
Drug-Eluting Stent Use in Percutaneous Coronary Interventions—A Narrative Review


Abstract
1. Introduction
1.1. Objectives of the Review
1.2. Methodology
1.3. Coronary Artery Disease
1.4. Percutaneous Coronary Intervention
1.5. Evolution of Stents
2. Stent Structure
2.1. Metallic Platform
2.2. Polymers
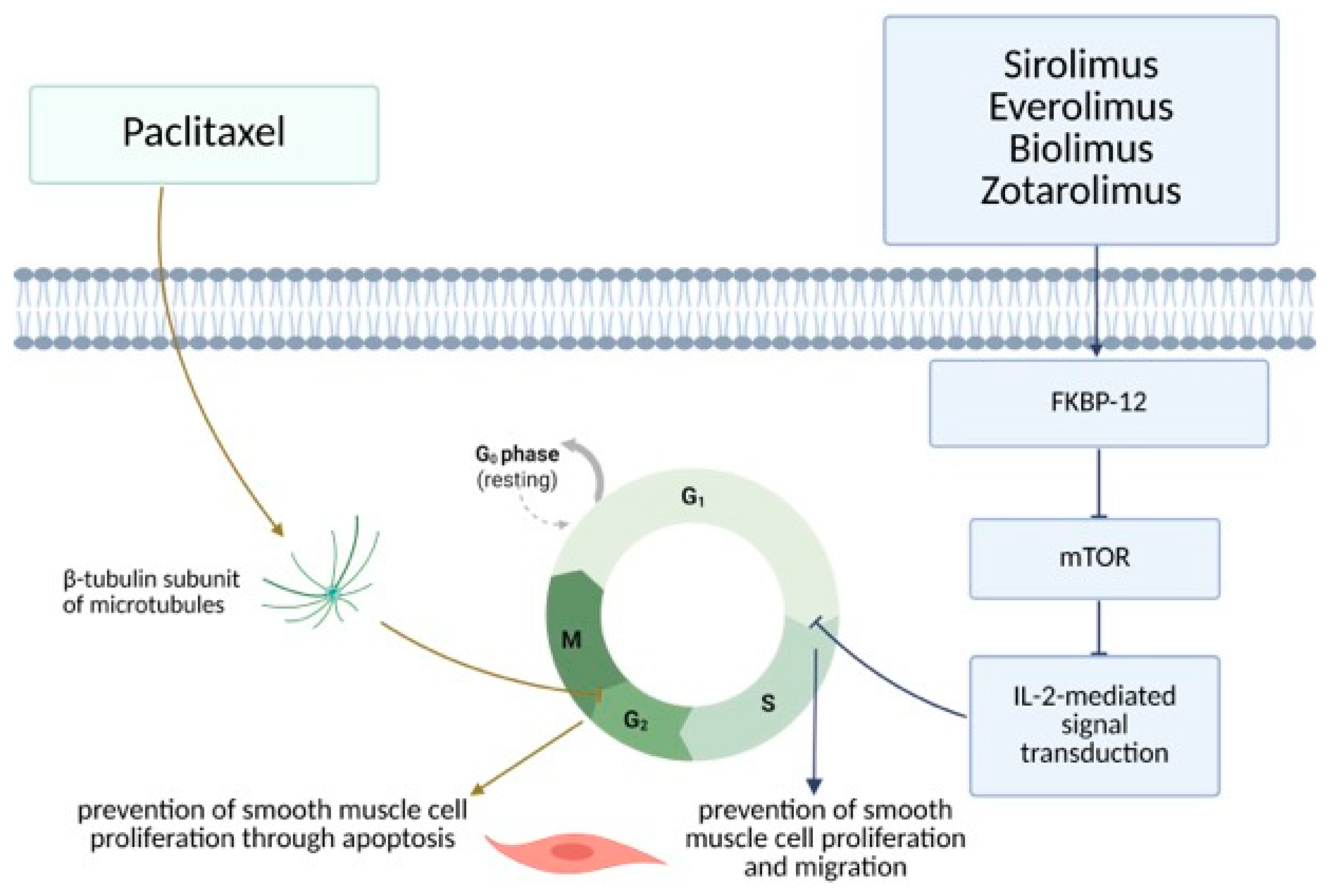
2.3. Anti-Proliferative Agents
Mechanism of Action
3. Drug-Eluting Stent Comparison
3.1. Stent Platform Comparison
3.2. Polymer Comparison
3.3. Anti-Proliferative Drug Comparison
3.3.1. Biolimus- Versus Everolimus-Eluting Stents
3.3.2. Biolimus- Versus Sirolimus-Eluting Stents
3.3.3. Biolimus- Versus Zotarolimus-Eluting Stents
3.3.4. Everolimus- Versus Sirolimus-Eluting Stents
3.3.5. Everolimus Versus Zotarolimus-Eluting Stents
3.3.6. Sirolimus- Versus Zotarolimus-Eluting Stents
4. Gene-Eluting Stents
5. Ongoing Development and Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CAD | Coronary artery disease |
| ACS | Acute coronary syndrome |
| NSTEMI | Non-ST elevation myocardial infarction |
| STEMI | Myocardial infarction with ST elevation |
| PCI | Percutaneous coronary intervention |
| CABG | Coronary artery bypass grafting |
| POBA | Plain old balloon angioplasty |
| BMS | Bare metal stent |
| ISR | In-stent restenosis |
| DES | Drug-eluting stent |
| ST | Stent thrombosis |
| mTOR | Mammalian target of rapamycin |
| DNA | Deoxyribonucleic acid |
| DCB | Drug-coated balloon |
| BRS | Bioresorbable scaffold system |
| GES | Gene-eluting stent |
| BVS | Bioabsorbable vascular stent |
References
- Ralapanawa, U.; Sivakanesan, R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J. Epidemiol. Glob. Health 2021, 11, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Bottardi, A.; Prado, G.F.A.; Lunardi, M.; Fezzi, S.; Pesarini, G.; Tavella, D.; Scarsini, R.; Ribichini, F. Clinical Updates in Coronary Artery Disease: A Comprehensive Review. J. Clin. Med. 2024, 13, 4600. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the Management of Acute Coronary Syndromes: Developed by the Task Force on the Management of Acute Coronary Syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al. 2024 ESC Guidelines for the Management of Chronic Coronary Syndromes: Developed by the Task Force for the Management of Chronic Coronary Syndromes of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2024, 45, 3415–3537. [Google Scholar] [CrossRef]
- Iqbal, J.; Gunn, J.; Serruys, P.W. Coronary Stents: Historical Development, Current Status and Future Directions. Br. Med. Bull. 2013, 106, 193–211. [Google Scholar] [CrossRef]
- Chhabra, L.; Zain, M.A.; Siddiqui, W.J. Coronary Stents. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Htay, T.; Liu, M.W. Drug-Eluting Stent: A Review and Update. Vasc. Health Risk Manag. 2005, 1, 263–276. [Google Scholar] [CrossRef]
- Goh, D.; Tan, A.; Farhatnia, Y.; Rajadas, J.; Alavijeh, M.S.; Seifalian, A.M. Nanotechnology-Based Gene-Eluting Stents. Mol. Pharm. 2013, 10, 1279–1298. [Google Scholar] [CrossRef]
- Parker, W.; Iqbal, J. Comparison of Contemporary Drug-Eluting Coronary Stents—Is Any Stent Better than the Others? Heart Int. 2020, 14, 34–42. [Google Scholar] [CrossRef]
- Eccleston, D.S.; Chowdhury, E.; Rafter, T.; Sage, P.; Whelan, A.; Reid, C.; Liew, D.; Duong, M.; Schwarz, N.; Worthley, S.G. Long-Term Outcomes of Contemporary Percutaneous Coronary Intervention with the Xience Drug-Eluting Stent: Results from a Multicentre Australian Registry. J. Clin. Med. 2022, 12, 280. [Google Scholar] [CrossRef] [PubMed]
- Philip, F.; Stewart, S.; Southard, J.A. Very Late Stent Thrombosis with Second Generation Drug Eluting Stents Compared to Bare Metal Stents: Network Meta-Analysis of Randomized Primary Percutaneous Coronary Intervention Trials. Catheter. Cardiovasc. Interv. 2016, 88, 38–48. [Google Scholar] [CrossRef]
- Farshidi, H.; Abdi, A.; Madani, A.; Moshiri, S.; Ghasemi, A.; Hakimian, R. Major Adverse Cardiovascular Event (MACE) after Percutaneous Coronary Intervention in One-Year Follow-up Study. Electron. Physician 2018, 10, 6383–6389. [Google Scholar] [CrossRef] [PubMed]
- Hannan, E.L.; Racz, M.; Walford, G.; Holmes, D.R.; Jones, R.H.; Sharma, S.; Katz, S.; King, S.B. Drug-Eluting versus Bare-Metal Stents in the Treatment of Patients with ST-Segment Elevation Myocardial Infarction. JACC Cardiovasc. Interv. 2008, 1, 129–135. [Google Scholar] [CrossRef]
