

Comparative Effectiveness of Combination Versus Single-Modality Physiotherapy for Rotator Cuff-Related Shoulder Pain: A Systematic Review and Network Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Database Searches and Study Identification
2.2. Inclusion and Exclusion Criteria
2.3. Standardization for Comparison
2.4. Modeling for Network Meta-Analysis
2.5. Methodological Quality Appraisal
2.6. Primary Outcome: Functional Improvement (Standardized Mean Difference)
2.7. Secondary Outcomes: Pain Reduction (Standardized Mean Difference)
2.8. Data Extraction, Management, and Conversion
2.9. Statistical Analysis
2.10. Sensitivity Analyses
2.11. Publication Bias
3. Results
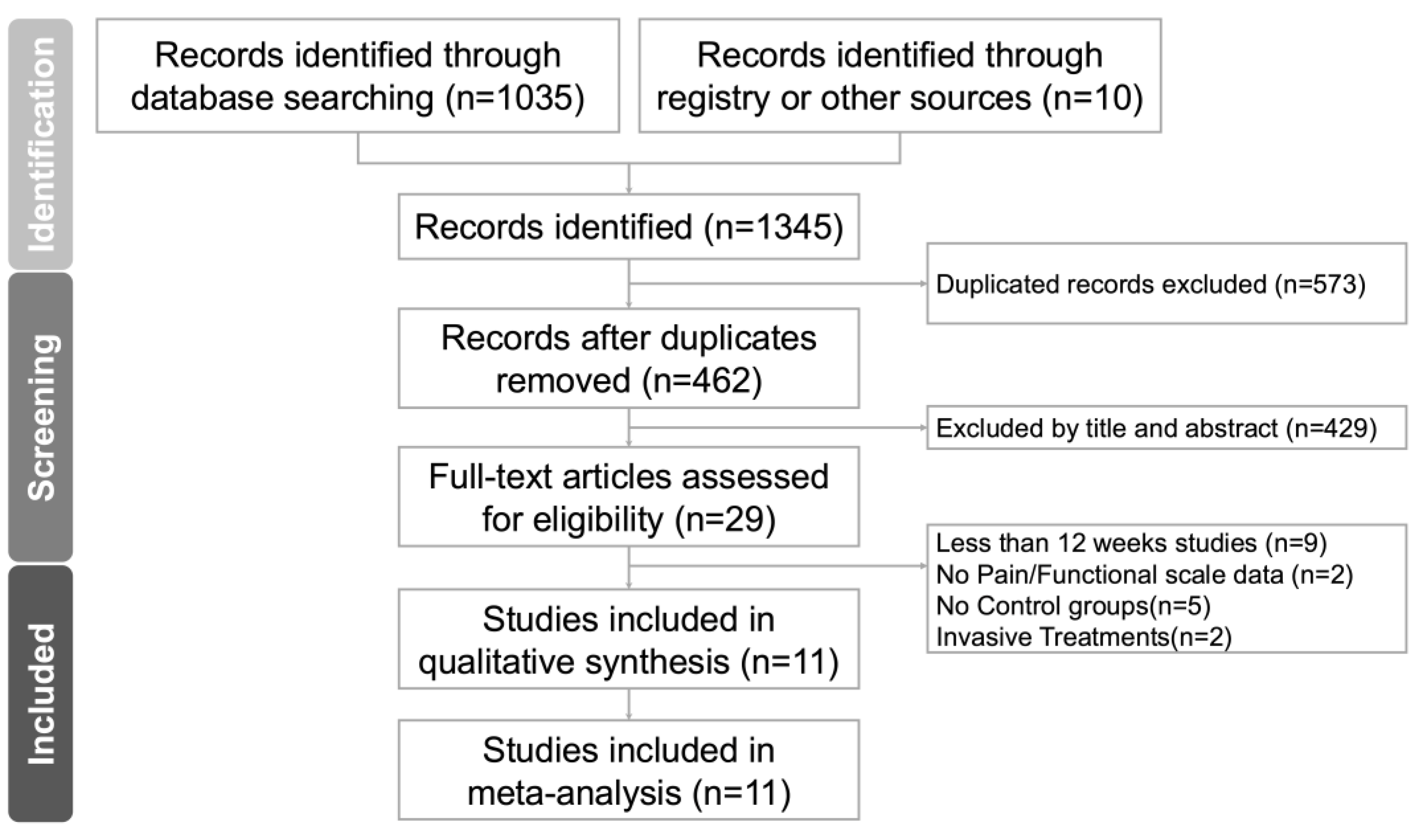
3.1. Study Identification and Network Model Formation
3.2. Methodological Quality of the Included Studies
3.3. Primary Outcome: Combination Therapy Most Effective for Functional Improvement
3.4. Secondary Outcome: Combination Therapy Most Effective for Pain Reduction
3.5. Inconsistency Test
3.6. Sensitivity Analyses
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RCRSP | Rotator cuff-related shoulder pain |
| NMA | Meta-analysis |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PRISMA-NMA | PRISMA extension guidelines for network meta-analysis |
| KT | Kinesio taping |
| SPADI | Shoulder Pain and Disability Index |
| DASH | Disabilities of the Arm, Shoulder and Hand |
| VAS | Visual Analog Scale |
| NPRS | Numeric Pain Rating Scale |
| SIS | Subacromial impingement syndrome |
| TENS | Transcutaneous electrical nerve stimulation |
| EMS | Electrical muscular stimulation |
| PNF | Proprioceptive neuromuscular facilitation |
| SM | Shoulder mobilization |
| TrP-DN | Trigger point dry needling |
| SPS | Subacromial pain syndrome |
| PENS | Percutaneous electrical nerve stimulation |
| ESWT | Extracorporeal shock wave therapy |
| MET | Muscle energy technique |
References
- Aguilar García, M.; González Muñoz, A.; Pérez Montilla, J.J.; Aguilar Nuñez, D.; Hamed Hamed, D.; Pruimboom, L.; Navarro Ledesma, S. Which Multimodal Physiotherapy Treatment Is the Most Effective in People with Shoulder Pain? A Systematic Review and Meta-Analyses. Healthcare 2024, 12, 1234. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, F.C.L.; Pairot de Fontenay, B.; Bouyer, L.J.; Desmeules, F.; Roy, J.S. Kinesiotaping for the Rehabilitation of Rotator Cuff-Related Shoulder Pain: A Randomized Clinical Trial. Sports Health 2021, 13, 161–172. [Google Scholar] [CrossRef]
- Hunter, D.J.; Rivett, D.A.; McKiernan, S.; Luton, R.; Snodgrass, S.J. Thoracic Manual Therapy Improves Pain and Disability in Individuals with Shoulder Impingement Syndrome Compared with Placebo: A Randomized Controlled Trial With 1-Year Follow-up. Arch. Phys. Med. Rehabil. 2022, 103, 1533–1543. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-Espinoza, H.; Araya-Quintanilla, F.; Cereceda-Muriel, C.; Alvarez-Bueno, C.; Martinez-Vizcaino, V.; Cavero-Redondo, I. Effect of supervised physiotherapy versus home exercise program in patients with subacromial impingement syndrome: A systematic review and meta-analysis. Phys. Ther. Sport. 2020, 41, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Diaz, M.; Ruiz-Redondo, R.; Escobio-Prieto, I.; De la Fuente-Costa, M.; Albornoz-Cabello, M.; Casana, J. A Systematic Review of the Effectiveness of Dry Needling in Subacromial Syndrome. Biology 2022, 11, 243. [Google Scholar] [CrossRef]
