
Histological Analysis of Intracranial Cerebral Arteries for Elastin Thickness, Wall Thickness, and Vessel Diameters: An Atlas for Computational Modeling and a Proposed Predictive Multivariable Model of Elastin Thickness

 , ,
, , 
Abstract
1. Introduction
Cerebrovascular Pathology and Management
2. Methods
2.1. Tissue Procurement and Preparation
2.2. Processing and Histological Analysis
2.3. Statistical Analysis
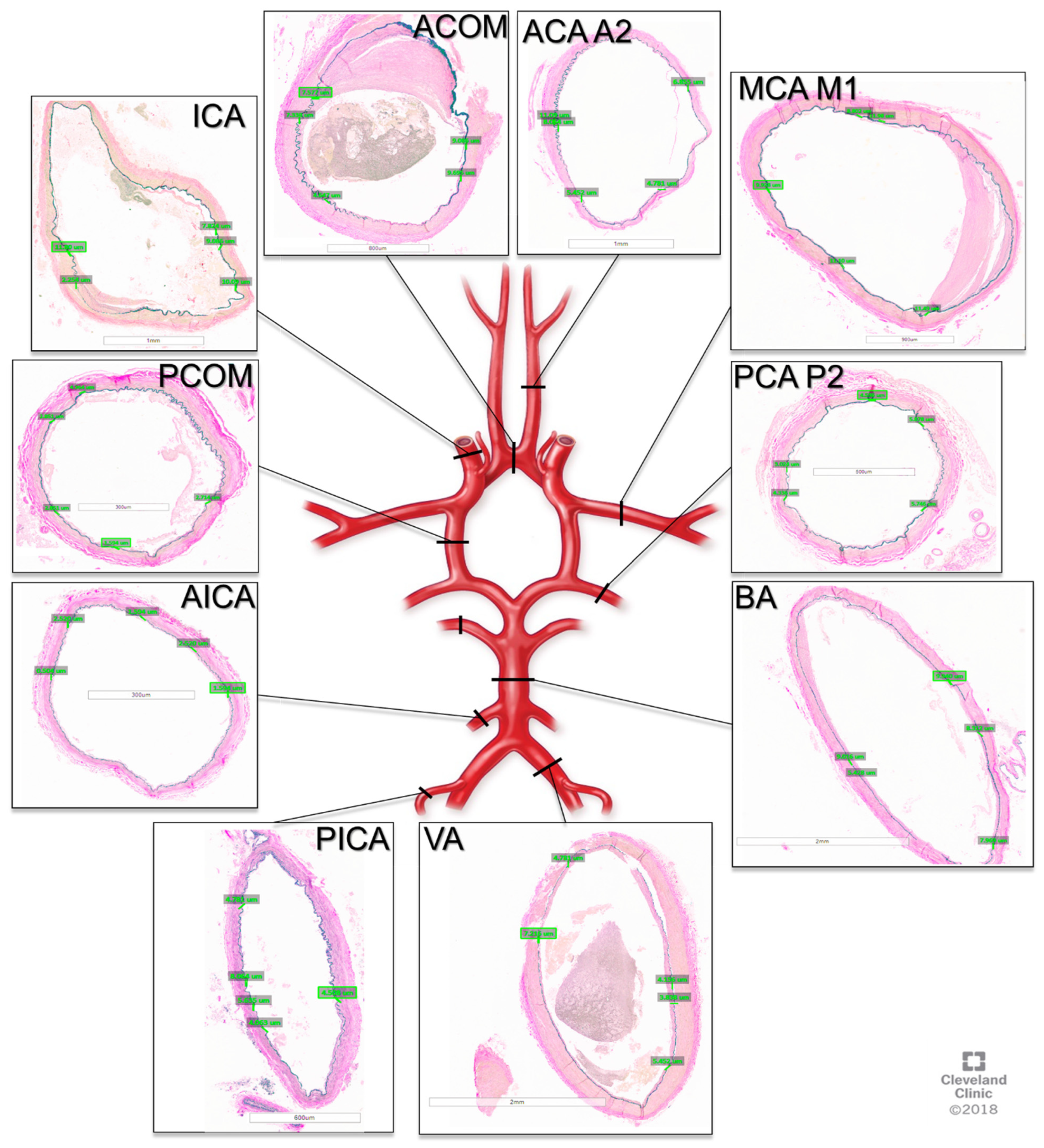
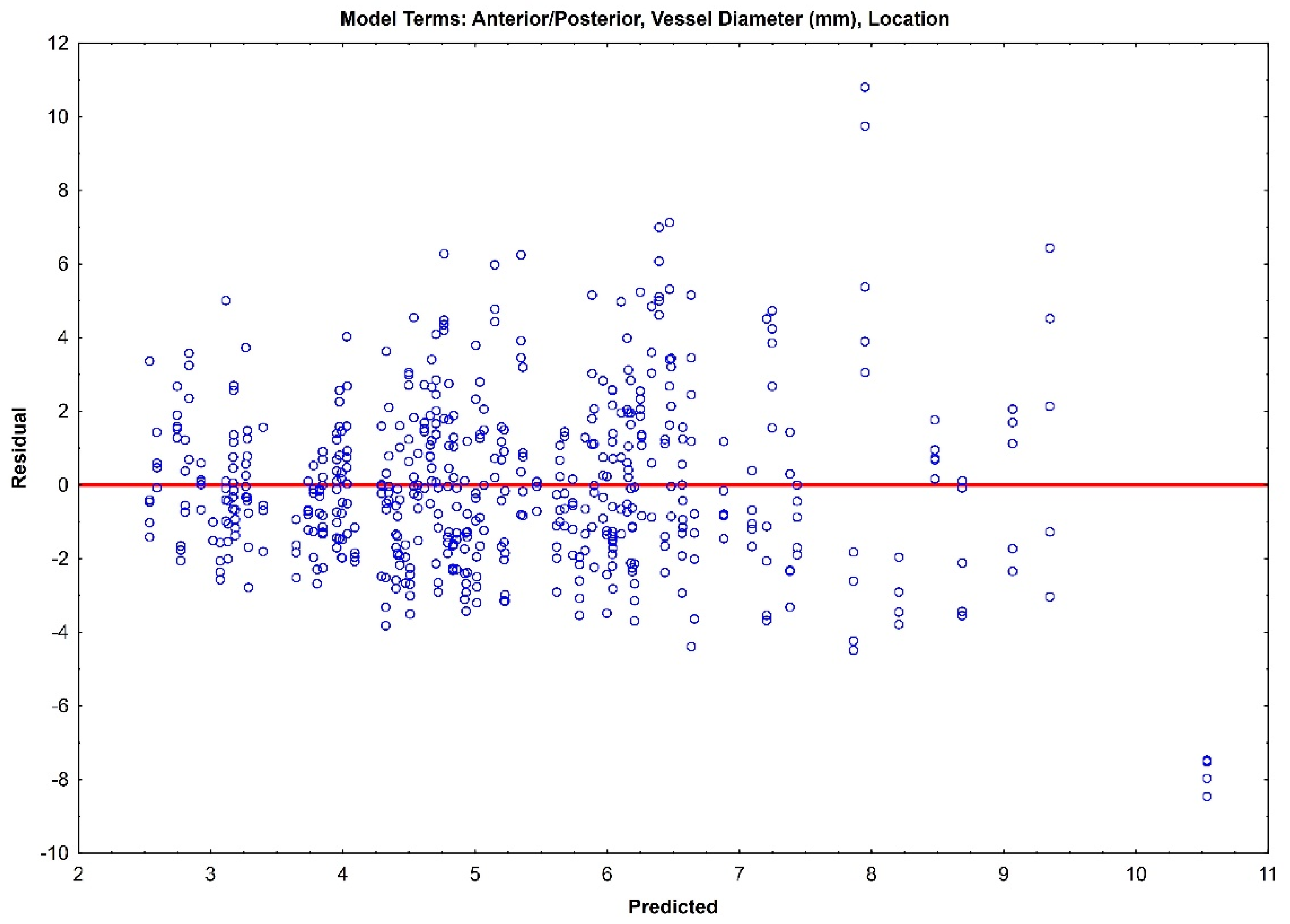
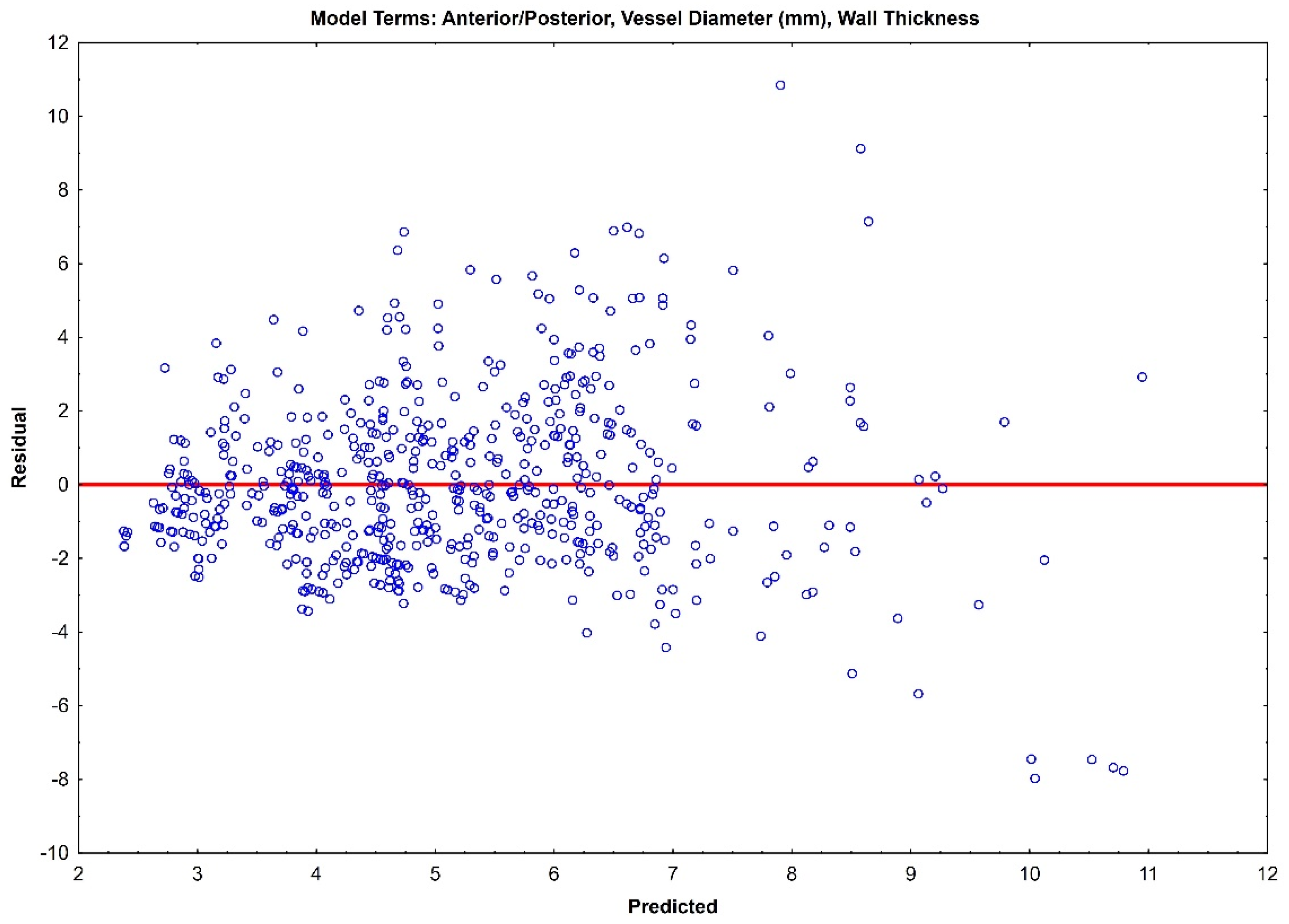
3. Results
4. Discussion
4.1. Elastin Thickness, Anterior Versus Posterior Circulation, and the Link to Cerebral Aneurysm Rupture Risk
4.2. Clinical Translation and Predictive Modeling
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiebers, D.O.; Whisnant, J.P.; Huston, J., 3rd; Meissner, I.; Brown, R.D., Jr.; Piepgras, D.G.; Forbes, G.S.; Thielen, K.; Nichols, D.; O’Fallon, W.M.; et al. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet (Lond. Engl.) 2003, 362, 103–110. [Google Scholar] [CrossRef]
- Ohaegbulam, S.C. The epidemiology of brain arteriovenous malformations. Neurosurgery 2001, 49, 226–228. [Google Scholar]
- Keedy, A. An overview of intracranial aneurysms. Mcgill J. Med. 2006, 9, 141–146. [Google Scholar] [CrossRef]
- Etminan, N.; Brown, R.D., Jr.; Beseoglu, K.; Juvela, S.; Raymond, J.; Morita, A.; Torner, J.C.; Derdeyn, C.P.; Raabe, A.; Mocco, J.; et al. The unruptured intracranial aneurysm treatment score: A multidisciplinary consensus. Neurology 2015, 85, 881–889. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Backes, D.; Vergouwen, M.D.; Tiel Groenestege, A.T.; Bor, A.S.; Velthuis, B.K.; Greving, J.P.; Algra, A.; Wermer, M.J.; van Walderveen, M.A.; terBrugge, K.G.; et al. PHASES Score for Prediction of Intracranial Aneurysm Growth. Stroke 