- Hannan, E.L.; Samadashvili, Z.; Walford, G.; Holmes, D.R.; Jacobs, A.K.; Stamato, N.J.; Venditti, F.J.; Sharma, S.; Fergus, I.; King, S.B. Comparison of Outcomes for Patients Receiving Drug-Eluting versus Bare Metal Stents for Non-ST-Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2011, 107, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Changal, K.H.; Mir, T.; Khan, S.; Nazir, S.; Elzanatey, A.; Meenakshisundaram, C.; Mubbasher, S.; Sheikh, M.A. Drug-Eluting Stents Versus Bare-Metal Stents in Large Coronary Artery Revascularization: Systematic Review and Meta-Analysis. Cardiovasc. Revasc Med. 2021, 23, 42–49. [Google Scholar] [CrossRef]
- Eftekhari, A.; Christiansen, E.H.; Lassen, J.F.; Raungaard, B.; Jakobsen, L.; Jensen, L.O. Randomized Comparison of the Combined Sirolimus Eluting and Endothelial Progenitor Cell Combo Stent vs. Biolimus Eluting Absorbable Polymer Coated Biomatrix Alpha Stent in Patients Undergoing Percutaneous Coronary Intervention: Rationale and Study Design of the Scandinavian Organization for Randomized Trials with Clinical Outcome (SORT OUT) XI Trial. Am. Heart J. 2025, 283, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Bravo Baptista, S. The third generation of drug-eluting stents: Reassuring data while we wait for the next one. Rev. Port. Cardiol. 2021, 40, 77–80. [Google Scholar] [CrossRef]
- Ma, W.-R.; Chandrasekharan, K.H.; Nai, C.-S.; Zhu, Y.-X.; Iqbal, J.; Chang, S.; Cheng, Y.-W.; Wang, X.-Y.; Bourantas, C.V.; Zhang, Y.-J. Clinical Outcomes of Percutaneous Coronary Intervention for de Novo Lesions in Small Coronary Arteries: A Systematic Review and Network Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 1017833. [Google Scholar] [CrossRef]
- Mutema, M.; Shenoy, V.; Sardar, P.; Parikh, S.; Chatterjee, S. Systematic Review on Role of Drug Eluting Stent (DES) Versus Drug-Coated Balloon (DCB) in Small Vessel Coronary Artery Disease. Curr. Cardiol. Rep. 2024, 26, 681–688. [Google Scholar] [CrossRef]
- Megaly, M.; Buda, K.; Saad, M.; Tawadros, M.; Elbadawi, A.; Basir, M.; Abbott, J.D.; Rinfret, S.; Alaswad, K.; Brilakis, E.S. Outcomes With Drug-Coated Balloons vs. Drug-Eluting Stents in Small-Vessel Coronary Artery Disease. Cardiovasc. Revasc Med. 2022, 35, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.-L.; Huang, Q.-J.; Chen, M.-H. Efficacy and Safety of Drug-Coated Balloon for de Novo Lesions of Large Coronary Arteries: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Heliyon 2024, 10, e25264. [Google Scholar] [CrossRef]
- Abdelaziz, A.; Hafez, A.; Atta, K.; Elsayed, H.; Abdelaziz, M.; Elaraby, A.; Kadhim, H.; Mechi, A.; Ezzat, M.; Fadel, A.; et al. Drug-Coated Balloons versus Drug-Eluting Stents in Patients with Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention: An Updated Meta-Analysis with Trial Sequential Analysis. BMC Cardiovasc. Disord. 2023, 23, 605. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Wang, D.-Y.; Deng, W.-Q.; Lai, S.-J.; Wang, X. Bioresorbable Scaffolds vs. Drug-Eluting Stents on Short- and Mid-Term Target Lesion Outcomes in Patients after PCI: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 949494. [Google Scholar] [CrossRef]
- Popma, J.J.; Mauri, L.; O’Shaughnessy, C.; Overlie, P.; McLaurin, B.; Almonacid, A.; Kirtane, A.; Leon, M.B. Frequency and Clinical Consequences Associated With Sidebranch Occlusion During Stent Implantation Using Zotarolimus-Eluting and Paclitaxel-Eluting Coronary Stents. Circ. Cardiovasc. Interv. 2009, 2, 133–139. [Google Scholar] [CrossRef]
- Yasmin, F.; Zaidi, S.F.; Moeed, A.; Khan, M.; Ali, E.; Asghar, M.S.; Ullah, W.; Savage, M.P.; Vishnevsky, A.; Ruggiero, N.J.; et al. Long-Term Outcomes Following Ultrathin vs. Thin-Strut Drug-Eluting Stents for Percutaneous Coronary Intervention: An Updated Systematic Review and Meta-Analysis of Randomized Control Trials. Am. J. Cardiovasc. Dis. 2024, 14, 267–280. [Google Scholar] [CrossRef]
- Velagapudi, C.; Madassery, S. Drug-Eluting Stents. Semin. Intervent Radiol. 2022, 39, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Tataru, D.-A.; Lazar, F.-L.; Onea, H.-L.; Homorodean, C.; Ober, M.-C.; Olinic, M.; Spinu, M.; Olinic, D.-M. Benefits and Challenges of Drug-Coated Balloons in Peripheral Artery Disease: From Molecular Mechanisms to Clinical Practice. Int. J. Mol. Sci. 2024, 25, 8749. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Park, S. Local Delivery of Antiproliferative Agents via Stents. Polymers 2014, 6, 755–775. [Google Scholar] [CrossRef]
- Grube, E.; Buellesfeld, L. Current Clinical Experience and Future Directions. In Endovascular Today; Publishing Bryn Mawr Communications II, LLC: Conshohocken, PA, USA, 2004. [Google Scholar]
- Moreno, R. Drug-Eluting Stents and Other Anti-Restenosis Devices. Rev. Española Cardiol. (Engl. Ed.) 2005, 58, 842–862. [Google Scholar] [CrossRef]