- Dube, M.O.; Desmeules, F.; Lewis, J.S.; Roy, J.S. Does the addition of motor control or strengthening exercises to education result in better outcomes for rotator cuff-related shoulder pain? A multiarm randomised controlled trial. Br. J. Sports Med. 2023, 57, 457–463. [Google Scholar] [CrossRef]
- Hopewell, S.; Keene, D.J.; Heine, P.; Marian, I.R.; Dritsaki, M.; Cureton, L.; Dutton, S.J.; Dakin, H.; Carr, A.; Hamilton, W.; et al. Progressive exercise compared with best-practice advice, with or without corticosteroid injection, for rotator cuff disorders: The GRASP factorial RCT. Health Technol. Assess. 2021, 25, 1–158. [Google Scholar] [CrossRef]
- Lathiere, T.; Jaubert, A.; Lewis, J.; David-Tchouda, S.; Beard, D.; Pinsault, N. The health economic analysis of surgery versus rehabilitation in non-traumatic musculoskeletal shoulder disorders: A systematic review of trial-based studies. Clin. Rehabil. 2025, 39, 139–152. [Google Scholar] [CrossRef]
- Blume, C.; Wang-Price, S.; Trudelle-Jackson, E.; Ortiz, A. Comparison of Eccentric and Concentric Exercise Interventions in Adults with Subacromial Impingement Syndrome. Int. J. Sports Phys. Ther. 2015, 10, 441–455. [Google Scholar]
- Christiansen, D.H.; Hjort, J. Group-based exercise, individually supervised exercise and home-based exercise have similar clinical effects and cost-effectiveness in people with subacromial pain: A randomised trial. J. Physiother. 2021, 67, 124–131. [Google Scholar] [CrossRef]
- Gutiérrez-Espinoza, H.; Araya-Quintanilla, F.; Gutiérrez-Monclus, R.; Ríos-Riquelme, M.; Álvarez-Bueno, C.; Martínez-Vizcaino, V.; Cavero-Redondo, I. Does pectoralis minor stretching provide additional benefit over an exercise program in participants with subacromial pain syndrome? A randomized controlled trial. Musculoskelet. Sci. Pract. 2019, 44, 102052. [Google Scholar] [CrossRef]
- Aytar, A.; Baltaci, G.; Uhl, T.L.; Tuzun, H.; Oztop, P.; Karatas, M. The effects of scapular mobilization in patients with subacromial impingement syndrome: A randomized, double-blind, placebo-controlled clinical trial. J. Sport. Rehabil. 2015, 24, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Frassanito, P.; Cavalieri, C.; Maestri, R.; Felicetti, G. Effectiveness of Extracorporeal Shock Wave Therapy and kinesio taping in calcific tendinopathy of the shoulder: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Umay-Altas, E.; Ecem-Konak, H.; Unsal-Delialioglu, S.; Sahin-Onat, S.; Gunay-Ucurum, S. Mid-term effects of two different Kinesio tape treatments in female patients with subacromial impingement syndrome: Randomized controlled ultrasonographic study. J. Hand Ther. 2023, 36, 514–522. [Google Scholar] [CrossRef]
- de Oliveira, A.K.A.; da Costa, K.S.A.; de Lucena, G.L.; de Oliveira Sousa, C.; Filho, J.F.M.; Brasileiro, J.S. Comparing exercises with and without electromyographic biofeedback in subacromial pain syndrome: A randomized controlled trial. Clin. Biomech. 2022, 93, 105596. [Google Scholar] [CrossRef] [PubMed]
