week, 6 weeks) | 16 (9/7) | I: 7 H: 9 | 57.50 (9.90) | 232.50 (53.10) (chronic) | CT (30 min/day, 5 days/week, 6 weeks) + CT (45 min/day 3 days/week, 6 weeks) | BBS TUG 10 MWT FMA MBI |
| Park et al. (2020) [37] | 7 (-/-) | I: 7 H: 2 | 76.29 | <14.00 (subacute) | Walkbot locomotor training, (P&S Mechanics, Seoul, Republic of Korea) | CT (60 min/day, 7 days/week, 2 weeks) + RAGT (30 min/day, 7 days/week, 2 weeks) | 7 (4/3) | I: 7 H: 0 | 69.86 | <14.00 (subacute) | CT (60 min/day, 7 days/week, 2 weeks) + CT (30 min/day, 7 days/week, 2 weeks) | BBS FAC |
| Peurala et al. (2005) [38] | 15 (13/2) | I: 7 H: 8 | 51.20 (7.90) | 876.00 (949.00) (chronic) | Gait Trainer (GT1 Reha-Stim, Berlin, Germany) | CT (55 min/day, 5 days/week, 3 weeks) + RAGT (20 min/day 5 days/week, 3 weeks) | 15 (11/4) | I: 8 H: 7 | 52.30 (6.80) | 1460.00 (2117.00) (chronic) | CT (55 min/day, 5 days/week, 3 weeks) + CT (20 min/day 5 days/week, 3 weeks) | 10 MWT 6 MWT FIM |
| Pohl et al. (2007) [16] | 77 (50/27) | I: 61 H: 16 | 62.30 (12.00) | 29.40 (12.60) (subacute) | Electromechanical Gait Trainer (Reha-Stim, Berlin, Germany) | CT (20 min/day 5 days/week, 4 weeks) + RAGT (25 min/day 5 days/week, 4 weeks) | 78 (54/24) | I: 63 H: 15 | 64.00 (11.60) | 31.50 (13.30) (subacute) | CT (20 min/day 5 days/week, 4 weeks) + CT (25 min/day 5 days/week, 4 weeks) | FAC BI RMI MI |
| Taveggia et al. (2016) [39] | 13 (7/6) | NR | 71.00 (5.00) | 60.10 (49.50) (subacute) | Lokomat (Hocoma AG, Zurich, Switzerland) | CT (60 min/day 5 days/week, 5 weeks) + RAGT (30 min/day 5 days/week, 5 weeks) | 15 (10/5) | NR | 73.00 (7.00) | 39.40 (31.70) (subacute) | CT (60 min/day 5 days/week, 5 weeks) + CT (30 min/day 5 days/week, 5 weeks) | 6 MWT 10 MWT FIM |
| Tong et al. (2006) [40] | 15 (9/6) | I: 11 H: 4 | 66.10 (9.90) | 18.90 (9.10) (subacute) | Gait Trainer (GT II Reha-Stim, Berlin, Germany) | CT (40 min/day 5 days/week, 4 weeks) + RAGT (20 min/day 5 days/week, 4 weeks) | 20 (12/8) | I: 17 H: 3 | 71.40 (14.00) | 18.90 (8.40) (subacute) | CT (40 min/day 5 days/week, 4 weeks) + CT (20 min/day 5 days/week, 4 weeks) | MI BBS FAC BI FIM |
| Wu et al. (2012) [41] | 24 (15/9) | I: 9 H: 15 | 50.00 (12.00) | 27.00 (7.00) (subacute) | AVATAR-02 (Shanghai Zhanghua Technology Development Company, Shanghai, China) | CT (45 min/day 6 days/week, 8 weeks) + RAGT (10∼20 min/day 6 days/week, 8 weeks) | 24 (16/8) | I: 11 H: 13 | 49.00 (10.00) | 26.00 (8.00) (subacute) | CT (45 min/day 6 days/week, 8 weeks) + CT (10∼20 min/day 6 days/week, 8 weeks) | FMA FAC MBI |
| Yoo et al. (2023) [42] | 9 (4/5) | I: 7 H: 2 | 61.00 | 19.00 (subacute) | ExoAtlet Medy (ExoAtlet Asia Co., Ltd., Seoul, Republic of Korea) | CT (90 min/day 5 days/week, 4 weeks) + RAGT (30 min/day 3 days/week, 4 weeks) | 8 (5/3) | I: 5 H: 3 | 65.00 | 43.00 (subacute) | CT (90 min/day 5 days/week, 4 weeks) + CT (30 min/day 3 days/week, 4 weeks) | FAC FMA-LE BBS TUG 10 MWT K-MBI |
| Outcome | Overall Effect Size (95% CI) | Subgroup 1 | Subgroup 2 | I2 (%) |
|---|---|---|---|---|
| Gait Function | SMD = 0.51 (0.21–0.81) | End-effector: 0.53 | Exoskeleton: 0.55 | 73 |
| Gait Speed | SMD = 0.47 (0.12–0.83) | Subacute: 0.31 | Chronic: 0.76 | 62 |
| Balance | MD = 4.58 (3.03–6.13) | – | – | 2 |
| ADLs | SMD = 0.35 (0.14–0.56) | ≤15 sessions: High | >15 sessions: Moderate | 39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Kim, G. Effectiveness of Robot-Assisted Gait Training in Stroke Rehabilitation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2025, 14, 4809. https://doi.org/10.3390/jcm14134809
Lee JH, Kim G. Effectiveness of Robot-Assisted Gait Training in Stroke Rehabilitation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2025; 14(13):4809. https://doi.org/10.3390/jcm14134809
Chicago/Turabian StyleLee, Jun Hyeok, and Gaeun Kim. 2025. "Effectiveness of Robot-Assisted Gait Training in Stroke Rehabilitation: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 14, no. 13: 4809. https://doi.org/10.3390/jcm14134809
APA StyleLee, J. H., & Kim, G. (2025). Effectiveness of Robot-Assisted Gait Training in Stroke Rehabilitation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 14(13), 4809. https://doi.org/10.3390/jcm14134809