Abstract
Aim: To compare the three-year surgical outcomes among the Kahook dual blade (KDB), Tanito microhook (TMH), T-hook, and 360° suture trabeculotomy (S-lot) cohorts. Study design: Retrospective interventional comparative study conducted at a single eye center. Subjects and Methods: A total of 224 eyes that underwent combined cataract surgery with either KDB, TMH, T-hook, or S-lot procedures were retrospectively analyzed over the three-year period. Results: According to Tukey’s multiple comparison test, postoperative intraocular pressure (IOP) in the S-lot cohort was significantly lower than in the TMH cohort from 1 month to 3 years (p = 0.01 to <0.001), lower than in the KDB cohort between 6 months and 1 year (p = 0.026 to <0.001), and lower than in the T-hook cohort at 1 month (p = 0.012) and from 6 to 12 months (p < 0.001). The survival probability of achieving ≤15 mmHg and ≤18 mmHg in the S-lot cohort was significantly better than in others by p < 0.001 and 0.005, respectively. At 3 months, the T-hook cohort showed significantly lower IOP than the TMH cohort (p = 0.029), and at 1 week, IOP was marginally lower than in the KDB (p = 0.063) and TMH (p = 0.052) cohorts, based on Dunnett’s test. However, no significant differences in postoperative IOP were observed among the three sectorial canal-opening surgery (COS) groups beyond 6 months. Conclusions: Among the four MIGS cohorts, S-lot provided the most substantial mid-term postoperative IOP reduction. The T-hook cohort showed marginally superior IOP reduction at 1 week compared to the KDB and TMH groups.
1. Introduction
Canal-opening surgeries (COSs), performed from inside the eye, are increasingly used to treat mild to moderate glaucoma.
A variety of devices, such as Trabectome, BANG (bent ab interno needle goniotomy), and others, are employed to open the Schlemm’s canal. These procedures preserve the conjunctiva, are associated with fewer severe postoperative complications, and maintain good postoperative visual acuity. Previous reports suggest that both the technique and the extent of trabecular meshwork incision may influence surgical outcomes; however, expert opinions remain divided. Some reports indicate that a wider incision results in better intraocular pressure (IOP) reduction [1,2,3], whereas others report no significant impact [4,5,6]. Wider incisions may increase the risk of hyphema [7], which may be associated with postoperative IOP spikes and potentially affect final surgical outcomes [8].
Although most cases of postoperative hyphema are resolved shortly after surgery, the design of the surgical instrument—whether hook, blade, or suture—may influence the incidence and severity of bleeding. Devices with a curved distal tip [9] or those using sutures (as in 360° trabeculotomy) may reduce the risk of damaging the posterior wall of the Schlemm’s canal and thereby minimize bleeding. However, evidence remains limited regarding how different surgical techniques affect postoperative bleeding and long-term IOP control.
In this study, we aimed to compare the mid-term surgical outcomes and complication profiles of four canal-opening procedures.
2. Materials and Methods
This retrospective study included patients with mild to moderate primary open-angle glaucoma (POAG), exfoliation glaucoma (XFG), or ocular hypertension (OH), all of whom were indicated for concomitant internal COS and small-incision cataract surgery. Patients who underwent stent-based procedures or mini-tube insertions were excluded.
A total of 389 eyes from 279 patients who underwent concomitant phacoemulsification, implantation of intraocular lens, and COSs between May 2018 and July 2024 at Sensho-kai Eye Institute were included. The three-year outcomes of four different COS procedures, namely, Kahook dual blade (KDB: New World Medical, Rancho Cucamonga, CA, USA, 22BAIBZX00022000 JFC), Tanito microhook (TMH: Inami, Tokyo, Japan, M2215S), T-hook (Inami, Tokyo, Japan, M-2225 and Handaya, Tokyo, Japan, HS-9939), and 360° suture trabeculotomy (S-lot: Handaya, Tokyo, Japan, HS 2756), were analyzed. The choice of device primarily depended on the timing of the introduction of these devices at Sensho-kai; KDB was selected between 2016 and 2019, TMH between 2018 and 2021, and T-hook between 2021 and 2024. The criteria for selecting sectorial COS procedures (KDB, TMH, T-hook, and S-lot) were the same. The selection of S-lot was at the discretion of one of the authors (TC), who preferred this procedure.
Preoperative intraocular pressure (IOP) was defined as the highest IOP recorded within the three months prior to surgery. Additionally, the “preoperative 3-mean IOP” was calculated as the average of three consecutive IOP measurements taken under medication before surgery.
Inclusion criteria: Patients were aged 40 years or older (range: 44–90 years) and had a documented preoperative IOP ≥ 18 mmHg within three months prior to surgery. If both eyes were eligible, only the right eye was included in the analysis.
Exclusion criteria: Patients were excluded if they met any of the following conditions:
A mean of three consecutive preoperative IOP measurements under topical medications exceeded 35 mmHg. History of prior glaucoma surgery or selective laser trabeculoplasty. Intraoperative rupture of the posterior capsule or lens luxation. Diagnosis of primary angle-closure glaucoma, secondary glaucoma, congenital glaucoma, or normal tension glaucoma. Underwent standalone COS without combined cataract surgery. Postoperative follow-up period less than 6 months.