2015, 46, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Backes, D.; Rinkel, G.J.E.; Greving, J.P.; Velthuis, B.K.; Murayama, Y.; Takao, H.; Ishibashi, T.; Igase, M.; terBrugge, K.G.; Agid, R.; et al. ELAPSS score for prediction of risk of growth of unruptured intracranial aneurysms. Neurology 2017, 88, 1600–1606. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.Q.; Chen, R.D.; Xu, W.D.; Li, H.; Yu, J.S. A predictive hemodynamic model based on risk factors for ruptured mirror aneurysms. Front. Neurol. 2022, 13, 998557. [Google Scholar] [CrossRef]
- Mohr, J.P.; Parides, M.K.; Stapf, C.; Moquete, E.; Moy, C.S.; Overbey, J.R.; Salman, R.A.-S.; Vicaut, E.; Young, W.L.; Houdart, E.; et al. Medical management with or without interventional therapy for unruptured brain arteriovenous malformations (ARUBA): A multicentre, non-blinded, randomised trial. Lancet (Lond. Engl.) 2014, 383, 614–621. [Google Scholar] [CrossRef]
- Bijlenga, P.; Ebeling, C.; Jaegersberg, M.; Summers, P.; Rogers, A.; Waterworth, A.; Iavindrasana, J.; Macho, J.; Pereira, V.M.; Bukovics, P.; et al. Risk of rupture of small anterior communicating artery aneurysms is similar to posterior circulation aneurysms. Stroke 2013, 44, 3018–3026. [Google Scholar] [CrossRef]
- De Simone, M.; Fontanella, M.M.; Choucha, A.; Schaller, K.; Machi, P.; Lanzino, G.; Bijlenga, P.; Kurz, F.T.; Lövblad, K.O.; De Maria, L. Current and Future Applications of Arterial Spin Labeling MRI in Cerebral Arteriovenous Malformations. Biomedicines 2024, 12, 753. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schnell, S.; Wu, C.; Ansari, S.A. Four-dimensional MRI flow examinations in cerebral and extracerebral vessels—Ready for clinical routine? Curr. Opin. Neurol. 2016, 29, 419–428. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Samaniego, E.A.; Dabus, G.; Meyers, P.M.; Kan, P.T.; Frösen, J.; Lanzino, G.; Welch, B.G.; Volovici, V.; Gonzalez, F.; Fifi, J.; et al. Most Promising Approaches to Improve Brain AVM Management: ARISE I Consensus Recommendations. Stroke 2024, 55, 1449–1463. [Google Scholar] [CrossRef] [PubMed]
