
Hepatitis C—Everything a Primary Care Physician Needs to Know About Diagnosis, Management, and Follow-Up †
 , , and
, , and
Abstract
1. Introduction
2. Role of Primary Care Physicians
3. Objective
4. Prevalence of HCV Worldwide
5. Prevalence and Mortality of HCV in the United States (US)
6. HCV Routes of Transmission
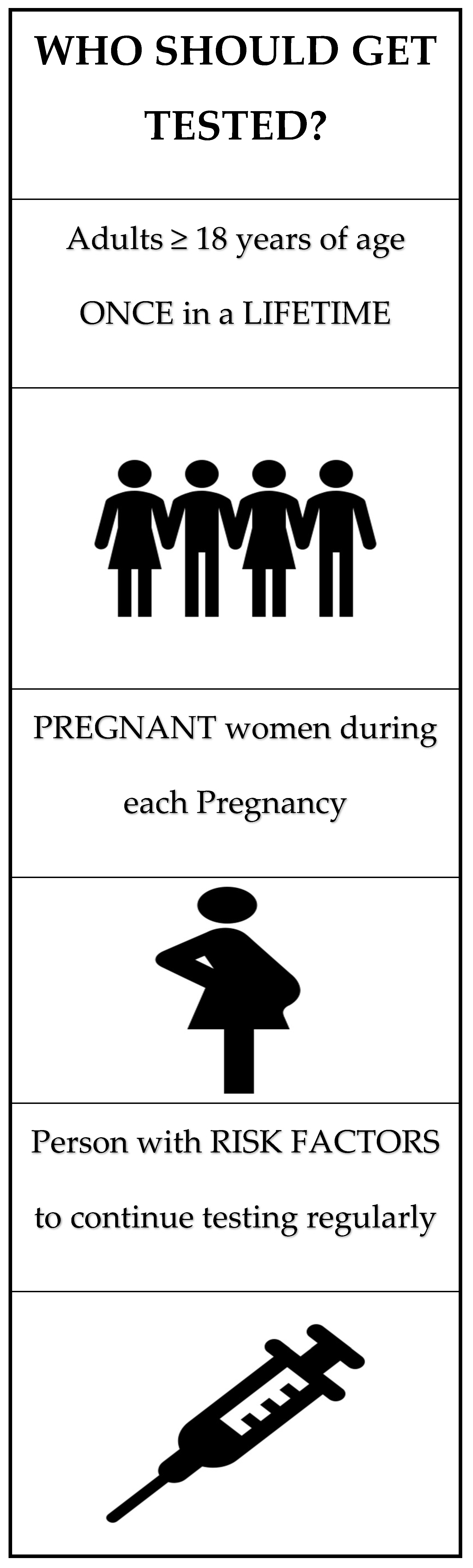
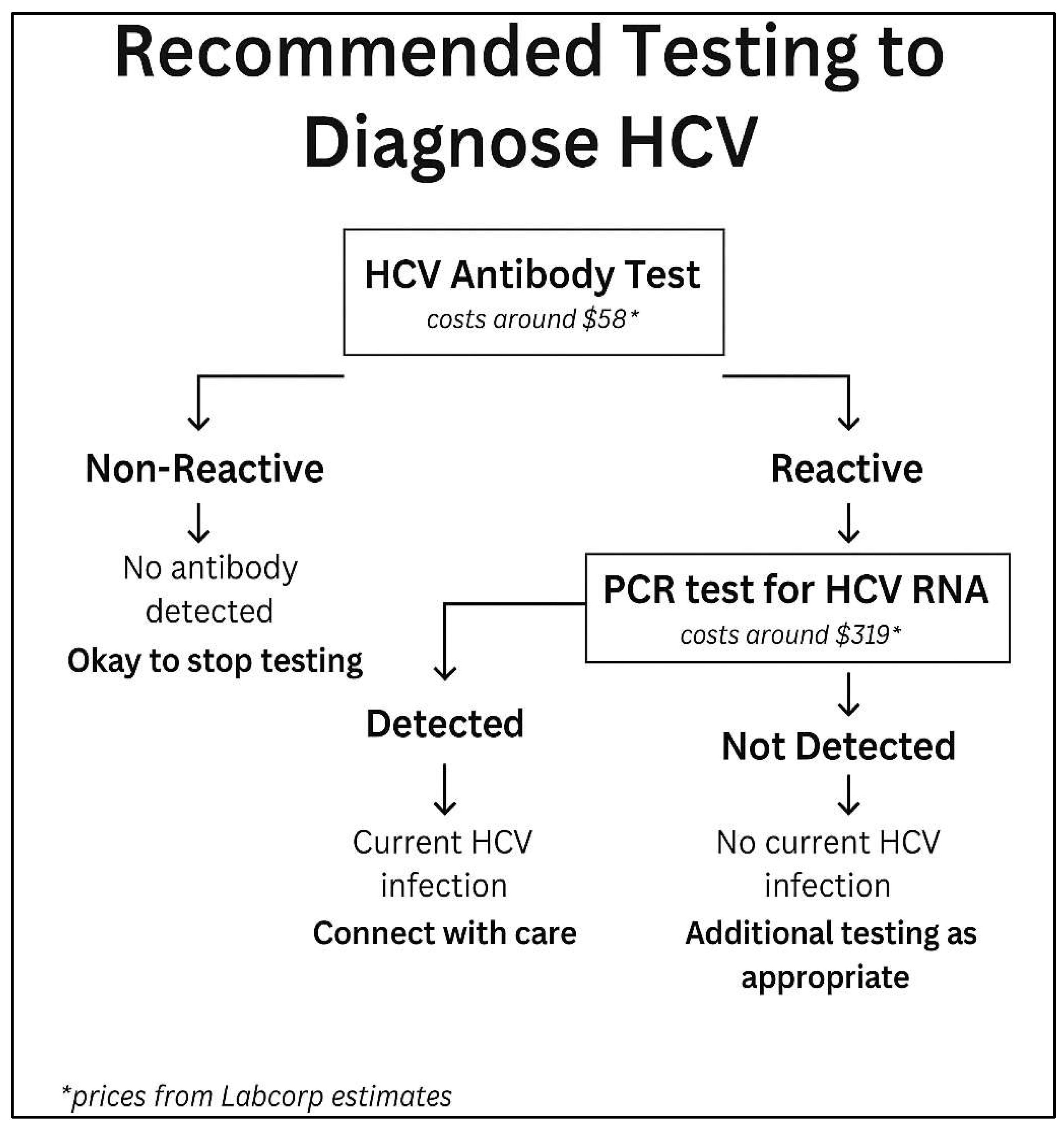
7. Diagnosis and Screening for HCV
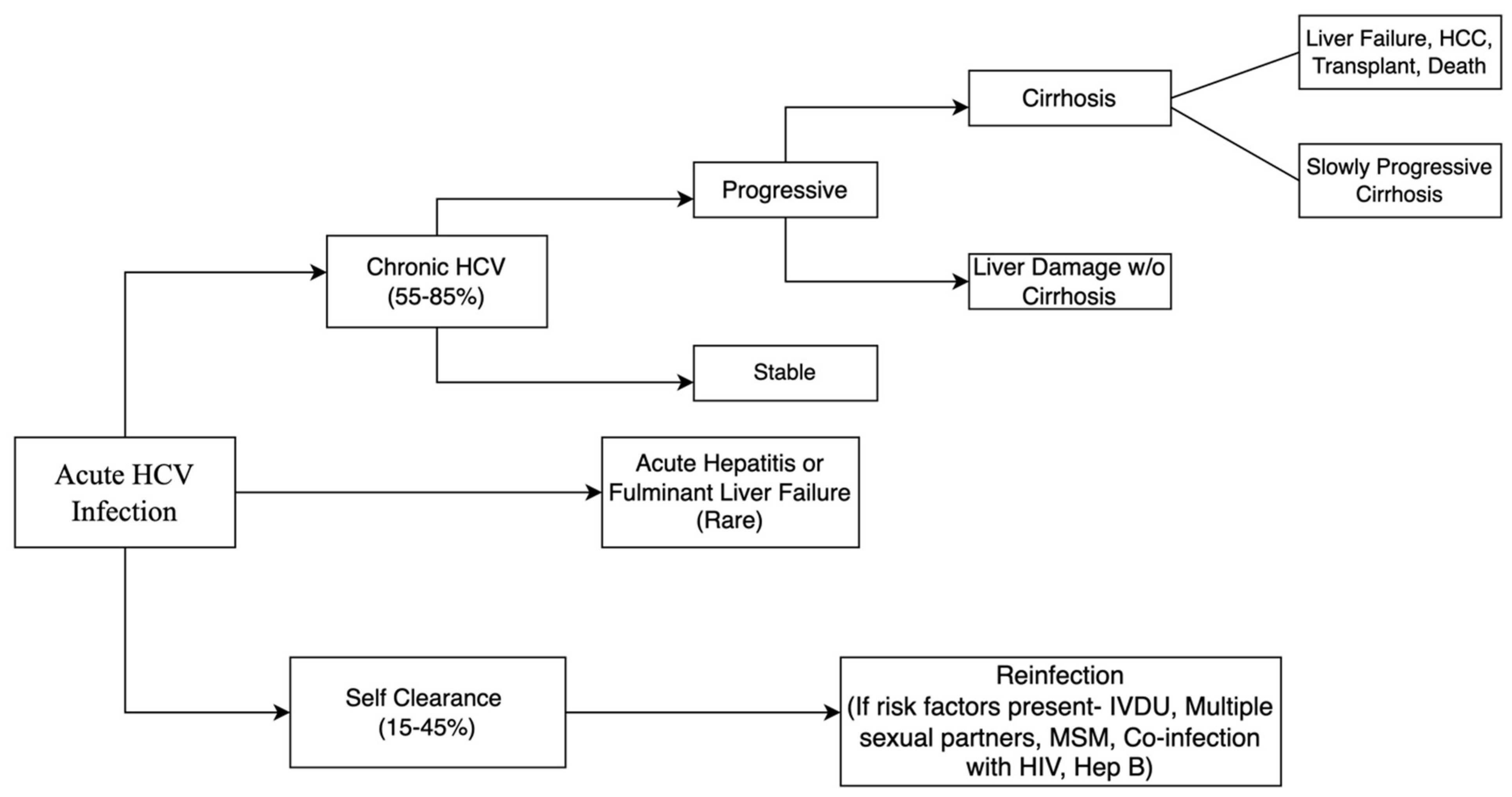
8. Natural History of Infection
9. Complications of HCV Infection
9.1. Hepatic
9.2. Extrahepatic
10. History of HCV Treatment
11. Considerations for Primary Care Physicians Before Initiating HCV Treatment
12. Current HCV Treatment Guidelines
13. Cost of Hepatitis C and Its Treatment
14. Summary of Steps PCPs Should Take in HCV Detection and Treatment
15. Follow-Up for Patients with Cirrhosis
16. Follow-Up for Patients Without Cirrhosis
17. Treatment Failure
18. HCV Treatment in Special Populations
19. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tsoulfas, G.; Goulis, I.; Giakoustidis, D.; Akriviadis, E.; Agorastou, P.; Imvrios, G.; Papanikolaou, V. Hepatitis C and liver transplantation. Hippokratia 2009, 13, 211–215. [Google Scholar] [PubMed]