After applying the exclusion criteria, one eye from 224 patients (43 KDB, 57 TMH, 86 T-hook, and 38 S-lot eyes) was enrolled and included in the final analysis.
Low visual acuity was converted to logMAR values according to the British conversion method [10]: counting fingers, hand motion, positive light sense, and no light sense were converted to logMAR values of 2.1, 2.4, 2.7, and 3.0, respectively.
2.1. Surgical Procedures
The surgical procedures have been previously reported [9]. In brief, all surgeries were performed in conjunction with cataract surgery. Following the injection of viscoelastic material and completion of anterior capsulorhexis, the devices (KDB, TMH, and T-hook) were inserted through a clear corneal opening at the 10 o’clock position, and the trabecular meshwork was incised over 120 to 150 degrees using a double-mirror Ahmed surgical goniolens (UADVX-H, Ocular, WA, USA). After completing the internal trabeculotomy, phacoemulsification, aspiration, and intraocular lens implantation were performed. After completion of cataract surgery, a 0.25% acetylcholine solution was injected into the anterior chamber, and the corneal wound was closed with a single 10-0 nylon suture. Anti-glaucoma medications were administered if postoperative IOP was elevated. Following the surgery, Gatifloxacin, 0.1% Betamethasone and 2% pilocarpine eye drops were applied four times per day for 2 to 4 weeks. The extent of canal opening was obtained from operative notes.
In the case of S-lot, a small incision of the trabecular meshwork was made using a fine slit knife after completion of capsulorhexis. A small amount of viscoelastic material was then injected into the Schlemm’s canal to expand it, and a specially designed 5-0 nylon suture adapted for suture trabeculotomy (Handaya Tokyo HS 2756) was inserted into the Schlemm’s canal. The 5-0 nylon was grasped with forceps and gently advanced to achieve 360-degree insertion into the Schlemm’s canal. If strong resistance was encountered and the nylon suture did not advance, an additional incision of the trabecular meshwork was created at a different meridian, the nylon suture was grasped at this second point, and insertion was attempted again. When the end of the suture appeared at the initial insertion site, both ends of the nylon suture were grasped and pulled to open the Schlemm’s canal.
2.2. Classification of Intracameral Bleedings
Post-surgical bleeding into the anterior chamber in these patients was classified using the Shimane University grading system [11], which categorizes hyphema based on severity and density, as well as the presence of clot formation. Severity of hyphema (layering) was classified into 4 categories: L0: no hyphema; L1: layered blood less than 1 mm; L2: layered blood ≥ 1 mm but not exceeding the inferior pupillary margin; L3: layered blood exceeding the inferior pupillary margin. Density of intracameral bleeding was classified into 4 categories: R0: no floating red blood cell; R1: iris patterns clearly visible despite the presence of floating red blood cells; R2: Iris patterns are not clearly visible due to floating red blood cells; R3: iris pattern completely obscured. Intracameral clot formation was classified into 2 categories: C0: no blood clot formation; C1: presence of intracameral blood clot formation.
Statistical analysis: Statistical analyses were performed using Bell Curve for Excel (Social Survey Research Information Co., Tokyo, Japan). Multiple comparisons were evaluated using Tukey’s and Dunnett’s tests. Kaplan–Meier survival analysis was used to assess surgical success over time. The Wilcoxon signed-rank test was employed for paired comparison; Haberman residual analysis was used for categorical data.
3. Results
Demographic baseline data are presented in Table 1. There was no significant difference among the cohorts in baseline age, logMAR best-corrected visual acuity, preoperative IOP, the mean of three consecutive preoperative IOP measurements under topical medications, or the number of preoperative medications. However, the refractive error in the T-hook cohort was significantly less than that in the S-lot cohort (p = 0.048). The mean deviation (MD) of the Humphrey Visual Field Analyzer was significantly worse in the S-lot cohort compared to the other three COS cohorts (p < 0.005).

Table 1.
Baseline characteristics of the four canal-opening surgery cohorts.
The extent of canal opening in the S-lot cohort was 325 ± 87°, which was significantly greater than that in the T-hook (153 ± 52), KDB (137 ± 28), and TMH (129 ± 23°) cohorts (p < 0.001). The difference between T-hook and TMH (p = 0.067) and between T-hook and KDB (p = 0.43) were not statistically significant according to Tukey’s multiple comparison test.
The mean follow-up periods were as follows: KDB, 47.9 ± 16.8 months; TMH, 30.3 ± 18.9 months; T-hook, 16.0 ± 9.7 months; and S-lot, 35.1 ± 21.1 months. The follow-up period for the T-hook cohort was significantly shorter (p < 0.001), while that for the KDB cohort was significantly longer than the other three COS cohorts (p < 0.005), as determined by Tukey’s multiple comparison test.
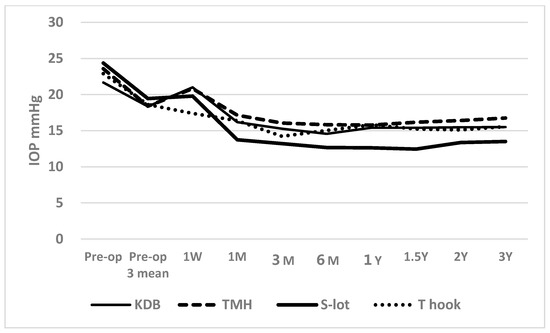
Figure 1.
