
The Effect of Preoperative Intravenous Iron Supplementation on Mortality and Blood Transfusion Requirements in Elderly Patients Undergoing Hip Fracture Surgery: A Prospective Randomized Controlled Trial
Abstract

1. Introduction
2. Patients and Methods
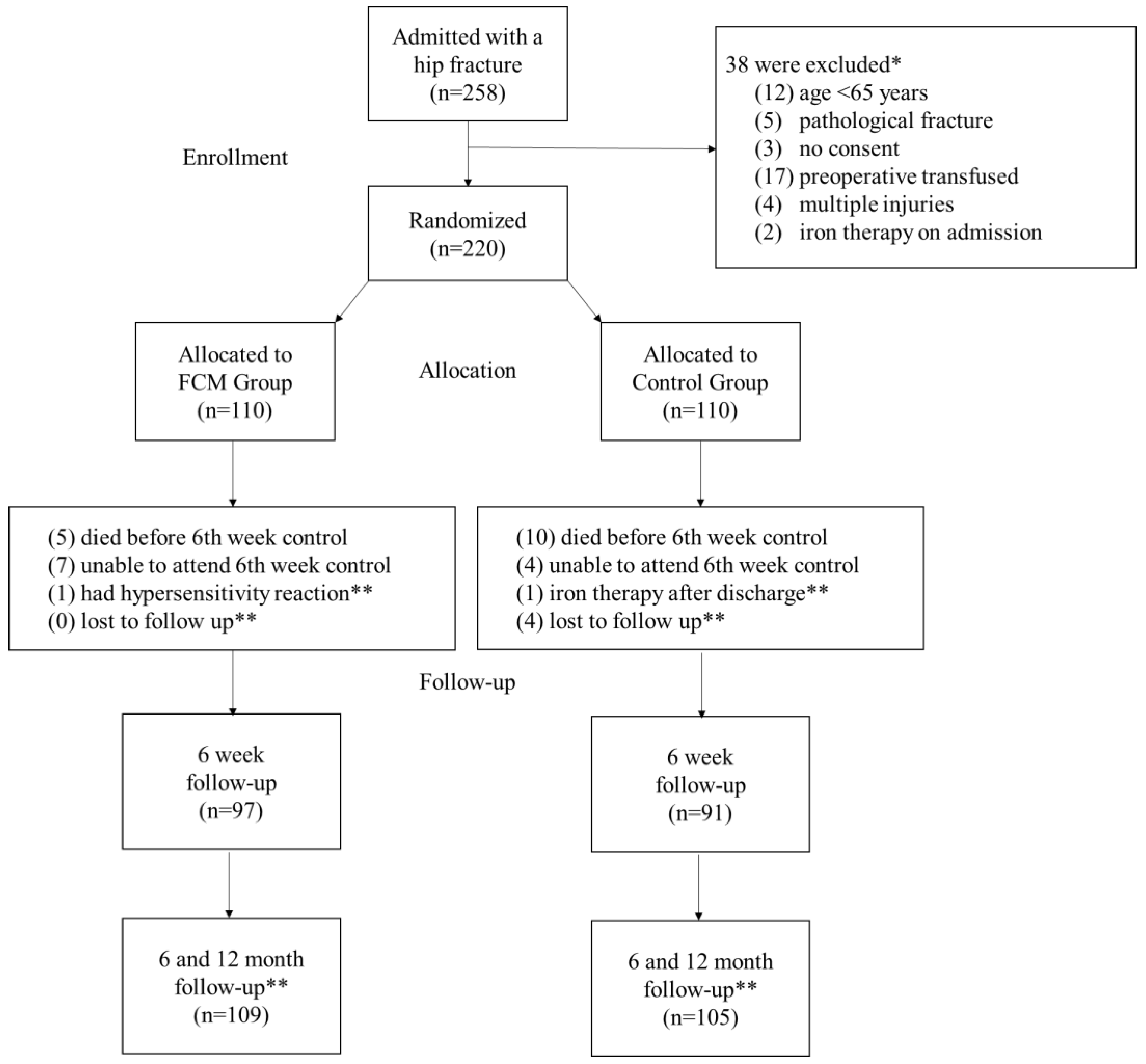
2.1. Study Design and Eligibility Criteria
2.2. Randomization and Intervention
2.3. Perioperative Transfusion Protocol
2.4. Outcome Measures and Follow-Up Protocol
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Comorbidity Profile
3.2. Primary Outcomes: Mortality Rates
3.3. Secondary Outcomes
3.3.1. Anemia Status
3.3.2. Hemoglobin Trends over Time
3.3.3. Perioperative Transfusion Characteristics
3.3.4. Length of Hospitalization
3.3.5. Adverse Events Related to FCM Administration
3.4. Multivariate Analysis of Mortality Outcomes
3.4.1. 6-Month Mortality
3.4.2. 1-Year Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists physical status classification; |
| BMI | Body Mass Index; |
| CCI | Charlson Comorbidity Index; |
| COPD | Chronic Obstructive Pulmonary Disease; |
| ES | Erythrocyte Suspension; |
| FCM | Ferric Carboxymaltose; |
| IMN | Intramedullary Nailing; |
| THA | Total Hip Arthroplasty. |
References
- Gullberg, B.; Johnell, O.; Kanis, J. World-wide projections for hip fracture. Osteoporos. Int. 1997, 7, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.J. Iron supplementation for anemia after hip fracture surgery: A randomized trial of 300 patients. JBJS 2010, 92, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Gruson, K.I.; Aharonoff, G.B.; Egol, K.A.; Zuckerman, J.D.; Koval, K.J. The relationship between admission hemoglobin level and outcome after hip fracture. J. Orthop. Trauma 2002, 16, 39–44. [Google Scholar] [CrossRef]
- Koval, K.J.; Rosenberg, A.D.; Zuckerman, J.D.; Aharonoff, G.B.; Skovron, M.L.; Bernstein, R.L.; Chakka, M. Does blood transfusion increase the risk of infection after hip fracture? J. Orthop. Trauma 1997, 11, 260–265. [Google Scholar] [CrossRef]
- Smeets, S.; Verbruggen, J.; Poeze, M. Effect of blood transfusion on survival after hip fracture surgery. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 1297–1303. [Google Scholar] [CrossRef]
- Shin, H.J.; Kim, J.H.; Han, S.-B.; Park, J.H.; Jang, W.Y. Allogeneic red blood cell transfusion is an independent risk factor for 1-year mortality in elderly patients undergoing femoral neck fracture surgery: Retrospective study. Medicine 2020, 99, e21897. [Google Scholar] [CrossRef] [PubMed]