- Cunningham, E.B.; Applegate, T.L.; Lloyd, A.R.; Dore, G.J.; Grebely, J. Mixed HCV infection and reinfection in people who inject drugs—impact on therapy. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 218–230. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Rosenthal, E.M.; Hall, E.W.; Barker, L.; Hofmeister, M.G.; Sullivan, P.S.; Dietz, P.; Mermin, J.; Ryerson, A.B. Prevalence of Hepatitis C Virus Infection in US States and the District of Columbia, 2013 to 2016. JAMA Netw. Open 2018, 1, e186371. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.C.; Barker, L.K.; Jiles, R.B.; Gupta, N. Estimated Prevalence and Awareness of Hepatitis C Virus Infection Among US Adults: National Health and Nutrition Examination Survey, January 2017–March 2020. Clin. Infect. Dis. 2023, 77, 1413–1415. [Google Scholar] [CrossRef]
- Cox, A.L.; El-Sayed, M.H.; Kao, J.H.; Lazarus, J.V.; Lemoine, M.; Lok, A.S.; Zoulim, F. Progress towards elimination goals for viral hepatitis. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 533–542. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for the Care and Treatment of Persons Diagnosed with Chronic Hepatitis C Virus Infection. Available online: https://iris.who.int/bitstream/handle/10665/273174/9789241550345-eng.pdf?sequence=1 (accessed on 22 December 2023).