Time course of postoperative IOP in the four canal-opening surgery cohorts. A transient elevation (“hump”) in IOP was observed at 1 week postoperatively in the KDB, TMH, and S-lot cohorts, likely reflecting a response to postoperative intracameral bleeding. Following this initial rise, IOP significantly decreased in all cohorts and remained reduced through 3 years of follow-up. Postoperative IOP in the S-lot cohort was significantly lower than in the other three sectorial COS cohorts, as determined by Tukey’s multiple comparison test (Table 2).
Postoperatively, the IOP between 1 month and 3 years was significantly lower than preoperative IOP in all four cohorts, with a p < 0.001 using the Wilcoxon signed-rank test. A short-term elevation in IOP was observed at 1 week in the KDB, TMH, and S-lot cohorts, likely reflecting the effects of postoperative intracameral bleeding. Despite this early increase, the IOP at 1 week remained significantly lower than preoperative levels in the TMH (p = 0.005), S-lot (p = 0.011), and T-hook (p < 0.001) cohorts; however, the reduction in the KDB cohort was not significant (p = 0.198).
The number of anti-glaucoma medications significantly decreased from baseline in all cohorts. Preoperative medications used in the KDB, TMH, S-lot, and T-hook cohorts were 2.6 ± 1.3, 2.7 ± 1.5, 3.2 ± 1.1, and 2.8 ± 1.3, respectively. At 3 months postoperatively, the number of medications decreased to 1.2 ± 1.0, 1.7 ± 1.4, 2.1 ± 1.3, and 1.8 ± 1.3, respectively (all p < 0.001, Wilcoxon signed-rank test). A gradual increase in medication use was observed at 2 years, reaching 1.6 ± 1.2, 1.8 ± 1.3, 2.4 ± 1.4, and 2.4 ± 0.9, respectively. Despite this increase, the number of medications at two years remained significantly lower than the preoperative baseline in all cohorts (p < 0.05, Wilcoxon signed-rank test).
Although there was no difference in baseline preoperative IOP or the mean of three preoperative IOP measurements under medication among the four COS cohorts, one-way ANOVA revealed a significant difference in postoperative IOP among the cohorts over the follow-up period from 1 month to 3 years (p < 0.05, Table 2).
Table 2.
Time course of IOP after four different COS procedures, and differences among them assessed by multiple comparison test.
According to Tukey’s multiple comparison test, the postoperative IOP in the S-lot cohort was significantly lower than that in the TMH cohort at 1 month through 3 years, the KDB cohort at 6 months and 12 months, and the T-hook cohort at 1 month, 6 months, and 1 year, respectively (Table 2).
A significant difference in the percentage reduction in IOP was observed among the four COS cohorts between 3 months and 2 years, as determined by one-way ANOVA (Table 3). Using Tukey’s multiple comparison test, the percentage IOP reduction in the S-lot cohort was significantly greater than that in the KDB cohort between 3 months and 1 year, the TMH cohort between 6 months and 2 years, and the T-hook cohort between 6 months and 1 year. In contrast, no significant differences were observed in the percentage IOP reduction among the three sectorial COS procedures (KDB, TMH, and T-hook).
Table 3.
Comparison of percentage IOP reduction among four COS procedures and statistical differences assessed by multiple comparison tests.
According to Dunnett’s multiple comparison test, the comparison between T-hook and KDB cohorts yielded a p-value of 0.089 at 3 months. Although the T-hook cohort showed greater IOP reduction, this difference was not statistically significant.
When comparing postoperative IOP among three sectorial COS cohorts (KDB, TMH, and T-hook), a transient elevation above the mean of three preoperative IOP measurements at 1 week was observed in KDB and TMH cohorts (Figure 2). According to Dunnett’s multiple comparison test, IOP measurements in the KDB (p = 0.063) and TMK (p = 0.052) cohorts at 1 week were marginally higher than in the T-hook cohort, possibly due to greater intracameral bleeding and clot formation in the KDB and TMH cohorts (Table 4 and Table 5). The significant difference in IOP between the T-hook cohort and TMH cohort at 3 months (p = 0.029), according to Dunnett’s multiple comparison test, may also reflect effects of intracameral bleedings (Table 2). After 3 months, no significant differences in IOP were detected among the three sectorial COS groups through 3 years of follow-up (Table 2).
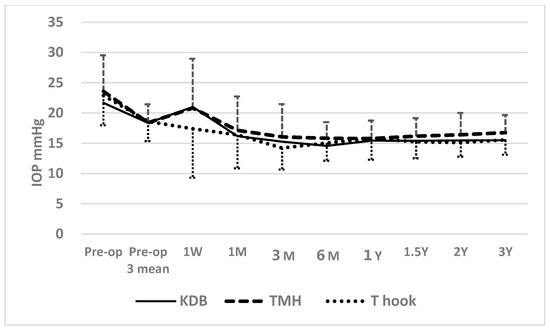
Figure 2.