- Nazary-Moghadam, S.; Zarei-Moghadam, F.; Zeinalzadeh, A.; Ebrahimzadeh, M.H.; Moradi, A.; Emadzadeh, M.; Hasson, S. Effects of comprehensive physiotherapy compared with routine physiotherapy on pain and function in patients with subacromial pain syndrome: A randomized clinical trial with 6-month follow-up. J. Bodyw. Mov. Ther. 2024, 40, 270–278. [Google Scholar] [CrossRef]
- Boudreau, N.; Gaudreault, N.; Roy, J.S.; Bedard, S.; Balg, F. The Addition of Glenohumeral Adductor Coactivation to a Rotator Cuff Exercise Program for Rotator Cuff Tendinopathy: A Single-Blind Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2019, 49, 126–135. [Google Scholar] [CrossRef]
- Menek, B.; Tarakci, D.; Algun, Z.C. The effect of Mulligan mobilization on pain and life quality of patients with Rotator cuff syndrome: A randomized controlled trial. J. Back. Musculoskelet. Rehabil. 2019, 32, 171–178. [Google Scholar] [CrossRef]
- Saracoglu, I.; Emuk, Y.; Taspinar, F. Does taping in addition to physiotherapy improve the outcomes in subacromial impingement syndrome? A systematic review. Physiother. Theory Pract. 2018, 34, 251–263. [Google Scholar] [CrossRef]
- Camargo, P.R.; Alburquerque-Sendin, F.; Avila, M.A.; Haik, M.N.; Vieira, A.; Salvini, T.F. Effects of Stretching and Strengthening Exercises, With and Without Manual Therapy, on Scapular Kinematics, Function, and Pain in Individuals With Shoulder Impingement: A Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2015, 45, 984–997. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Owen, R.K.; Bradbury, N.; Xin, Y.; Cooper, N.; Sutton, A. MetaInsight: An interactive web-based tool for analyzing, interrogating, and visualizing network meta-analyses using R-shiny and netmeta. Res. Synth. Methods 2019, 10, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Gillison, F.B.; Skevington, S.M.; Sato, A.; Standage, M.; Evangelidou, S. The effects of exercise interventions on quality of life in clinical and healthy populations; a meta-analysis. Soc. Sci. Med. 2009, 68, 1700–1710. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Ager, A.L.; de Oliveira, F.C.L.; Roy, J.S.; Borms, D.; Deraedt, M.; Huyge, M.; Deschepper, A.; Cools, A.M. Effects of elastic kinesiology taping on shoulder proprioception: A systematic review. Braz. J. Phys. Ther. 2023, 27, 100514. [Google Scholar] [CrossRef]
- Guo, R.; Luo, Y.; Xu, Y.; Lan, K.; Zhao, Y. Efficacy of modified posterior shoulder stretching exercises on shoulder function in subacromial impingement syndrome: A comprehensive meta-analysis. Medicine 2025, 104, e41117. [Google Scholar] [CrossRef]
- Yang, F.; Li, X.; Wang, J.; Gao, Q.; Pan, M.; Duan, Z.; Ren, C.; Guo, P.; Zhang, Y. Efficacy of different analgesic strategies combined with conventional physiotherapy program for treating chronic shoulder pain: A systematic review and network meta-analysis. J. Orthop. Surg. Res. 2024, 19, 544. [Google Scholar] [CrossRef]
- Chaimani, A.C.D.; Li, T.; Higgins, J.P.T.; Salanti, G. Chapter 11: Undertaking network meta-analyses [last updated October 2019]. In Cochrane Handbook for Systematic Reviews of Interventions Version 65; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Deeks, J.J. Chapter 6: Choosing effect measures and computing estimates of effect [last updated August 2023]. In Cochrane Handbook for Systematic Reviews of Interventions Version 65; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G.; McKenzie, J.E.; Veroniki, A.A. Chapter 10: Analysing data and undertaking meta-analyses [last updated November 2024]. In Cochrane Handbook for Systematic Reviews of Interventions Version 65; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024. [Google Scholar]