- Saito, T.; Ueno, Y. Transmission of hepatitis C virus: Self-limiting hepatitis or chronic hepatitis? World J. Gastroenterol. 2013, 19, 6957–6961. [Google Scholar] [CrossRef]
- Brunner, N.; Bruggmann, P. Trends of the Global Hepatitis C Disease Burden: Strategies to Achieve Elimination. J. Prev. Med. Public Health 2021, 54, 251–258. [Google Scholar] [CrossRef]
- Bartenschlager, R.; Frese, M.; Pietschmann, T. Novel insights into hepatitis C virus replication and persistence. Adv. Virus Res. 2004, 63, 71–180. [Google Scholar] [CrossRef]
- Lindenbach, B.D.; Rice, C.M. Unravelling hepatitis C virus replication from genome to function. Nature 2005, 436, 933–938. [Google Scholar] [CrossRef]
- Kiser, J.J.; Flexner, C. Direct-acting antiviral agents for hepatitis C virus infection. Annu. Rev. Pharmacol. Toxicol. 2013, 53, 427–449. [Google Scholar] [CrossRef]
- Martinello, M.; Naggie, S.; Rockstroh, J.K.; Matthews, G.V. Direct-Acting Antiviral Therapy for Treatment of Acute and Recent Hepatitis C Virus Infection: A Narrative Review. Clin. Infect. Dis. 2023, 77 (Suppl. S3), S238–S244. [Google Scholar] [CrossRef] [PubMed]
- Aghemo, A.; Piroth, L.; Bhagani, S. What do clinicians need to watch for with direct-acting antiviral therapy? J. Int. AIDS Soc. 2018, 21 (Suppl. S2), e25076. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, T.; Horváth, I.; Fenz, L.; Schmutterer, I.; Rosian-Schikuta, I.; Mårdh, O. Interventions to increase linkage to care and adherence to treatment for hepatitis C among people who inject drugs: A systematic review and practical considerations from an expert panel consultation. Int. J. Drug Policy 2022, 102, 103588. [Google Scholar] [CrossRef]
- Spaulding, A.C.; Weinbaum, C.M.; Lau, D.T.; Sterling, R.; Seeff, L.B.; Margolis, H.S.; Hoofnagle, J.H. A framework for management of hepatitis C in prisons. Ann. Intern. Med. 2006, 144, 762–769. [Google Scholar] [CrossRef]
- Facente, S.N.; Burk, K.; Eagen, K.; Mara, E.S.; Smith, A.A.; Lynch, C.S. New Treatments Have Changed the Game: Hepatitis C Treatment in Primary Care. Infect. Dis. Clin. N. Am. 2018, 32, 313–322. [Google Scholar] [CrossRef]
- Rattay, T.; Dumont, I.P.; Heinzow, H.S.; Hutton, D.W. Cost-Effectiveness of Access Expansion to Treatment of Hepatitis C Virus Infection Through Primary Care Providers. Gastroenterology 2017, 153, 1531–1543.e2. [Google Scholar] [CrossRef]
- Simoncini, G.M.; Koren, D.E. Hepatitis C Update and Expanding the Role of Primary Care. J. Am. Board Fam. Med. 2019, 32, 428–430. [Google Scholar] [CrossRef]
- Lohia, P.; Kapur, S.; Crane, L. A Comprehensive Hepatitis C Treatment Program—An Observational Study of Collaboration Between Infectious Disease Specialists and General Internal Medicine Provider Serving a Majority Black Population. Infect. Dis. Clin. Pract. 2022, 30, e1165. [Google Scholar] [CrossRef]
- Guss, D.; Sherigar, J.; Rosen, P.; Mohanty, S.R. Diagnosis and Management of Hepatitis C Infection in Primary Care Settings. J. Gen. Intern. Med. 2018, 33, 551–557. [Google Scholar] [CrossRef]
- Oru, E.; Trickey, A.; Shirali, R.; Kanters, S.; Easterbrook, P. Decentralisation, integration, and task-shifting in hepatitis C virus infection testing and treatment: A global systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e431–e445. [Google Scholar] [CrossRef]
- Kattakuzhy, S.; Gross, C.; Emmanuel, B.; Teferi, G.; Jenkins, V.; Silk, R.; Akoth, E.; Thomas, A.; Ahmed, C.; Espinosa, M.; et al. Expansion of Treatment for Hepatitis C Virus Infection by Task Shifting to Community-Based Nonspecialist Providers: A Nonrandomized Clinical Trial. Ann. Intern. Med. 2017, 167, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Majagi, A.; Almujarkesh, M.K.; Carter, K.S.; Picardal, A.; Kapur, S.; Levine, D.L.; Lohia, P. June. A.B. Hepatitis c: Everything a primary care physician needs to know about hepatitis c from diagnosis to long term follow up. J. Gen. Intern. Med. 2024, 39, S609–S610. [Google Scholar]
- World Health Organization. Hepatitis C. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 21 November 2023).