Time course of postoperative IOP in the three sectorial COS cohorts. At 1 week postoperatively, IOP in the KDB (p = 0.063) and TMH (p = 0.052) cohorts was marginally higher than in the T-hook cohort. At 3 months, IOP in the TMH cohort was significantly higher than in the T-hook cohort (p = 0.029; Table 2), potentially reflecting a higher prevalence of postoperative clot formation and a greater density of red blood cells in the anterior chamber (Table 4 and Table 5). However, from 6 months onward, no differences in IOP were observed among the three sectorial COS cohorts.
Table 4.
Prevalence of intracameral blood coagula formation in each COS cohort.
Table 5.
Density of intracameral bleeding the next day after surgery.
The Kaplan–Meier life table analysis supported these findings. A significant difference was observed among the four COS cohorts in achieving postoperative IOP targets of ≤15 mmHg and ≤18 mmHg under medication. At 3 years, cumulative success probability for achieving IOP ≤ 15 mmHg was highest in the S-lot cohort (65.9 ± 9.4%), compared to KDB (23.9 ± 7.0%), T-hook (39.9 ± 7.4%), and TMH (18.4 ± 6.4%), with a significant difference by log-rank test (p < 0.001; Figure 3). In contrast, no significant difference was found among the three sectorial COS procedures for this outcome (p = 0.478, log-rank test).
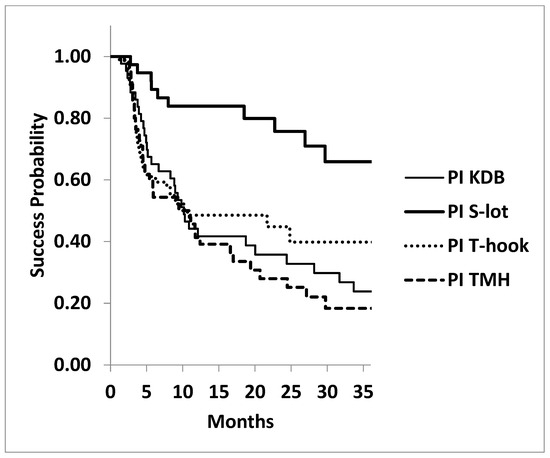
Figure 3.
Kaplan–Meier survival curves: probability of achieving postoperative IOP ≤ 15 mmHg following four types of canal-opening, minimally invasive glaucoma surgeries (MIGSs). The cumulative success probability of achieving postoperative IOP ≤ 15 mmHg at three years was significantly higher in the 360° canal-opening procedure (S-lot cohort) compared to the three sectorial canal-opening procedures (Kahook dual blade, Tanito microhook, and T-hook) (p < 0.001, log-rank test). No statistically significant differences were found among the three sectorial canal-opening procedures (p = 0.478, log-rank test).
The success probability at three years for achieving IOP ≤ 18 mmHg under medications was also significantly higher in the S-lot cohort (93.1 ± 4.9%) compared to the KDB (73.9 ± 7.8%), T-hook (77.7 ± 5.7%), and TMH (56.2 ± 8.3%) cohorts (p = 0.0052, log-rank test; Figure 4). However, no significant differences were observed among the three sectorial COS procedures (p = 0.121, log-rank test).
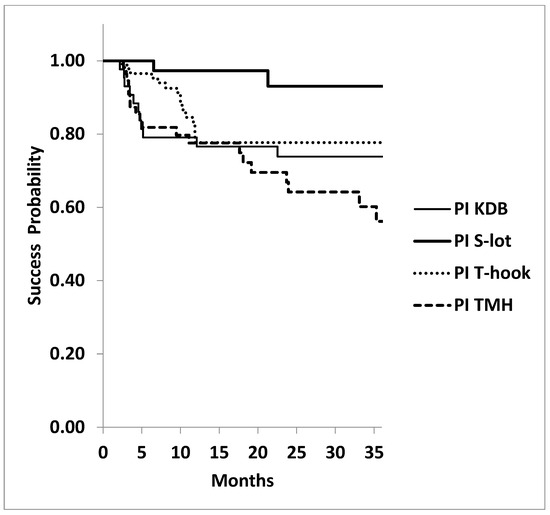
Figure 4.
Kaplan–Meier analysis: probability of achieving postoperative IOP ≤ 18 mmHg at 3 years under medications following four types of canal-opening, minimally invasive glaucoma surgeries (MIGSs). The cumulative success probability of achieving postoperative IOP ≤ 18 mmHg at three years was again significantly higher in the 360º canal-opening procedure (S-lot cohort) compared to the other three sectorial canal-opening procedures (Kahook dual blade, Tanito microhook, and T-hook) (p = 0.0052, log-rank test). No significant differences in success probability were observed among the three sectorial canal-opening procedures (p = 0.121, log-rank test).
The success probability for achieving ≥20% IOP reduction at three years in KDB, S-lot, T-hook, and TMH was 59.2 ± 7.7%, 78.4 ± 7.7%, 56.3 ± 10.0%, and 45.1 ± 8.1%, respectively. And the difference was marginally significant (p = 0.0518, log-rank test).