- Page, M.J.; Higgins, J.P.T.; Sterne, J.A.C. Chapter 13: Assessing risk of bias due to missing evidence in a meta-analysis [last updated August 2024]. In Cochrane Handbook for Systematic Reviews of Interventions version 65; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024. [Google Scholar]
- Higgins, J.P.T.; Eldridge, S.; Li, T. Chapter 23: Including variants on randomized trials [last updated October 2019]. In Cochrane Handbook for Systematic Reviews of Interventions Version 65; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2024. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Fixed-Effect Versus Random-Effects Models: Introduction to Meta-Analysis; John Wiley & Sons: Chichester, UK, 2009; pp. 77–86. [Google Scholar]
- Kelley, K.; Preacher, K.J. On Effect Size. Psychol. Methods 2012, 17, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Igrek, S.; Colak, T.K. Comparison of the effectiveness of proprioceptive neuromuscular facilitation exercises and shoulder mobilization patients with Subacromial Impingement Syndrome: A randomized clinical trial. J. Bodyw. Mov. Ther. 2022, 30, 42–52. [Google Scholar] [CrossRef]
- Arias-Buria, J.L.; Fernandez-de-Las-Penas, C.; Palacios-Cena, M.; Koppenhaver, S.L.; Salom-Moreno, J. Exercises and Dry Needling for Subacromial Pain Syndrome: A Randomized Parallel-Group Trial. J. Pain. 2017, 18, 11–18. [Google Scholar] [CrossRef]
- Valenzuela-Rios, C.; Arias-Buria, J.L.; Rodriguez-Jimenez, J.; Palacios-Cena, M.; Fernandez-de-Las-Penas, C. Effects of Adding Four Sessions of Ultrasound-Guided Percutaneous Electrical Nerve Stimulation to an Exercise Program in Patients with Shoulder Pain: A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 3171. [Google Scholar] [CrossRef]
- Gunay Ucurum, S.; Kaya, D.O.; Kayali, Y.; Askin, A.; Tekindal, M.A. Comparison of different electrotherapy methods and exercise therapy in shoulder impingement syndrome: A prospective randomized controlled trial. Acta Orthop. Traumatol. Turc. 2018, 52, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Moslehi, M.; Letafatkar, A.; Miri, H. Feedback improves the scapular-focused treatment effects in patients with shoulder impingement syndrome. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 2281–2288. [Google Scholar] [CrossRef]
- Karamanlioglu, D.S.; Kaysin, M.Y.; Begoglu, F.A.; Akpinar, P.; Ozkan, F.U.; Aktas, I. Effects of acupuncture on pain and function in patients with subacromial impingement syndrome: A randomized sham-controlled trial. Integr. Med. Res. 2024, 13, 101049. [Google Scholar] [CrossRef] [PubMed]
- Arias-Buria, J.L.; Truyols-Dominguez, S.; Valero-Alcaide, R.; Salom-Moreno, J.; Atin-Arratibel, M.A.; Fernandez-de-Las-Penas, C. Ultrasound-Guided Percutaneous Electrolysis and Eccentric Exercises for Subacromial Pain Syndrome: A Randomized Clinical Trial. Evid. Based Complement. Altern. Med. 2015, 2015, 315219. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Merino, L.; Casajuana, M.; Bernal, G.; Faba, J.; Astilleros, A.; González, R.; Giralt, M.; Romeu, M.; Nogués, M. Evaluation of the effectiveness of three physiotherapeutic treatments for subacromial impingement syndrome: A randomised clinical trial. Physiotherapy 2016, 102, 57–63. [Google Scholar] [CrossRef]