- Gounis, M.J.; Ughi, G.J.; Marosfoi, M.; Lopes, D.K.; Fiorella, D.; Bezerra, H.G.; Liang, C.W.; Puri, A.S. Intravascular Optical Coherence Tomography for Neurointerventional Surgery. Stroke 2019, 50, 218–223. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Thiyagarajah, N.; Achey, R.; Rashidi, M.; Moore, N.Z. Computational Fluid–Structure Interactions in the Human Cerebrovascular System: Part 1—A Review of the Current Understanding of Cerebrovascular Biomechanics. ASME J. Med. Diagn. 2022, 5, 030801. [Google Scholar] [CrossRef]
- Qin, G.; Wang, L.; Hua, Y.; Hou, H.; Zou, Q.; Wang, D.; Hu, Z.; Lu, D. Comparative morphology of the internal elastic lamina of cerebral and peripheral arteries. Int. J. Clin. Exp. Pathol. 2020, 13, 764–770. [Google Scholar]
- Bank, A.J.; Wang, H.; Holte, J.E.; Mullen, K.; Shammas, R.; Kubo, S.H. Contribution of collagen, elastin, and smooth muscle to in vivo human brachial artery wall stress and elastic modulus. Circulation 1996, 94, 3263–3270. [Google Scholar] [CrossRef] [PubMed]
- Wagenseil, J.E.; Mecham, R.P. Elastin in large artery stiffness and hypertension. J. Cardiovasc. Transl. Res. 2012, 5, 264–273. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, R.M. Morphology of cerebral arteries. Pharmacol. Ther. 1995, 66, 149–173. [Google Scholar] [CrossRef]
- Kiliç, T.; Akakin, A. Anatomy of cerebral veins and sinuses. Front. Neurol. Neurosci. 2008, 23, 4–15. [Google Scholar]
- Cipolla, M.J. The Cerebral Circulation; National Library of Medicine: Bethesda, MD, USA, 2009. [Google Scholar] [CrossRef]