There was no significant difference among the four COS procedures at 3 years in achieving an IOP ≤ 21 mmHg at three years. The success probability in KDB, S-lot, T-hook, and TMH cohorts was 95.0 ± 3.4%, 93.1 ± 4.8%, 92.0 ± 3.9%, and 88.6 ± 4.4%, respectively (p = 0.511, log-rank test).
3.1. Postoperative Intracameral Bleeding
When post-surgical intracameral bleeding was compared among the four cohorts, L1 layer bleeding was observed in 36.8% of patients who underwent S-lot, which was the highest incidence among the four COS cohorts (p = 0.001, Haberman residual analysis; Table 6).
Table 6.
Difference in incidence of intracameral layer bleeding among four COS cohorts.
Blood coagula formation in the anterior chamber was observed in 19.8% of cases in the T-hook cohort, which was significantly lower than in the other three COS cohorts (p < 0.001). In contrast, coagula were observed in 49.1% of cases in the TMH cohort, representing the highest prevalence among the four groups (p = 0.004).
R0 (no floating red blood cell on the first postoperative day) was observed in 27.9% of patients who underwent the T-hook procedure, significantly more frequent than in the other cohorts (p < 0.001). In contrast, the R0 was rare in the TMH (p = 0.004) and S-lot (p = 0.009) cohorts. R2 (iris pattern not clearly visible due to floating red blood cells) was noted in 39.5% of S-lot cases, which was significantly higher than in other cohorts. While it was observed in only 15.1% of T-hook cases, which was significantly lower than others (p = 0.013).
The average time required for resolution of intracameral bleeding was shorter in the S-lot cohort at 3.1 ± 2.4 days, significantly faster than that in the KDB cohort, which required 9.1 ± 6.0 days (p = 0.006, Tukey’s multiple comparison test).
The resolution times for the T-hook and TMH cohorts were 6.4 ± 8.1 days and 6.3 ± 6.8 days, respectively. Differences among the KDB, T-hook, and TMH groups were not statistically significant (p = 0.43–1.00, multiple comparison test).
3.2. Postoperative IOP Spike
A postoperative spike was defined as an elevation of ≥5mmHg above the mean of three consecutive preoperative IOP measurements occurring within two weeks after surgery. The T-hook cohort had the lowest spike rate at 36.0%, which was significantly less than in the other three COS groups (p < 0.001; Haberman residual analysis, Table 7). In contrast, the TMH cohort had the highest spike rate at 66.7%, significantly more frequent than in other cohorts (p = 0.004, Table 7).
Table 7.
Prevalence of postoperative IOP spike in each COS cohort.
4. Discussion
There are several factors that may influence postoperative IOP following canal-opening surgery. One such factor is the extent of the Schlemm’s canal opening. Theoretically, a wider opening of the canal should result in greater IOP reduction [12]. However, if one or two intact aqueous veins are sufficient to drain enough aqueous humor [13], a broad canal opening may not be necessary. It is reported that active aqueous veins are located in the inferonasal quadrant of the angle [14,15], suggesting that a sectorial opening in this region alone may be sufficient to reduce IOP. Several reports suggest that an opening of 90 to 120 degrees can be sufficient for significant IOP reduction [7,16,17,18,19]. Some reports even suggest that implantation of a single iStent may achieve an IOP reduction comparable to that seen with KDB procedures [20,21]. Conversely, other studies have shown that 360° goniotomy results in greater IOP reduction than sectorial goniotomy [1,2,22,23].
Since blood coagula tend to settle in the inferior half of the eye, peripheral anterior synechia (PAS), which also commonly develops in this region, may obstruct the inferior canal opening. In this study, the mid-term IOP reduction in eyes that underwent sectorial opening of the Schlemm’s canal in the inferior quadrant was less pronounced compared to that in the S-lot cohort, where the trabecular meshwork was circumferentially opened. This finding suggests that enhanced aqueous outflow through the superior quadrant in eyes with 360° trabecular meshwork incision may have contributed to greater IOP reduction than in eyes treated with inferior sectorial incisions (KDB, TMH, and T-hook cohorts).
Postoperative intracameral bleeding may contribute to PAS formation, transient IOP spikes, and poor IOP control [8,24]. The trabecular meshwork is avascular, and injury to the trabecular meshwork is not responsible for postoperative bleeding. The main cause of postoperative bleeding is attributed to backflow from the collector channel and impairment of backyard tissue named Bell [25]. Here, the sharp tip of devices may cause penetration of the Bell and bleeding. In this study, postoperatively, the IOP at 1 week was marginally higher in the TMH and KDB cohorts compared to the T-hook cohort, in which the incidence of clot formation and the density of intracameral bleeding were significantly lower. As shown in Figure 2, the IOP at 1 week in the KDB and TMH cohorts exceeded the mean of three consecutive preoperative IOP measurements, whereas the T-hook cohort showed a lower IOP. These findings suggest that the higher incidence of clot formation and intracameral bleeding may have contributed to the transient IOP elevation observed in KDB and TMH cohorts at 1 week. Despite the short-term IOP rise in KDB and TMH cohorts at 1 week and the higher IOP in the TMH cohort at 3 months, no significant differences in postoperative IOP were observed among the three sectorial COS groups after 6 months. This finding suggests that the impact of postoperative bleeding on IOP is transient and does not persist long-term.