- Ager, A.L.; Roy, J.S.; Gamache, F.; Hebert, L.J. The Effectiveness of an Upper Extremity Neuromuscular Training Program on the Shoulder Function of Military Members With a Rotator Cuff Tendinopathy: A Pilot Randomized Controlled Trial. Mil. Med. 2019, 184, e385–e393. [Google Scholar] [CrossRef]
- Menek, B.; Tarakci, D.; Tarakci, E.; Menek, M.Y. Investigation on the Efficiency of the Closed Kinetic Chain and Video-Based Game Exercise Programs in the Rotator Cuff Rupture: A Randomized Trial. Games Health J. 2022, 11, 298–306. [Google Scholar] [CrossRef]
- Ingwersen, K.G.; Jensen, S.L.; Sørensen, L.; Jørgensen, H.R.; Christensen, R.; Søgaard, K.; Juul-Kristensen, B. Three Months of Progressive High-Load Versus Traditional Low-Load Strength Training Among Patients With Rotator Cuff Tendinopathy: Primary Results From the Double-Blind Randomized Controlled RoCTEx Trial. Orthop. J. Sports Med. 2017, 5, 2325967117723292. [Google Scholar] [CrossRef]
- Al Anazi, A.; Alghadir, A.H.; Gabr, S.A. Handgrip Strength Exercises Modulate Shoulder Pain, Function, and Strength of Rotator Cuff Muscles of Patients with Primary Subacromial Impingement Syndrome. Biomed. Res. Int. 2022, 2022, 9151831. [Google Scholar]
- Celik, E.B.; Tuncer, A. Comparing the Efficacy of Manual Therapy and Exercise to Synchronized Telerehabilitation with Self-Manual Therapy and Exercise in Treating Subacromial Pain Syndrome: A Randomized Controlled Trial. Healthcare 2024, 12, 1074. [Google Scholar] [CrossRef]
- Raeesi, J.; Negahban, H.; Kachooei, A.R.; Moradi, A.; Ebrahimzadeh, M.H.; Daghiani, M. Comparing the effect of physiotherapy and physiotherapy plus corticosteroid injection on pain intensity, disability, quality of life, and treatment effectiveness in patients with Subacromial Pain Syndrome: A randomized controlled trial. Disabil. Rehabil. 2023, 45, 4218–4226. [Google Scholar] [CrossRef]
- Daghiani, M.; Negahban, H.; Ebrahimzadeh, M.H.; Moradi, A.; Kachooei, A.R.; Raeesi, J.; Divandari, A. The effectiveness of comprehensive physiotherapy compared with corticosteroid injection on pain, disability, treatment effectiveness, and quality of life in patients with subacromial pain syndrome: A parallel, single-blind, randomized controlled trial. Physiother. Theory Pract. 2023, 39, 1591–1605. [Google Scholar] [CrossRef] [PubMed]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef]
- Roy, J.S.; MacDermid, J.C.; Woodhouse, L.J. Measuring shoulder function: A systematic review of four questionnaires. Arthritis Rheum. 2009, 61, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Deloach, J.; Porucznik, C.A.; Powell, A.P. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease. J. Shoulder Elb. Surg. 2009, 18, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Stancati, A.; Silvestri, C.A.; Ciapetti, A.; Grassi, W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur. J. Pain. 2004, 8, 283–291. [Google Scholar] [CrossRef]