- Jensen, L.; Maeng, M.; Raungaard, B.; Hansen, K.; Kahlert, J.; Jensen, S.; Hansen, H.; Lassen, J.; Bøtker, H.; Christiansen, E. Two-Year Outcome after Biodegradable Polymer Sirolimus- and Biolimus-Eluting Coronary Stents (from the Randomised SORT OUT VII Trial). EuroIntervention 2018, 13, 1587–1590. [Google Scholar] [CrossRef]
- Ge, J. Limus-Eluting Stents with Poly-L-Lactic Acid Coating. Asia-Pac. Cardiol. 2007, 1, 42–43. [Google Scholar] [CrossRef]
- Vlachojannis, G.; Puricel, S.; Natsuaki, M.; Morimoto, T.; Smits, P.; Kimura, T. Biolimus-Eluting versus Everolimus-Eluting Stents in Coronary Artery Disease: A Pooled Analysis from the NEXT (NOBORI Biolimus-Eluting versus XIENCE/PROMUS Everolimus-Eluting Stent) and COMPARE II (Abluminal Biodegradable Polymer Biolimus-Eluting Stent versus Durable Polymer Everolimus-Eluting Stent) Randomised Trials. EuroIntervention 2017, 12, 1970–1977. [Google Scholar] [CrossRef]
- Mehta, A.B.; Chandra, P.; Dalal, J.; Shetty, P.; Desai, D.; Chocklingam, K.; Prajapati, J.; Kumar, P.; Magarkar, V.; Vasawada, A.; et al. One-Year Clinical Outcomes of BioMatrixTM-Biolimus A9TM Eluting Stent: The e-BioMatrix Multicenter Post Marketing Surveillance Registry in India. Indian. Heart J. 2013, 65, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Ostojic, M.; Sagic, D.; Jung, R.; Zhang, Y.-L.; Nedeljkovic, M.; Mangovski, L.; Stojkovic, S.; Debeljacki, D.; Colic, M.; Beleslin, B.; et al. The Pharmacokinetics of Biolimus A9 after Elution from the Nobori Stent in Patients with Coronary Artery Disease: The NOBORI PK Study. Catheter. Cardiovasc. Interv. 2008, 72, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, Y.; Matsuo, K.; Ueda, Y.; Sugihara, R.; Hirata, A.; Murakami, A.; Kashiwase, K.; Higuchi, Y.; Yasumura, Y. Angioscopic Comparison of Resolute and Endeavor Zotarolimus-Eluting Stents. Circ. J. 2016, 80, 650–656. [Google Scholar] [CrossRef]
- Iqbal, J.; Serruys, P.W.; Silber, S.; Kelbaek, H.; Richardt, G.; Morel, M.-A.; Negoita, M.; Buszman, P.E.; Windecker, S. Comparison of Zotarolimus- and Everolimus-Eluting Coronary Stents: Final 5-Year Report of the RESOLUTE All-Comers Trial. Circ. Cardiovasc. Interv. 2015, 8, e002230. [Google Scholar] [CrossRef]
- Kang, D.-Y.; Jang, J.-S.; Chang, M.; Lee, C.H.; Lee, P.H.; Ahn, J.-M.; Lee, S.-W.; Kim, Y.-H.; Park, S.-W.; Park, D.-W.; et al. Comparison of Different Types of Drug-Eluting Stents for De Novo Long Coronary Artery Lesions. JACC Asia 2022, 2, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.J.; Hyun, J.; Lee, J.; Kim, J.H.; Yang, Y.; Choe, K.; Lee, J.S.; Park, H.; Cho, S.-C.; Kang, D.-Y.; et al. Comparison of Contemporary Drug-Eluting Stents in Patients Undergoing Complex High-Risk Indicated Procedures. JACC Asia 2022, 2, 182–193. [Google Scholar] [CrossRef]
- Yang, Y.; Hyun, J.; Lee, J.; Kim, J.H.; Lee, J.B.; Kang, D.-Y.; Lee, P.H.; Ahn, J.-M.; Park, D.-W.; Park, S.-J. Effectiveness and Safety of Contemporary Drug-Eluting Stents in Patients With Diabetes Mellitus. JACC Asia 2021, 1, 173–184. [Google Scholar] [CrossRef]
- Lee, M.S.; Mahmud, E.; Ang, L.; Lluri, G.; Cheng, R.K.; Aragon, J.; Sheiban, I. Comparison of Sirolimus-, Paclitaxel-, and Everolimus-Eluting Stent in Unprotected Left Main Coronary Artery Percutaneous Coronary Intervention. J. Saudi Heart Assoc. 2013, 25, 75–78. [Google Scholar] [CrossRef]
- Smits, P.C.; Hofma, S.; Togni, M.; Vázquez, N.; Valdés, M.; Voudris, V.; Slagboom, T.; Goy, J.-J.; Vuillomenet, A.; Serra, A.; et al. Abluminal Biodegradable Polymer Biolimus-Eluting Stent versus Durable Polymer Everolimus-Eluting Stent (COMPARE II): A Randomised, Controlled, Non-Inferiority Trial. Lancet 2013, 381, 651–660. [Google Scholar] [CrossRef]
- Natsuaki, M.; Kozuma, K.; Morimoto, T.; Kadota, K.; Muramatsu, T.; Nakagawa, Y.; Akasaka, T.; Igarashi, K.; Tanabe, K.; Morino, Y.; et al. Biodegradable Polymer Biolimus-Eluting Stent versus Durable Polymer Everolimus-Eluting Stent: A Randomized, Controlled, Noninferiority Trial. J. Am. Coll. Cardiol. 2013, 62, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Natsuaki, M.; Kozuma, K.; Morimoto, T.; Kadota, K.; Muramatsu, T.; Nakagawa, Y.; Akasaka, T.; Hanaoka, K.I.; Tanabe, K.; Morino, Y.; et al. Five-Year Outcome of a Randomised Trial Comparing Second-Generation Drug-Eluting Stents Using Either Biodegradable Polymer or Durable Polymer: The NOBORI Biolimus-Eluting versus XIENCE/PROMUS Everolimus-Eluting Stent Trial (NEXT). EuroIntervention 2018, 14, 815–818. [Google Scholar] [CrossRef] [PubMed]
- Puricel, S.; Arroyo, D.; Corpataux, N.; Baeriswyl, G.; Lehmann, S.; Kallinikou, Z.; Muller, O.; Allard, L.; Stauffer, J.-C.; Togni, M.; et al. Comparison of Everolimus- and Biolimus-Eluting Coronary Stents with Everolimus-Eluting Bioresorbable Vascular Scaffolds. J. Am. Coll. Cardiol. 2015, 65, 791–801. [Google Scholar] [CrossRef]