- Tykocki, T.; Kostkiewicz, B. Aneurysms of the anterior and posterior cerebral circulation: Comparison of the morphometric features. Acta Neurochir. (Wien) 2014, 156, 1647–1654. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bergel, D.H. The dynamic elastic properties of the arterial wall. J. Physiol. 1961, 156, 458–469. [Google Scholar] [CrossRef]
- Davison, M.; McCune, M.; Thiyagarajah, N.; Kashkoush, A.; Achey, R.; Shost, M.; Toth, G.; Bain, M.; Moore, N. The incidence of infratentorial arteriovenous malformation-associated aneurysms: An institutional case series and systematic literature review. J. Neurointerv. Surg. 2024. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.F.M.; Gelfand, A.E. Bayesian Statistics without Tears: A Sampling-Resampling Perspective. Am. Stat. 1992, 46, 84–88. [Google Scholar] [CrossRef]
- Fonck, E.; Feigl, G.G.; Fasel, J.; Sage, D.; Unser, M.; Rüfenacht, D.A.; Stergiopulos, N. Effect of aging on elastin functionality in human cerebral arteries. Stroke 2009, 40, 2552–2556. [Google Scholar] [CrossRef] [PubMed]
- Dorňák, T.; Král, M.; Hazlinger, M.; Herzig, R.; Veverka, T.; Buřval, S.; Šaňák, D.; Zapletalová, J.; Antalíková, K.; Kaňovský, P. Posterior vs. anterior circulation infarction: Demography, outcomes, and frequency of hemorrhage after thrombolysis. Int. J. Stroke 2015, 10, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Doddasomayajula, R.; Chung, B.; Hamzei-Sichani, F.; Putman, C.M.; Cebral, J.R. Differences in Hemodynamics and Rupture Rate of Aneurysms at the Bifurcation of the Basilar and Internal Carotid Arteries. AJNR Am. J. Neuroradiol. 2017, 38, 570–576. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specimen | Age | Gender | BMI | Past Medical History |
|---|---|---|---|---|
| 1 | 80 | M | 21 | Parkinson’s disease, Alzheimer’s, prostate cancer in remission |