- Petruzziello, A.; Marigliano, S.; Loquercio, G.; Cozzolino, A.; Cacciapuoti, C. Global epidemiology of hepatitis C virus infection: An up-date of the distribution and circulation of hepatitis C virus genotypes. World J. Gastroenterol. 2016, 22, 7824–7840. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Reduce Reported Rate of Hepatitis C-Related Deaths by 20% or More. 2022. Available online: https://www.cdc.gov/hepatitis/policy/npr/2022/reduce-reported-hepatitis-c-deaths.htm (accessed on 29 November 2023).
- Hall, E.W.; Schillie, S.; Vaughan, A.S.; Jones, J.; Bradley, H.; Lopman, B.; Rosenberg, E.S.; Sullivan, P.S. County-Level Variation in Hepatitis C Virus Mortality and Trends in the United States, 2005–2017. Hepatology 2021, 74, 582–590. [Google Scholar] [CrossRef]
- Grebely, J.; Prins, M.; Hellard, M.; Cox, A.L.; Osburn, W.O.; Lauer, G.; Page, K.; Lloyd, A.R.; Dore, G.J. Hepatitis C virus clearance, reinfection, and persistence, with insights from studies of injecting drug users: Towards a vaccine. Lancet. Infect. Dis. 2012, 12, 408–414. [Google Scholar] [CrossRef]
- Chandra, N.; Joshi, N.; Raju, Y.S.; Kumar, A.; Teja, V.D. Hepatitis B and/or C co-infection in HIV infected patients: A study in a tertiary care centre from South India. Indian J. Med. Res. 2013, 138, 950–954. [Google Scholar] [PubMed]
- Schillie, S.; Wester, C.; Osborne, M.; Wesolowski, L.; Ryerson, A.B. CDC Recommendations for Hepatitis C Screening Among Adults—United States, 2020. MMWR Recomm. Rep. 2020, 69, 1–17. [Google Scholar] [CrossRef]
- Cox, A.L.; Netski, D.M.; Mosbruger, T.; Sherman, S.G.; Strathdee, S.; Ompad, D.; Vlahov, D.; Chien, D.; Shyamala, V.; Ray, S.C.; et al. Prospective evaluation of community-acquired acute-phase hepatitis C virus infection. Clin. Infect. Dis. 2005, 40, 951–958. [Google Scholar] [CrossRef]
- Poynard, T.; Bedossa, P.; Opolon, P. Natural history of liver fibrosis progression in patients with chronic hepatitis C. The OBSVIRC, METAVIR, CLINIVIR, and DOSVIRC groups. Lancet 1997, 349, 825–832. [Google Scholar] [CrossRef]
- Thomson, E.C.; Nastouli, E.; Main, J.; Karayiannis, P.; Eliahoo, J.; Muir, D.; McClure, M.O. Delayed anti-HCV antibody response in HIV-positive men acutely infected with HCV. AIDS 2009, 23, 89–93. [Google Scholar] [CrossRef]
- Vanhommerig, J.W.; Thomas, X.V.; van der Meer, J.T.M.; Geskus, R.B.; Bruisten, S.M.; Molenkamp, R.; Prins, M.; Schinkel, J. Hepatitis C virus (HCV) antibody dynamics following acute HCV infection and reinfection among HIV-infected men who have sex with men. Clin. Infect. Dis. 2014, 59, 1678–1685. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Clinical Screening and Diagnosis for Hepatitis C. 2023. Available online: https://www.cdc.gov/hepatitis-c/hcp/diagnosis-testing/index.html (accessed on 1 December 2023).
- Gupta, E.; Bajpai, M.; Choudhary, A. Hepatitis C virus: Screening, diagnosis, and interpretation of laboratory assays. Asian J. Transfus. Sci. 2014, 8, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Lingala, S.; Ghany, M.G. Natural History of Hepatitis C. Gastroenterol. Clin. N. Am. 2015, 44, 717–734. [Google Scholar] [CrossRef] [PubMed]
- Thein, H.H.; Yi, Q.; Dore, G.J.; Krahn, M.D. Estimation of stage-specific fibrosis progression rates in chronic hepatitis C virus infection: A meta-analysis and meta-regression. Hepatology 2008, 48, 418–431. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M. Natural history of HCV infection. Hepatol. Int. 2012, 6, 684–695. [Google Scholar] [CrossRef]
- Everhart, J.E.; Wright, E.C.; Goodman, Z.D.; Dienstag, J.L.; Hoefs, J.C.; Kleiner, D.E.; Ghany, M.G.; Mills, A.S.; Nash, S.R.; Govindarajan, S.; et al. Prognostic value of Ishak fibrosis stage: Findings from the hepatitis C antiviral long-term treatment against cirrhosis trial. Hepatology 2010, 51, 585–594. [Google Scholar] [CrossRef]
- Mari, P.C.; Gulati, R.; Fragassi, P. Adolescent Hepatitis C: Prevalence, Impact, and Management Challenges. Adolesc. Health Med. Ther. 2021, 12, 45–53. [Google Scholar] [CrossRef]
- Pradat, P.; Voirin, N.; Tillmann, H.L.; Chevallier, M.; Trépo, C. Progression to cirrhosis in hepatitis C patients: An age-dependent process. Liver Int. 2007, 27, 335–339. [Google Scholar] [CrossRef]
- Mehta, S.H.; Brancati, F.L.; Sulkowski, M.S.; Strathdee, S.A.; Szklo, M.; Thomas, D.L. Prevalence of type 2 diabetes mellitus among persons with hepatitis C virus infection in the United States. Ann. Intern. Med. 2000, 133, 592–599. [Google Scholar] [CrossRef]
- Agnello, V.; Chung, R.T.; Kaplan, L.M. A role for hepatitis C virus infection in type II cryoglobulinemia. N. Engl. J. Med. 1992, 327, 1490–1495. [Google Scholar] [CrossRef]