- Engoren, M.; Mitchell, E.; Perring, P.; Sferra, J. The effect of erythrocyte blood transfusions on survival after surgery for hip fracture. J. Trauma Acute Care Surg. 2008, 65, 1411–1415. [Google Scholar] [CrossRef]
- Arshi, A.; Lai, W.C.; Iglesias, B.C.; McPherson, E.J.; Zeegen, E.N.; Stavrakis, A.I.; Sassoon, A.A. Blood transfusion rates and predictors following geriatric hip fracture surgery. Hip Int. 2021, 31, 272–279. [Google Scholar] [CrossRef]
- Khatib, Y.; Bal, G.; Liu, R.; Ashaia, W.; Sorial, R. A randomised controlled trial assessing the effect of tranexamic acid on post-operative blood transfusions in patient with intra-capsular hip fractures treated with hemi-or total hip arthroplasty. Arch. Orthop. Trauma Surg. 2024, 144, 3095–3102. [Google Scholar] [CrossRef]
- Gregersen, M.; Borris, L.C.; Damsgaard, E.M. Postoperative blood transfusion strategy in frail, anemic elderly patients with hip fracture: The TRIFE randomized controlled trial. Acta Orthop. 2015, 86, 363–372. [Google Scholar] [CrossRef]
- Hung, K.-C.; Chang, L.-C.; Ho, C.-N.; Hsu, C.-W.; Yu, C.-H.; Wu, J.-Y.; Lin, C.-M.; Chen, I.-W. Efficacy of intravenous iron supplementation in reducing transfusion risk following cardiac surgery: An updated meta-analysis of randomised controlled trials. Br. J. Anaesth. 2024, 133, 1137–1149. [Google Scholar] [CrossRef] [PubMed]
- Froessler, B.; Palm, P.; Weber, I.; Hodyl, N.A.; Singh, R.; Murphy, E.M. The important role for intravenous iron in perioperative patient blood management in major abdominal surgery: A randomized controlled trial. Ann. Surg. 2016, 264, 41–46. [Google Scholar] [CrossRef]
- Kulnigg, S.; Stoinov, S.; Simanenkov, V.; Dudar, L.V.; Karnafel, W.; Garcia, L.C.; Sambuelli, A.M.; D’haens, G.; Gasche, C. A novel intravenous iron formulation for treatment of anemia in inflammatory bowel disease: The ferric carboxymaltose (FERINJECT®) randomized controlled trial. Off. J. Am. Coll. Gastroenterol.|ACG 2008, 103, 1182–1192. [Google Scholar] [CrossRef] [PubMed]
- Van Wyck, D.B.; Martens, M.G.; Seid, M.H.; Baker, J.B.; Mangione, A. Intravenous ferric carboxymaltose compared with oral iron in the treatment of postpartum anemia: A randomized controlled trial. Obstet. Gynecol. 2007, 110 Pt 1, 267–278. [Google Scholar] [CrossRef]
- Camaschella, C. Iron-deficiency anemia. N. Engl. J. Med. 2015, 372, 1832–1843. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.-H.; Lee, B.S.; Won, H.; Kim, H.-K.; Lee, Y.-K.; Koo, K.-H. Preoperative iron supplementation and restrictive transfusion strategy in hip fracture surgery. Clin. Orthop. Surg. 2019, 11, 265. [Google Scholar] [CrossRef]