| 2 | 91 | M | 19 | Coronary artery disease, Alzheimer’s |
| 3 | 87 | F | 27 | Coronary artery disease, Mallory–Weiss tear with GI bleed, dementia, hypothyroidism, cardiomyopathy |
| 4 | 90 | F | 23 | Congestive heart failure, hypertension, chronic obstructive pulmonary disease, Alzheimer’s |
| 5 | 51 | M | 23 | End-stage spindle cell carcinoma with brain metastases, hypertension, coronary artery disease, 30 pack per year smoker |
| Vessel | Reviewer 1 | Reviewer 2 | Combined Data | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (µm) | SD (µm) | Median (µm) | Mean (µm) | SD (µm) | Median (µm) | Mean (µm) | SD (µm) | Median (µm) | ||
| Anterior Circulation | ICA | 6.3 | 3.4 | 5.6 | 8.9 | 3.7 | 8.6 | 7.6 | 3.8 | 7.2 |
| MCA M1 | 8.2 | 3.7 | 7.6 | 8.9 | 3.1 | 8.6 | 8.6 | 3.4 | 8.2 | |
| MCA M2 | 5.7 | 2.0 | 5.0 | 8.9 | 2.2 | 5.3 | 5.6 | 2.1 | 5.1 | |
| MCA M3 | 3.6 | 1.3 | 3.3 | 3.7 | 1.8 | 3.5 | 3.7 | 1.6 | 3.3 | |
| MCA M4 | 3.1 | 1.7 | 2.9 | 3.1 | 1.6 | 3.2 | 3.1 | 1.6 | 3.0 | |
| ACA A1 | 7.9 | 3.4 | 7.3 | 7.5 | 2.5 | 7.6 | 7.7 | 2.9 | 7.4 | |
| ACA A2 | 6.7 | 2.4 | 6.3 | 6.3 | 1.8 | 6.1 | 6.5 | 2.1 | 6.3 | |
| ACOM | 6.2 | 4.6 | 5.3 | 6.8 | 2.4 | 6.7 | 6.5 | 3.7 | 6.1 | |
| Posterior Circulation | VA | 4.3 | 2.0 | 4.2 | 4.2 | 1.7 | 3.9 | 4.2 | 1.8 | 4.0 |
| BA | 4.2 | 3.1 | 4.0 | 7.1 | 4.4 | 8.3 | 5.6 | 4.0 | 4.3 | |
| PICA | 3.3 | 1.5 | 3.5 | 3.3 | 1.8 | 3.2 | 3.3 | 1.7 | 3.4 | |
| AICA | 2.6 | 2.0 | 2.3 | 2.5 | 2.1 | 1.5 | 2.6 | 1.7 | 2.2 | |
| SCA | 3.9 | 1.3 | 4.0 | 3.7 | 1.2 | 3.8 | 3.8 | 1.2 | 3.9 | |
| PCA P1 | 6.8 | 3.7 | 7.1 | 6.7 | 3.0 | 6.6 | 6.8 | 3.4 | 7.0 | |
| PCA P2 | 5.7 | 2.1 | 5.6 | 5.6 | 1.9 | 5.7 | 5.7 | 2.0 | 5.6 | |
| PCOM | 4.2 | 1.5 | 3.8 | 4.3 | 1.5 | 4.2 | 4.2 | 1.4 | 4.0 | |
| CV | 1.1 | 1.3 | 0.6 | 0.9 | 1.1 | 0.3 | 1.0 | 1.2 | 0.5 | |