In the S-lot cohort, postoperative IOP elevation at 1 week was 19.9 ± 10.0, which was milder than that observed in the KDB and TMH cohorts (Table 2). The intracameral bleeding resolved in an average of only 3.1 days, which was shorter than in the other cohorts. This suggests that the wide circumferential opening of the trabecular meshwork may have facilitated efficient clearance of red blood cells from the anterior chamber.
Another potential confounding factor affecting surgical outcome is the wound-healing response at the trabecular meshwork. Suture trabeculotomy does not involve excision of the trabecular meshwork, whereas KDB excises the meshwork tissue. In contrast, TMH and T-hook do not remove the trabecular meshwork but instead displace it to create a “double door” opening. Despite these differences in the mechanism of canal opening, previous studies comparing KDB, TMH, and T-hook have not demonstrated significant differences in surgical outcomes [26,27]. The findings of the current study similarly suggest that, in terms of mid-term outcomes, there is no significant difference in IOP reduction among the three sectorial COS procedures.
Therefore, excision of the trabecular meshwork tissue may not be essential in achieving mid-term IOP reduction.
Although postoperative bleeding typically resolves shortly after surgery in most cases, severe complications such as corneal blood staining can occasionally occur. In case of massive hyphema accompanied by intense pain, surgical interventions such as paracentesis and anterior chamber washout may be required. The lower incidence of postoperative bleeding and IOP spikes in the T-hook cohort suggests that the use of the T-hook may offer clinical benefits for patients.
The T-hook features blades on both sides of the shaft, allowing it to bilaterally incise the trabecular meshwork. Compared to other canal-opening surgery (COS) devices, it has the advantage of enabling a broader incision with a single insertion into the anterior chamber. Furthermore, the rounded distal tip minimizes the risk of damaging the outer wall of the Schlemm’s canal, thereby reducing the likelihood of traumatic bleeding.
In Figure 5, we summarized features of four devices and a brief summary of relevant complications.
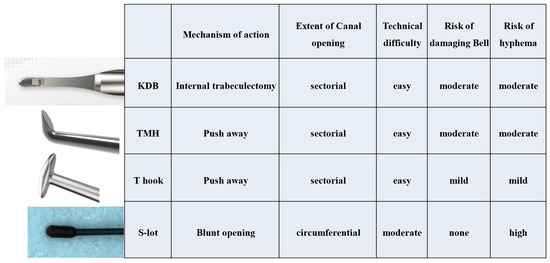
Figure 5.
Designs of four devices and brief summary of relevant complications.
In this study, we included POAG, XFG, and OH for analysis. XFG is characterized by higher IOP, faster visual field deterioration, and a poor response to medical therapy. Several authors have reported that IOP reduction in XFG achieved through canal-opening surgery surpasses that observed in POAG [28,29], whereas others have reported equivalent IOP reduction between XFG and POAG [30]. Therefore, the potential difference in surgical response between XFG and POAG may warrant further investigation in future studies.
Another confounding factor is the effects of combined cataract surgery. Many reports have shown that the combination of cataract and canal-opening surgery (COS) provides additional benefit in IOP reduction [1,31]. However, several authors have reported no enhanced IOP reduction with combined cataract and COS compared to COS alone [17]. In this study, we studied outcomes exclusively in cases of combined surgery, so the effects of cataract surgery will not influence the results.
5. Conclusions
Postoperative IOP reduction was compared among four canal-opening MIGS procedures. The most significant IOP reduction was observed in the S-lot cohort.
The T-hook cohort showed the least postoperative intracameral bleeding. While intracameral bleeding in the KDB and TMH cohorts was associated with short-term IOP elevation, it did not impact long-term IOP outcomes between 6 months and 3 years.
6. Limitation of This Study
This study is retrospective and non-randomized. Although preoperative IOP was comparable among cohorts, the S-lot cohort exhibited significantly more advanced visual field defects, suggesting that surgeons may have preferentially selected S-lot for more severe glaucoma cases. This could represent a potential bias that may have affected the outcomes. Randomized selection of surgical procedure is desirable for future studies. Additionally, the follow-up period for the T-hook cohort was significantly shorter, likely due to the recent introduction of the device.
To allow for a more accurate and unbiased comparison of surgical procedures, future studies should adopt a prospective, randomized design.
Author Contributions
Conceptualization, E.C.; methodology, E.C.; software, E.C.; validation, E.C. and T.C.; formal analysis, E.C.; investigation, E.C.; resources, E.C.; data curation, E.C.; writing—original draft preparation, E.C.; writing—review and editing, T.C.; visualization, E.C.; supervision, T.C.; project administration, E.C.; funding acquisition, E.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Sensho-kai Eye Institute #25000009 (protocol code C2023-01R dated 5 September 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study. Written informed consent for publication was not specifically obtained from the participating patients; however, the possibility of publication was disclosed during the process of obtaining consent for surgical agreement.
Data Availability Statement
The research data used in this research is available upon request from the corresponding author.