- Stone, G.W.; Teirstein, P.S.; Meredith, I.T.; Farah, B.; Dubois, C.L.; Feldman, R.L.; Dens, J.; Hagiwara, N.; Allocco, D.J.; Dawkins, K.D.; et al. A Prospective, Randomized Evaluation of a Novel Everolimus-Eluting Coronary Stent: The PLATINUM (a Prospective, Randomized, Multicenter Trial to Assess an Everolimus-Eluting Coronary Stent System [PROMUS Element] for the Treatment of Up to Two de Novo Coronary Artery Lesions) Trial. J. Am. Coll. Cardiol. 2011, 57, 1700–1708. [Google Scholar] [CrossRef]
- Fajadet, J.; Neumann, F.-J.; Hildick-Smith, D.; Petronio, S.; Zaman, A.; Spence, M.; Wöhrle, J.; Elhadad, S.; Roberts, D.; Hovasse, T.; et al. Twelve-Month Results of a Prospective, Multicentre Trial to Assess the Everolimus-Eluting Coronary Stent System (PROMUS Element): The PLATINUM PLUS All-Comers Randomised Trial. EuroIntervention 2017, 12, 1595–1604. [Google Scholar] [CrossRef] [PubMed]
- Iantorno, M.; Lipinski, M.J.; Garcia-Garcia, H.M.; Forrestal, B.J.; Rogers, T.; Gajanana, D.; Buchanan, K.D.; Torguson, R.; Weintraub, W.S.; Waksman, R. Meta-Analysis of the Impact of Strut Thickness on Outcomes in Patients With Drug-Eluting Stents in a Coronary Artery. Am. J. Cardiol. 2018, 122, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Bangalore, S.; Toklu, B.; Patel, N.; Feit, F.; Stone, G.W. Newer-Generation Ultrathin Strut Drug-Eluting Stents Versus Older Second-Generation Thicker Strut Drug-Eluting Stents for Coronary Artery Disease. Circulation 2018, 138, 2216–2226. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Mauri, L.; Koolen, J.J.; Massaro, J.M.; Doros, G.; Garcia-Garcia, H.M.; Bennett, J.; Roguin, A.; Gharib, E.G.; Cutlip, D.E.; et al. Ultrathin, Bioresorbable Polymer Sirolimus-Eluting Stents versus Thin, Durable Polymer Everolimus-Eluting Stents in Patients Undergoing Coronary Revascularisation (BIOFLOW V): A Randomised Trial. Lancet 2017, 390, 1843–1852. [Google Scholar] [CrossRef]
- von Birgelen, C.; Zocca, P.; Buiten, R.A.; Jessurun, G.A.J.; Schotborgh, C.E.; Roguin, A.; Danse, P.W.; Benit, E.; Aminian, A.; van Houwelingen, K.G.; et al. Thin Composite Wire Strut, Durable Polymer-Coated (Resolute Onyx) versus Ultrathin Cobalt-Chromium Strut, Bioresorbable Polymer-Coated (Orsiro) Drug-Eluting Stents in Allcomers with Coronary Artery Disease (BIONYX): An International, Single-Blind, Randomised Non-Inferiority Trial. Lancet 2018, 392, 1235–1245. [Google Scholar] [CrossRef]
- von Birgelen, C.; Kok, M.M.; van der Heijden, L.C.; Danse, P.W.; Schotborgh, C.E.; Scholte, M.; Gin, R.M.T.J.; Somi, S.; van Houwelingen, K.G.; Stoel, M.G.; et al. Very Thin Strut Biodegradable Polymer Everolimus-Eluting and Sirolimus-Eluting Stents versus Durable Polymer Zotarolimus-Eluting Stents in Allcomers with Coronary Artery Disease (BIO-RESORT): A Three-Arm, Randomised, Non-Inferiority Trial. Lancet 2016, 388, 2607–2617. [Google Scholar] [CrossRef]
- Pilgrim, T.; Heg, D.; Roffi, M.; Tüller, D.; Muller, O.; Vuilliomenet, A.; Cook, S.; Weilenmann, D.; Kaiser, C.; Jamshidi, P.; et al. Ultrathin Strut Biodegradable Polymer Sirolimus-Eluting Stent versus Durable Polymer Everolimus-Eluting Stent for Percutaneous Coronary Revascularisation (BIOSCIENCE): A Randomised, Single-Blind, Non-Inferiority Trial. Lancet 2014, 384, 2111–2122. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, E.H.; Jensen, L.O.; Thayssen, P.; Tilsted, H.-H.; Krusell, L.R.; Hansen, K.N.; Kaltoft, A.; Maeng, M.; Kristensen, S.D.; Bøtker, H.E.; et al. Biolimus-Eluting Biodegradable Polymer-Coated Stent versus Durable Polymer-Coated Sirolimus-Eluting Stent in Unselected Patients Receiving Percutaneous Coronary Intervention (SORT OUT V): A Randomised Non-Inferiority Trial. Lancet 2013, 381, 661–669. [Google Scholar] [CrossRef]
- Raungaard, B.; Christiansen, E.H.; Bøtker, H.E.; Hansen, H.S.; Ravkilde, J.; Thuesen, L.; Aarøe, J.; Villadsen, A.B.; Terkelsen, C.J.; Krusell, L.R.; et al. Comparison of Durable-Polymer Zotarolimus-Eluting and Biodegradable-Polymer Biolimus-Eluting Coronary Stents in Patients With Coronary Artery Disease: 3-Year Clinical Outcomes in the Randomized SORT OUT VI Trial. JACC Cardiovasc. Interv. 2017, 10, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Windecker, S.; Serruys, P.W.; Wandel, S.; Buszman, P.; Trznadel, S.; Linke, A.; Lenk, K.; Ischinger, T.; Klauss, V.; Eberli, F.; et al. Biolimus-Eluting Stent with Biodegradable Polymer versus Sirolimus-Eluting Stent with Durable Polymer for Coronary Revascularisation (LEADERS): A Randomised Non-Inferiority Trial. Lancet 2008, 372, 1163–1173. [Google Scholar] [CrossRef]