- Cuenca, J.; García-Erce, J.A.; Martínez, A.A.; Solano, V.M.; Molina, J.; Munoz, M. Role of parenteral iron in the management of anaemia in the elderly patient undergoing displaced subcapital hip fracture repair: Preliminary data. Arch. Orthop. Trauma Surg. 2005, 125, 342–347. [Google Scholar] [CrossRef]
- Carson, J.L.; Stanworth, S.J.; Guyatt, G.; Valentine, S.; Dennis, J.; Bakhtary, S.; Cohn, C.S.; Dubon, A.; Grossman, B.J.; Gupta, G.K. Red blood cell transfusion: 2023 AABB international guidelines. JAMA 2023, 330, 1892–1902. [Google Scholar] [CrossRef]
- Horvath, B.; Kloesel, B.; Todd, M.M.; Cole, D.J.; Prielipp, R.C. The evolution, current value, and future of the American Society of Anesthesiologists Physical Status Classification System. Anesthesiology 2021, 135, 904–919. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Miralles-Muñoz, F.A.; Perez-Aznar, A.; Gonzalez-Parreño, S.; Sebastia-Forcada, E.; Mahiques-Segura, G.; Lizaur-Utrilla, A.; Vizcaya-Moreno, M.F. Change in 1-year mortality after hip fracture surgery over the last decade in a European population. Arch. Orthop. Trauma Surg. 2023, 143, 4173–4179. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Jang, E.J.; Jo, J.; Jo, J.G.; Nam, S.; Kim, H.; Lee, H.; Ryu, H.G. The association between hospital case volume and in-hospital and one-year mortality after hip fracture surgery: A population-based retrospective cohort study. Bone Jt. J. 2020, 102, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Huette, P.; Abou-Arab, O.; Djebara, A.-E.; Terrasi, B.; Beyls, C.; Guinot, P.-G.; Havet, E.; Dupont, H.; Lorne, E.; Ntouba, A. Risk factors and mortality of patients undergoing hip fracture surgery: A one-year follow-up study. Sci. Rep. 2020, 10, 9607. [Google Scholar] [CrossRef]
- Bernabeu-Wittel, M.; Romero, M.; Ollero-Baturone, M.; Aparicio, R.; Murcia-Zaragoza, J.; Rincón-Gómez, M.; Monte-Secades, R.; Melero-Bascones, M.; Rosso, C.M.; Ruiz-Cantero, A.; et al. Ferric carboxymaltose with or without erythropoietin in anemic patients with hip fracture: A randomized clinical trial. Transfusion 2016, 56, 2199–2211. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, M.; Gómez-Ramírez, S.; Cuenca, J.; García-Erce, J.A.; Iglesias-Aparicio, D.; Haman-Alcober, S.; Ariza, D.; Naveira, E. Very-short-term perioperative intravenous iron administration and postoperative outcome in major orthopedic surgery: A pooled analysis of observational data from 2547 patients. Transfusion 2014, 54, 289–299. [Google Scholar] [CrossRef]