Acknowledgments
We extend our gratitude to the technicians at Sensho-kai for providing data that contributed to this study. All of them consented to the acknowledgement. During the preparation of this manuscript, the authors used Chat GPT 4 for the purposes of editing English. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| KDB | Kahook dual blade |
| TMH | Tanito microhook |
| S-lot | 360° suture trabeculotomy |
| COS | Canal-opening surgery |
| MIGS | Minimally invasive glaucoma surgery |
| PAS | Peripheral anterior synechia |
References
- Takata, M.; Ishikawa, H.; Ikeda, T.; Gomi, F. Conventional Trabeculotomy versus Gonioscopy-Assisted Transluminal Trabeculotomy: A Retrospective Cohort Study. J. Clin. Med. 2021, 11, 46. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wang, Y.E.; Quan, A.; Grajewski, A.; Hodapp, E.; Vanner, E.A.; Chang, T.C. Risk Factors for Complications and Failure after Gonioscopy-Assisted Transluminal Trabeculotomy in a Young Cohort. Ophthalmol. Glaucoma 2020, 3, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Irie, A.; Nakashima, K.I.; Inoue, T.; Kojima, S.; Takihara, Y.; Takahashi, E. Trabeculotomy Using the Kahook Dual Blade for Exfoliation Glaucoma and Primary Open Angle Glaucoma: Comparison of Outcomes According to Incision Range. J. Glaucoma 2024, 33, 270–276. [Google Scholar] [CrossRef]
- Sugihara, K.; Shimada, A.; Ichioka, S.; Harano, A.; Tanito, M. Comparison of Phaco-Tanito Microhook Trabeculotomy between Propensity-Score-Matched 120-Degree and 240-Degree Incision Groups. J. Clin. Med. 2023, 12, 7460. [Google Scholar] [CrossRef]
- Kuerten, D.; Walter, P.; Baumgarten, S.; Fuest, M.; Plange, N. 12-month outcomes of ab interno excisional goniotomy combined with cataract surgery in primary open-angle glaucoma and normal tension glaucoma. Int. Ophthalmol. 2023, 43, 2605–2612. [Google Scholar] [CrossRef]
- Wecker, T.; Anton, A.; Neuburger, M.; Jordan, J.F.; van Oterendorp, C. Trabeculotomy opening size and IOP reduction after Trabectome® surgery. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1643–1650. [Google Scholar] [CrossRef]
- Song, Y.; Zhu, X.; Zhang, Y.; Shu, J.; Dang, G.; Zhou, W.; Sun, L.; Li, F.; Lin, F.; Zhang, Y.; et al. Outcomes of Partial Versus Complete Goniotomy with or Without Phacoemulsification for Primary Open Angle Glaucoma: A Multicenter Study. J. Glaucoma 2023, 32, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wang, H.; Oatts, J.T.; Xin, C.; Yin, P.; Zhang, L.; Tian, J.; Zhang, Y.; Cao, K.; Han, Y.; et al. A Prospective Study of Intraocular Pressure Spike and Failure After Gonioscopy-Assisted Transluminal Trabeculotomy in Juvenile Open-Angle Glaucoma: A Prospective Study of GATT in JOAG. Am. J. Ophthalmol. 2022, 236, 79–88. [Google Scholar] [CrossRef]
- Chihara, E.; Chihara, T. Development and Application of a New T-shaped Internal Trabeculotomy Hook (T-hook). Clin. Ophthalmol. 2022, 16, 3919–3926. [Google Scholar] [CrossRef]
- Day, A.C.; Donachie, P.H.; Sparrow, J.M.; Johnston, R.L. The Royal College of Ophthalmologists’ National Ophthalmology Database study of cataract surgery: Report 1, visual outcomes and complications. Eye 2015, 29, 552–560. [Google Scholar] [CrossRef]
- Ishida, A.; Ichioka, S.; Takayanagi, Y.; Tsutsui, A.; Manabe, K.; Tanito, M. Comparison of Postoperative Hyphemas between Microhook Ab Interno Trabeculotomy and iStent Using a New Hyphema Scoring System. J. Clin. Med. 2021, 10, 5541. [Google Scholar] [CrossRef] [PubMed]
- Rosenquist, R.; Epstein, D.; Melamed, S.; Johnson, M.; Grant, W.M. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr. Eye Res. 1989, 8, 1233–1240. [Google Scholar] [CrossRef]
- Stepanik, J. Measuring velocity of flow in aqueous veins. Am. J. Ophthalmol. 1954, 37, 918–922. [Google Scholar] [CrossRef]
- De Vries, S. De Zichtbare Afvoer Van Het Kammerwater; Drukkerij Kinsbergen: Amsterdam, The Netherlands, 1947. [Google Scholar]