- El-Hayek, G.; Bangalore, S.; Casso Dominguez, A.; Devireddy, C.; Jaber, W.; Kumar, G.; Mavromatis, K.; Tamis-Holland, J.; Samady, H. Meta-Analysis of Randomized Clinical Trials Comparing Biodegradable Polymer Drug-Eluting Stent to Second-Generation Durable Polymer Drug-Eluting Stents. JACC Cardiovasc. Interv. 2017, 10, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Sotomi, Y.; Suzuki, S.; Suwannasom, P.; Nakatani, S.; Morino, Y.; Ako, J.; Kozuma, K.; Hirayama, A.; Sakata, Y.; et al. Five-Year Clinical Efficacy and Safety of Contemporary Thin-Strut Biodegradable Polymer versus Durable Polymer Drug-Eluting Stents: A Systematic Review and Meta-Analysis of 9 Randomized Controlled Trials. Cardiovasc. Interv. Ther. 2020, 35, 250–258. [Google Scholar] [CrossRef]
- Versaci, F.; Kufner, S.; Cassese, S.; Joner, M.; Mayer, K.; Xhepa, E.; Koch, T.; Wiebe, J.; Ibrahim, T.; Laugwitz, K.-L.; et al. Very Long-Term Outlook of Acute Coronary Syndromes after Percutaneous Coronary Intervention with Implantation of Polymer-Free versus Durable-Polymer New-Generation Drug-Eluting Stents. Minerva Med. 2023, 114, 590–600. [Google Scholar] [CrossRef]
- Yin, J.; Li, Y.; Chen, Y.; Wang, C.; Song, X. Biodegradable Polymer Everolimus-Eluting Stents versus Contemporary Drug-Eluting Stents: A Systematic Review and Meta-analysis. Sci. Rep. 2023, 13, 1715. [Google Scholar] [CrossRef]
- Monjur, M.R.; Said, C.F.; Bamford, P.; Parkinson, M.; Szirt, R.; Ford, T. Ultrathin-Strut Biodegradable Polymer versus Durable Polymer Drug-Eluting Stents: A Meta-Analysis. Open Heart 2020, 7, e001394. [Google Scholar] [CrossRef]
- Baber, U.; Chandiramani, R.; Mehta, S.R.; Sartori, S.; Zhang, Z.; Claessen, B.E.; Briguori, C.; Sharma, S.; Dangas, G.; Mehran, R. Safety and Efficacy of the Bioabsorbable Polymer Everolimus-Eluting Stent versus Durable Polymer Drug-Eluting Stents in High-Risk Patients Undergoing PCI: TWILIGHT-SYNERGY. Catheter. Cardiovasc. Interv. 2021, 97, 63–71. [Google Scholar] [CrossRef]
- de Winter, R.J.; Katagiri, Y.; Asano, T.; Milewski, K.P.; Lurz, P.; Buszman, P.; Jessurun, G.A.J.; Koch, K.T.; Troquay, R.P.T.; Hamer, B.J.B.; et al. A Sirolimus-Eluting Bioabsorbable Polymer-Coated Stent (MiStent) versus an Everolimus-Eluting Durable Polymer Stent (Xience) after Percutaneous Coronary Intervention (DESSOLVE III): A Randomised, Single-Blind, Multicentre, Non-Inferiority, Phase 3 Trial. Lancet 2018, 391, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Koch, T.; Lenz, T.; Joner, M.; Xhepa, E.; Koppara, T.; Wiebe, J.; Coughlan, J.J.; Aytekin, A.; Ibrahim, T.; Kessler, T.; et al. Ten-Year Clinical Outcomes of Polymer-Free versus Durable Polymer New-Generation Drug-Eluting Stent in Patients with Coronary Artery Disease with and without Diabetes Mellitus: Results of the Intracoronary Stenting and Angiographic Results: Test Efficacy of Sirolimus- and Probucol- and Zotarolimus-Eluting Stents (ISAR-TEST 5) Trial. Clin. Res. Cardiol. 2021, 110, 1586–1598. [Google Scholar] [CrossRef]
- Jensen, L.O.; Thayssen, P.; Maeng, M.; Ravkilde, J.; Krusell, L.R.; Raungaard, B.; Junker, A.; Terkelsen, C.J.; Veien, K.T.; Villadsen, A.B.; et al. Randomized Comparison of a Biodegradable Polymer Ultrathin Strut Sirolimus-Eluting Stent With a Biodegradable Polymer Biolimus-Eluting Stent in Patients Treated With Percutaneous Coronary Intervention: The SORT OUT VII Trial. Circ. Cardiovasc. Interv. 2016, 9, e003610. [Google Scholar] [CrossRef]
- Maeng, M.; Christiansen, E.H.; Raungaard, B.; Kahlert, J.; Terkelsen, C.J.; Kristensen, S.D.; Carstensen, S.; Aarøe, J.; Jensen, S.E.; Villadsen, A.B.; et al. Everolimus-Eluting Versus Biolimus-Eluting Stents With Biodegradable Polymers in Unselected Patients Undergoing Percutaneous Coronary Intervention: A Randomized Noninferiority Trial With 1-Year Follow-Up (SORT OUT VIII Trial). JACC Cardiovasc. Interv. 2019, 12, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Urban, P.; Meredith, I.T.; Abizaid, A.; Pocock, S.J.; Carrié, D.; Naber, C.; Lipiecki, J.; Richardt, G.; Iñiguez, A.; Brunel, P.; et al. Polymer-Free Drug-Coated Coronary Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2015, 373, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Chiarito, M.; Sardella, G.; Colombo, A.; Briguori, C.; Testa, L.; Bedogni, F.; Fabbiocchi, F.; Paggi, A.; Palloshi, A.; Tamburino, C.; et al. Safety and Efficacy of Polymer-Free Drug-Eluting Stents. Circ. Cardiovasc. Interv. 2019, 12, e007311. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, C.; Galatius, S.; Jeger, R.; Gilgen, N.; Skov Jensen, J.; Naber, C.; Alber, H.; Wanitschek, M.; Eberli, F.; Kurz, D.J.; et al. Long-Term Efficacy and Safety of Biodegradable-Polymer Biolimus-Eluting Stents: Main Results of the Basel Stent Kosten-Effektivitäts Trial-PROspective Validation Examination II (BASKET-PROVE II), a Randomized, Controlled Noninferiority 2-Year Outcome Trial. Circulation 2015, 131, 74–81. [Google Scholar] [CrossRef]