- Spahn, D.R. Anemia and patient blood management in hip and knee surgery: A systematic review of the literature. Anesthesiology 2010, 113, 482–495. [Google Scholar] [CrossRef]
- Qunibi, W.Y.; Martinez, C.; Smith, M.; Benjamin, J.; Mangione, A.; Roger, S.D. A randomized controlled trial comparing intravenous ferric carboxymaltose with oral iron for treatment of iron deficiency anaemia of non-dialysis-dependent chronic kidney disease patients. Nephrol. Dial. Transplant. 2011, 26, 1599–1607. [Google Scholar] [CrossRef]
- Avni, T.; Bieber, A.; Grossman, A.; Green, H.; Leibovici, L.; Gafter-Gvili, A. The safety of intravenous iron preparations: Systematic review and meta-analysis. Mayo Clin. Proc. 2015, 90, 12–23. [Google Scholar] [CrossRef]
- Muñoz, M.; Gómez-Ramírez, S.; Auerbach, M. Stimulating erythropoiesis before hip fracture repair for reducing blood transfusion: Should we change the hemoglobin cutoff level for defining anemia in females? Transfusion 2016, 56, 2160–2163. [Google Scholar] [CrossRef]
- Richards, T.; Wijaya, L.K.; Lim, J.; Dugan, C.; Dahly, D. Intravenous Iron–Induced Hypophosphatemia in Surgical Patients. JAMA Netw. Open 2025, 8, e253093. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | FCM Group | Control Group | p Values | |
|---|---|---|---|---|
| Number of patients | n | 109 | 105 | |
| Age (years) | Mean ± SD Median (IQR) | 78.19 ± 10.79 80.0 (71.0–87.0) | 78.91 ± 9.20 79.0 (74.0–88.0) | 0.98 |
| Gender | (n, %) | |||
| Female | 65 (60%) | 68 (65%) | 0.44 | |
| Male | 44 (40%) | 37 (35%) | ||
| BMI (kg/m2) | 29.5 (±2.3) 29 (28.0–31.0) | 28.8 (±3.1) 28.5 (26.5–31.0) | 0.19 | |
| ASA grade | (n, %) | |||
| I | 8 | 6 | 0.290 | |
| II | 45 | 43 | ||
| III | 50 | 51 | ||
| IV | 6 | 5 | ||
| Fracture location | (n, %) | |||
| Femoral neck fracture | 39 (36%) | 38 (36%) | 0.53 | |
| Intertrochanteric fracture | 70 (64%) | 67 (64%) | ||
| Surgery | (n, %) | |||
| Hemiarthroplasty | 35 (32.1%) | 31 (29.5%) | 0.658 | |
| Total hip arthroplasty | 6 (5.5%) | 9 (8.6%) | ||
| Intramedullary nail | 68 (62.4%) | 65 (61.9%) | ||
| Preoperative hemoglobin level (g/dL) | Mean ± SD Median (IQR) | 10.78 ± 1.74 10.85 (9.6–12.0) | 10.47 ± 1.96 10.55 (9.2–11.7) | 0.955 |
| Preoperative anemia | (n, %) | 88 (81%) | 86 (82%) | 0.826 |
| Preoperative phosphate level (mg/dL) | Mean ± SD Median (IQR) | 3.51 ± 0.73 3.47 (2.93–3.96) | 3.27 ± 0.78 3.21 (2.82–3.75) | 0.023 |
| Preoperative hypophosphatemia | (n, %) | 19 (17%) | 26 (25%) | 0.188 |
| Comorbidities | FCM Group (n = 109) | Control Group (n = 105) | p Values |
|---|---|---|---|