| Parameter | Class Values | Coefficient | Std Error | p-Value |
|---|---|---|---|---|
| Intercept | 2.32 | 0.46 | 0.001 | |
| Anterior/Posterior | Anterior = 1, Posterior = 0 | 1.01 | 0.61 | 0.139 |
| Vessel Diameter (mm) | 1.27 | 0.07 | <0.0001 | |
| Location Right/Left | Left = 1 Right = 0 | 0.38 | 0.14 | 0.024 |
| Observer 1 vs. 2 | Observer 1 = 1 Observer 2 = 0 | −0.043 | 0.14 | 0.77 |
| Parameter | Class Values | Coefficient | Std Error | p-Value |
|---|---|---|---|---|
| Intercept | 2.10 | 0.30 | 0.0001 | |
| Anterior/Posterior | Anterior = 1, Posterior = 0 | 1.72 | 0.35 | 0.0011 |
| Wall Thickness (µm) | 0.015 | 0.001 | <0.0001 | |
| Right/Left Location | Left = 1 Right = 0 | −0.027 | 0.18 | 0.88 |
| Parameter | Class Values | Coefficient | Std Error | p-Value |
|---|---|---|---|---|
| Intercept | 29.42 | 13.38 | 0.059 | |
| Anterior/Posterior | Anterior = 1, Posterior = 0 | −33.32 | 18.23 | 0.105 |
| Vessel Diameter (mm) | 77.59 | 2.06 | <0.0001 | |
| Right/Left Location | Left = 1 Right = 0 | 11.78 | 4.02 | 0.017 |
| Parameter | Class Values | Coefficient | Std Error | p-Value |
|---|---|---|---|---|
| Intercept | 4.46 | 0.43 | <0.0001 | |
| Anterior/Posterior | Anterior = 1, Posterior = 0 | 1.45 | 0.61 | 0.044 |
| Model #1 | ||||
|---|---|---|---|---|
| Parameter | Class Values | Coefficient | Std Error | p-Value |
| Intercept | 2.1029 | 0.41 | 0.0009 | |
| Anterior/Posterior | Anterior = 1, Posterior = 0 | 1.1277 | 0.53 | 0.066 |
| Vessel Diameter (mm) | 1.3548 | 0.096 | <0.0001 | |
| Right/Left Location | Left = 1 Right = 0 | 0.4237 | 0.18 | 0.048 |
| Model #2 | ||||
| Intercept | 2.1151 | 0.35 | 0.0003 | |
| Anterior/Posterior | Anterior = 1, Posterior = 0 | 1.3325 | 0.45 | 0.0182 |
| Vessel Diameter (mm) | 0.9044 | 0.17 | <0.0001 | |