- Cha, E.D.K.; Xu, J.; Gong, L.; Gong, H. Variations in active outflow along the trabecular outflow pathway. Exp. Eye Res. 2016, 146, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Manabe, S.I.; Sawaguchi, S.; Hayashi, K. The effect of the extent of the incision in the Schlemm canal on the surgical outcomes of suture trabeculotomy for open-angle glaucoma. Jpn. J. Ophthalmol. 2017, 61, 99–104. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, P.; Sugihara, K.; Zhu, X.; Yang, X.; Li, X.; Liu, Y.; Zhang, H.; Yan, X.; Lin, F.; et al. Influence of Goniotomy Size on Treatment Safety and Efficacy for Primary Open-Angle Glaucoma: A Multicenter Study. Am. J. Ophthalmol. 2023, 256, 118–125. [Google Scholar] [CrossRef]
- Sugihara, K.; Ida, C.; Ohtani, H.; Tanito, M. Comparison of Standalone Tanito Microhook Trabeculotomy Between Unilateral and Bilateral Incision Groups. J. Clin. Med. 2025, 14, 1976. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, M.T.; Lee, D.; King, J.T.; Thomsen, S.; An, J.A. Comparison of Surgical Outcomes Of 360° Circumferential Trabeculotomy Versus Sectoral Excisional Goniotomy with The Kahook Dual Blade at 6 Months. Clin. Ophthalmol. 2019, 13, 2017–2024. [Google Scholar] [CrossRef]
- Le, C.; Kazaryan, S.; Hubbell, M.; Zurakowski, D.; Ayyala, R.S. Surgical Outcomes of Phacoemulsification Followed by iStent Implantation Versus Goniotomy with the Kahook Dual Blade in Patients with Mild Primary Open-angle Glaucoma with a Minimum of 12-Month Follow-up. J. Glaucoma 2019, 28, 411–414. [Google Scholar] [CrossRef]
- Asaoka, R.; Nakakura, S.; Mochizuki, T.; Ishida, A.; Fujino, Y.; Ishii, K.; Obana, A.; Tanito, M.; Kiuchi, Y. Which is More Effective and Safer? Comparison of Propensity Score-Matched Microhook Ab Interno Trabeculotomy and iStent Inject. Ophthalmol. Ther. 2023, 12, 2757–2768. [Google Scholar] [CrossRef]
- Qiao, Y.; Tan, C.; Chen, X.; Sun, X.; Chen, J. Gonioscopy-assisted transluminal trabeculotomy versus goniotomy with Kahook dual blade in patients with uncontrolled juvenile open-angle glaucoma: A retrospective study. BMC Ophthalmol. 2021, 21, 395. [Google Scholar] [CrossRef]
- Elhusseiny, A.M.; El Sayed, Y.M.; El Sheikh, R.H.; Gawdat, G.I.; Elhilali, H.M. Circumferential Schlemm’s Canal Surgery in Adult and Pediatric Glaucoma. Curr. Eye Res. 2019, 44, 1281–1290. [Google Scholar] [CrossRef]
- Rao, A.; Khan, S.M.; Mukherjee, S. Causes of Immediate and Early IOP Spikes After Circumferential Gonioscopy-Assisted Transluminal Trabeculotomy Using ASOCT. Clin. Ophthalmol. 2023, 17, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Crowell, E.L.; Baker, L.; Chuang, A.Z.; Feldman, R.M.; Bell, N.P.; Chévez-Barrios, P.; Blieden, L.S. Characterizing Anterior Segment OCT Angle Landmarks of the Trabecular Meshwork Complex. Ophthalmology 2018, 125, 994–1002. [Google Scholar] [CrossRef]
- Mori, S.; Tanito, M.; Shoji, N.; Yokoyama, Y.; Kameda, T.; Shoji, T.; Mizoue, S.; Saito, Y.; Ishida, K.; Ueda, T.; et al. Noninferiority of Microhook to Trabectome: Trabectome versus Ab Interno Microhook Trabeculotomy Comparative Study (Tram Trac Study). Ophthalmol. Glaucoma 2022, 5, 452–461. [Google Scholar] [CrossRef]
- Omoto, T.; Fujishiro, T.; Asano-Shimizu, K.; Sugimoto, K.; Sakata, R.; Murata, H.; Asaoka, R.; Honjo, M.; Aihara, M. Comparison of 12-month surgical outcomes of ab interno trabeculotomy with phacoemulsification between spatula-shaped and dual-blade microhooks. Jpn. J. Ophthalmol. 2021, 65, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Tanihara, H.; Negi, A.; Akimoto, M.; Terauchi, H.; Okudaira, A.; Kozaki, J.; Takeuchi, A.; Nagata, M. Surgical effects of trabeculotomy ab externo on adult eyes with primary open angle glaucoma and pseudoexfoliation syndrome. Arch. Ophthalmol. 1993, 111, 1653–1661. [Google Scholar] [CrossRef]
- Ting, J.L.; Damji, K.F.; Stiles, M.C.; Group, T.S. Ab interno trabeculectomy: Outcomes in exfoliation versus primary open-angle glaucoma. J. Cataract. Refract. Surg. 2012, 38, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Aktas, Z.; Ozdemir Zeydanli, E.; Uysal, B.S.; Yigiter, A. Outcomes of Prolene Gonioscopy Assisted Transluminal Trabeculotomy in Primary Open Angle Glaucoma and Pseudoexfoliation Glaucoma: A Comparative Study. J. Glaucoma 2022, 31, 751–756. [Google Scholar] [CrossRef]
- Tojo, N.; Abe, S.; Miyakoshi, M.; Hayashi, A. Comparison of intraocular pressure fluctuations before and after ab interno trabeculectomy in pseudoexfoliation glaucoma patients. Clin. Ophthalmol. 2017, 11, 1667–1675. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).