| Number of comorbidities | |||
| 0–1 | 32 (29%) | 31 (30%) | 0.979 |
| ≥2 | 77 (71%) | 74 (70%) | |
| Renal dysfunction | 11 (10%) | 12 (11%) | 0.752 |
| Hypertension | 78 (72%) | 71 (68%) | 0.531 |
| Cardiac disease a | 36 (33%) | 32 (31%) | 0.689 |
| Diabetes Mellitus | 33 (30%) | 35 (33%) | 0.631 |
| Thyroid dysfunction | 12 (11%) | 13 (12%) | 0.910 |
| COPD | 20 (19%) | 13 (12%) | 0.149 |
| Neurological disorders b | 17 (16%) | 13 (12%) | 0.498 |
| Dementia | 7 (7%) | 19 (17%) | 0.016 |
| Malignancy | 10 (9%) | 6 (6%) | 0.336 |
| CCI, Mean ± SD Median (IQR) | 4.81 ± 1.68 5 (2–4) | 4.58 ± 1.52 4 (1–2) | 0.326 |
| Variables | FCM Group (n = 109) | Control Group (n = 105) | p Values | |
|---|---|---|---|---|
| Primary Outcomes | ||||
| 6-month mortality rate | n (%) | 25 (23%) | 41 (39%) | 0.011 |
| 1-year mortality rate | 31 (28%) | 45 (43%) | 0.028 | |
| Secondary Outcomes | ||||
| Anemia rates | ||||
| Preoperative | n (%) | 88 (81%) | 86 (82%) | 0.826 |
| Postoperative | 107 (98%) | 101 (96%) | 0.382 | |
| At discharge | 106 (97%) | 99 (94%) | 0.281 | |
| At 6th week | 86 (89%) | 89 (98%) | 0.029 | |
| Hemoglobin levels (g/dL) | ||||
| Preoperative | Mean ± SD Median (IQR) | 10.76 ± 1.74 10.8 [9.7–12.3] | 10.46 ± 1.96 10.5 [9.2–11.7] | 0.427 |
| Postoperative | 9.70 ± 1.35 9.6 [9.0–10.8] | 9.91 ± 1.20 9.9 [9.0–10.6] | 0.159 | |
| At discharge | 9.78 ± 1.03 9.7 [7.3–12.4] | 10.29 ± 1.01 10.2 [9.6–11.4] | 0.001 | |
| At 6th week | 11.57 ± 1.16 10.4 [9.4–11.0] | 10.30 ± 0.91 10.3 [9.9–10.9] | 0.242 | |
| Perioperative transfusion characteristics | ||||
| Transfused patients (ES replacement) | n (%) | 34 (30%) | 48 (46%) | 0.013 |
| 1–2 units | 33 (97%) | 45 (94%) | ||
| ≥3 units | 1 (3%) | 3 (6%) | ||
| Length of hospitalization (days) | Mean ± SD Median (IQR) | 12.19 ± 9.58 10 [6–10] | 15.14 ± 12.7 11 [7–14] | 0.250 |
| Phosphate level at discharge (mg/dL) | 3.42 ± 1 3.41 [2.79–4.05] | 3.14 ± 0.79 3.06 [2.6–3.64] | 0.029 | |
| Change in phosphate levels at discharge (mg/dL) | 0.10 ± 0.99 0.12 [0.71–(−0.58)] | 0.13 ± 0.87 0.19 [0.69–(−0.48)] | 0.776 | |
| Hypophosphatemia at discharge | n (%) | 27 (25%) | 38 (36%) | 0.069 |
| Variable Included in Step 12 | OR (Exp(B)) | 95% CI | p Values |
|---|---|---|---|
| Preoperative IV FCM administration (Received vs. Not received) | 0.330 | 0.158–0.690 | 0.003 |
| Age (per year increase) | 1.062 | 1.017–1.109 | 0.006 |
| Gender (female vs. male) | 0.424 | 0.188–0.956 | 0.038 |
| Fracture type (femoral neck vs. intertrochanteric) | 0.388 | 0.179–0.843 | 0.017 |