- Liu, S.; Chen, L.; Shi, Q.; Fang, Y.; Da, W.; Xue, C.; Li, X. Efficacy of manual therapy on shoulder pain and function in patients with rotator cuff injury: A systematic review and meta-analysis. Biomed. Rep. 2024, 20, 89. [Google Scholar] [CrossRef]
- Jensen, M.P.; Chen, C.; Brugger, A.M. Interpretation of visual analog scale ratings and change scores: A reanalysis of two clinical trials of postoperative pain. J. Pain. 2003, 4, 407–414. [Google Scholar] [CrossRef]
- Cadogan, A.; Laslett, M.; Hing, W.A.; McNair, P.J.; Coates, M.H. A prospective study of shoulder pain in primary care: Prevalence of imaged pathology and response to guided diagnostic blocks. BMC Musculoskelet. Disord. 2011, 12, 119. [Google Scholar] [CrossRef]
- Croft, P.; Pope, D.; Silman, A. The clinical course of shoulder pain: Prospective cohort study in primary care: Primary Care Rheumatology Society Shoulder Study Group. BMJ 1996, 313, 601–602. [Google Scholar] [CrossRef] [PubMed]
- Walker-Bone, K.; van der Windt, D.A.W.M. Shoulder Pain—Where Are We Now? Curr. Treat. Options Rheumatol. 2021, 7, 285–306. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author and Year | Enrolled Population (Group population) | Population in Nodes | 12-Week DASH Improvement | 12-Week VAS Reduction | Summary |
|---|---|---|---|---|---|
| Aytar, 2015 [12] | Subacromial impingement syndrome; Total 66 (Manual: 22, Control:22, Exercise:22) | Manual Control Exercise | −12.7 ± 14.2 −17.4 ± 11.5 −17.0 ± 10.4 | −3.0 ± 2.5 −1.4 ± 1.5 −2.5 ± 1.7 | This randomized controlled trial compared scapular mobilization, sham mobilization, and supervised exercise for subacromial impingement syndrome (SAIS). All groups improved similarly in shoulder function, pain, and range of motion, without significant differences between interventions. Scapular mobilization showed no additional benefit over supervised exercise or sham treatment in managing SAIS symptoms. |
| Arias-Buría, 2017 [36] | Subacromial pain syndrome; Total: 50 (Exercise: 25, Exercise+ TrP-DN: 25) | Combination (Exercise + TrP-DN) Exercise | −50.7 ± 4.1 −28.2 ± 7.4 | −3.4 ± 0.9 −3.2 ± 0.9 | This trial assessed the effectiveness of adding Trigger Point Dry Needling (TrP-DN) to exercises in patients with SAPS. Results indicated both groups improved in pain, but the exercise plus TrP-DN group showed significantly greater improvements in shoulder-related disability across all follow-ups (3, 6, and 12 months), demonstrating sustained functional benefits. |
| Gunay-Ucurum, 2018 [38] | Subacromial pain syndrome; Total: 39 (Interferential + Exercise: 20, Exercise: 19) | Combination (Interferential + Exercise) Exercise | −24.1 ± 13.0 −18.4 ± 14.0 | −1.5 ± 1.9 −1.9 ± 1.7 | This randomized controlled trial evaluated exercise therapy combined with electrotherapy modalities in patients with shoulder impingement syndrome. All groups improved significantly in pain, function, and physical quality of life at 3 months, with interferential current providing additional significant benefits in mental quality of life compared to others. |