- Gill, K.; Ghazinian, H.; Manch, R.; Gish, R. Hepatitis C virus as a systemic disease: Reaching beyond the liver. Hepatol. Int. 2016, 10, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Phelan, M.; Cook, C. A treatment revolution for those who can afford it? Hepatitis C treatment: New medications, profits and patients. BMC Infect. Dis. 2014, 14 (Suppl. S6), S5. [Google Scholar] [CrossRef]
- Ippolito, G.; Capobianchi, M.R.; Lanini, S.; Antonelli, G. Is hepatitis C virus eradication around the corner only 25 years after its discovery? Int. J. Antimicrob. Agents 2015, 45, 111–112. [Google Scholar] [CrossRef]
- Brzdęk, M.; Zarębska-Michaluk, D.; Invernizzi, F.; Cilla, M.; Dobrowolska, K.; Flisiak, R. Decade of optimizing therapy with direct-acting antiviral drugs and the changing profile of patients with chronic hepatitis C. World J. Gastroenterol. 2023, 29, 949–966. [Google Scholar] [CrossRef]
- Kish, T.; Aziz, A.; Sorio, M. Hepatitis C in a New Era: A Review of Current Therapies. Pharm. Ther. 2017, 42, 316–329. [Google Scholar]
- Lee, S.W.; Lee, T.Y.; Yang, S.S.; Peng, Y.C.; Yeh, H.Z.; Chang, C.S. Prevalence of Hepatitis B Reactivation Among Chinese Individuals with Chronic Hepatitis C Treated with Pan-Oral Direct-Acting Antivirals. Gastroenterol. Res. 2018, 11, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Mavilia, M.G.; Wu, G.Y. HBV-HCV Coinfection: Viral Interactions, Management, and Viral Reactivation. J. Clin. Transl. Hepatol. 2018, 6, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Mücke, M.M.; Backus, L.I.; Mücke, V.T.; Coppola, N.; Preda, C.M.; Yeh, M.-L.; Tang, L.S.Y.; Belperio, P.S.; Wilson, E.M.; Yu, M.-L.; et al. Hepatitis B virus reactivation during direct-acting antiviral therapy for hepatitis C: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2018, 3, 172–180. [Google Scholar] [CrossRef]
- University of Liverpool. Interactions with HCV DAAs and Ribavirin. Available online: www.hep-druginteractions.org/prescribing_resources/hep-summaries-hcv (accessed on 10 March 2025).
- Norton, B.L.; Fleming, J.; Bachhuber, M.A.; Steinman, M.; DeLuca, J.; Cunningham, C.O.; Johnson, N.; Laraque, F.; Litwin, A.H. High HCV cure rates for people who use drugs treated with direct acting antiviral therapy at an urban primary care clinic. Int. J. Drug Policy 2017, 47, 196–201. [Google Scholar] [CrossRef]
- Hui, V.W.-K.; Au, C.L.; Lam, A.S.M.; Yip, T.C.-F.; Tse, Y.-K.; Lai, J.C.-T.; Chan, H.L.-Y.; Wong, V.W.-S.; Wong, G.L.-H. Drug-drug interactions between direct-acting antivirals and co-medications: A territory-wide cohort study. Hepatol. Int. 2022, 16, 1318–1329. [Google Scholar] [CrossRef]
- Hayes, K.N.; Burkard, T.; Weiler, S.; Tadrous, M.; Burden, A.M. Global adverse events reported for direct-acting antiviral therapies for the treatment of hepatitis C: An analysis of the World Health Organization VigiBase. Eur. J. Gastroenterol. Hepatol. 2021, 33 (Suppl. S1), e1017–e1021. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Pockros, P.J.; Norkrans, G.; Smith, C.I.; Morgan, T.R.; Häussinger, D.; Shiffman, M.L.; Hadziyannis, S.J.; Schmidt, W.N.; Jacobson, I.M.; et al. Long-term clearance of hepatitis C virus following interferon α-2b or peginterferon α-2b, alone or in combination with ribavirin. J. Viral Hepat. 2013, 20, 524–529. [Google Scholar] [CrossRef]
- Swain, M.G.; Lai, M.-Y.; Shiffman, M.L.; Cooksley, W.G.E.; Zeuzem, S.; Dieterich, D.T.; Abergel, A.; Pessôa, M.G.; Lin, A.; Tietz, A.; et al. A sustained virologic response is durable in patients with chronic hepatitis C treated with peginterferon alfa-2a and ribavirin. Gastroenterology 2010, 139, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Marinho, R.T.; Vitor, S.; Velosa, J. Benefits of curing hepatitis C infection. J. Gastrointestin. Liver Dis. 2014, 23, 85–90. [Google Scholar] [CrossRef]
- Fabrizi, F.; Dixit, V.; Messa, P. Antiviral therapy of symptomatic HCV-associated mixed cryoglobulinemia: Meta-analysis of clinical studies. J. Med. Virol. 2013, 85, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Maddison, A.R.; Fisher, J.; Johnston, G. Preventive medication use among persons with limited life expectancy. Prog. Palliat. Care 2011, 19, 15–21. [Google Scholar] [CrossRef]
- Holmes, H.M.; Hayley, D.C.; Alexander, G.C.; Sachs, G.A. Reconsidering medication appropriateness for patients late in life. Arch. Intern. Med. 2006, 166, 605–609. [Google Scholar] [CrossRef]
- Razavi, H.; Elkhoury, A.C.; Elbasha, E.; Estes, C.; Pasini, K.; Poynard, T.; Kumar, R. Chronic hepatitis C virus (HCV) disease burden and cost in the United States. Hepatology 2013, 57, 2164–2170. [Google Scholar] [CrossRef]
- U.S. Senate Committee on Finance. The Price of Sovaldi and Its Impact on the US Health Care System. 2015. Available online: https://www.finance.senate.gov/download/the-price-of-sovaldi-and-its-impact-on-the-us-health-care-system-full-report (accessed on 10 April 2024).