- Saito, S.; Valdes-Chavarri, M.; Richardt, G.; Moreno, R.; Iniguez Romo, A.; Barbato, E.; Carrie, D.; Ando, K.; Merkely, B.; Kornowski, R.; et al. A Randomized, Prospective, Intercontinental Evaluation of a Bioresorbable Polymer Sirolimus-Eluting Coronary Stent System: The CENTURY II (Clinical Evaluation of New Terumo Drug-Eluting Coronary Stent System in the Treatment of Patients with Coronary Artery Disease) Trial. Eur. Heart J. 2014, 35, 2021–2031. [Google Scholar] [CrossRef]
- Maurina, M.; Chiarito, M.; Leone, P.P.; Testa, L.; Montorfano, M.; Reimers, B.; Esposito, G.; Monti, F.; Ferrario, M.; Latib, A.; et al. Randomized Clinical Trial of Abluminus DES+ Sirolimus-Eluting Stent versus Everolimus-Eluting DES for Percutaneous Coronary Intervention in Patients with Diabetes Mellitus: An Optical Coherence Tomography Study. Catheter. Cardiovasc. Interv. 2023, 102, 1020–1033. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Nie, S.; Hou, Y.; Huang, G.; Fu, G.; Zhou, H.; Wei, M.; Lu, F.; Zhang, F.; Wang, L.; et al. A Randomized Comparison of Bioheart Sirolimus-Eluting Bioresorbable Scaffold and Everolimus-Eluting Stents: The BIOHEART-II Trial. JACC Cardiovasc. Interv. 2025, 18, 15–27. [Google Scholar] [CrossRef]
- Patel, K.P.; Lansky, A.J.; Kelbæk, H.; Xu, B.; van Royen, N.; Johnson, T.W.; Anderson, R.; Wijns, W.; Baumbach, A. Long-Term Percutaneous Coronary Intervention Outcomes in Chronic Versus Acute Coronary Syndromes (TARGET All Comers Trial). Am. J. Cardiol. 2024, 217, 94–101. [Google Scholar] [CrossRef]
- von Birgelen, C.; Sen, H.; Lam, M.K.; Danse, P.W.; Jessurun, G.A.J.; Hautvast, R.W.M.; van Houwelingen, G.K.; Schramm, A.R.; Gin, R.M.T.J.; Louwerenburg, J.W.; et al. Third-Generation Zotarolimus-Eluting and Everolimus-Eluting Stents in All-Comer Patients Requiring a Percutaneous Coronary Intervention (DUTCH PEERS): A Randomised, Single-Blind, Multicentre, Non-Inferiority Trial. Lancet 2014, 383, 413–423. [Google Scholar] [CrossRef]
- Rasmussen, K.; Maeng, M.; Kaltoft, A.; Thayssen, P.; Kelbaek, H.; Tilsted, H.H.; Abildgaard, U.; Christiansen, E.H.; Engstrøm, T.; Krusell, L.R.; et al. Efficacy and Safety of Zotarolimus-Eluting and Sirolimus-Eluting Coronary Stents in Routine Clinical Care (SORT OUT III): A Randomised Controlled Superiority Trial. Lancet 2010, 375, 1090–1099. [Google Scholar] [CrossRef] [PubMed]
- Bundhun, P.K.; Yanamala, C.M.; Huang, W.-Q. Comparing Stent Thrombosis Associated with Zotarolimus Eluting Stents versus Everolimus Eluting Stents at 1 Year Follow up: A Systematic Review and Meta-Analysis of 6 Randomized Controlled Trials. BMC Cardiovasc. Disord. 2017, 17, 84. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.E.; McDonald, R.A.; Oldroyd, K.G.; Nicklin, S.A.; Baker, A.H. Prevention of Coronary In-Stent Restenosis and Vein Graft Failure: Does Vascular Gene Therapy Have a Role? Pharmacol. Ther. 2012, 136, 23–34. [Google Scholar] [CrossRef]
- Sim, D.S.; Jeong, M.H. Development of Novel Drug-Eluting Stents for Acute Myocardial Infarction. Chonnam Med. J. 2017, 53, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, L.; Christiansen, E.H.; Freeman, P.; Kahlert, J.; Veien, K.; Maeng, M.; Raungaard, B.; Ellert, J.; Villadsen, A.B.; Kristensen, S.D.; et al. Dual-Therapy CD34 Antibody-Covered Sirolimus-Eluting COMBO Stents versus Sirolimus-Eluting Orsiro Stents in Patients Treated with Percutaneous Coronary Intervention: The Three-Year Outcomes of the SORT OUT X Randomised Clinical Trial. EuroIntervention 2023, 19, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Pasceri, V.; Zimarino, M.; De Luca, G.; De Caterina, R.; Mehran, R.; Dangas, G. Endothelial Progenitor Cells in Coronary Atherosclerosis and Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. Cardiovasc. Revasc Med. 2022, 42, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Kedhi, E.; Suryapranata, H.; Galasso, G.; Dudek, D.; De Luca, G. Poly (l-Lactic Acid) Bioresorbable Scaffolds versus Metallic Drug-Eluting Stents for the Treatment of Coronary Artery Disease: A Meta-Analysis of 11 Randomized Trials. Catheter. Cardiovasc. Interv. 2020, 96, 813–824. [Google Scholar] [CrossRef]
- Erlinge, D.; Andersson, J.; Fröbert, O.; Törnerud, M.; Hamid, M.; Kellerth, T.; Grimfjärd, P.; Winnberg, O.; Jurga, J.; Wagner, H.; et al. Bioadaptor Implant versus Contemporary Drug-Eluting Stent in Percutaneous Coronary Interventions in Sweden (INFINITY-SWEDEHEART): A Single-Blind, Non-Inferiority, Registry-Based, Randomised Controlled Trial. Lancet 2024, 404, 1750–1759. [Google Scholar] [CrossRef]

{kind=link}