| Wall Thickness (µm) | 0.005754 | 0.002 | 0.0017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thiyagarajah, N.; Witek, A.; Davison, M.; Butler, R.; Erdemir, A.; Tsiang, J.; Hussain, M.S.; Prayson, R.; Bain, M.; Moore, N.Z. Histological Analysis of Intracranial Cerebral Arteries for Elastin Thickness, Wall Thickness, and Vessel Diameters: An Atlas for Computational Modeling and a Proposed Predictive Multivariable Model of Elastin Thickness. J. Clin. Med. 2025, 14, 4320. https://doi.org/10.3390/jcm14124320
Thiyagarajah N, Witek A, Davison M, Butler R, Erdemir A, Tsiang J, Hussain MS, Prayson R, Bain M, Moore NZ. Histological Analysis of Intracranial Cerebral Arteries for Elastin Thickness, Wall Thickness, and Vessel Diameters: An Atlas for Computational Modeling and a Proposed Predictive Multivariable Model of Elastin Thickness. Journal of Clinical Medicine. 2025; 14(12):4320. https://doi.org/10.3390/jcm14124320
Chicago/Turabian StyleThiyagarajah, Nishanth, Alex Witek, Mark Davison, Robert Butler, Ahmet Erdemir, John Tsiang, Mohammed Shazam Hussain, Richard Prayson, Mark Bain, and Nina Z. Moore. 2025. "Histological Analysis of Intracranial Cerebral Arteries for Elastin Thickness, Wall Thickness, and Vessel Diameters: An Atlas for Computational Modeling and a Proposed Predictive Multivariable Model of Elastin Thickness" Journal of Clinical Medicine 14, no. 12: 4320. https://doi.org/10.3390/jcm14124320
APA StyleThiyagarajah, N., Witek, A., Davison, M., Butler, R., Erdemir, A., Tsiang, J., Hussain, M. S., Prayson, R., Bain, M., & Moore, N. Z. (2025). Histological Analysis of Intracranial Cerebral Arteries for Elastin Thickness, Wall Thickness, and Vessel Diameters: An Atlas for Computational Modeling and a Proposed Predictive Multivariable Model of Elastin Thickness. Journal of Clinical Medicine, 14(12), 4320. https://doi.org/10.3390/jcm14124320