- Silseth, S.; Shaw, H. Analysis of Prescription Drugs for the Treatment of Hepatitis C in the United States. 2021. Available online: https://edge.sitecorecloud.io/millimaninc5660-milliman6442-prod27d5-0001/media/Milliman/PDFs/2021-Articles/6-11-21-Analysis-prescription-drugs-treatment-hepatitis-C-US.pdf (accessed on 2 May 2024).
- He, T.; Lopez-Olivo, M.A.; Hur, C.; Chhatwal, J. Systematic review: Cost-effectiveness of direct-acting antivirals for treatment of hepatitis C genotypes 2-6. Aliment. Pharmacol. Ther. 2017, 46, 711–721. [Google Scholar] [CrossRef]
- Szabó, E.; Lotz, G.; Páska, C.; Kiss, A.; Schaff, Z. Viral hepatitis: New data on hepatitis C infection. Pathol. Oncol. Res. 2003, 9, 215–221. [Google Scholar] [CrossRef]
- Moreno, R.; Berenguer, M. Liver transplantation in patients with chronic viral hepatitis. Rev. Gastroenterol. Mex. 2005, 70, 180–191. [Google Scholar]
- van der Hilst, C.S.; Ijtsma, A.J.; Slooff, M.J.; Tenvergert, E.M. Cost of liver transplantation: A systematic review and meta-analysis comparing the United States with other OECD countries. Med. Care Res. Rev. 2009, 66, 3–22. [Google Scholar] [CrossRef]
- Leidner, A.J.; Chesson, H.W.; Xu, F.; Ward, J.W.; Spradling, P.R.; Holmberg, S.D. Cost-effectiveness of hepatitis C treatment for patients in early stages of liver disease. Hepatology 2015, 61, 1860–1869. [Google Scholar] [CrossRef] [PubMed]
- Artenie, A.A.; Bruneau, J.; Lévesque, A.; Wansuanganyi, J.M. Role of primary care providers in hepatitis C prevention and care: One step away from evidence-based practice. Can. Fam. Physician 2014, 60, 881–882. [Google Scholar]
- Ghany, M.G.; Morgan, T.R.; Panel, A.-I. HCG. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases-Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef]
- Strassl, R.; Rutter, K.; Stättermayer, A.F.; Beinhardt, S.; Kammer, M.; Hofer, H.; Ferenci, P.; Popow-Kraupp, T. Real-Time PCR Assays for the Quantification of HCV RNA: Concordance, Discrepancies and Implications for Response Guided Therapy. PLoS ONE 2015, 10, e0135963. [Google Scholar] [CrossRef] [PubMed]
- Stauber, R.E.; Lackner, C. Noninvasive diagnosis of hepatic fibrosis in chronic hepatitis C. World J. Gastroenterol. 2007, 13, 4287–4294. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.L.; Hu, K.Q. Clinical Monitoring of Chronic Hepatitis C Based on its Natural History and Therapy. N. Am. J. Med. Sci. 2014, 7, 21–27. [Google Scholar]
- U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA Warns of Serious Slowing of the Heart Rate When Antiarrhythmic Drug Amiodarone Is Used with Hepatitis C Treatments Containing Sofosbuvir (Harvoni) or Sovaldi in Combination with Another Direct Acting Antiviral Drug. 2015. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-warns-serious-slowing-heart-rate-when-antiarrhythmic-drug (accessed on 25 June 2025).
- Morisco, F.; Granata, R.; Stroffolini, T.; Guarino, M.; Donnarumma, L.; Gaeta, L.; Loperto, I.; Gentile, I.; Auriemma, F.; Caporaso, N. Sustained virological response: A milestone in the treatment of chronic hepatitis C. World J. Gastroenterol. 2013, 19, 2793–2798. [Google Scholar] [CrossRef]
- AASLD; IDSA. Monitoring Patients Who Are Starting HCV Treatment, Are on Treatment, or Have Completed Therapy. 2023. Available online: https://www.hcvguidelines.org/evaluate/monitoring (accessed on 25 June 2025).
- Sarrazin, C.; Isakov, V.; Svarovskaia, E.S.; Hedskog, C.; Martin, R.; Chodavarapu, K.; Brainard, D.M.; Miller, M.D.; Mo, H.; Molina, J.-M.; et al. Late Relapse Versus Hepatitis C Virus Reinfection in Patients with Sustained Virologic Response After Sofosbuvir-Based Therapies. Clin. Infect. Dis. 2017, 64, 44–52. [Google Scholar] [CrossRef]
- Simmons, B.; Saleem, J.; Hill, A.; Riley, R.D.; Cooke, G.S. Risk of Late Relapse or Reinfection with Hepatitis C Virus After Achieving a Sustained Virological Response: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2016, 62, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.D.; Sarrazin, C. Management of HCV-Associated Liver Cirrhosis. Visc. Med. 2016, 32, 96–104. [Google Scholar] [CrossRef]
- Maness, D.L.; Riley, E.; Studebaker, G. Hepatitis C: Diagnosis and Management. Am. Fam. Physician 2021, 104, 626–635. [Google Scholar]
- AASLD; IDSA. HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Available online: https://www.hcvguidelines.org/treatment-experienced/sof-and-elb-grz-failures (accessed on 10 April 2025).