| Frassanito, 2018 [13] | Rotator cuff calcific tendinopathy; Total: 42 (ESWT + KT: 21, ESWT:21) | Combination (ESWT + KT) Kinesio Taping | −23.6 ± 5.4 −27.9 ± 6.1 | −2.1 ± 0.9 −2.8 ± 1.1 | This randomized controlled trial assessed whether combining Extracorporeal Shock Wave Therapy (ESWT) with Kinesio Taping (KT) is superior to ESWT alone for rotator cuff calcific tendinopathy. Forty-two patients participated, showing that ESWT combined with KT provided significantly faster pain relief and improved shoulder function compared to ESWT alone, with sustained benefits at 12 weeks post-treatment. |
| Gutiérrez-Espinoza, 2019 [11] | Subacromial pain syndrome; Total: 80 (Exercise + Manual: 40, Exercise: 40) | Combination (Exercise + Manual) Exercise | −18.5 ± 7.3 −23.9 ± 7.3 | −3.3 ± 1.1 −2.9 ± 1.1 | This randomized controlled trial compared an exercise program alone versus an exercise program combined with pectoralis minor stretching for subacromial pain syndrome (SPS). Results showed no significant short-term clinical benefits in function, pain, or muscle length with the addition of pectoralis minor stretching to the exercise program in SPS participants. |
| İğrek, 2022 [35] | Subacromial Impingement Syndrome; Total: 44 (Control: 14, SM: 15, PNF: 15) | Exercise Manual Control | −46.4 ± 14.6 −50.1 ± 14.7 −37.6 ± 11.0 | −3.2 ± 1.3 −3.0 ± 0.9 −3.3 ± 0.9 | This randomized clinical trial compared proprioceptive neuromuscular facilitation (PNF) and shoulder mobilization (SM) added to conventional physiotherapy for SIS. Both treatments improved pain and functionality better than conventional therapy alone. SM showed greater benefits in shoulder flexion range of motion, while PNF improved shoulder extension strength more effectively. |
| Hunter, 2022 [3] | Shoulder impingement syndrome; Total 50 (MET + Soft tissue massage: 25, Control: 25) | Manual (MET + Soft tissue massage) Control | −13.4 ± 10.5 −29.6 ± 8.7 | −0.5 ± 1.3 −2.1 ± 1.1 | This trial compared the thoracic spine muscle energy technique (MET) plus soft tissue massage and placebo in patients with SIS. MET significantly reduced shoulder pain and disability at 6 and 12 months compared to placebo, suggesting thoracic manual therapy as beneficial for long-term SIS management. |
| de Oliveira 2022 [15] | Subacromial pain syndrome; Total 24 (BioFB+ Exercise: 12, Exercise: 12) | Combination (BioFB + Exercise) Exercise | −22.5 ± 8.1 −8.5 ± 6.3 | −4.6 ± 1.9 −4.4 ± 1.8 | This trial compared exercises alone versus exercises with electromyographic biofeedback for subacromial pain syndrome (SPS). Both groups improved pain and function; however, adding biofeedback did not further enhance pain relief or function. Biofeedback significantly increased scapular upward rotation but did not provide superior outcomes in strength, range of motion, or muscle activation. |
| Umay-Altaş, 2023 [14] | Subacromial pain syndrome; Total 60 (Exercise + KT: 30 Exercise: 30) | Combination (Exercise + KT) Exercise | −22.4 ± 5.9 −15.5 ± 5.3 | −4.6 ± 1.1 −0.8 ± 1.3 | This randomized controlled study compared a Kinesio Taping (KT) method in female SIS patients. The KT applications improved pain, function, grip strength, acromiohumeral distance (AHD), and supraspinatus tendon thickness versus control. Taping on the deltoid muscle provided superior short- and mid-term improvements, particularly for pain, functional status, and AHD, supporting its clinical effectiveness. |