| Name of the Study | DES Compared | Population | Endpoints Observed | Outcomes | Reference |
|---|---|---|---|---|---|
| COMPARE-II | Biodegradable polymer biolimus-eluting stent vs. thin strut durable biocompatible polymer everolimus-eluting stent | 2707 patients (age > 18 years, life expectancy > 5 years, reference vessel diameter 2–4 mm) | Cardiac death and non-fatal myocardial infarction or clinically indicated target vessel revascularization at 12 months | 93 patients (5.2%) vs. 44 patients (4.8%); pnon-inferiority < 0.001 | [42] |
| BASKET PROVE II | Biodegradable polymer biolimus-eluting DES vs. permanent polymer everolimus-eluting DES (additionally vs. thin strut silicon-carbide-coated BMS) | 2291 patients presenting with acute or stable coronary disease needing stents ≥ 3.0 mm in diameter | Combined cardiac death, myocardial infarction, and clinically indicated target-vessel revascularization within 2 years | 7.6% vs. 6.8%; pnon-inferiority = 0.042 12.7% in the BMS group | [69] |
| NEXT | Biodegradable polymer biolimus-eluting stent vs. durable polymer everolimus-eluting stent | 3235 patients who underwent PCI using DES | Death or myocardial infarction | 159 patients (9.9%) vs. 166 patients (10.3%); pnon-inferiority < 0.001 No significant difference between groups in target-lesion revascularization and cumulative incidence of death or myocardial infarction at 1 year between the 2 groups | [44] |
| SORT-OUT V | Biodegradable polymer biolimus-eluting stent vs. durable polymer sirolimus-eluting stent | 2468 patients aged 18 years or older with chronic stable coronary artery disease or acute coronary syndromes, and at least one coronary artery lesion (>50% diameter stenosis) | A composite of safety (cardiac death, myocardial infarction, definite ST) and efficacy—target vessel revascularization at 9 months | Intention-to-treat analysis, primary endpoint: 50 patients (4.1%) vs. 39 patients (3.1%); pnon-inferiority = 0.06 Definite ST at 12 months: 0.7% vs. 0.2%; p = 0.034 Per-protocol analysis, primary endpoint: 3.8% vs. 3.2%; pnon-inferiority = 0.03 | [54] |
| SORT-OUT VII | The thin strut cobalt–chromium sirolimus-eluting stent vs. stainless-steel biolimus-eluting stent | 2525 patients aged 18 years or older, chronic stable coronary artery disease or acute coronary syndrome, and at least 1 coronary lesion with >50% diameter stenosis, requiring treatment with a DES | Target lesion failure—a composite of cardiac death, myocardial infarction (not related to the index lesion), or target lesion revascularization within 1 year | 48 patients (3.8%) vs. 58 patients (4.6%); pnon-inferiority < 0.001 | [65] |
| SORT-OUT VI | Biocompatible durable-polymer zotarolimus-eluting stent vs. biodegradable-polymer biolimus-eluting stent | 2999 patients with chronic stable coronary artery disease or acute coronary syndrome and at least 1 coronary artery lesion requiring treatment with a DES | Major adverse cardiac events; a composite of safety (cardiac death and myocardial infarction not clearly attributable to a non-target lesion) and target lesion revascularization: all-cause mortality; any myocardial infarction; target vessel revascularization; and definite or probable ST at 36 months | Cardiac death: 2.7% vs. 3.4% (not statistically significant) myocardial infarction not clearly attributable to a non-target lesion: 2.7% vs. 2.5% (not statistically significant) Target lesion revascularization: 5.4% vs. 5.5% (not statistically significant) Definite very late ST: 6 patients (0.4%) vs. 10 patients (0.7%); p = 0.33 | [55] |
| BIOSCIENCE | Ultrathin strut biodegradable polymer cobalt–chromium sirolimus-eluting stent vs. thin strut durable polymer everolimus-eluting stent | 2119 patients aged 18 years or older with chronic stable coronary artery disease or acute coronary syndromes undergoing PCI | Target lesion failure—a composite of cardiac death, target vessel myocardial infarction, and clinically indicated target lesion revascularization at 12 months | Target lesion failure in 69 patients (6.5%) vs. 70 (6.6%) at 12 months; pnon-inferiority < 0.001 No significant differences in rates of definite ST 9 (0.9%) vs. 4 (0.4%); p = 0.16 | [53] |
| CENTURY II | Bioresorbable polymer sirolimus-eluting stent vs. permanent polymer everolimus-eluting stent | 1123 patients requiring PCI with implantation of DES | Absence of target lesion failure at 9 months (composite of cardiac death, target-vessel-related myocardial infarction and target lesion revascularization | 95.6% vs. 95.1%; pnon-inferiority < 0.001 Cardiac death and myocardial infarction rate were 2.9% and 3.8%; p = 0.40 Target vessel revascularization was 4.5% vs. 4.2%; p = 0.77 ST rate was 0.9% in both groups | [70] |