- Re, V.L.; Kallan, M.J.; Tate, J.P.; Localio, A.R.; Lim, J.K.; Goetz, M.B.; Klein, M.B.; Rimland, D.; Rodriguez-Barradas, M.C.; Butt, A.A.; et al. Hepatic decompensation in antiretroviral-treated patients co-infected with HIV and hepatitis C virus compared with hepatitis C virus-monoinfected patients: A cohort study. Ann. Intern. Med. 2014, 160, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Kirk, G.D.; Mehta, S.H.; Astemborski, J.; Galai, N.; Washington, J.; Higgins, Y.; Balagopal, A.; Thomas, D.L. HIV, age, and the severity of hepatitis C virus-related liver disease: A cohort study. Ann. Intern. Med. 2013, 158, 658–666. [Google Scholar] [CrossRef]
- Rockstroh, J.K.; Lacombe, K.; Viani, R.M.; Orkin, C.; Wyles, D.; Luetkemeyer, A.F.; Soto-Malave, R.; Flisiak, R.; Bhagani, S.; Sherman, K.E.; et al. Efficacy and Safety of Glecaprevir/Pibrentasvir in Patients Coinfected with Hepatitis C Virus and Human Immunodeficiency Virus Type 1: The EXPEDITION-2 Study. Clin. Infect. Dis. 2018, 67, 1010–1017. [Google Scholar] [CrossRef] [PubMed]
- Wyles, D.; Bräu, N.; Kottilil, S.; Daar, E.S.; Ruane, P.; Workowski, K.; Luetkemeyer, A.; Adeyemi, O.; Kim, A.Y.; Doehle, B.; et al. Sofosbuvir and Velpatasvir for the Treatment of Hepatitis C Virus in Patients Coinfected with Human Immunodeficiency Virus Type 1: An Open-Label, Phase 3 Study. Clin. Infect. Dis. 2017, 65, 6–12. [Google Scholar] [CrossRef]
- Naggie, S.; Cooper, C.; Saag, M.; Workowski, K.; Ruane, P.; Towner, W.J.; Marks, K.; Luetkemeyer, A.; Baden, R.P.; Sax, P.E.; et al. Ledipasvir and Sofosbuvir for HCV in Patients Coinfected with HIV-1. N. Engl. J. Med. 2015, 373, 705–713. [Google Scholar] [CrossRef]
- Bhattacharya, D.; Belperio, P.S.; Shahoumian, T.A.; Loomis, T.P.; Goetz, M.B.; Mole, L.A.; Backus, L.I. Effectiveness of All-Oral Antiviral Regimens in 996 Human Immunodeficiency Virus/Hepatitis C Virus Genotype 1-Coinfected Patients Treated in Routine Practice. Clin. Infect. Dis. 2017, 64, 1711–1720. [Google Scholar] [CrossRef]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Donahue, K.; Doubeni, C.A.; Epling, J.W., Jr.; Kubik, M.; et al. Screening for Hepatitis C Virus Infection in Adolescents and Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2020, 323, 970–975. [Google Scholar] [CrossRef]
- Conte, D.; Fraquelli, M.; Prati, D.; Colucci, A.; Minola, E. Prevalence and clinical course of chronic hepatitis C virus (HCV) infection and rate of HCV vertical transmission in a cohort of 15,250 pregnant women. Hepatology 2000, 31, 751–755. [Google Scholar] [CrossRef]
- Gervais, A.; Bacq, Y.; Bernuau, J.; Martinot, M.; Auperin, A.; Boyer, N.; Kilani, A.; Erlinger, S.; Valla, D.; Marcellin, P. Decrease in serum ALT and increase in serum HCV RNA during pregnancy in women with chronic hepatitis C. J. Hepatol. 2000, 32, 293–299. [Google Scholar] [CrossRef] [PubMed]
- AASLD; IDSA. HCV in Pregnancy. 2023. Available online: https://www.hcvguidelines.org/unique-populations/pregnancy (accessed on 24 June 2025).
- Rogal, S.S.; Yan, P.; Rimland, D.; Re, V.L.; Al-Rowais, H.; Fried, L.; Butt, A.A. Incidence and Progression of Chronic Kidney Disease After Hepatitis C Seroconversion: Results from ERCHIVES. Dig. Dis. Sci. 2016, 61, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Fabrizi, F.; Verdesca, S.; Messa, P.; Martin, P. Hepatitis C Virus Infection Increases the Risk of Developing Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2015, 60, 3801–3813. [Google Scholar] [CrossRef] [PubMed]
- El-Sherif, O.; Jiang, Z.G.; Tapper, E.B.; Huang, K.C.; Zhong, A.; Osinusi, A.; Charlton, M.; Manns, M.; Afdhal, N.H.; Mukamal, K.; et al. Baseline Factors Associated with Improvements in Decompensated Cirrhosis After Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection. Gastroenterology 2018, 154, 2111–2121.e8. [Google Scholar] [CrossRef]
- Terrault, N.A.; McCaughan, G.W.; Curry, M.P.; Gane, E.; Fagiuoli, S.; Fung, J.Y.Y.; Agarwal, K.; Lilly, L.; Strasser, S.I.; Brown, K.A.; et al. International Liver Transplantation Society Consensus Statement on Hepatitis C Management in Liver Transplant Candidates. Transplantation 2017, 101, 945–955. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Genotype | Condition | HCV Treatment Regimens |
|---|---|---|
| Genotype 1a | Well Compensated or No Cirrhosis | - Glecaprevir/pibrentasvir (Mavyret) 300/120 mg once daily for 8 weeks - Ledipasvir/sofosbuvir (Harvoni) 90/400 mg once daily for 12 weeks - Sofosbuvir/velpatasvir (Epclusa) 400/100 mg once daily for 12 weeks - Ledipasvir/Sofosbuvir 90/400 for 8 weeks for HIV-uninfected and HCV RNA < 6 million IU/ml - Elbasvir/grazoprevir (Zepatier) 50/100 mg once daily for 12 weeks (alternate) |