| Nazary-Moghadam, 2024 [16] | Subacromial Pain Syndrome; Total: 40 (CPT: 20, RPT: 20) | Combination (Exercise + Manual) Exercise | −31.3 ± 13.71 −8.3 ± 10.64 | −1.7 ± 1.4 −3.8 ± 1.1 | This randomized trial compared comprehensive physiotherapy (CPT), including scapular exercises and thoracic mobilization, with routine physiotherapy (RPT) for subacromial pain syndrome. Both groups improved immediately, but at 6 months, CPT significantly outperformed RPT in reducing pain, improving shoulder function, and enhancing quality of life, suggesting sustained long-term benefits with the comprehensive approach. |
| Valenzuela-Rios, 2024 [37] | Subacromial pain syndrome; Total 39 (PENS+ Exercise: 20 Exercise: 19) | Combination (PENS+ Exercise) Exercise | −25.0 ± 14.1 −17.3 ± 12.7 | −2.5 ± 0.9 −3.1 ± 1.4 | This trial compared exercise alone, exercise with percutaneous electrical nerve stimulation (PENS), and exercise with placebo PENS for SAPS. All groups improved in disability and psychological outcomes. Adding PENS provided a small, short-term advantage only in shoulder pain reduction at one month; however, there were no significant differences in disability or psychological outcomes. |
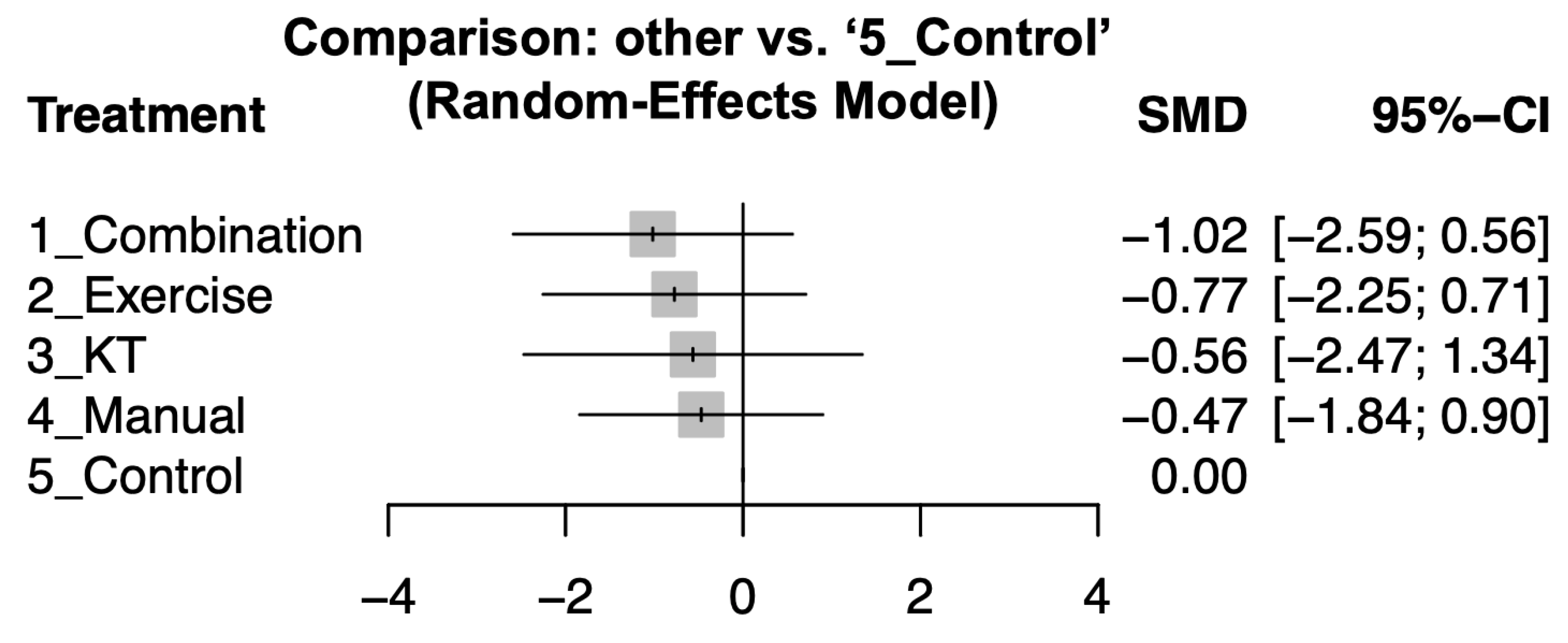
| Combination | −0.08 [−1.10; 0.93] | −0.11 [−2.57; 2.36] | −1.87 [−4.38; 0.63] | . |
| −0.24 [−1.19; 0.70] | Exercise | . | −0.04 [−1.83; 1.75] | −0.31 [−2.09; 1.47] |
| −0.45 [−2.36; 1.46] | −0.21 [−2.20; 1.78] | KT | . | −0.22 [−2.68; 2.23] |
| −0.55 [−2.04; 0.94] | −0.30 [−1.72; 1.12] | −0.09 [−2.21; 2.02] | Manual | −0.76 [−2.21; 0.70] |
| −1.02 [−2.59; 0.56] | −0.77 [−2.25; 0.71] | −0.56 [−2.47; 1.34] | −0.47 [−1.84; 0.90] | Control |
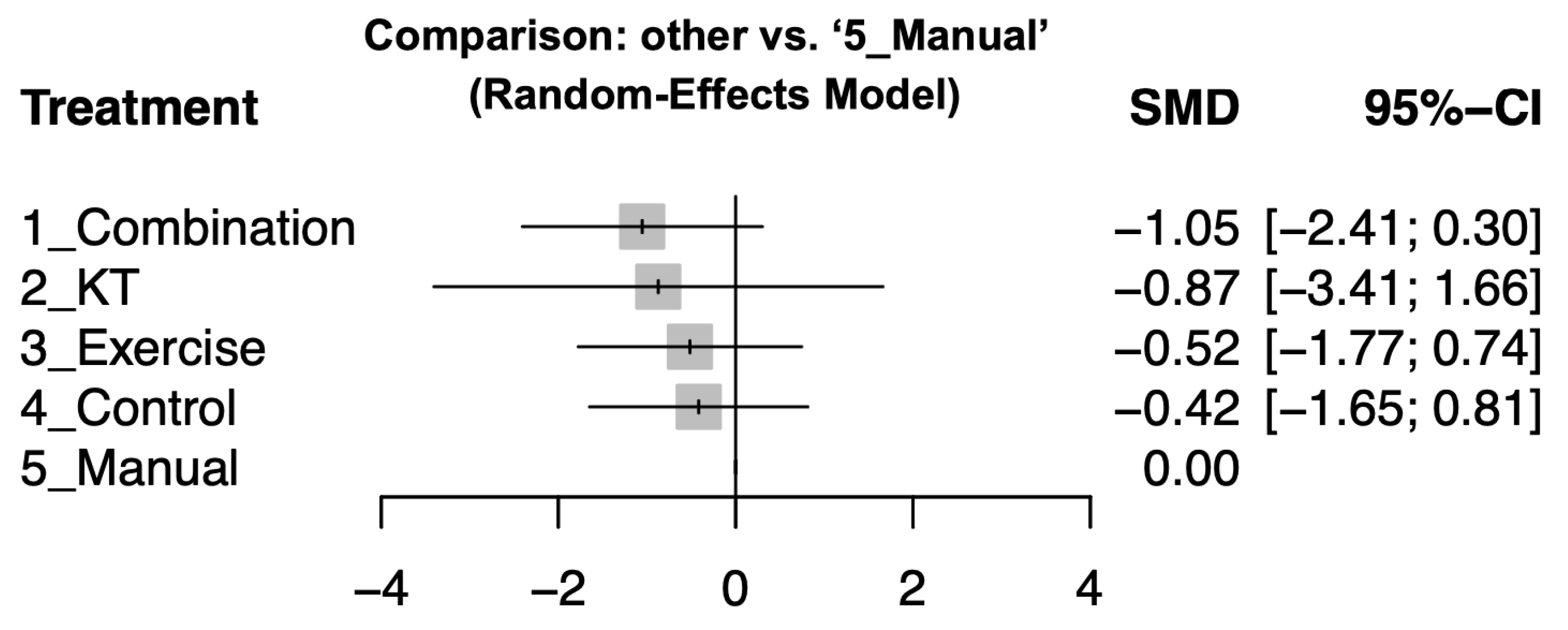
| Combination | −0.18 [−2.32; 1.96] | −0.45 [−1.33; 0.42] | . | −1.56 [−3.73; 0.61] |
| −0.18 [−2.32; 1.96] | KT | . | . | . |
| −0.54 [−1.37; 0.30] | −0.36 [−2.66; 1.94] | Exercise | −0.24 [−1.79; 1.31] | 0.03 [−1.53; 1.60] |
| −0.64 [−2.17; 0.90] | −0.46 [−3.09; 2.18] | −0.10 [−1.49; 1.30] | Control | −0.33 [−1.59; 0.94] |
| −1.05 [−2.41; 0.30] | −0.87 [−3.41; 1.66] | −0.52 [−1.77; 0.74] | −0.42 [−1.65; 0.81] | Manual |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, C.-S.; Chen, K.-C.; Shih, J.-C.; Cheng, B.; Chao, W.-C. Comparative Effectiveness of Combination Versus Single-Modality Physiotherapy for Rotator Cuff-Related Shoulder Pain: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2025, 14, 4765. https://doi.org/10.3390/jcm14134765
Lo C-S, Chen K-C, Shih J-C, Cheng B, Chao W-C. Comparative Effectiveness of Combination Versus Single-Modality Physiotherapy for Rotator Cuff-Related Shoulder Pain: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2025; 14(13):4765. https://doi.org/10.3390/jcm14134765
Chicago/Turabian StyleLo, Chien-Sheng, Kuan-Chung Chen, Jui-Chi Shih, Bill Cheng, and Wei-Cheng Chao. 2025. "Comparative Effectiveness of Combination Versus Single-Modality Physiotherapy for Rotator Cuff-Related Shoulder Pain: A Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 14, no. 13: 4765. https://doi.org/10.3390/jcm14134765
APA StyleLo, C.-S., Chen, K.-C., Shih, J.-C., Cheng, B., & Chao, W.-C. (2025). Comparative Effectiveness of Combination Versus Single-Modality Physiotherapy for Rotator Cuff-Related Shoulder Pain: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine, 14(13), 4765. https://doi.org/10.3390/jcm14134765