| CCI score (per point) | 1.398 | 1.070–1.827 | 0.014 |
| ASA class (high vs. low) | 2.309 | 1.063–5.016 | 0.035 |
| Hypertension (Present vs. Absent) | 6.446 | 2.004–20.735 | 0.002 |
| Neurologic disorders (Present vs. Absent) | 1.292 | 1.092–1.926 | 0.037 |
| Surgery: THA vs. Hemiarthroplasty | 0.203 | 0.023–1.785 | 0.150 |
| Surgery: IMN vs. Hemiarthroplasty | 1.257 | 0.448–3.526 | 0.659 |
| ES transfusion (Received vs. Not received) | 2.074 | 0.988–4.355 | 0.054 |
| Variable Included in Step 13 | OR (Exp(B)) | 95% CI | p Values |
|---|---|---|---|
| Preoperative IV FCM administration (Received vs. Not received) | 0.449 | 0.227–0.887 | 0.021 |
| Age (per year increase) | 1.059 | 1.020–1.100 | 0.003 |
| Gender (female vs. male) | 0.445 | 0.233–0.849 | 0.015 |
| CCI score (per point) | 1.248 | 1.036–1.504 | 0.019 |
| ASA class (high vs. low) | 2.309 | 1.063–5.016 | 0.035 |
| Hypertension (Present vs. Absent) | 3.583 | 1.676–7.656 | 0.001 |
| Neurologic disorders (Present vs. Absent) | 3.266 | 1.230–8.673 | 0.018 |
| ES transfusion (Received vs. Not received) | 1.995 | 0.938–4.243 | 0.070 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kizilkurt, T.; Ozkaya, M.; Balli, M.; Demirel, M.; Asik, M. The Effect of Preoperative Intravenous Iron Supplementation on Mortality and Blood Transfusion Requirements in Elderly Patients Undergoing Hip Fracture Surgery: A Prospective Randomized Controlled Trial. J. Clin. Med. 2025, 14, 4713. https://doi.org/10.3390/jcm14134713
Kizilkurt T, Ozkaya M, Balli M, Demirel M, Asik M. The Effect of Preoperative Intravenous Iron Supplementation on Mortality and Blood Transfusion Requirements in Elderly Patients Undergoing Hip Fracture Surgery: A Prospective Randomized Controlled Trial. Journal of Clinical Medicine. 2025; 14(13):4713. https://doi.org/10.3390/jcm14134713
Chicago/Turabian StyleKizilkurt, Taha, Mustafa Ozkaya, Mert Balli, Mehmet Demirel, and Mehmet Asik. 2025. "The Effect of Preoperative Intravenous Iron Supplementation on Mortality and Blood Transfusion Requirements in Elderly Patients Undergoing Hip Fracture Surgery: A Prospective Randomized Controlled Trial" Journal of Clinical Medicine 14, no. 13: 4713. https://doi.org/10.3390/jcm14134713
APA StyleKizilkurt, T., Ozkaya, M., Balli, M., Demirel, M., & Asik, M. (2025). The Effect of Preoperative Intravenous Iron Supplementation on Mortality and Blood Transfusion Requirements in Elderly Patients Undergoing Hip Fracture Surgery: A Prospective Randomized Controlled Trial. Journal of Clinical Medicine, 14(13), 4713. https://doi.org/10.3390/jcm14134713