| Genotype 1b | Well Compensated or No Cirrhosis | - Glecaprevir/pibrentasvir (Mavyret) 300/120 mg once daily for 8 weeks - Ledipasvir/sofosbuvir (Harvoni) 90/400 mg once daily for 12 weeks - Sofosbuvir/velpatasvir (Epclusa) 400/100 mg once daily for 12 weeks - Ledipasvir/Sofosbuvir 90/400 for 8 weeks for HIV-uninfected and HCV RNA < 6 million IU/ml - Elbasvir/grazoprevir (Zepatier) 50/100 mg once daily for 12 weeks |
| Genotype 1 | Decompensated Liver Disease | - Paritaprevir 150 mg + ritonavir 100 mg + ombitasvir 25 mg + dasabuvir 250 mg twice daily + ribavirin for 12 weeks - Sofosbuvir 400 mg/ledipasvir 90 mg + low-dose ribavirin (600 mg; increase as tolerated) for 12 weeks - Sofosbuvir 400 mg/velpatasvir 100 mg + weight-based ribavirin for 12 weeks |
| Genotype 2 | Well Compensated or No Cirrhosis | - Glecaprevir/pibrentasvir (Mavyret) 300/120 mg once daily for 8 weeks - Sofosbuvir/velpatasvir (Epclusa) 400/100 mg once daily for 12 weeks |
| Decompensated Liver Disease | - Sofosbuvir 400 mg/velpatasvir 100 mg + weight-based ribavirin for 12 weeks | |
| Genotype 3 | Well Compensated or No Cirrhosis | - Glecaprevir/pibrentasvir (Mavyret) 300/120 mg once daily for 8 weeks - Sofosbuvir/velpatasvir (Epclusa) 400/100 mg once daily for 12 weeks - Sofosbuvir/daclatasvir (Sovaldi) 400/60 mg once daily +/− RBV (compensated cirrhosis) for 12 weeks |
| Decompensated Liver Disease | - Sofosbuvir 400 mg/velpatasvir 100 mg + weight-based ribavirin for 12 weeks | |
| Genotype 4 | Well Compensated or No Cirrhosis | - Glecaprevir/pibrentasvir (Mavyret) 300/120 mg once daily for 8 weeks - Sofosbuvir/velpatasvir (Epclusa) 400/100 mg once daily for 12 weeks - Ledipasvir/sofosbuvir (Harvoni) 90/400 mg once daily for 12 weeks - Elbasvir/grazoprevir (Zepatier) 50/100 mg once daily for 12 weeks |
| Decompensated Liver Disease | - Sofosbuvir 400 mg/ledipasvir 90 mg + low-dose ribavirin (600 mg; increase as tolerated) for 12 weeks - Sofosbuvir 400 mg/velpatasvir 100 mg + weight-based ribavirin for 12 weeks | |
| Genotypes 5 and 6 | Well Compensated or No Cirrhosis | - Glecaprevir/pibrentasvir (Mavyret) 300/120 mg once daily for 8 weeks - Sofosbuvir/velpatasvir (Epclusa) 400/100 mg once daily for 12 weeks - Ledipasvir/sofosbuvir (Harvoni) 90/400 mg once daily for 12 weeks |
| Decompensated Liver Disease | - Sofosbuvir 400 mg/ledipasvir 90 mg + low-dose ribavirin (600 mg; increase as tolerated) for 12 weeks - Sofosbuvir 400 mg/velpatasvir 100 mg + weight-based ribavirin for 12 weeks | |
| Genotypes 1–6 | Renal Failure (CrCl < 30 mL/min) | No dose adjustment in direct-acting antivirals is required when using recommended regimens |
| Genotypes 1–6 | Decompensated Cirrhosis—Ribavirin Ineligible | - Sofosbuvir/velpatasvir (Epclusa) 400/100 mg once daily for 24 weeks |
| Genotype 1, 4, 5, or 6 Only | Decompensated Cirrhosis—Ribavirin Ineligible | - Ledipasvir/sofosbuvir (Harvoni) 90/400 mg once daily for 24 weeks |
| Cautions for Concurrent PPI Use | - PPIs may lower ledipasvir, so administer 4 hours before - PPI may increase concentrations of ombitasvir and dasabuvir—8 weeks for patients without HIV with HCV RNA level < 6 million IU/mL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benjaram, S.; Kapur, S.; McKay, A.; Almujarkesh, M.K.; Carter, K.S.; Picardal, A.; Levine, D.; Lohia, P. Hepatitis C—Everything a Primary Care Physician Needs to Know About Diagnosis, Management, and Follow-Up. J. Clin. Med. 2025, 14, 4801. https://doi.org/10.3390/jcm14134801
Benjaram S, Kapur S, McKay A, Almujarkesh MK, Carter KS, Picardal A, Levine D, Lohia P. Hepatitis C—Everything a Primary Care Physician Needs to Know About Diagnosis, Management, and Follow-Up. Journal of Clinical Medicine. 2025; 14(13):4801. https://doi.org/10.3390/jcm14134801
Chicago/Turabian StyleBenjaram, Sindhuri, Shweta Kapur, Anusha McKay, Mohamad Khaled Almujarkesh, Kassandra S. Carter, Alexandra Picardal, Diane Levine, and Prateek Lohia. 2025. "Hepatitis C—Everything a Primary Care Physician Needs to Know About Diagnosis, Management, and Follow-Up" Journal of Clinical Medicine 14, no. 13: 4801. https://doi.org/10.3390/jcm14134801
APA StyleBenjaram, S., Kapur, S., McKay, A., Almujarkesh, M. K., Carter, K. S., Picardal, A., Levine, D., & Lohia, P. (2025). Hepatitis C—Everything a Primary Care Physician Needs to Know About Diagnosis, Management, and Follow-Up. Journal of Clinical Medicine, 14(13), 4801. https://doi.org/10.3390/jcm14134801