| ABILITY | Biodegradable polymer sirolimus-eluting stent vs. durable polymer everolimus-eluting stent | 131 patients with diabetes and coronary artery disease | Neointimal volume at 9–12-month follow-up Target lesion failure | 29.11 ± 18.90 mm3 vs. 25.48 ± 17.04 mm3; p = 0.40 Target lesion failure: 21.2% vs. 19.6% | [71] |
| BIOHEART-II | Bioresorbable sirolimus-eluting stent vs. cobalt–chromium everolimus-eluting stent | 434 patients with coronary artery disease | 12-month in-segment late loss 12-month proportion of covered struts assessed on optical coherence tomography Target lesion failure at 3 years | 12-month in-segment late loss 0.17 ± 0.38 mm vs. 0.14 ± 0.24 mm; pnon-inferiority < 0.001 The proportion of covered struts was 97.9% vs. 98.5%; pnon-inferiority < 0.001; psuperiority = 0.91 Target lesion failure at 3 years: 5.6% vs. 5.2%; p = 0.84 | [72] |
| TARGET All Comers Trial | Biodegradable polymer sirolimus-eluting stent vs. durable polymer everolimus-eluting stent | 1653 patients with acute or chronic coronary syndrome | Target lesion failure, ischemia-driven target revascularization and definite or probable ST in both groups at 5 years | Acute coronary syndrome: target lesion failure 16.0% vs. 14.9%; p = 0.70, ischemia-driven target lesion revascularization 5.6% vs. 8.3%; p = 0.17, and definite/probable ST 2.7% vs. 4.6%; p = 0.18 Target lesion failure 18.0% vs. 17.4%; p = 0.82, ischemia-driven target lesion revascularization 6.4% vs. 5.0%; p = 0.37, and definite/probable ST 3.0% vs. 1.8%; p = 0.26 | [73] |
| DUTCH PEERS | Cobalt–chromium zotarolimus-eluting stent vs. platinum–chromium everolimus-eluting stent | 1811 patients aged 18 years and older who required a percutaneous coronary intervention with implantation of DES | Target-vessel failure—a composite of safety (cardiac death or target-vessel-related myocardial infarction) and efficacy (target-vessel revascularization) at 12 months | Target-vessel failure: 55 patients (6%) vs. 47 patients (5%); pnon-inferiority = 0.006 Definite ST: 3 (0.3%) patients vs. 6 (0.7%) patients; p = 0.34 | [74] |
| RESOLUTE | Zotarolimus-eluting stent vs. everolimus-eluting stent | 2292 adult patients with chronic, stable coronary artery disease or acute coronary syndrome | Patient-oriented composite endpoint (combination of all-cause mortality, myocardial infarction, and any revascularizations) at 5-year follow-up Device-oriented composite endpoint (combination of cardiac death, target vessel myocardial infarction, and clinically indicated target lesion revascularization) at 5-year follow-up Major adverse cardiac events (combination of all-cause death, all myocardial infarction, emergent coronary bypass surgery, or clinically indicated target lesion revascularization) at 5-year follow-up | Patient-oriented composite endpoint 35.3% vs. 32.0%; p = 0.11 Device-oriented composite endpoint 17.0% vs. 16.2%; p = 0.61 Major adverse cardiac events 21.9% vs. 21.6%; p = 0.88 definite/probable ST 2.8% vs. 1.8%; p = 0.12 | [37] |
| SORT-OUT III | Zotarolimus-eluting stent vs. sirolimus-eluting stent | 2332 adult patients with chronic stable coronary artery disease or acute coronary syndrome and at least one target lesion | Primary endpoint (a composite of major adverse cardiac events within 9 months: cardiac death, myocardial infarction, and target vessel revascularization) Intention-to-treat analyses were done at 9-month and 18-month follow-up | Primary endpoint at 9-month follow-up: 72 (6%) vs. 34 (3%); p < 0.001 Primary endpoint at 18-month follow-up: 113 (10%) vs. 53 (5%); p < 0.001 All-cause-mortality at 9-month follow-up: 25 (2%) vs. 18 (2%); p = 0.28 All-cause mortality at 18-month follow-up: 51 (4%) vs. 32 (3%); p = 0.035 | [75] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arh, R.; Balevski, I.; Granda, S.; Bevc, S. Drug-Eluting Stent Use in Percutaneous Coronary Interventions—A Narrative Review. J. Clin. Med. 2025, 14, 4643. https://doi.org/10.3390/jcm14134643
Arh R, Balevski I, Granda S, Bevc S. Drug-Eluting Stent Use in Percutaneous Coronary Interventions—A Narrative Review. Journal of Clinical Medicine. 2025; 14(13):4643. https://doi.org/10.3390/jcm14134643
Chicago/Turabian StyleArh, Rok, Igor Balevski, Samo Granda, and Sebastjan Bevc. 2025. "Drug-Eluting Stent Use in Percutaneous Coronary Interventions—A Narrative Review" Journal of Clinical Medicine 14, no. 13: 4643. https://doi.org/10.3390/jcm14134643
APA StyleArh, R., Balevski, I., Granda, S., & Bevc, S. (2025). Drug-Eluting Stent Use in Percutaneous Coronary Interventions—A Narrative Review. Journal of Clinical Medicine, 14(13), 4643. https://doi.org/10.3390/jcm14134643